

Abstract
Background:
Health behaviors, such as diet and exercise, are actions individuals take that can potentially impact gastrointestinal (GI) symptoms and the gut microbiota. Little is known about how health behaviors impact GI symptoms and the gut microbiota after anti-cancer therapies.
Methods:
This is a secondary analysis of a cross-sectional study that investigated relationships between GI symptoms, gut microbiota, and patient-reported outcomes in adult cancer survivors. Gut microbiota was assessed from stool samples using 16 S rRNA gene sequencing. GI symptoms and health behaviors were measured via self-report. Descriptive statistics, multiple regression, and correlation analyses are reported.
Results:
A total of 334 cancer survivors participated, and a subsample of 17 provided stool samples. Most survivors rated their diet as moderately healthy (55.7%) and reported engaging in low intensity exercise (53.9%) for ≤5 h/week (69.1%). Antibiotic use was associated with more belly pain, constipation, and diarrhea (P < .05). Survivors consuming a healthier diet had fewer symptoms of belly pain (P = .03), gas/bloating (P = .01), while higher protein consumption was associated with less belly pain (P = .03). Better diet health was positively correlated with Lachnospiraceae abundance, and negatively with Bacteroides abundance (P < .05). Greater exercise frequency positively correlated with abundance of Lachnospiraceae, Faecalibacterium, Bacteroides, Anaerostipes, Alistipes, and Subdoligranulum (P < .05).
Conclusion:
Results provide evidence for associations between antibiotic use, probiotic use, dietary health behaviors, and GI symptoms. Diet and exercise behaviors are related to certain types of bacteria, but the direction of causality is unknown. Dietary-based interventions may be optimally suited to address survivors’ GI symptoms by influencing the gut microbiota. Larger trials are needed.
Keywords: health behaviors, gastrointestinal symptoms, gut microbiota, diet, exercise, cancer survivors
Introduction
Health behaviors, specifically diet and exercise, are a crucial part of maintaining human health and a key strategy in cancer care.1,2 Yet cancer rates continue to rise, with an estimated 233 900 Canadians being diagnosed with cancer in 2022, 3 and 1.9 million new cancer cases and 609 360 cancer deaths for Americans that same year. 4 Modifiable health behaviors, specifically exercise and nutrition, can impact cancer risk and recovery. Despite evidence demonstrating numerous beneficial effects of exercise and healthy dietary behaviors,5-7 many individuals continue to engage in a sedentary lifestyle and poor nutritional habits.
Health behaviors are actions that can directly affect one’s health outcomes. Smoking tobacco, excessive consumption of alcohol, unhealthy diet, and inactivity are prime examples of adverse health behaviors that increase one’s risk of developing cancer. 2 Studies have found that healthy dietary behaviors exert protective effects against cancer risk and mortality.8,9 A “healthy diet” refers to “health-promoting and disease-preventing. It provides adequacy without excess, of nutrients and health-promoting substances from nutritious foods and avoids the consumption of health-harming substances.” 10 Additionally, dietary patterns with high consumption of processed sugars and meats, which are known carcinogens,11,12 and limited fruit and vegetable intake, such as the Standard Western diet, is characterized by local inflammation of the GI tract and increased intestinal permeability, 13 and associated with greater incidence and severity of mental health symptom burden. 14
The American Institute of Cancer Research, 15 the American Cancer Society, 1 and other organizations have published numerous, evidence-based resources and guidelines to support clinicians in counseling patients, and patients in making informed decisions about their dietary choices. However, there exists a paucity of evidence describing dietary health behaviors among survivors of cancer, particularly in comparison to healthy peers. Moreover, evidence-based nutritional guidance from health care providers throughout the cancer care continuum has been identified as one of the main unmet needs for patients and their families. 16
Physical inactivity has also been linked to increased risk for cancer and poorer survival post-diagnosis. 8 The American Cancer Society recommends that adult cancer survivors engage in 150 to 300 minutes of moderate-intensity, or 75 to 150 minutes of vigorous-intensity, physical activity per week with an emphasis on aiming to meet or exceed the upper limit of 300 minutes. 1 However, relative to healthy peers with no history of cancer, survivors of cancer tend to engage in less physical activity 17 that does not meet the recommended guidelines despite evidence showing that survivors’ engagement in physical activity exerts protective effects against cancer recurrence, improved physical function, and quality of life.1,18
Exercise, and especially diet, have been implicated as important health behavior factors impacting the human gut microbiota, which consists of the community of microorganisms, notably bacteria, fungi, archaea and eukaryotes, that colonize the gastrointestinal (GI) tract. 19 Previous studies with rodents and humans using randomized controlled trials and observational designs, have shown that regular exercise can impact the composition of the gut microbiota.6,13 Furthermore, several recent, comprehensive reviews drawing on clinical and preclinical evidence have detailed how specific dietary behaviors, such as the Mediterranean diet, can impact the gut microbiota.13,20,21
