

Abstract
Induction regimens for multiple myeloma (MM) commonly include bortezomib, which has typically been administered twice weekly despite studies demonstrating comparable efficacy and less peripheral neuropathy (PN) with once-weekly bortezomib. We aimed to analyze the real-world prevalence and efficacy of once-weekly versus twice-weekly bortezomib regimens in newly diagnosed MM. We analyzed 2497 US patients aged 18–70 years treated with commercial first-line bortezomib using nationwide Flatiron Health electronic health record-derived data, including 910 (36.4%) patients who received twice-weekly and 1522 (63.2%) who received once-weekly bortezomib. Once-weekly bortezomib use increased over time, from 57.7% in 2017 to 73.1% in 2022. Multivariate analysis identified worsened performance status and more recent year of diagnosis with higher odds of receiving once-weekly bortezomib. Real-world progression-free survival (median 37.2 months with once-weekly versus 39.6 months with twice-weekly, p = 0.906) and overall survival (medians not reached in either cohort, p = 0.800) were comparable. PN rates were higher in patients receiving twice-weekly bortezomib (34.7% versus 18.5%, p < 0.001). In conclusion, once-weekly bortezomib is clearly associated with similar efficacy and fewer toxicities compared to twice-weekly bortezomib. Our findings support once-weekly bortezomib as a standard-of-care regimen for newly diagnosed patients with MM.
Subject terms: Myeloma, Epidemiology
Introduction
Multiple myeloma (MM) is a hematologic malignancy of post-germinal plasma cells [1, 2]. Outcomes in MM have drastically improved over the past two decades with the incorporation of new classes and combinations of drugs [3, 4]. Induction regimens for MM commonly include the selective 26S proteasome inhibitor bortezomib, which has typically been administered twice per week in 21-day or 28-day cycles. However, bortezomib-related peripheral neuropathy (PN) can impact quality of life and may occur more commonly in Black patients and other vulnerable populations [3, 5, 6]. Based on early studies suggesting comparable outcomes with less frequent dosing of bortezomib [7, 8], later retrospective single-center studies as well as a large systematic review have shown that once-weekly bortezomib has comparable efficacy with less PN as compared to twice-weekly bortezomib [9–11]. These findings have also been confirmed in several secondary analyses of prospective phase 3 data evaluating bortezomib-based regimens in transplant-ineligible MM patients [8, 12–14]. In addition, pharmacokinetic prediction models confirm that once-weekly bortezomib dosing constitutes an optimal therapeutic regimen with comparable antineoplastic activity but significantly reduced risk of thrombocytopenia [15].
Outside of clinical scenarios requiring swift disease control, once-weekly bortezomib has been widely adopted in real-world clinical practice. Nonetheless, most clinical trial protocols continue to dose bortezomib on a twice-weekly schedule. Previous analyses evaluating once-weekly bortezomib prescribing patterns are limited by their single-center design and use of historical data largely preceding 2018 [9, 10]. Consequently, our goal was to assess the prevalence, effectiveness, and toxicities of once-weekly versus twice-weekly bortezomib dosing regimens in a broader and more contemporary cohort of patients newly diagnosed with multiple myeloma.
Methods
Data source
This retrospective observational study used data from the US nationwide Flatiron Health electronic health record (EHR)-derived de-identified longitudinal database. The Flatiron Health database contains structured and unstructured data curated via technology-enabled abstraction from approximately 280 cancer clinics and 800 unique sites of care [16, 17]. Patients were included in our analysis if they had newly diagnosed MM (ICD-9 203.0x or ICD-10 C90.0x, confirmed with clinical review), were aged 18–70 years at diagnosis, had at least two EHR-documented clinic visits, and at least six months of follow-up before June 30, 2023 (data cut-off). Although the Flatiron Health database includes patients diagnosed since 2011, we only analyzed patients diagnosed on or after January 1, 2017, to focus on a more modern cohort. Given the prevalence of “VRd-lite” regimens (i.e., modified dosing of lenalidomide, bortezomib and dexamethasone) employing once-weekly bortezomib for older or frailer patients, we excluded patients a priori who were aged >70 years at diagnosis [18, 19]. All patients had documented treatment with bortezomib during their first line (1L) of treatment. Patients who received bortezomib as part of a clinical trial were excluded. This retrospective study was reviewed and exempted by the University of Texas Southwestern Institutional Review Board.
Exposure and covariate definitions
Twice-weekly bortezomib was defined as patients for whom the most frequent interval between two doses of 1L bortezomib within a cycle was 3.0-4.9 days. Once-weekly bortezomib was defined as a corresponding interval of 5.0–9.9 days. The frequency of patients who started with one prescribing pattern and switched to the other pattern was noted; however, these patients were excluded from subsequent analyses. Key covariates included age at diagnosis, gender, race/ethnicity (non-Latinx White, non-Latinx Black, Hispanic/Latinx, non-Latinx Asian, other and unknown), practice type (academic, community, both), insurance status, Eastern Cooperative Oncology Group (ECOG) performance status (PS) at 1L initiation (0, 1, ≥2, unknown), ISS stage (I, II, III, unknown/not documented) [20], year of diagnosis, serum creatinine at treatment initiation ( ≤ 1.2 mg/dL, 1.3–2.9 mg/dL, ≥3 mg/dL, and unknown), hemoglobin (g/dL) level at treatment initiation, number of high-risk cytogenetic abnormalities (HRCA) tested any time prior to or within days of 1 L initiation (HRCA 0, 1, ≥2), and route of first dose of bortezomib (subcutaneous versus intravenous). HRCA included gain(1q)/amp(1q), t(4;14), t(14;16), t(14;20), and del(17p) [21, 22]. Insurance status was categorized hierarchically as Medicaid, Medicare, Commercial Health Plan, other, or unknown/uninsured; for patients aged ≥65 years at diagnosis with missing insurance status, insurance was assumed to be Medicare.
