

Abstract
Objectives:
Carpal tunnel syndrome (CTS) is common among office workers and limits functional hand ability and the ability to work. Carpal tunnel syndrome prevention programs implementation are still insufficient among office workers. In view of the fact that physical activity is the best method of preventing musculoskeletal complaints the aim of the study was to evaluate the effectiveness of prevention exercises protocol for hand and wrist pain among office workers.
Material and Methods:
Study group consists form 62 office workers, reporting complaints of hand and wrist pain. Exercise group it was 49 subjects who performed the exercise protocol and the non-exercise group consisted of 13 subjects. An exercises program, consisting of 7 exercises. The program was planned for daily routine during 8 weeks. The effectiveness of the exercise program was assessed by physical parameters (hand grip and pinch grip strength, force of forearm muscles) and questionnaires (Visual Analog Scale pain scale, Carpal Tunnel Syndrome Symptom Severity Scale, and Carpal Tunnel Syndrome Functional Status Scale functional hand assessment questionnaires) were performed. Assessment was performed before and after the intervention.
Results:
Statistical analysis of the data showed significant changes in the value of measured hand grip of the right hand (Z = −2.85, p < 0.01). For pinch grip, changes were significant for both the right (Z = −2.12, p < 0.05) and the left hands (Z = −2.35, p < 0.05). Functional performance improved significantly in bought groups. There was no statistically significant change in the intensity of experienced pain.
Conclusions:
The results of the study indicate that performing a preventive exercise program regularly has an effect on increasing forearm muscle strength in a group of office workers. Office workers with symptoms of CTS who exercised regularly had higher results in hand grip and pincer grip strength. Exercises do not affect the level of pain complaints, which may indicate a more complex etiology of pain perception in this study group.
Keywords: pain, physical activity, office workers, functional ability, hand grip, carpal tunnel syndrome
INTRODUCTION
Carpal tunnel syndrome (CTS) is the most common upper limb compression neuropathy nowadays [1–3]. Thiese et al. [4] report that the prevalence of carpal tunnel ranges 6.3–11.7%, and its occurrence is already considered an epidemic. According to Pourmemari et al. [5] its incidence ranges 2.2–5.4% per 1000 people. Researchers on the topic of CTS also agree that the highest incidence of the condition is observed among occupational groups performing repetitive hands flexion and extension movements [6,7]. Among people who perform repetitive manual work, especially during activities that require repeated flexion and extension of the hands, the incidence of CTS increases up to 10% [8]. Office workers are one of the occupational groups at risk of wrist/hand symptoms especially if they are women [9] and if they are >30 years of age [10], although according to the Polish certification CTS is not defined as an occupational disease among office workers (using computers).
Carpal tunnel syndrome occurs as a result of an increase in pressure in the carpal canal, which occurs through the interaction of internal and external mechanical factors leading to a decrease in the volume of the carpal canal or an increase in the volume of the elements within it. Compression of the nerve causes paresthesia's of the palmar-radial part of the hand, pain in the area of the wrist joint and hand, and sometimes in the forearm or shoulder. As a consequence, sensory loss may occur in the first 3 fingers on the palmar side or weakness and atrophy of the muscles involved in thumb inversion and oppositions [7]. Among the various forms of therapeutic improvement for patients with mild to moderate CTS, physiotherapy is the most commonly used method. Among the treatments used are ultrasound, electrotherapy, laser therapy and magnetotherapy, as well as kinesitherapy, which involves treatment with movement [11]. According to Wilk [12], the most effective exercises are those aimed at stretching and neuromobilization of the median nerve. Few reports are available on the effectiveness of conducting therapy using exercise alone. Most of the interventions presented in the publications are aimed at people diagnosed with CTS and not prevention of people who are at risk and experiencing the first symptoms that may indicate the appearance of neuropathy in the future. The purpose of this study was to evaluate the effectiveness of prevention exercises protocol for hand and wrist pain among office workers.
MATERIAL AND METHODS
The study enrolled 65 subjects, all of whom were office workers. The exercise group consisted of 49 subjects who performed the exercise protocol min. 3 times/week, and non-exercise group consisted of 13 subjects who performed hand exercises <3 times/week. The respondents performed all their work duties normally during these 8 weeks, and there were no changes in the timing or number of duties at work. The exercise program was completed by 62 subjects (3 subjects dropped out). Table 1 presents the biometric data of the study population.
Table 1.