While health behaviors are clearly implicated in the health and function of the gut microbiota, adverse events such as exposure to chemotherapy treatment for cancer adversely affects the gut microbiota acutely and may also result in chronic gut microbial perturbations, with potential effects on GI and mental health.22,23 Alterations in the gut microbiota are associated with inflammatory GI conditions such as inflammatory bowel disease (IBD), irritable bowel syndrome (IBS), 24 and GI mucositis (ie, painful inflammation and ulceration of the mucous membranes lining the digestive tract), which have been implicated in the onset and maintenance of post-chemotherapy GI symptoms.22,25 Primary work from our Chemo-Gut study found that within the first 6 months to 1-year post-chemotherapy, survivors had significantly reduced gut microbiota alpha diversity compared to survivors greater than 1-year post-treatment and healthy peers. 26 Moreover, compared to healthy peers with no history of cancer, the relative abundances of specific taxa remained different in survivors up to 5-years post-treatment; Certain bacterial taxa were correlated with psychosocial outcomes, including increased depression and poorer cognitive function. 26 Our previous work also found that survivors experience chronic, moderate to severe, GI symptoms, lasting for an average of 2.5 years post-treatment, and that higher GI symptom burden is associated with poorer mental health. 27 However, the potential impact of diet and exercise behaviors on survivors’ gut microbiota remains to be elucidated.
The present study is an analysis of secondary outcomes from the Chemo-Gut project. The objectives of this study were to: (i) describe health behaviors related to diet and exercise in a cohort of cancer survivors; (ii) investigate associations between health behaviors, specifically diet and exercise, and GI symptoms in a cohort of cancer survivors; and (ii) explore associations between exercise and dietary health behaviors and the gut microbiota in a subset of our sample that provided stool samples for analysis.
Materials and Methods
Participants
Participants for this secondary analysis were combined from both the Chemo-Gut Pilot study 26 and the Chemo-Gut Survey study. 27 The demographic, clinical, and GI outcome related data were similar between the 2 studies, thus allowing us to pool the results for the health behavior and GI outcome data. The full methodology including sample size calculations are previously described.26,27 Briefly, participants for the survey study cohort were recruited virtually via social media channels, and the sample was comprised of Canadians who had previously been diagnosed with cancer, were currently aged 18 years or older, and had received and completed anti-cancer therapies (eg, chemotherapy, radiotherapy). Participants for the pilot study were recruited from the Tom Baker Cancer Centre in Calgary, Canada and via social media and local cancer support groups. Participants in this cohort were between 18 and 39 years of age, diagnosed with a blood cancer or solid tumor, had previously received chemotherapy, and were within 5 years from their final cancer treatments. These studies were approved by the Health Research Ethics Board of Alberta Cancer Committee (HREBA.CC-19-0018).
Procedure
All demographic, clinical, and GI outcome measures were administered via a link made available to participants through Remote Electronic Data Capture (REDCap), a secure browser-based application designed to support Electronic Data Capture for research studies provided through the Clinical Research Unit (CRU) in the University of Calgary Cumming School of Medicine. Full data and stool collection procedures are previously described.26-28 Briefly, participants were instructed to use the investigator-provided home stool collection kit. Samples were collected in a sterile conical tube, placed in a biohazard bag, and stored in the participant’s freezer until pick-up, no more than 3 days from time of collection. Samples were picked-up by research personnel and transported on ice directly to the University of Calgary Faculty of Kinesiology and stored at −80°C degrees until analysis.
Demographic, Clinical and GI Measures
Details regarding patient reported outcomes have previously been published.27,28 The demographic and clinical health outcomes questionnaire was a locally designed survey that was developed based on patient partner input, and coauthor expertise. Data collected and used for this secondary analysis included dietary and exercise behaviors. Dietary behaviors related use of antibiotics or probiotics within the last 2 years, dummy coded as No (0) or Yes (1). We also inquired about the number of times per week participants consumed processed foods/meals, and their self-rated diet healthiness. Specifically, we asked, “on average, how many times per week do you consume ready-made/processed meals (eg, macaroni and cheese, pizza from a box, etc.)” and “In general, how would you rate your current diet?.” Response options are detailed in Table 1.
