ABSTRACT
This study aimed to identify an ecosystem of urban endemism that explains the persistence of SARS-CoV-2 during the first 18 months of the pandemic in the municipality of Petrópolis, Rio de Janeiro, Brazil. We analyzed official records of monthly COVID-19 cases, georeferenced according to the residence address of each confirmed case. Monthly heat maps identifying points with different spatial densities of the disease were constructed by applying the kernel methodology. Heat spots with five intensity levels were identified for the spatial density of cases. The points of highest intensity, known as hotspots, remained constant throughout the period in a polygon of approximately 4 km2 located in the center of the city of Petrópolis. In conclusion, we found that the highest concentration of cases remained in the same location over time, despite the sporadic dispersion of cases within the municipal territory.
Keywords: SARS-CoV-2, COVID-19, Pandemics, Ecoepidemiology, Disease Hotspot, Spatial Analysis, Brazil
INTRODUCTION
During the COVID-19 pandemic, several researchers used spatial analysis methods to identify the territorial determinants of its distribution, focusing on social inequalities and inequities in access to medical care. These studies have covered the risk of the disease at the regional or municipal level, using statistical records from the epidemiological surveillance systems of different countries, such as Ecuador 1, Mexico 2, Portugal 3, Germany 4, among others. In addition, there are extensive literature reviews on the use of geographic information analysis methods, particularly in China 5 and the United States 6.
Some authors have used heat maps to identify areas with a high relative density of cases, known as hotspots, in places as diverse as the state of Sergipe in Brazil 7 and Punjab in Pakistan 8. These studies have analyzed epidemiological surveillance data according to geopolitical divisions or through the use of heat maps of different scales, in order to define and describe areas of higher or lower epidemic risk at different times of the pandemic. In all cases, the virus is assumed to have been introduced in areas with a high risk of exposure, and it is considered that these hotspots experience epidemic outbreaks of different magnitudes depending on the size and density of the territory, but that they tend to decrease when the immunity of the exposed population reaches a certain level.
Over the last century, several concepts have been constructed on the basis of the “natural nidality of communicable diseases” developed by Pavlovsky 9; these concepts highlight the relevance of geographic space in determining the health-disease process 10. This allows us to analyze, in an integrated and dialectical manner, the effects of human intervention on environmental and climatic changes, as well as their impact on health, particularly regarding the emergence of new communicable diseases 11. In this context, the theory of the natural niches of communicable diseases was developed, which includes proposals for the control and even eradication of causal agents, in this respect Roche states that “we can define the niche of an organism as the position of this organism within its environment, available resources and competitors. Then, it is characterized by all the conditions required to sustain a viable population of the organism, in space and time.” 12.
Normally, these perspectives are applied to rural spaces or large geographical areas where different elements related with the viability, maintenance and transmission of the infectious agent coexist, including vectors or reservoirs, in addition to the susceptible host 13. This is considered an endemic condition, that is, a geographic space in which the infection is constantly maintained at a level that allows the continuous transmission of the disease 13. Thus, this study aimed to identify an ecosystem of urban endemism that explains the persistence of SARS-CoV-2 during the first 18 months of the pandemic in the municipality of Petrópolis, Rio de Janeiro, Brazil.
KEY MESSAGES
Motivation for the study. During the COVID-19 pandemic, spatial analysis methodologies were used to identify the territorial determinants of its distribution and social inequalities in access to medical care.
Main findings. We found a concentration of cases in a specific location of the municipality, which remained constant throughout the study period, with sporadic outbreaks in other areas.
Implications. It is necessary to pay attention to possible endemic foci of viral diseases in urban settings and to take measures to eliminate them as well as to prevent their spread within and outside the area.
THE STUDY
We carried out a descriptive and spatial analysis of confirmed cases of SARS-CoV-2 infection in the municipality of Petrópolis, located in the State of Rio de Janeiro, at a distance of approximately 70 km from the city of Rio de Janeiro. The municipality has a total area of 795,798 km2 and an average altitude of 738 m. According to projections, the total population was 306,678 inhabitants in 2020.