Biometric data of office workers reporting complaints of hand and wrist pain, tested at the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Variable | Participants (N = 62) | p | |
|---|---|---|---|
| exercise group (N = 49) | non-exercise group (N = 13) | ||
| Age [years] (M±SD) | 47.25±9.55 | 46.07±8.19 | 0.686 |
| Body mass [kg] (M±SD) | 74.34±14.87 | 67.27±15.93 | 0.138 |
| Body high [cm] (M±SD) | 169.02±7.80 | 168.67±6.29 | 0.882 |
The following inclusion criteria were used in the study: office work, the presence of CTS in the early stage of the disease diagnosed by a physician on the basis of presenting symptoms (positive at least 1 of the 4 provocative tests performed: Tinel's test, Phalen's test, reverse Phalen's test, Durkan's test), duration of symptoms (pain, numbness and tingling of the fingers of the hand, weakness of grip strength) persisting for >3 months, no contraindications to physical exercise. Exclusion criteria included: the presence of other pathological conditions in the wrists, a history of fractures of the forearm or hand, a history of an accident in the last 6 months, a diagnosis of malignant neoplasm ever in life, a diagnosis of autoimmune or other systemic disease ever in life, a diagnosis of other diseases causing symptoms characteristic of CTS (differential diagnosis).
Developed based on the available literature and the researchers' clinical experience, the set of exercises consisted of 7 exercises. Table 2 show detailed descriptions of the exercises. Participants took part in detailed, individual instruction in the exercises by a specialist (a physiotherapist) before beginning to perform the exercise program on their own, and were given a specially prepared script describing how to perform each exercise. The exercises were performed independently by the subjects. If the participant was unable to perform the recommended exercise, an individual modification was proposed, with the same effect and no difficulty in performance. They were advised to perform the exercises regularly, a minimum of 3 times a week. Participants were provided with contact with the researcher (physiotherapist) throughout the project, and were able to ask questions and voice their concerns.
Table 2.
Descriptions of the exercises for preventing musculoskeletal complaints, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Exercise | Starting position | End position/motion | Comments | Picture |
|---|---|---|---|---|
| Mobilization of the median nerve | standing position, feet set at hip width, one upper limb hangs freely along the torso, the other is visited at the shoulder joint to 90°, rotation of the head and neck in the direction opposite to the exercised upper limb, gaze directed forward (ahead) | perform alternating flexion and extension movements of the wris |
|

|
| Stretching the median nerve | standing position, feet positioned at hip width, upper limbs abducted at the shoulder joints to 90°, and the palmar side of the hands is facing the ground, gaze facing forward (in front) | make a movement of straightening your hands and lengthening your arms by spreading them out to the sides (a movement as if you want to push the walls apart) |
|
|
| Chest stretching | standing position (sideways to the wall), feet set at hip width, one upper limb hangs freely along the torso, the other is visited at the shoulder joint to a right angle and the hand rests on the wall (arm in external rotation that is, fingers pointing backwards), gaze directed forward (in front of you) | take a small step, turning your torso away from the wall while keeping your hand position unchanged |
|
|
| Stretching the flexor muscles of the hand and fingers | kneel supported, fingers abducted at the metacarpophalangeal joints, thumb and fingers flat against the floor | shift your weight forward so that your arms are as straight as possible |
|
|
| Hand extension with resistance | standing position, feet set hip-width apart, one upper limb hanging freely along the torso, the other limb bent at the elbow joint to 90°, forearm pronated, weight held in the hand | perform alternating flexion and extension movements of the hand with resistance |
|
|
| Hand flexion with resistance | standing position, feet set hip-width apart, one upper limb hanging freely along the torso, the other limb bent at the elbow joint to 90°, forearm supinated, weight held in the hand | perform alternating flexion and extension movements of the hand with resistance |
|
|
| Pronation and supination of the forearm with resistance | standing position, feet set hip-width apart, one upper limb hanging freely along the torso, the other limb bent at the elbow joint to 90°, forearm pronated, weight held in the hand | perform alternating forearm supination and pronation movements with resistance |
|
Evaluation of effectiveness the exercises protocol based on objective measurements and results of survey questionnaires, performed before and after the program. Measurement of hand grip strength and pincer grip strength (separately for the right and left sides), under static conditions, was carried out using the DR3 hand dynamometer and the DMP2 phalangeal dynamometer (JBA Zb. Staniak, Warsaw, Poland). Both measurements were performed in a standing position with the subject's arm held close to the body, the forearm was positioned parallel to the ground (angle at the elbow joint 90°), the radial-carpal joint in a neutral position (Figure 1a). When measuring pincer grip strength, the subject pressed the sensor, located on the joint between the distal and middle phalanges, of the index finger with the thumb (Figure 1b). Force measurements were always started with the healthy hand (without complaints), and the test subject generated the maximum force, twice with a pause of a few seconds between measurements, then the procedure was repeated for the other limb. The pincer grip force was then measured. The test subject was asked to hold the tension for about 3 s.