Concurrent anti-MM treatments alongside bortezomib were defined as follows: bortezomib only, cyclophosphamide-bortezomib-dexamethasone (CyBorD), daratumumab-bortezomib-dexamethasone (D-Vd), daratumumab-bortezomib-lenalidomide-dexamethasone (D-VRd), bortezomib-dexamethasone (Vd), bortezomib-lenalidomide-dexamethasone (VRd), and other. Neuropathy during 1L treatment was defined as the presence of at least one of the following: billing codes for drug-induced neuropathy (ICD-9 357.6, ICD-10 G62.2), billing codes for other neuropathies (ICD-9: 356.9, 357.4, 357.7; ICD-10: G62.9), and initiation of medications typically reserved for neuropathy (gabapentin, pregabalin, and/or duloxetine).
Endpoints and statistical analysis
Real-world overall survival (rwOS) was defined as the time from start of first treatment (index date) to the date of death or last confirmed activity before the data cut-off [23, 24]. Real-world progression free survival (rwPFS) was defined as time from start of first treatment to the first derived date of progressive disease, death, or last confirmed activity before the data cut-off. Disease progression status was derived using International Myeloma Working Group (IMWG) criteria [25] using the results of serum protein electrophoresis (SPEP) testing (abstracted from unstructured health record information if value ≥1.0 g/dL at baseline), 24-h urine protein electrophoresis (UPEP) testing (abstracted from unstructured health record notes if value ≥200 mg per 24 h at baseline), and serum free light chain (FLC) testing (abstracted from structured laboratory information). Patients with no documented progression or death were censored at the date of the last test of the assigned biomarker type.
Descriptive statistics were used to describe demographic, clinical, disease, and treatment characteristics. Continuous variables were reported as means, medians, and interquartile ranges (IQRs). Categorical variables were reported as number (n) and percent (%) of eligible patients. We used multivariate logistic regression to assess demographic and clinical factors associated with once-weekly versus twice-weekly (reference) bortezomib. Estimated adjusted odds ratios (OR) and corresponding 95% confidence intervals (CI) were summarized. The Kaplan-Meier method was used to estimate rwOS and rwPFS. Outcomes were compared using Cox proportional hazards (PH) models including stem cell transplant as a time-varying covariate and adjustment for other demographic and clinical factors. Adjusted hazard ratio (HR) and corresponding 95% CI of once-weekly bortezomib, as compared to twice-weekly bortezomib, were summarized for each outcome. The PH assumption of the bortezomib prescribing pattern coefficient was tested using a score test in the multivariate model with time-varying transplant variable. All statistical analyses were performed using R version 4.1.3.
Results
As shown in Fig. 1, we included 2520 patients diagnosed with MM between 2017 and 2022 who received 1L bortezomib. Twenty-three patients (0.9%) were excluded due to changing bortezomib frequencies during 1L, leaving 2497 (99.1%) evaluable patients. Of these 2497 patients, 910 (36.4%) received twice-weekly bortezomib and 1587 (63.6%) received once-weekly bortezomib. Patients had a median age at diagnosis of 62 years (IQR: 56–67 years) and 44.6% of the patients were female. Approximately half of patients (49.7%) were non-Latinx White, 22.1% were non-Latinx Black, and 8.5% were Latinx. Most patients were treated in the community setting (77.1%) (Table 1).
Fig. 1. Flow chart of analyzed patients.
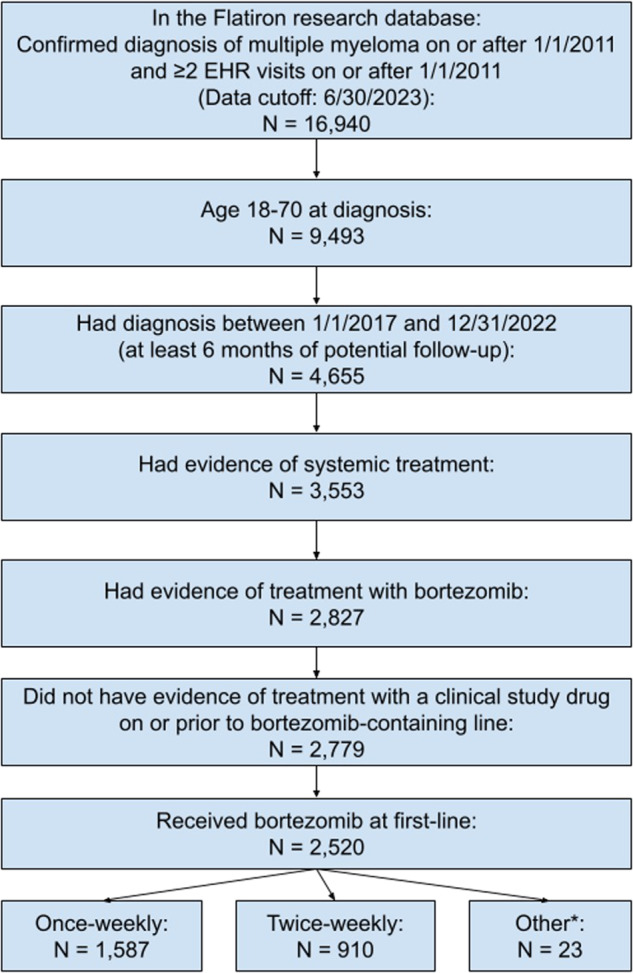
Abbreviations: EHR, Electronic Health Record. * Other: Patients whose bortezomib dosing frequency changed during induction.