A total of 49,050 records of confirmed SARS-CoV-2 cases during the period from March 1, 2020 to August 31, 2021 (Table 1) were geocoded. The data were provided by the Municipal Health Secretariat - SMS/Petrópolis. We used the QuantumGIS® software to produce the maps and the Google® cartographic base was used for geocoding (Google Maps® API). In cases where the algorithm presented errors, such as in unnumbered routes, passages, avenues or lanes, data was verified by analyzing satellite images from Google Earth® and on-site visits to the identified addresses. In order to guarantee anonymity of the records, monthly heat maps were prepared that identified clusters with a higher spatial density of cases.
Table 1. Number of monthly records of geocoded COVID-19 cases in the Municipality of Petrópolis (March 2020 to August 2021).
| Month and year | n |
|---|---|
| March 2020 | 41 |
| April 2020 | 795 |
| May 2020 | 1012 |
| June 2020 | 1127 |
| July 2020 | 1129 |
| August 2020 | 1044 |
| September 2020 | 1065 |
| October 2020 | 578 |
| November 2020 | 1173 |
| December 2020 | 2949 |
| January 2021 | 2677 |
| February 2021 | 1381 |
| March 2021 | 2319 |
| April 2021 | 2945 |
| May 2021 | 7918 |
| June 2021 | 6710 |
| July 2021 | 5737 |
| August 2021 | 8428 |
Source: Prepared by the authors based on data from the Municipal Health Secretariat of Petrópolis.
The kernel density estimation, widely known and used in the epidemiological context 14, was used to identify the areas with the highest concentration of cases. This estimation transforms the vector layer of points (georeferenced records) into a monochromatic raster data showing the concentration of cases across 30 cm pixels. The kernel density is a function that counts all points within a given region of influence, with probabilistic weighting based on the distance of each point from the location of interest 15-17.
We used two basic parameters for applying the kernel density method: the radius of influence and the k function 18. The radius of influence defines the area centered on the estimation point, which indicates how many events contribute to the estimate of the intensity function λ 15. For this study, we determined a radius of influence of 1 km, based on previous research 18.
The k function is less relevant than the radius of influence, since an alteration of the radius affects the entire possible interpolation field 19, which is more critical for the representation of the phenomena. We chose the quartic function among the most commonly used functions, which proved to be the most effective one in identifying clusters of cases (hotspots) within the chosen radius, without losing contact areas between hotspots (average areas), which made it possible to analyze the expansion or retraction of the virus over time, as well as its persistence in specific areas.
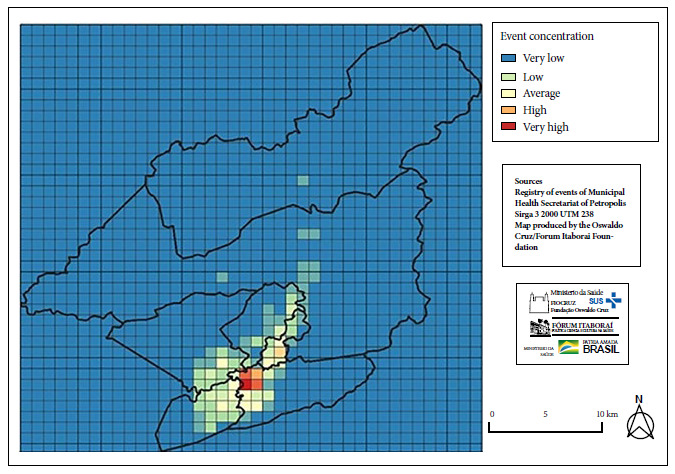
In order to better identify the physical area of the hotspots with the highest intensity and to monitor monthly disease persistence, a coordinate grid was created with squares of 1 km2 area, using the equirectangular projected coordinate system, in a layout similar to a Cartesian plane 20. Maps generated by kernel interpolation were overlaid on the squares to calculate a persistence score for each km2. The areas of highest heat intensity were transformed into vector data, where each pixel produced by the kernel interpolator was converted into a point with a weight proportional to its density. In this way, approximately 11 million pixel points were obtained for each 1 km square. The vector values of each of the monthly maps produced by kernel interpolation were summed, generating a quantifiable value for each square. These values were classified using the “false color” representation, simulating a multiband raster, which allowed the creation of a taxonomy of three-color spectra: blue (minimum values), yellow (intermediate values) and red (maximum values), with a gradient of five classes, including two intermediate classes.
Data from the 2010 Census 21, corresponding to the sectors relevant to the study and projected to the total population estimated for 2021 22, were used to characterize the area with the highest concentration of cases. Other relevant comments about the area were obtained through face-to-face visits by the researchers.