Table 1.
Diet and Exercise Health Behaviors in Cancer Survivors.
| Health behavior | % (n) |
|---|---|
| Antibiotic use (≤2 y) | |
| Yes | 47.3 (158) |
| No | 44.6 (149) |
| Nonresponse | 8.1 (27) |
| Probiotic use (≤2 y) | |
| Yes | 34.7 (116) |
| No | 59.0 (197) |
| Nonresponse | 6.3 (21) |
| Self-rated diet healthiness | |
| Somewhat unhealthy or unhealthy | 17.0 (57) |
| Moderately healthy | 55.7 (186) |
| Healthy | 21.9 (73) |
| Nonresponse | 5.4 (18) |
| Consumption of processed foods/meals (per week) | |
| 0 | 50.9 (170) |
| 1-3 | 39.8 (133) |
| 4-6 | 3.0 (10) |
| 7-9 | 0.3 (1) |
| Nonresponse | 6.0 (20) |
| Servings of vegetables (per day) | |
| 2 or less | 38.6 (129) |
| 3-5 | 46.7 (156) |
| 6-8 | 7.8 (26) |
| More than 9 | 1.5 (5) |
| Nonresponse | 5.4 (18) |
| Servings of fruits (per day) | |
| 2 or less | 52.1 (174) |
| 3-5 | 38.0 (127) |
| 6-8 | 3.9 (13) |
| More than 9 | 0 (0) |
| Nonresponse | 6.0 (20) |
| Servings of proteins (per day) | |
| Less than 2 | 34.1 (114) |
| 2-4 | 48.8 (163) |
| More than 4 | 11.4 (38) |
| Nonresponse | 5.7 (19) |
| Servings of whole grains (per day) | |
| 2 or less | 48.2 (161) |
| 3-5 | 41.3 (138) |
| 6-8 | 3.6 (12) |
| More than 8 | 0.3 (1) |
| Nonresponse | 6.6 (22) |
| Exercise frequency (hours per week) | |
| 2 or less | 32.3 (108) |
| 3-5 | 36.8 (123) |
| 6-9 | 18.3 (61) |
| 9 or more | 8.7 (29) |
| Nonresponse | 3.9 (13) |
| Exercise intensity | |
| Low (eg, walking) | 53.9 (180) |
| Moderate (eg, jogging) | 38.3 (128) |
| High (eg, HIIT, spin) | 3.9 (13) |
| Nonresponse | 3.9 (13) |
For daily consumption of different food groups, we inquired about participants average intake of vegetables, fruits, proteins, and whole grains. Examples were provided to help participants quantify their intake and response options were created in consultation with one of the co-authors who is a registered dietitian. Regarding vegetable consumption the question stated: “a standard serving of vegetables is about 75 g (24-84 calories) (eg, ½ cup cooked green or orange vegetables (eg, broccoli, carrots), ½ cup cooked dried or canned beans, peas or lentils, or 1 cup green leafy or raw salad vegetables). On average, how many servings of vegetables do you consume each day?.” For fruit consumption, the question stated: “A standard serving of fruits is about 1 cup (eg, 1 medium apple; 1 medium banana; 6 large strawberries). On average, how many servings of fruits do you consume each day?”. For proteins, the question asked: “In general, 1 ounce of meat, fish or poultry (size of a deck of cards), ¼ cup cooked beans, 1 egg, 1 tablespoon of peanut butter, or ½ ounce of nuts or seeds is considered as 1 ounce-serving from the protein food group. On average, how many servings of protein do you consume each day?.” For grains, the question stated: “A serving of whole grains is 16 g in a whole grain product (eg, 1/2 cup cooked brown rice, 100% whole grain pasta, oatmeal, or other cooked grain; 1 slice 100% whole grain bread). On average, how many servings of whole grains do you consume each day?.” Response options are shown in Table 1.