Table 1.
Baseline characteristics between twice-weekly and once-weekly bortezomib.
| ALL | Twice-weekly | Once-weekly | p-value | |
|---|---|---|---|---|
| N = 2497 | N = 910 | N = 1587 | ||
| Age at index | 62.0 [56.0;67.0] | 62.0 [57.0;67.0] | 62.0 [56.0;67.0] | 0.774 |
| Gender | 0.478 | |||
| Male | 1383 (55.4%) | 513 (56.4%) | 870 (54.8%) | |
| Female | 1114 (44.6%) | 397 (43.6%) | 717 (45.2%) | |
| Race/ethnicity | <0.001 | |||
| Non-Latinx White | 1242 (49.7%) | 467 (51.3%) | 775 (48.8%) | |
| Non-Latinx Black | 552 (22.1%) | 208 (22.9%) | 344 (21.7%) | |
| Hispanic or Latinx | 212 (8.5%) | 102 (11.2%) | 110 (6.9%) | |
| Non-Latinx Asian | 58 (2.3%) | 14 (1.5%) | 44 (2.8%) | |
| Other | 117 (7.1%) | 52 (5.7%) | 125 (7.9%) | |
| Unknown | 256 (10.3%) | 67 (7.4%) | 189 (11.9%) | |
| Practice type | 0.040 | |||
| Community | 1925 (77.1%) | 723 (79.5%) | 1202 (75.7%) | |
| Academic | 451 (18.1%) | 154 (16.9%) | 297 (18.7%) | |
| Both | 121 (4.8%) | 33 (3.6%) | 88 (5.5%) | |
| Year of diagnosis | 2019 [2018;2021] | 2019 [2018;2021] | 2020 [2018;2021] | <0.001 |
| ECOG PS at 1L | 0.016 | |||
| 0 | 839 (33.6%) | 334 (36.7%) | 505 (31.8%) | |
| 1 | 782 (31.3%) | 288 (31.6%) | 494 (31.1%) | |
| ≥2 | 344 (13.8%) | 105 (11.5%) | 239 (15.1%) | |
| Unknown | 532 (21.3%) | 183 (20.1%) | 349 (22.0%) | |
| ISS stage | 0.180 | |||
| Stage I | 685 (27.4%) | 265 (29.1%) | 420 (26.5%) | |
| Stage II | 516 (20.7%) | 181 (19.9%) | 335 (21.1%) | |
| Stage II | 533 (21.3%) | 205 (22.5%) | 328 (20.7%) | |
| Unknown | 763 (30.6%) | 259 (28.5%) | 504 (31.8%) | |
| Insurance status at 1L | 0.905 | |||
| Commercial Health Plan | 778 (31.2%) | 276 (30.3%) | 502 (31.6%) | |
| Medicare | 798 (32.0%) | 300 (33.0%) | 498 (31.4%0 | |
| Medicaid | 191 (7.6%) | 67 (7.4%) | 124 (7.8%) | |
| Other payer | 219 (8.8%) | 82 (9.0%) | 137 (8.6%) | |
| Unknown/ uninsured | 511 (20.5%) | 185 (20.3%) | 326 (20.5%) | |
| Number of HRCA | 0.266 | |||
| 0 | 1733 (69.4%) | 619 (68.0%) | 1114 (70.2%) | |
| 1 | 564 (22.6%) | 208 (22.9%) | 356 (22.4%) | |
| ≥2 | 200 (8.0%) | 83 (9.1%) | 117 (7.4%) | |
| Serum creatinine level at 1L | 0.802 | |||
| ≤1.2 mg/dL | 1216 (48.7%) | 434 (47.7%) | 782 (49.3%) | |
| 1.3–2.9 mg/dL | 494 (19.8%) | 183 (20.1%) | 311 (19.6%) | |
| ≥3 mg/dL | 202 (8.1%) | 79 (8.7%) | 123 (7.8%) | |
| Unknown | 585 (23.4%) | 214 (23.5%) | 371 (23.4%) | |
| Hemoglobin level (g/dL) | 10.7 [9.1;12.3] | 10.6 [9.0;12.3] | 10.7 [9.2; 12.3] | 0.385 |
| Concurrent therapy at 1L | ||||
| Bortezomib only | 27 (1.1%) | 9 (1.0%) | 18 (1.1%) | |
| CyBorD | 305 (12.2%) | 74 (8.1%) | 231 (14.6%) | |
| D-Vd | 41 (1.6%) | 8 (0.9%) | 33 (2.1%) | |
| D-VRd | 276 (11.1%) | 83 (9.1%) | 193 (12.2%) | |
| Other | 5 (0.2%) | < 5 | < 5 | |
| Vd | 130 (5.2%) | 54 (5.9%) | 76 (4.8%) | |
| VRd | 1713 (68.6%) | 681 (74.8%) | 1032 (65.0%) | |
| Bortezomib starting routes at 1L | <0.001 | |||
| Subcutaneous | 2368 (94.9%) | 841 (92.4%) | 1527 (96.3%) | |
| Intravenous | 128 (5.1%) | 69 (7.6%) | 59 (3.7%) | |
| Any neuropathy diagnosis or medication for severe neuropathy | 610 (24.4%) | 316 (34.7%) | 294 (18.5%) | <0.001 |
| Drug-induced neuropathy diagnosis | 134 (5.4%) | 87 (9.6%) | 47 (3.0%) | <0.001 |
| Other neuropathy diagnosis | 141 (5.6%) | 78 (8.6%) | 63 (4.0%) | <0.001 |
| Medication for severe neuropathy | 506 (20.3%) | 272 (29.9%) | 234 (14.7%) | <0.001 |
ECOG Eastern Cooperative Oncology Group, PS performance status, HRCA high-risk cytogenetic abnormality, CyBorD cyclophosphamide-bortezomib-dexamethasone, D-Vd daratumumab-bortezomib-dexamethasone, D-VRd daratumumab-bortezomib-lenalidomide-dexamethasone, Vd: bortezomib-dexamethasone, VRd bortezomib-lenalidomide-dexamethasone.