The Municipal Health Secretariat of the Municipality of Petrópolis authorized and provided the household records of the confirmed cases of COVID-19 as part of its epidemiological surveillance actions.
FINDINGS
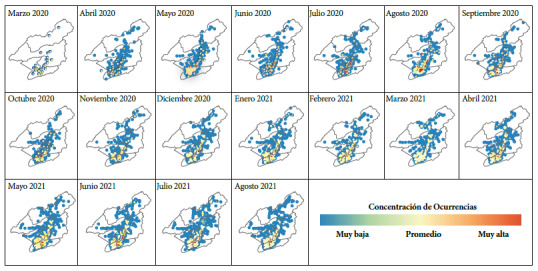
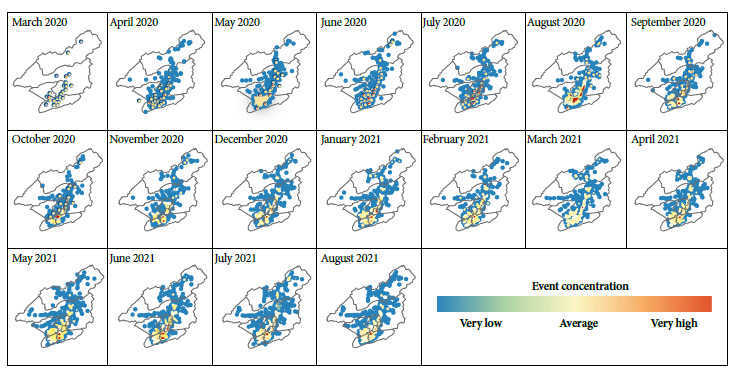
We found that, from April 2020 onwards, the same location had the highest concentration of cases for the following 18 months, regardless of the total number of records in each month and the dispersion of cases in the municipal territory (Figure 1).
Figure 1. Monthly maps of COVID-19 records in the municipality of Petrópolis based on the kernel density methodology (March 2020 to August 2021).
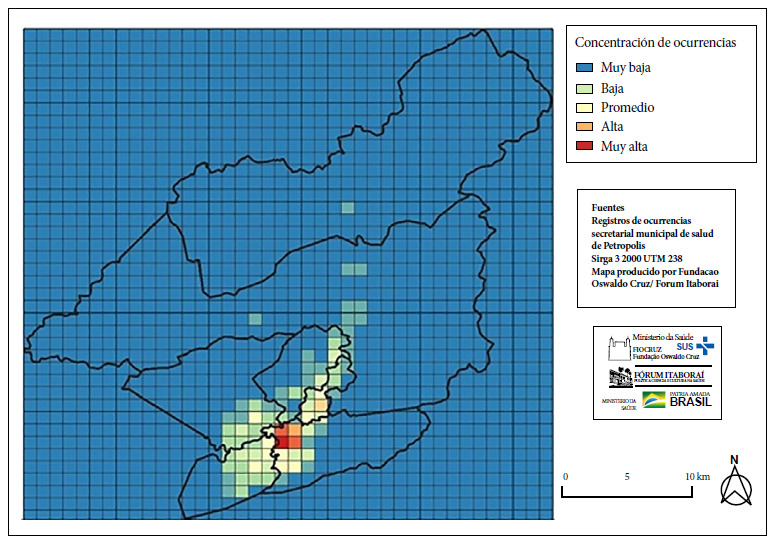
Four quadrants with higher persistence were identified by adding the vector values corresponding to each month in each square of the 1 km2 coordinate system (Figure 2), forming a polygon similar to the areas of higher heat intensity observed monthly. Therefore, we identified that the epidemic in Petrópolis was concentrated in a single location, with sporadic outbreaks in other quadrants of the municipality.
Figure 2. Areas of higher persistence of COVID-19 cases through the determination of vector values of 1 km² quadrants (March 2020 to August 2021).