Figure 1.

Measurement position of a) hand grip strength, b) pincer grip strength, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
Photos: Patrycja Łach.
Measurements of maximum force moments in the distal joints of the upper extremities were carried out using the Biodex Multi-Joint System (Biodex Medical Systems, Inc., Shirley, NY, USA). The force tests were performed in the sitting position, the backrest angle was 85° to the seat. The torso was stabilized with 2-point belts running from the shoulder joint, to the opposite hip plate, and a pelvic belt to stabilize the upper body and avoid additional torso movements. Torque values were measured during forearm rotation and inversion (Figure 2a) and during arm flexion and extension (Figure 2b). The subject performed isometric tension 3 times, performing the reversal and inversion of the forearm and the extension and flexion of the arm as showed Figure 3.
Figure 2.

Measuring position during the measurement of muscular moments of a) supination and pronation of the forearm, and b) flexion and extension of the hand, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
Photos: Patrycja Łach.
Figure 3.
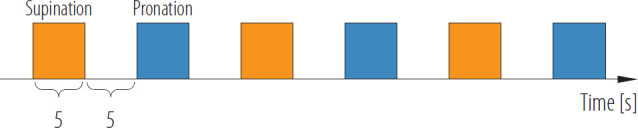
Schematic of the measurement procedure during the test of the strength of the muscles of the supination and pronation of the forearm on the Biodex Multi-Joint System, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, 2021
Photos: Patrycja Łach.
Validated survey questionnaires were also used to evaluate the effectiveness of the exercise set: Carpal Tunnel Syndrome Symptom Severity Scale (CTS SSS), Carpal Tunnel Syndrome Functional Status Scale (CTS FSS), Visual Analog Scale (VAS) pain level. The CTS SSS and CTS FSS questionnaires by Levine [13] were translated and adapted among Polish patients with CTS. In both questionnaires there are a total of 19 questions assessing the level of pain during activities of daily living, in which answers are rated on a scale of 1 (“no pain”) to 5 (“unbearable pain”). The questionnaires were completed 3 times (before, during and after the program).
Ethics
The Ethics Committee for Scientific Research Involving Human Subjects at the Institute of Human Nutrition Sciences at the Warsaw University of Life Sciences, Warsaw, Poland has approved the study (No. 34/2021, August 23, 2021).
Statistics
Statistical analysis of the collected data was conducted with the SPSS program. The normality of the distributions of the analyzed variables was checked using the Kolmogorov-Smirnov test. If the normality of the distribution was confirmed, statistical analysis of the variables was carried out using parametric tests, otherwise non-parametric tests were used. Non-parametric test for dependent variables, Wilcoxon test for pairs of observations and parametric test, Student's t-test were used. When comparing 3 dependent variables, the nonpara-metric Friedmann test or parametric test, ANOVA analysis of variance was performed. Statistical significance was set at p < 0.05.
RESULTS
Statistical analysis showed, significant differences in the value of measured grip strength of the right hand before and after the intervention in the experimental group. The mean value of force increased from 324.63 N to 338.75 N. For the left hand, the changes were not statistically significant. For pincer grip strength, the changes were significant for both the right hand and the left hand. There were no statistically significant differences in hand grip strength and pincer grip strength in the non-exercise group. Table 3 compares the initial and final measurements in the 2 study groups. There were no statistically significant difference in the value of measured grips strength before and after the intervention between both experimental groups (Table 4).
Table 3.