Compared to patients with twice-weekly bortezomib, patients who received once-weekly bortezomib were less likely to be Hispanic/Latinx (6.9% versus 11.2%, p < 0.001). Conversely, they were more likely to be treated at academic practices (18.7% versus 16.9%, p = 0.040), have ECOG PS ≥ 2 (15.1% versus 11.5%, p = 0.016), and to have started bortezomib subcutaneously (96.3% versus 92.4%, p < 0.001) (Table 1). Other demographic and clinical characteristics were similar between the two groups, including age, gender, ISS stage, hemoglobin, number of HRCAs and concurrent therapies. The frequency of once-weekly bortezomib use did increase over time, from 57.7% in 2017 to 73.1% in 2022. In addition, we observed a step up in once-weekly dosing frequency between 2017–2019 (57.5% of eligible patients) versus 2020-2022 (69.9% of eligible patients (Fig. 2).
Fig. 2.

Proportion of patients treated with once-weekly bortezomib.
In multivariate logistic regression analysis, ECOG PS ≥ 2 (OR 1.57 [95% CI 1.19-2.08] versus ECOG PS 0), and more recent year of diagnosis (OR 1.18 [95% CI 1.12–1.24] per year) were associated with higher odds of receiving once-weekly bortezomib (Table 2). A trend was found between twice-weekly bortezomib and ≥2 HRCA at 1L (OR 0.74 [0.54-1.00] versus 0 HRCA). Conversely, once-weekly bortezomib administration was less common among Hispanic/Latinx patients compared to non-Latinx White (OR 0.65 [95% CI 0.48–0.89]) and among patients dosed intravenously rather than subcutaneously (OR 0.44 [95% CI 0.30–0.65]) had lower odds of receiving once-weekly bortezomib administration. No significant associations were found between gender, ISS stage, practice setting, insurance category, or baseline creatinine.
Table 2.
Predictors of once-weekly bortezomib dosing.
| Characteristic | ORa | 95% CIa | p-value |
|---|---|---|---|
| Age at diagnosis | 1.00 | 0.99, 1.01 | 0.817 |
| Gender | |||
| Male | – | – | |
| Female | 1.07 | 1.27 | 0.443 |
| Race/ ethnicity | |||
| Non-Latinx White | – | – | |
| Non-Latinx Black | 0.95 | 0.76, 1.17 | 0.607 |
| Hispanic or Latinx | 0.65 | 0.48, 0.89 | 0.007 |
| Non-Latinx Asian | 1.98 | 1.08, 3.84 | 0.033 |
| Other | 1.55 | 1.10, 2.23 | 0.015 |
| Unknown | 1.69 | 1.24, 2.33 | <0.001 |
| Practice type | |||
| Community | – | – | |
| Academic | 1.14 | 0.90, 1.43 | 0.275 |
| Both | 1.76 | 1.17, 2.72 | 0.009 |
| ECOG PS | |||
| 0 | – | – | |
| 1 | 1.16 | 0.94, 1.43 | 0.165 |
| ≥2 | 1.57 | 1.19, 2.08 | 0.002 |
| Unknown | 1.29 | 1.02, 1.66 | 0.037 |
| ISS stage | |||
| Stage I | – | – | |
| Stage II | 1.17 | 0.92, 1.50 | 0.205 |
| Stage II | 1.03 | 0.79, 1.34 | 0.855 |
| Unknown | 1.29 | 1.02, 1.62 | 0.031 |
| Insurance at 1L | |||
| Commercial Health plan | – | – | |
| Medicare | 0.97 | 0.76, 1.24 | 0.809 |
| Medicaid | 0.98 | 0.69, 1.39 | 0.908 |
| Other payer | 1.01 | 0.74, 1.40 | 0.935 |
| Unknown/ uninsured | 1.09 | 0.86, 1.39 | 0.475 |
| Number of HRCA at 1L | |||
| 0 | – | – | |
| 1 | 0.95 | 0.77, 1.16 | 0.598 |
| ≥2 | 0.74 | 0.54, 1.00 | 0.051 |
| Diagnosis year | 1.18 | 1.12, 1.24 | <0.001 |
| Serum creatinine level at 1L | |||
| ≤1.2 mg/dL | – | – | |
| 1.3–2.9 mg/dL | 0.95 | 0.75, 1.21 | 0.689 |
| ≥3 mg/dL | 0.83 | 0.59, 1.17 | 0.277 |
| Unknown | 1.02 | 0.82, 1.26 | 0.877 |
| Bortezomib starting routes | |||
| Subcutaneous | – | – | |
| Intravenous | 0.44 | 0.30, 0.65 | <0.001 |
OR odds ratio, CI confidence interval, ECOG Eastern Cooperative Oncology Group, PS performance status, ISS International Staging System, HRCA high-risk cytogenetic abnormality.