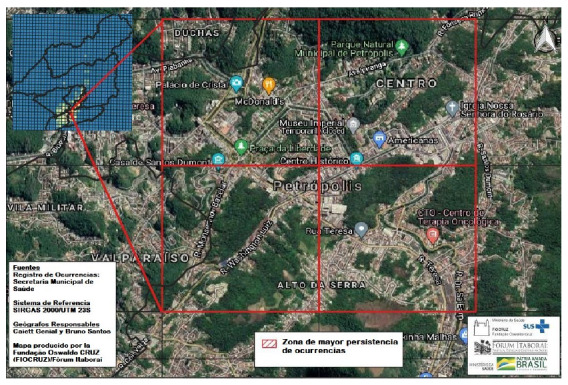
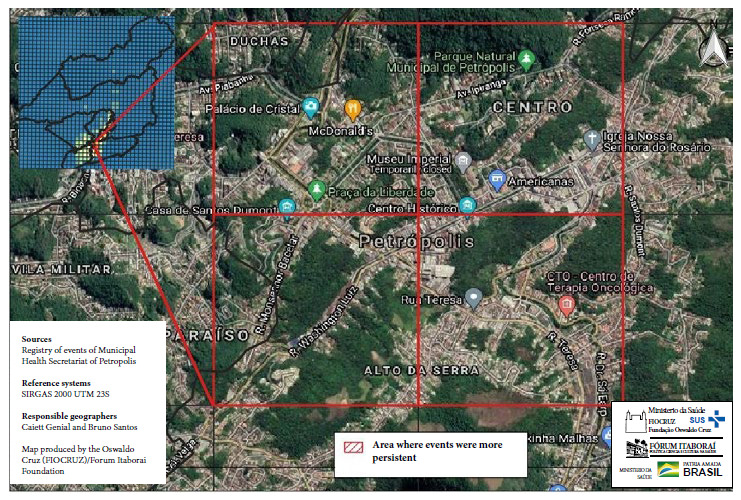
To identify this area of persistence, the Google ® satellite photo was superimposed on the cartographic base of the selected grids, which allowed the identification of the area corresponding to the “Historic Center” of the city and its immediate surroundings (Figure 3).
Figure 3. Area of higher persistence of COVID-19 in Petrópolis, enlarged with GoogleEarth® satellite images (March 2020 to August 2021).
Other central areas of the municipality also presented a considerable number of registered cases. However, this situation was not persistent throughout the period, suggesting the occurrence of possible localized outbreaks in time and space.
DISCUSSION
The use of spatial epidemiology in our study allowed us to understand the population dynamics of the disease, based on the urban organization of the municipality and the sociodemographic conditions. This provides the possibility of designing specific strategies to address each of these conditions, taking into account not only individual risk factors and virus transmission during epidemics or outbreaks, but also the characteristics of disease persistence in a given territory.
Most epidemiological analyses of the COVID-19 pandemic assume a transmission cycle that begins with the introduction of the agent into a given territory, followed by community transmission and the subsequent epidemic spread with transmission rates (Tr) greater than 1. This cycle is characterized by an initial increase in cases, followed by a plateau with transmission rates near 1, and finally a decrease as the number of susceptible individuals decreases. These successive epidemic waves may be attributed to the relaxation of social isolation measures 23 or to the introduction of new variants of the virus.
These reasons explain the persistence of the pandemic for more than 18 months at the global or national level, until finally a consistent decline occurred thanks to the high vaccination coverage achieved in developed countries. Therefore, health services around the world have focused on control mechanisms through sanitary barriers, whether at the international, national or local level. However, these measures, which have been effective in containing pandemics and more localized epidemic outbreaks in the past, appear to have been insufficient to contain the current COVID-19 pandemic. One possible reason for the shortfall of this strategy may be the lack of attention paid to potential endemic foci, i.e., “natural nests of the virus” in urban settings.
In this study, we considered a radius of 1 km to outline the heat circles. Theoretically, in territories of this size, a hotspot should rapidly achieve enough herd immunity to stop or at least significantly reduce virus transmission 24. However, the largest hot spot in the entire municipal territory was consistent during 18 months since the beginning of the epidemic, with small shifts that always remained within a polygon of less than 4 km2. Identifying the mechanisms by which the SARS-CoV-2 virus remains endemic would allow the implementation of measures that could not only eliminate this hotspot, but also prevent the effects of transmission within and beyond this endemic area.
The identified hotspot contains demographic and urban elements that explain the phenomenon. Petrópolis is a highly centralized municipality, like many in Brazil 25. The hotspot area coincides with the downtown area, which contains approximately 7% of the population. The tallest buildings in the city are located there, as well as a precarious community of significant size. This community interacts constantly with the nodal center of the polygon, 1-2 km2 away. The center concentrates federal, state and municipal public services, mostly exclusive to the entire municipality. In addition, there are medical offices, supermarkets, offices, popular and exclusive stores, markets and street fairs. There are also museums and tourist attractions, which generate a constant flow of municipal public transportation to the area.