Hand grip strength and pincer grip strength before and after intervention in between the study groups of office workers reporting complaints of hand and wrist pain, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Variable | Measurement before the exercises | Measurement after the exercises | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| exercises group | non-exercises group | p | exercises group | non-exercises group | p | |||||
| M±SD | 95% CI | M±SD | 95% CI | M±SD | 95% CI | M±SD | 95% CI | |||
| Grip strength [N] | ||||||||||
| right hand | 324.63±111.48 | 292.61–356.66 | 370.95±102.98 | 308.72–433.19 | 0.128 | 338.75±100.86 | 309.78–367.72 | 367.75±103.51 | 305.20–430.30 | 0.426 |
| left hand | 303.04±96.94 | 275.19–330.88 | 338.94±106.63 | 274.50–403.37 | 0.316 | 311.85±94.05 | 284.84–338.86 | 342.65±125.87 | 266.58–418.71 | 0.622 |
| Pincer grip strength [N] | ||||||||||
| right hand | 76.47±22.89 | 69.90–83.05 | 81.96±19.99 | 69.88–94.04 | 0.402 | 80.59±26.62 | 72.94–88.23 | 82.62±22.93 | 68.76–96.48 | 0.628 |
| left hand | 71.86±22.89 | 65.29–78.43 | 77.04±16.38 | 67.14–86.94 | 0.299 | 76.60±23.20 | 69.94–83.27 | 76.68±23.40 | 62.55–90.82 | 0.842 |
Table 4.
Hand grip strength and pincer grip strength before and after intervention in the study groups of office workers reporting complaints of hand and wrist pain, divided into right and left sides, the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland 2021
| Parameter | Measurement | Z | p | |
|---|---|---|---|---|
| before the exercises | after the exercises | |||
| Grip strength [N] (M±SD) | ||||
| right hand | ||||
| exercises group | 324.63±111.48 | 338.75±100.86 | −2.85 | 0.004* |
| non-exercises group | 370.95±102.98 | 367.75±103.51 | −0.18 | 0.861 |
| left hand | ||||
| exercises group | 303.04±96.94 | 311.85±94.05 | −1.47 | 0.142 |
| non-exercises group | 338.94±106.63 | 342.65±125.87 | −0.25 | 0.807 |
| Pincer grip strength [N] (M±SD) | ||||
| right hand | ||||
| exercises group | 76.47±22.89 | 80.59±26.62 | −2.12 | 0.034* |
| non-exercises group | 81.96±19.99 | 82.62±22.93 | −0.38 | 0.701 |
| left hand | ||||
| exercises group | 71.86±22.89 | 76.60±23.20 | −2.38 | 0.017* |
| non-exercises group | 77.04±16.38 | 76.68±23.40 | −0.31 | 0.753 |
p < 0.05.
In the experimental group, the values of maximum muscle force moments showed statistically significant differences during right and left forearm pronation and right and left hand straightening and flexion. In the non-exercise group, the values of maximum moments of forces in the forearm and radial-carpal joints on the right and left sides showed no statistically significant differences. Table 5 presents the detailed results of the performed measurements of the maximum moments of muscle forces.
Table 5.
Maximum moments of muscle forces in the distal joints of the upper limbs among the office workers reporting complaints of hand and wrist pain, tested at the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Parameter | Measurement | Z | p | |
|---|---|---|---|---|
| before the exercises | after the exercises | |||
| Supination [Nm] (M±SD) | ||||
| right forearm | ||||
| exercises group | 3.78±2.32 | 4.03±2.56 | −1.23 | 0.220 |
| non-exercises group | 4.18±2.27 | 4.60±2.36 | −0.52 | 0.600 |
| left forearm | ||||
| exercises group | 3.06±2.13 | 3.33±2.41 | −0.98 | 0.327 |
| non-exercises group | 3.34±2.43 | 3.06±2.85 | −0.67 | 0.505 |
| Pronation [Nm] (M±SD) | ||||
| right forearm | ||||
| exercises group | 5.26±2.37 | 6.13±2.70 | −3.48 | 0.001* |
| non-exercises group | 6.11 ±2.65 | 6.38±2.28 | −1.01 | 0.311 |
| left forearm | ||||
| exercises group | 5.11 ±2.18 | 6.26±2.57 | −4.42 | 0.001* |
| non-exercises group | 5.61 ±1.79 | 5.97±2.01 | −0.94 | 0.345 |
| Extension [Nm] (M±SD) | ||||
| right hand | ||||
| exercises group | 6.09±2.90 | 7.09±2.94 | −3.14 | 0.002* |
| non-exercises group | 8.02±3.69 | 8.03±2.59 | −0.59 | 0.552 |
| left hand | ||||
| exercises group | 5.86±2.65 | 6.49±2.59 | −2.31 | 0.021* |
| non-exercises group | 6.99±3.17 | 7.02±3.33 | 0.00 | 1.00 |
| Flexion [Nm] (M±SD) | ||||
| right hand | ||||
| exercises group | 10.84±4.44 | 12.92±4.92 | −4.07 | 0.001* |
| non-exercises group | 13.60±4.97 | 13.40±4.97 | −0.35 | 0.727 |
| left hand | ||||
| exercises group | 11.04±4.77 | 12.83±5.05 | −3.93 | 0.001* |
| non-exercises group | 14.95±5.99 | 13.71±6.06 | −1.64 | 0.101 |
p < 0.05.