aAdjusted for age at diagnosis, gender, race/ethnicity, practice type, ECOG PS, ISS stage, insurance, number of HRCAs, year of diagnosis, creatinine level and treatment starting route; Treatment reference group: Twice-weekly prescribing at 1L.
As shown in Fig. 3A, there was no statistically significant difference in rwPFS among patients receiving once-weekly (median 37.2 months, 95% CI 33.1–42.4 months) versus twice-weekly bortezomib (median 39.6 months, 95% CI 33.2-46.1 months). The adjusted HR was 0.90 with 95% CI 0.79–1.03 (Table 3). As shown in Fig. 3B, there was also no statistically significant difference in rwOS with median 27.1 months follow-up. Median rwOS was not reached in either group, with a HR 0.90 [95% CI 0.75–1.08]. No violations of the PH assumption were observed. The cumulative neuropathy rate, encompassing any PN diagnosis or initiation of medications for neuropathy was 24.4% overall. As shown in Table 1, PN was significantly more common with twice-weekly bortezomib than once-weekly bortezomib (34.7% versus 18.5%, p < 0.001).
Fig. 3. Real-world PFS and OS based on bortezomib dosing frequency.

A Real-world PFS. B Real-world OS.
Table 3.
Associations between bortezomib dosing and survival.
| Number of patients | Median (months) (95% CI) | HRa(95% CI) | p-value | |
|---|---|---|---|---|
| rwPFS | ||||
| Twice-weekly | 835 | 39.6 (33.2–46.1) | 1.00 (ref) | 0.135 |
| Once-weekly | 1457 | 37.2 (31.1–42.4) | 0.90 (0.79–1.03) | |
| rwOS | ||||
| Twice-weekly | 910 | NA (NA–NA) | 1.00 (ref) | 0.271 |
| Once-weekly | 1587 | NA (76.3–NA) | 0.90 (0.75–1.08) | |
aAdjusted for age at diagnosis, gender, race/ethnicity, practice type, ECOG PS, ISS stage, insurance, number of HRCAs, year of diagnosis, creatinine level and treatment starting route; Treatment reference group: Twice-weekly prescribing at 1L.
Discussion
The incorporation of bortezomib into MM treatment regimens represents a major advancement in the management of this disease. In the frontline setting, for example, the SWOG S0777 and IFM 2005-01 trials demonstrated an overall survival benefit with the addition of twice-weekly bortezomib to induction regimens [26, 27]. Compared to its initial administration in SWOG S0777 and other early trials, bortezomib has largely shifted from intravenous to subcutaneous dosing based on the results of non-randomized analyses showing similar efficacy with fewer toxicities [28]. Indeed, over 90% of patients in our real-world analysis received subcutaneous bortezomib. However, clinical trials have largely continued to use twice-weekly bortezomib dosing even with the transition to subcutaneous dosing. Apart from the ALCYONE and BOSTON studies, relatively few Phase 3 trials in the past decade have incorporated once-weekly bortezomib [29, 30]. Several small studies from academic centers and a large systematic review have already shown that once-weekly dosing has similar efficacy [9–11]. We aimed to study this question with a much larger data set including patients treated in the community setting, who in fact comprised over 75% of our analyzed population.
The frequency of once-weekly bortezomib gradually increased over time, with the majority (73.1%) of patients receiving once-weekly bortezomib in 2022. The usage of once-weekly bortezomib in our data set is higher than these reported in two previous retrospective analyses evaluating bortezomib administration between 2005-2013 and 2008-2018, both of which showed that twice-weekly bortezomib was being prescribed roughly as often as once-weekly bortezomib regimens [9, 10]. This trend may reflect a growing consensus in the field that once-weekly bortezomib constitutes a standard-of-care regimen for MM [31]. Alternatively, some of these differences are likely attributable to the COVID-19 pandemic and a desire to minimize infectious exposures during each clinic visit for bortezomib injection. Indeed, a recent study examining over 7000 patients with MM using similar Flatiron Health data showed significant reductions in all types of cancer-related visits beginning in March 2020 with the pandemic [31, 32].