Exercise behaviors pertained to the average frequency of exercise per week, specifically we asked, “on average, how many hours each week of exercise do you get?,” as well as intensity, inquiring, “on average, how would you rate the intensity of your exercise?.” Response options are noted in Table 1. Regarding intensity, examples were provided for each (ie, “low intensity” is walking at a normal pace; “moderate intensity” could be jogging or weightlifting; “high intensity” includes high intensity interval training (HIIT), spin class, etc.) to help participants quantify the intensity of their exercise.
GI symptoms included patient-reported outcomes for constipation, diarrhea, gas/bloating, and abdominal pain as measured using the National Institutes for Health (NIH) Patient-Reported Outcomes Measurement Information System (PROMIS). 29 PROMIS measures are person-centered, validated, and reliable tools used to evaluate a variety of health-related outcomes in people with health conditions, including cancer and GI disorders.30-32
Gut Microbiota Profiling and Bioinformatics
Complete details regarding gut microbiota profiling and bioinformatics analysis are reported previously. 26 Briefly, bacterial DNA was extracted from ~60 mg of fecal matter using the FastDNA Spin Kits for feces (MP Biomedicals, Lachine, QC, Canada). The samples were then diluted to 4 ng/uL using the PicoGreen DNA quantification kit (Invitrogen, Carlbad, CA, USA) and stored at −20°C until sequencing. The MiSeq Illumina platform amplified the V3 and V4 region of the 16 S rRNA gene (Illumina, San Diego, CA, USA), which was used to evaluate microbial composition. Bacterial DNA samples were sequenced at the University of Calgary’s Centre for Health Genomics and Informatics. Bioinformatics were processed using R (version 4.1.2). Raw bacterial DNA sequence reads were pre-processed using DADA2 (version 1.22.0). 33 ASV taxonomic classification was assigned using the Silva database (version 138.1), 34 plots and summary statistics were provided using the phyloseq package (version 1.38.0) and the summary function from base R.
Data Analysis
To address objective 1, descriptive statistics and frequency analyses were used to describe health behaviors related to diet and exercise in this cohort of cancer survivors. For objective 2, investigating associations between health behaviors and GI symptoms, multiple regression analyses were used. Antibiotic and probiotic use, diet (ie, self-rated diet healthiness, processed foods, and daily food group consumption including fruits, vegetables, whole grains, and protein), and exercise (ie, frequency and intensity) behaviors were entered into the regression models to explore whether these behaviors were associated with GI symptoms (ie, gas/bloating, belly pain, constipation, and diarrhea). Beta values are reported as unstandardized. To address objective 3, Spearman’s rho correlation analyses for non-parametric data were used to explore associations between antibiotic and probiotic use, dietary, and exercise health behaviors and the gut microbiota. Only the first 30 most abundant ASV’s with n > 10 cases were used for analysis. 35 An ASV or amplicon sequence variant is a single DNA sequence whose level of resolution is very high. Unfortunately, however, most ASVs are not assigned nomenclature at the species or subspecies level, but rather are given a number to distinguish them from other ASVs. What is known from our data are the family (anything shown as f_) or genus (anything shown as g_), as we have listed them in our heatmaps showing the correlations. Since this is a relatively new field that is constantly evolving, different datasets show different numbers of ASVs belonging to the family Lachnospiraceae and Bacteroides, for instance. As this objective was exploratory and utilized a small sample, corrections for multiple comparisons were not conducted which increases the potential risk for Type I errors. Statistical analyses were completed using IBM Statistical Package for the Social Sciences (SPSS) version 28, with alpha set at P < .05.