The average pain score marked on the VAS, decreased from 53 pts to 39 pts, the change was not statistically significant. The results of pain levels in both study groups over the past 7 days are shown in Table 6.
Table 6.
The level of pain experienced in the last 7 days by the office workers reporting complaints of hand and wrist pain, tested at the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Study group | Pain level (M±SD) | t | p | |
|---|---|---|---|---|
| measurement before the exercises | measurement after the exercises | |||
| Exercises group (N = 49) | 49.36±19.73 | 48.48±17.33 | 0.22 | 0.830 |
| Non-exercises group (N = 13) | 53.00±8.87 | 38.75±25.62 | 1.70 | 0.188 |
Subjects in the experimental group rated the functional status of their hand better than those in the non-exercise group, a statistically significant difference. In contrast, lower symptom severity in the second and third measurements than before the exercise program was declared by subjects in both groups, with the change being higher in the experimental group. Table 7 shows the results of measurements of the functional status of the hand and the severity of symptoms in both study groups.
Table 7.
Results of functional status assessment of the hand and severity of carpal tunnel syndrome (CTS) complaints among the office workers reporting complaints of hand and wrist pain, tested at the Biomechanics Laboratory of Central Institute for Labor Protection – National Research Institute, Warsaw, Poland, 2021
| Variable | Measurement | X2 | p | ||
|---|---|---|---|---|---|
| first | second | third | |||
| Hand functional status (M±SD) | |||||
| exercises group | 1.84±0.74 | 1.65±0.80 | 1.64±0.80 | 9.68 | 0.008* |
| non-exercises group | 1.74±0.96 | 1.57±0.51 | 1.42±0.58 | 5.10 | 0.078 |
| Seventy of CTS complaints (M±SD) | |||||
| exercises group | 2.13±0.69 | 1.85±0.80 | 1.79±0.75 | 26.68 | 0.001* |
| non-exercises group | 1.73±0.55 | 1.73±0.54 | 1.48±0.47 | 13.15 | 0.001* |
p < 0.05.
DISCUSSION
Results of the study confirmed that developed program of exercises is effective in prevention for hand and wrist pain among office workers with symptoms of CTS. Improvements were shown in both muscle strength and grip tests, as well as in the subjects' functional status.
To evaluate the effectiveness of the exercise program, tools commonly used in the diagnosis of median nerve compression neuropathy were used [14]. An analysis of pain levels was included, using subjective assessment on VAS [15]. Respondents assessed the level of pain they experienced in the 7 days preceding the survey. In addition, the Boston Carpal Tunnel Questionnaire was completed as a basis for assessing functional capacity, when evaluating changes due to therapy or progression of ailments [16]. Functional assessment using the above questionnaire, was performed 3 times before, during and after the 2-month exercise program. Hand grip strength and pincer grip strength measurements were used as an objective tool [17]. In addition, measurements of the maximum force moments in the upper limb joints and the range of motion of the hand joints were carried out using the Biodex Multi-Joint System. Muscle force moments were measured under isometric conditions.
The study reports that grip strength decreases in patients diagnosed with CTS compared to those without neuropathy. The median nerve innervates the flexor muscles of the fingers and wrist, passing through the carpal tunnel. It is responsible for the motor innervation of the muscles and the sensation of the first 3 fingers, which is what makes it possible to perform a proper hand grip and pincer grasp with the fingers [18–21].