That being said, approximately a quarter of patients in our study continued to receive bortezomib dosed twice-weekly. Patients who received twice-weekly bortezomib were more likely to be Hispanic/Latinx and less likely to be Asian, a finding broadly in line with previous analyses of racial and ethnic disparities in bortezomib dosing [33]. Additionally, the use of twice-weekly bortezomib was less likely in patients with worsened performance status. While practice setting did not remain associated in multivariate logistic regression analysis, patients treated in community settings were slightly more likely to receive twice-weekly bortezomib. Twice-weekly bortezomib is often utilized in the setting of acute cast nephropathy, which necessitates rapid disease control; however, no relationship was found between creatinine levels at diagnosis and bortezomib dosing. While HRCAs were significantly more common among patients receiving twice-weekly bortezomib, this was not statistically significant in the multivariate analysis.
Regarding clinical outcomes, once-weekly and twice-weekly bortezomib demonstrated comparable rwPFS and rwOS: The median rwPFS was 38.1 months versus 39.8 months, and the median rwOS was not reached in either treatment group. This observation is consistent with outcomes/results of other smaller, single-center studies [9, 10, 12]. Fewer than 1% of patients in our analysis switched from twice-weekly to once-weekly bortezomib during the course of 1 L treatment, making this unlikely as a factor that might have affected the overlapping efficacy of different bortezomib dosing schedules. With regard to neuropathy defined either by billing codes or by the initiation of medications such as gabapentin, we found PN incidences of 18.5% with once-weekly bortezomib versus 34.7% with twice-weekly bortezomib. This matches the conclusion of a previous analysis of pooled data from Phase 3 trials; however, that study used physician determinations of PN and showed a 32% incidence with once-weekly versus 47% with twice-weekly bortezomib [12].
While this represents the largest and the most extensive real-world analysis of bortezomib dosing to date, our retrospective study is not without its limitations. Although we used direct laboratory values and abstracted chart data to assess IMWG responses rather than relying on physician documentation, we did not have full access to full imaging reports to corroborate responses in patients with extramedullary disease. Due to the nature of the Flatiron Health database, PN was identified based on surrogate measures of a combination of diagnostic codes for neuropathy and PN-associated medications. It is probable that patients with mild PN may have gone unreported or undocumented. Indeed, the frequency of initiation of PN-associated medications was approximately four times as high as that of documented PN diagnoses. Furthermore, there may have been unmeasured confounders that influenced physician decision-making around bortezomib dosing. A randomized controlled trial directly comparing once-weekly bortezomib versus twice-weekly bortezomib would be ideal approach to address this question. However, given the overwhelming preference for once-weekly bortezomib dosing among 90% of physicians across the world in a recently published international survey [31], there would not be equipoise for such a study to be launched today.
In conclusion, this study supports the incorporation of once-weekly bortezomib into standard-of-care regimens for newly diagnosed patients with MM. Just as with non-randomized comparisons of subcutaneous versus intravenous bortezomib, once-weekly bortezomib is associated with equivalent outcomes and a more favorable side-effect profile compared to twice-weekly dosing. More broadly, once-weekly bortezomib not only reduces the clinical burden of care by reducing visit frequency but may likely be more cost-effective as well.
Author contributions
FWH, RB, XW, JR, and GK were responsible for the study design. XW and JR performed the statistical analyses and FWH, RB, AMK, XW, JR, and GK interpreted the study results. FWH, RB, and XW wrote the manuscript, and RB, GK, and XW supervised the study. All authors reviewed the manuscript and provided valuable feedback. All authors approved the final version.
Data availability
The data that support the findings of this study have been originated by Flatiron Health, Inc. Requests for data sharing by license or by permission for the specific purpose of replicating results in this manuscript can be submitted to dataaccess@flatiron.com.
Competing interests
RB: Consulting: BMS, Caribou Biosciences, Genentech, Janssen, Karyopharm, Pfizer, Sanofi, SparkCures; Research: Pack Health. XW: Employment: Flatiron Health, Inc. (independent subsidiary of the Roche Group), stock ownership, Roche. JR: Employment: Flatiron Health, Inc. (independent subsidiary of the Roche Group), stock ownership, Roche. LDA Jr: Consulting: Janssen, Celgene, BMS, Amgen, GSK, AbbVie, Beigene, Cellectar, Sanofi, Prothena. Research: BMS, Celgene, GSK, Janssen, Abbvie. AJC: Consulting: BMS, Adaptive; Research: Adaptive Biotechnologies, Harpoon, Nektar, BMS, Janssen, Sanofi, AbbVie. GK: Consulting: BMS, Arcellx, Sanofi, Janssen, Cellectar, Pfizer, Kedrion; Research: BMS, Janssen, Abbvie. The remaining authors have no disclosures to report.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Fieke W. Hoff, Rahul Banerjee.