Our study has some limitations. First, we used data collected during a specific period (March 1, 2020 to August 31, 2021) in the municipality of Petrópolis, Rio de Janeiro, Brazil. This means that the findings and conclusions of the study are applicable only to that period and geographic location, limiting their applicability to other areas or times during the pandemic. In addition, the study focuses on the use of spatial analysis methodologies and heat maps to identify areas of high concentration of cases, known as hotspots. While this provides valuable information on the spatial distribution of COVID-19 in Petrópolis, it is important to keep in mind that heat maps can be sensitive to variations of the population and event density, which may result in bias. In addition, the study is based on data provided by the Municipal Health Secretariat of Petrópolis, which raises the possibility of underreporting or biases in the data collected. Therefore, the results should be interpreted carefully and further studies are needed to corroborate and extend these findings to other geographical and temporal contexts.
In conclusion, this study identified an urban endemic focus of COVID-19 in the municipality of Petrópolis, Rio de Janeiro, Brazil, during the first 18 months of the pandemic. Using spatial analysis, we found that the highest concentration of cases remained in the same location over time, despite the dispersion of cases throughout the municipal territory. The persistence of the endemic focus over time raises questions about the control strategies used so far, as they do not seem to have been sufficient to contain the spread of the virus in this specific area.
Acknowledgments.
To the Municipal Health Secretariat of the Municipality of Petrópolis for providing the household records of the confirmed cases of COVID-19.
Funding Statement
Oswaldo Cruz Foundation
Funding.: The study was funded entirely by the Oswaldo Cruz Foundation.
Rosenberg FJ, Genial C, dos Santos BC. Urban COVID-19 endemism in Petrópolis: detection of an endemic focus by spatial analysis. Rev Peru Med Exp Salud Publica. 2023;40(2):213-9. doi: 10.17843/rpmesp.2023.402.11341.
References
- 1.Ríos Quituizaca P, Calderón L, Piedra S, Guerrero J, Narváez A. Propuesta de análisis territorial para enfrentar la pandemia por SARS-CoV-2 basado en el perfil de neumonía e influenza en Ecuador 2016-2018 [Proposal for territorial analysis to face the SARS-CoV-2 pandemic based on the Profile of pneumonia and Influenza in Ecuador 2016-2018] Aten Primaria. 2021;53(5):102021–102021. doi: 10.1016/j.aprim.2021.102021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mas JF, Pérez-Vega A. Spatiotemporal patterns of the COVID-19 epidemic in Mexico at the municipality level. PeerJ. 2021;9:e12685. doi: 10.7717/peerj.12685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Azevedo L, Pereira MJ, Ribeiro MC, Soares A. Geostatistical COVID-19 infection risk maps for Portugal. Int J Health Geogr. 2020;19(1):25–25. doi: 10.1186/s12942-020-00221-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Scarpone C, Brinkmann ST, Große T, Sonnenwald D, Fuchs M, Walker BB. A multimethod approach for county-scale geospatial analysis of emerging infectious diseases a cross-sectional case study of COVID-19 incidence in Germany. Int J Health Geogr. 2020;19(1):32–32. doi: 10.1186/s12942-020-00225-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fatima M, O'Keefe KJ, Wei W, Arshad S, Gruebner O. Geospatial Analysis of COVID-19 A Scoping Review. Int J Environ Res Public Health. 2021;18(5):2336–2336. doi: 10.3390/ijerph18052336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Franch-Pardo I, Napoletano BM, Rosete-Verges F, Billa L. Spatial analysis and GIS in the study of COVID-19 A review. Sci Total Environ. 