All of the subjects had office jobs, in which they perform manual activities in a sitting position. Occupational risk factors influence the occurrence of upper extremity complaints, according to the study. Problems with compression neuropathy are more common in occupational groups exposed to repetitive flexion and extension movements of the hand [6,18], which occurs with inadequate, or prolonged use of computer equipment. In the study group, 79% of people spend >6 h at work in a sitting position. When using a keyboard and mouse, as many as 48.4% of respondents keep their hands in a position where the hands are below or above the forearms, resulting in excessive palmar or dorsal flexion. Prolonged mouse handling may be a factor in increasing the risk of upper extremity musculoskeletal disorders [9,22,23]. Studies show that physical activity has a preventive effect and reduces the risk of musculoskeletal complaints [24]. Studies show that regular exercise has a measurable effect in terms of improving muscle strength and improving the functional ability of the hands, despite the lack of significant differences in pain levels. This indicates that physical activity should be one of the main methods of counteracting pain associated with office work. On the other hand, physical exercise alone for advanced conditions and worsening complaints in diagnosed carpal tunnel may not be sufficient.
The topic of prevention of hand and wrist pain is often addressed due to the fact that CTS is the most common compression neuropathy of the upper limb [1,5]. Meta-analyses of the effectiveness of using different therapeutic strategies are inconclusive. Most studies tend to conclude that the most promising results are obtained when interventions are mixed and implemented at different levels [25,26]. A multifactorial intervention including exercise, massage, education and ergonomic guidelines appears to be the best workplace strategy of preventing musculoskeletal disorders [27]. In addition, the important impact of working with a therapist is often emphasized by researchers. Stand-alone exercises may not be as effective as working with a therapist. For a condition as specific as compression neuropathy, exercise alone may not be effective. Despite the fact that mobilization and stretching exercises have been proven to help improve the mobility of the median nerve, thus improving the transmission of nerve impulses, and the use of so-called gliding exercises leads to the stretching of soft tissue adhesions in the carpal tunnel, their effectiveness compared to working with a physiotherapist combined with manual therapy has less significant effects [28]. In contrast, for those with mild to moderate symptoms of CTS, it appears that the use of stretching exercises to mobilize upper limb structures may be a simple and effective method used as a preventive measure for those at risk of developing compression neuropathy [29,30].
Value and limitations of the study
One of the strengths of the study was develop the effective home and easy to do program of exercises for prevention CTS in early stage symptoms. Moreover the gained improvement in symptoms was a long-term effects what was assessed in follow up by functional status assessment of the hand and severity of CTS complaints. It is also worthy to highlight that prior to the start of the exercise program, exercise instruction by a professional (physiotherapist) was provided to ensure that the exercises were performed correctly. However, some limitations should be considered; First, the study groups was not equal. Second, there were no a priori sample size calculation perform before the study because lack of input data for estimation. Third, there weren't control variables for control the dependent variable, there were only, apart from recommending to keep a current lifestyle in both cases.
However, the mentioned limitations do not detract from the value of the presented publication.
CONCLUSIONS
-
–
The results of the study indicate that performing a preventive exercise program regularly, min. 3 times/week, has an effect on increasing forearm muscle strength in a group of office workers.
-
–
Office workers with symptoms of CTS who exercised regularly had higher results in squeeze strength and pincer grip strength.
-
–
Exercises performed for 2 months improve functional status, while they do not affect the level of pain complaints, which may indicate a more complex etiology of pain perception in this study group.
Footnotes
Funding: this research was supported by the National Centre for Research and Development (project No. I.PB.05 entitled “Development of an exercise program in overload syndromes of the musculoskeletal system of employees using VR techniques,” project manager: Patrycja Łach).