References
- 1.Anderson KC, Carrasco RD. Pathogenesis of myeloma. Annu Rev Pathol. 2011;6:249–74. doi: 10.1146/annurev-pathol-011110-130249. [DOI] [PubMed] [Google Scholar]
- 2.Cowan AJ, Green DJ, Kwok M, Lee S, Coffey DG, Holmberg LA, et al. Diagnosis and management of multiple myeloma: a review. JAMA. 2022;327:464–77. doi: 10.1001/jama.2022.0003. [DOI] [PubMed] [Google Scholar]
- 3.Durie BGM, Hoering A, Abidi MH, Rajkumar SV, Epstein J, Kahanic SP, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. 2017;389:519–27. doi: 10.1016/S0140-6736(16)31594-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Joseph NS, Kaufman JL, Dhodapkar MV, Hofmeister CC, Almaula DK, Heffner LT, et al. Long-term follow-up results of lenalidomide, bortezomib, and dexamethasone induction therapy and risk-adapted maintenance approach in newly diagnosed multiple myeloma. J Clin Oncol. 2020;38:1928–37. doi: 10.1200/JCO.19.02515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Argyriou AA, Iconomou G, Kalofonos HP. Bortezomib-induced peripheral neuropathy in multiple myeloma: a comprehensive review of the literature. Blood. 2008;112:1593–9. doi: 10.1182/blood-2008-04-149385. [DOI] [PubMed] [Google Scholar]
- 6.Sun LF, Maples KT, Hall KH, Liu Y, Cao Y, Joseph NS, et al. Impact of black race on peripheral neuropathy in patients with newly diagnosed multiple myeloma receiving bortezomib induction. JCO Oncol Pract. 2023;19:793–8. doi: 10.1200/OP.22.00781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tokuhira M, Watanabe R, Nemoto T, Hanzawa K, Sagawa M, Tomikawa T, et al. Successful treatment with a modified bortezomib schedule of weekly and longer intervals for patients with refractory/resistance multiple myeloma. Leuk Res. 2011;35:591–7. doi: 10.1016/j.leukres.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 8.Bringhen S, Larocca A, Rossi D, Cavalli M, Genuardi M, Ria R, et al. Efficacy and safety of once-weekly bortezomib in multiple myeloma patients. Blood. 2010;116:4745–53. doi: 10.1182/blood-2010-07-294983. [DOI] [PubMed] [Google Scholar]
- 9.Sidana S, Narkhede M, Elson P, Hastings D, Faiman B, Valent J, et al. Neuropathy and efficacy of once weekly subcutaneous bortezomib in multiple myeloma and light chain (AL) amyloidosis. PLoS ONE. 2017;12:e0172996. doi: 10.1371/journal.pone.0172996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cook J, Johnson I, Higgins A, Sidana S, Warsame R, Gonsalves W, et al. Outcomes with different administration schedules of bortezomib in bortezomib, lenalidomide and dexamethasone (VRd) as first-line therapy in multiple myeloma. Am J Hematol. 2021;96:330–7. doi: 10.1002/ajh.26074. [DOI] [PubMed] [Google Scholar]
- 11.Mateos MV, San-Miguel J, Goldschmidt H, Sonneveld P, Dimopoulos MA, Heeg B, et al. The effects of different schedules of bortezomib, melphalan, and prednisone for patients with newly diagnosed multiple myeloma who are transplant ineligible: a matching-adjusted indirect comparison. Leuk Lymphoma. 2020;61:680–90. doi: 10.1080/10428194.2019.1675881. [DOI] [PubMed] [Google Scholar]
- 12.Mateos MV, Bringhen S, Richardson PG, Lahuerta JJ, Larocca A, Oriol A, et al. Bortezomib cumulative dose, efficacy, and tolerability with three different bortezomib-melphalan-prednisone regimens in previously untreated myeloma patients ineligible for high-dose therapy. Haematologica. 2014;99:1114–22. doi: 10.3324/haematol.2013.099341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Palumbo A, Bringhen S, Larocca A, Rossi D, Di Raimondo F, Magarotto V, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: Updated follow-up and improved survival. J Clin Oncol. 2014;32:634–40. doi: 10.1200/JCO.2013.52.0023. [DOI] [PubMed] [Google Scholar]
- 14.Mateos MV, Oriol A, Martínez-López J, Gutiérrez N, Teruel AI, de Paz R, et al. Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial. Lancet Oncol. 2010;11:934–41. doi: 10.1016/S1470-2045(10)70187-X. [DOI] [PubMed] [Google Scholar]
- 15.Zhang L, Mager DE. Population-based meta-analysis of bortezomib exposure–response relationships in multiple myeloma patients. J Pharmacokinet Pharmacodyn. 2020;47:77–90. doi: 10.1007/s10928-019-09670-3. [DOI] [PubMed] [Google Scholar]
- 16.Birnbaum B, Nussbaum N, Seidl-Rathkopf K, Agrawal M, Estevez M, Estola E, et al. Model-assisted cohort selection with bias analysis for generating large-scale cohorts from the EHR for oncology research. Preprint at https://arxiv.org/abs/2001.09765 (2020).
- 17.Ma X, Long L, Moon S, Adamson BJS, Baxi S. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron Health, SEER, and NPCR. medRxiv (2020).