2020;739:140033–140033. doi: 10.1016/j.scitotenv.2020.140033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Andrade LA, Gomes DS, Góes MAO, Souza MSF, Teixeira DCP, Ribeiro CJN. Surveillance of the first cases of COVID-19 in Sergipe using a prospective spatiotemporal analysis the spatial dispersion and its public health implications. Rev Soc Bras Med Trop. 2020;53:e20200287. doi: 10.1590/0037-8682-0287-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Saeed U, Sherdil K, Ashraf U, Mohey-Ud-Din G, Younas I, Butt HJ. Identification of potential lockdown areas during COVID-19 transmission in Punjab, Pakistan. Public Health. 2021;190:42–51. doi: 10.1016/j.puhe.2020.10.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pavlovsky EN. Natural Nidality of Transmissible Diseases. Urbana and London: Univ. of Illinois Press; 1964. pp. 261–261. translation 1966, edited by N. D. Levine, xiv. [Google Scholar]
- 10.Silva da LJ. O conceito de espaço na epidemiologia das doenças infecciosas. Cad Saúde Pública. 1997;13(4):585–593. doi: 10.1590/S0102-311X1997000400002. [DOI] [PubMed] [Google Scholar]
- 11.Wolfe ND, Dunavan CP, Diamond J. Origins of major human infectious diseases. Nature. 2007;447(7142):279–283. doi: 10.1038/nature05775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Roche B, Broutin H, Choisy M, Godreuil S, de Magny GC, Chevaleyre Y. The niche reduction approach an opportunity for optimal control of infectious diseases in low-income countries?. BMC Public. Health. 2014;14:753–753. doi: 10.1186/1471-2458-14-753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rosenberg FJ, Astudillo VM, Goic RM. Proc. of the 2nd Int. Symp. on Veterinary Epidemiology and Economics. Canberra: Australian Government Printing Service; 1980. Regional strategies for the control of foot and mouth disease: an ecological outlook; pp. 587–596. [Google Scholar]
- 14.Gatrell AC, Bailey TC. Interactive spatial data analysis in medical geography. Soc Sci Med. 1996;42(6):843–855. doi: 10.1016/0277-9536(95)00183-2. [DOI] [PubMed] [Google Scholar]
- 15.Câmara G, Carvalho MS. Druck S, Carvalho MS, Câmara G, Monteiro AVM. Análise Espacial de Dados Geográficos. Brasília: EMBRAPA; 2004. Análise de eventos pontuais. [Google Scholar]
- 16.Bergamaschi RB. SIG aplicado a segurança no trânsito: estudo de caso no município de Vitória - ES. Trabalho de Conclusão de Curso. Vitória: Universidade Federal do Espírito Santo; 2010. [Google Scholar]
- 17.Kawamoto MT. Análise de técnicas de distribuição espacial com padrões pontuais e aplicação a dados de acidentes de trânsito e a dados de dengue de Rio Claro-SP. Botucatu, SP: Universidade Estadual Paulista, Instituto de Biociências de Botucatu; Universidade Estadual Paulista, Instituto de Biociências de Botucatu; 2012. maestría. [Google Scholar]
- 18.Rizzatti M, Lampert Batista N, Cezar Spode PL, Bouvier Erthal D, Mauro de Faria R, Volpato Scotti AA, et al. Mapeamento da COVID-19 por meio da densidade de Kernel. 3. [13 de junio de 2023]. pp. 44–53. RMA. Disponible en: https://publicacoes.ifc.edu.br/index.php/metapre/article/view/1312 . [Google Scholar]
- 19.Bailey TC, Gatrell AC. Interactive Spatial Data Analysis. London: Longman; 1995. [DOI] [PubMed] [Google Scholar]
- 20.Menezes PML, Fernandes MC. Roteiro de Cartografia. São Paulo: Oficina de textos; 2013. [Google Scholar]
- 21.Instituto Brasileiro de Geografia e Estatística . Características da população e dos domicílios. Censo demográfico de 2010. Rio de Janeiro: IBGE; 2020. [Google Scholar]
- 22.Instituto Brasileiro de Geografia e Estatística . Petrópolis. Cidades e Estados. Rio de Janeiro: IBGE; 2022. [Google Scholar]
- 23.Aguiar M, Van-Dierdonck JB, Mar J, Cusimano N, Knopoff D, Anam V. Critical fluctuations in epidemic models explain COVID-19 post-lockdown dynamics. Sci Rep. 2021;11(1):13839–13839. doi: 10.1038/s41598-021-93366-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Randolph HE, Barreiro LB. Herd Immunity Understanding COVID-19. Immunity. 2020;52(5):737–741. doi: 10.1016/j.immuni.2020.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Oliveira GA de., Júnior Redefinição da centralidade urbana em cidades médias. Soc Nat. 2008;20(1):205–220. doi: 10.1590/S1982-45132008000100014. [DOI] [Google Scholar]