Author contributions
Research concept: Patrycja Łach, Anna Katarzyna Cygańska
Research methodology: Patrycja Łach, Anna Katarzyna Cygańska
Collecting material: Patrycja Łach, Anna Katarzyna Cygańska
Statistical analysis: Patrycja Łach, Anna Katarzyna Cygańska
Interpretation of results: Patrycja Łach, Anna Katarzyna Cygańska
References: Patrycja Łach, Anna Katarzyna Cygańska
REFERENCES
- 1.Ghasemi-Rad M, Nosair E, Vegh A, Mohammadi A, Akkad A, Lesha E, et al. A handy review of carpal tunnel syndrome: From anatomy to diagnosis and treatment. World J Radiol. 2014;6(6):284. 10.4329/WJR.V6.I6.284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Aroori S, Spence RAJ, Carpal tunnel syndrome. Ulster Med J. 2008;77(1):6–17. [PMC free article] [PubMed] [Google Scholar]
- 3.Abicalaf CA, de Barros N, Sernik RA, Pimentel BF, Braga-Baiak A, Braga L, et al. Ultrasound evaluation of patients with carpal tunnel syndrome before and after endoscopic release of the transverse carpal ligament. Clin Radiol. 2007; 62(9): 891–4. 10.1016/J.CRAD.2007.01.029. [DOI] [PubMed] [Google Scholar]
- 4.Thiese MS, Hegmann KT, Wood EM, Garg A, Moore JS, Kapellusch J, et al. Prevalence of low back pain by anatomic location and intensity in an occupational population. BMC Musculoskeletal Disord. 2014;15(1):1–11. 10.1186/1471-2474-15-283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pourmemari MH, Heliövaara M, Viikari-Juntura E, Shiri R. Carpal tunnel release: Lifetime prevalence, annual incidence, and risk factors. Muscle Nerve. 2018;58(4):497–502, 10.1002/MUS.26145. [DOI] [PubMed] [Google Scholar]
- 6.Jackson R, Beckman J, Frederick M, Musolin K, Harrison R. Rates of Carpal Tunnel Syndrome in a State Workers' Compensation Information System, by Industry and Occupation – California, 2007–2014. MMWR Morb Mortal Wkly Rep. 2018; 67(39): 1094-7. 10.15585/MMWR.MM6739A4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Makowiec-Dąbrowska T, Sińczuk-Walczak H, Jóźwiak ZW, Krawczyk-Adamus P. [Work performance as a risk factor for carpal tunnel syndrome.] Med Pr. 2007;58(4):361–72. Polish. [PubMed] [Google Scholar]
- 8.Biernawska J, Niemczyk A, Pierzchała K. [Contribution of occupational and non-occupational factors in the pathogenesis of carpal tunnel syndrome.] Med Pr. 2005;56(2): 131–137. Polish. [PubMed] [Google Scholar]
- 9.Feng B, Chen K, Zhu X, Ip WY, Andersen LL, Page P, et al. Prevalence and risk factors of self-reported wrist and hand symptoms and clinically confirmed carpal tunnel syndrome among office workers in China: a cross-sectional study. BMC Public Health. 2021;21(1):1–10. 10.1186/S12889-020-10137-1/TABLES/4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Joshi A, Patel K, Mohamed A, Oak S, Zhang MH, Hsiung H, et al. Carpal tunnel syndrome: pathophysiology and comprehensive guidelines for clinical evaluation and treatment. Cureus. 2022;14(7):e27053. 10.7759/CUREUS.27053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Golabek R, Majcher P. Carpal tunnel syndrome. Sport i Turystyka. Środkowoeur Czas Nauk. 2018;1(1):123–40. 10.16926/sit.2018.01.09.Polish. [DOI] [Google Scholar]
- 12.Wilk I. The effectiveness of therapeutic massage in carpal tunnel syndrome. Puls Uczelni. 2015;(1):21–3. 10.5604/01.3001.0003.3186. [DOI] [Google Scholar]
- 13.Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH, et al. A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993; 75(11): 1585-92. 10.2106/00004623-199311000-00002. [DOI] [PubMed] [Google Scholar]
- 14.Erickson M, Lawrence M, Jansen CWS, Coker D, Amadio P, Cleary C. and pain and sensory deficits: Carpal tunnel syndrome: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of hand and upper extremity physical therapy and the academy of orthopaedic physical therapy of the American physical therapy association. J Orthop Sports Phys Ther. 2019;49(5):CPG1–85. 10.2519/JOSPT.2019.0301. [DOI] [PubMed] [Google Scholar]