- 18.McCaughan GJ, Gandolfi S, Moore JJ, Richardson PG. Lenalidomide, bortezomib and dexamethasone induction therapy for the treatment of newly diagnosed multiple myeloma: a practical review. Br J Haematol. 2022;199:190–204. doi: 10.1111/bjh.18295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.O’Donnell EK, Laubach JP, Yee AJ, Chen T, Huff CA, Basile FG, et al. A phase 2 study of modified lenalidomide, bortezomib and dexamethasone in transplant-ineligible multiple myeloma. Br J Haematol. 2018;182:222–30. doi: 10.1111/bjh.15261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Greipp PR, Miguel JS, Dune BGM, Crowley JJ, Barlogie B, Bladé J, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23:3412–20. doi: 10.1200/JCO.2005.04.242. [DOI] [PubMed] [Google Scholar]
- 21.Costa LJ, Chhabra S, Medvedova E, Dholaria BR, Schmidt TM, Godby KN, et al. Daratumumab, carfilzomib, lenalidomide, and dexamethasone with minimal residual disease response-adapted therapy in newly diagnosed multiple myeloma. J Clin Oncol. 2022;40:29001–2912. doi: 10.1200/JCO.21.01935. [DOI] [PubMed] [Google Scholar]
- 22.Palumbo A, Avet-Loiseau H, Oliva S, Lokhorst HM, Goldschmidt H, Rosinol L, et al. Revised international staging system for multiple myeloma: A report from international myeloma working group. J Clin Oncol. 2015;33:2863–9. doi: 10.1200/JCO.2015.61.2267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhang Q, Gossai A, Monroe S, Nussbaum NC, Parrinello CM. Validation analysis of a composite real-world mortality endpoint for patients with cancer in the United States. Health Serv Res. 2021;56:1281–7. doi: 10.1111/1475-6773.13669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Curtis MD, Griffith SD, Tucker M, Taylor MD, Capra WB, Carrigan G, et al. Development and validation of a high-quality composite real-world mortality endpoint. Health Serv Res. 2018;53:4460–76. doi: 10.1111/1475-6773.12872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17:e328–e346. doi: 10.1016/S1470-2045(16)30206-6. [DOI] [PubMed] [Google Scholar]
- 26.Durie BGM, Hoering A, Sexton R, Abidi MH, Epstein J, Rajkumar SV, et al. Longer term follow-up of the randomized phase III trial SWOG S0777: bortezomib, lenalidomide and dexamethasone vs. lenalidomide and dexamethasone in patients (Pts) with previously untreated multiple myeloma without an intent for immediate autologous stem cell transplant (ASCT) Blood Cancer J. 2020;10:53. doi: 10.1038/s41408-020-0311-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Harousseau JL, Attal M, Avet-Loiseau H, Marit G, Caillot D, Mohty M, et al. Bortezomib plus dexamethasone is superior to vincristine plus doxorubicin plus dexamethasone as induction treatment prior to autologous stem-cell transplantation in newly diagnosed multiple myeloma: Results of the IFM 2005-01 phase III trial. J Clin Oncol. 2010;28:4621–9. doi: 10.1200/JCO.2009.27.9158. [DOI] [PubMed] [Google Scholar]
- 28.Merz M, Salwender H, Haenel M, Mai EK, Bertsch U, Kunz C, et al. Subcutaneous versus intravenous bortezomib in two different induction therapies for newly diagnosed multiple myeloma: An interim analysis from the prospective GMMG-MM5 trial. Haematologica. 2015;100:964–9. doi: 10.3324/haematol.2015.124347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mateos MV, Cavo M, Blade J, Dimopoulos MA, Suzuki K, Jakubowiak A, et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): a randomised, open-label, phase 3 trial. Lancet. 2020;395:132–41. doi: 10.1016/S0140-6736(19)32956-3. [DOI] [PubMed] [Google Scholar]
- 30.Grosicki S, Simonova M, Spicka I, Pour L, Kriachok I, Gavriatopoulou M, et al. Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, phase 3 trial. Lancet. 2020;396:1563–73. doi: 10.1016/S0140-6736(20)32292-3. [DOI] [PubMed] [Google Scholar]
- 31.Banerjee R, Wang B, Anderson LD, McCaughan G, Mehra N, Cowan AJ, et al. Once-weekly bortezomib as the standard of care in multiple myeloma: results from an international survey of physicians. Blood Cancer J. 2023;13:162. doi: 10.1038/s41408-023-00937-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Goyal G, Lau KW, Wang X, Davidoff AJ, Huntington SF, Jamy O, et al. The COVID-19 Pandemic and In-Person Visit Rate Disruptions Among Patients With Hematologic Neoplasms in the US in 2020 to 2021. JAMA Netw Open. 2023;6:e2316642. doi: 10.1001/jamanetworkopen.2023.16642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ailawadhi S, Frank RD, Advani P, Swaika A, Temkit M, Menghani R, et al. Racial disparity in utilization of therapeutic modalities among multiple myeloma patients: a SEER-medicare analysis. Cancer Med. 2017;6:2876–85. doi: 10.1002/cam4.1246. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study have been originated by Flatiron Health, Inc. Requests for data sharing by license or by permission for the specific purpose of replicating results in this manuscript can be submitted to dataaccess@flatiron.com.