- 15.Sheereen FJ, Sarkar B, Sahay P, Shaphe MA, Alghadir AH, Iqbal A, et al. Comparison of Two Manual Therapy Programs, including Tendon Gliding Exercises as a Common Adjunct, While Managing the Participants with Chronic Carpal Tunnel Syndrome. Pain Res Manag. 2022;2022: 1975803. 10.1155/2022/1975803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.İlhan D, Toker S, Kilincioğlu V, Gülcan E. Assessment of the Boston questionnaire in diagnosis of idiopathic carpal tunnel syndrome: Comparing scores with clinical and neurophysiological findings. Duzce Med J. 2008;10(3):4–9. [Google Scholar]
- 17.Ha YC, Hwang SC, Song SY, Lee CH, Park KS, Yoo JIl. Hand grip strength measurement in different epidemiologic studies using various methods for diagnosis of sarcopenia: a systematic review. Eur Geriatr Med. 2018;9(3):277–88. 10.1007/S41999-018-0050-6. [DOI] [PubMed] [Google Scholar]
- 18.Lee SH, Gong HS. Grip Strength Measurement for Outcome Assessment in Common Hand Surgeries. Clin Orthop Surg. 2022; 14(1):1–12. 10.4055/CIOS21090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mathiowetz V, Weber K, Volland G, Kashman N. Reliability and validity of grip and pinch strength evaluations. J Hand Surg Am. 1984;9(2):222–6. 10.1016/S0363-5023(84)80146-X. [DOI] [PubMed] [Google Scholar]
- 20.Kozin SH, Porter S, Clark P, Thoder JJ. The contribution of the intrinsic muscles to grip and pinch strength. J Hand Surg Am. 1999;24(1): 64-72. 10.1053/JHSU.1999.JHSU24A0064. [DOI] [PubMed] [Google Scholar]
- 21.Peolsson A, Hedlund R, Oberg B. Intra- and inter-tester reliability and reference values for hand strength. J Rehabil Med. 2001;33(1):36–41. 10.1080/165019701300006524. [DOI] [PubMed] [Google Scholar]
- 22.Keir PJ, Farias Zuniga A, Mulla DM, Somasundram KG. Relationships and Mechanisms Between Occupational Risk Factors and Distal Upper Extremity Disorders. Hum Factors. 2021;63(1):5–31. 10.1177/0018720819860683. [DOI] [PubMed] [Google Scholar]
- 23.Lund CB, Mikkelsen S, Thygesen LC, Hansson GÅ, Thomsen JF. Movements of the wrist and the risk of carpal tunnel syndrome: a nationwide cohort study using objective exposure measurements. Occup Environ Med. 2019;76(8): 519-26. 10.1136/OEMED-2018-105619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Al Shahrani E, Al Shahrani A, Al-Maflehi N. Personal factors associated with carpal tunnel syndrome (CTS): a casecontrol study. BMC Musculoskeletal Disord. 2021;22(1):1–7. 10.1186/S12891-021-04941-Y/TABLES/3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Trillos-Chacón MC, Castillo-M JA, Tolosa-Guzman I, Sánchez Medina AF, Ballesteros SM. Strategies for the prevention of carpal tunnel syndrome in the workplace: A systematic review. Appl Ergon. 2021;93:103353. 10.1016/J.APERGO.2020.103353. [DOI] [PubMed] [Google Scholar]
- 26.Jiménez-del-Barrio S, Cadellans-Arróniz A, Ceballos-Laita L, Estébanez-de-Miguel E, López-de-Celis C, Bueno-Gracia E, et al. The effectiveness of manual therapy on pain, physical function, and nerve conduction studies in carpal tunnel syndrome patients: a systematic review and meta-analysis. Int Orthop. 2022;46(2):301. 10.1007/S00264-021-05272-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Da Silva NC, Ricci FPFM, de Castro VR, de Lima ACR, do Carmo Lopes ER, de Salvo Mauad LD, et al. Effects of workplace upper extremity resistance exercises on function and symptoms of workers at a tertiary hospital: a randomized controlled trial protocol. BMC Musculoskeletal Disord. 2022; 23(1):1–8. 10.1186/S12891-022-05059-5/FIGURES/2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Shem K, Wong J, Dirlikov B. Effective self-stretching of carpal ligament for the treatment of carpal tunnel syndrome: A double-blinded randomized controlled study. J Hand Ther. 2020;33(3):272–80. 10.1016/J.JHT.2019.12.002. [DOI] [PubMed] [Google Scholar]
- 29.Keskin Y, Kilic G, Taspinar O, Posul SO, Halac G, Eren F, et al. Effectiveness of home exercise in pregnant women with carpal tunnel syndrome: Randomized Control Trial. J Pak Med Assoc. 2020;70(2):202–7. 10.5455/JPMA.1846. [DOI] [PubMed] [Google Scholar]
- 30.de Arenas-Arroyo SN, Cavero-Redondo I, Torres-Costoso A, Reina-Gutiérrez S, Álvarez-Bueno C, Martínez-Vizcaíno V. Short-term Effects of Neurodynamic Techniques for Treating Carpal Tunnel Syndrome: A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2021;51(12): 566-80. 10.2519/JOSPT.2021.10533. [DOI] [PubMed] [Google Scholar]