Results
Objective 1: Describing the Health Behaviours of Cancer Survivors
Our sample consisted of N = 334 survivors of cancer. The mean current age of survivors was 46.2 (SD = 14.8) years, while the average age at diagnosis was 40.3 (SD = 15.2) years old. The sample was primarily female (83.2%) and comprised mainly of survivors of breast (41%), hematological (19.5%), gynecological (11.1%), and colorectal (6.6%) cancers. Cancer stages ranged from I through IV, although the majority of participants had been diagnosed with stage II (30.2%) or III (26.9%) malignancies. Most (86.8%) participants had received chemotherapy treatment, followed by surgery (76.9%) and radiation (61.1%). Among the 17 survivors who provided fecal samples, the mean current age in years was 32.0 (SD = 5.8), and 64.7% were female. The mean age at diagnosis was 30.1 (SD = 6.0) years old, while average time off treatment was 16.9 (SD = 16.4) months. Almost half (41.2%) had completed treatment within the last 6 months while 58.8% completed treatment between 11 months to 5 years prior to study participation. About two-thirds (64.7%) of survivors had a hematological cancer diagnosis. All survivors providing a fecal sample had previously received chemotherapy; 35.3% had also received surgery, and 17.6% received radiation therapy. Complete details of participant and treatment related outcomes are previously reported elsewhere.26,27
Data regarding diet and exercise related health-related behaviors are summarized in Table 1. Within the last 2 years 34.7% of survivors reported using probiotics, while 47.3% reported using antibiotics. Overall, survivors tended to rate their diet as moderately healthy (55.7%), and reported consuming none (50.9%) or few (39.8%) processed foods or meals per week. Regarding daily food group consumption, 38.6% report consuming 2 or fewer servings of vegetables or fruits (52.1%) per day, while about half (48.8%) reporting consuming 2 to 4 servings of protein per day. Daily consumption of 2 or fewer servings of whole grains were reported by 48.2% of participants. Most survivors reported engaging in exercise for 2 or less (32.3%) or 3 to 5 (36.8%) hours per week. A low exercise intensity was most frequently reported by 53.9% of participants.
Objective 2: Associations Between Health Behaviours and GI Symptoms
For GI symptoms, participants ranged from minimum outcome values indicating few to no symptoms that are within “normal” range, to scores >70, indicative of severe GI symptoms associated with poorer health (see Figure 1). 36 For belly pain the mean PROMIS score was 52.7 (n = 305, SD = 11.2, range = 34-77), while the mean score for constipation was 52.5 (n = 285, SD = 8.4, range = 37-79). For the GI symptom of diarrhea, the mean score was 51.1 (n = 282, SD = 9.1, range = 40-75). However, the only symptom reported with a mean value higher than the PROMIS healthy reference population was gas/bloating with a mean score of 56.2 (n = 287, SD = 8.1, range = 35-73), indicating a clinically meaningful difference from the healthy population normative score of 50. 37
Figure 1.
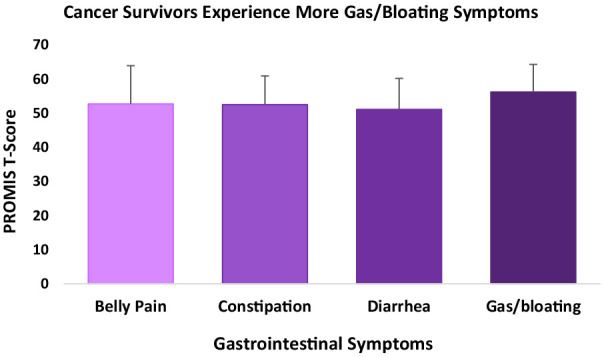
PROMIS measures for GI symptoms.
Table 2 details the results of the multiple regression analyses examining whether consumption of antibiotics or probiotics, dietary behaviors and exercise behaviors were predictive of GI symptoms. Antibiotic use within the past 2 years was associated with more symptoms of belly pain (B = 3.15, SE = 1.35, P < .02), constipation (B = 2.10, SE = 1.09, P < .05), and diarrhea (B = 3.08, SE = 1.16, P < .01). Also, probiotic use was associated with more belly pain (B = 4.95, SE = 1.39, P < .001) and gas/bloating (B = 4.54, SE = 1.05, P < .001) symptoms. For dietary behaviors and GI symptoms; we found that higher rated diet healthiness was associated with lower symptoms of belly pain (B = −2.76, SE = 1.26, P < .03), and gas/bloating (B = −2.65, SE = 0.96, P < .01), as well as a higher protein consumption at more than 2 servings daily was associated with lower belly pain symptoms (B = −2.52, SE = 1.13, P < .03). However, there is no significant relationships between exercise frequency or intensity and any of the GI symptoms.
Table 2.
Associations Between Antibiotic Use, Probiotic Use, Dietary Behaviors, Exercise Behaviors and GI Symptoms. Reported as Unstandardized Beta Coefficient (Standard Error).
| GI symptom | |||||
|---|---|---|---|---|---|
| Belly pain | Constipation | Diarrhea | Gas/bloating | ||
| Consumption of antibiotics and probiotics | Antibiotic | 3.15 (1.35)* | 2.10 (1.09)* | 3.08 (1.16)* | 0.97 (1.02) |
| Probiotic | 4.95 (1.39)* | 1.35 (1.11) | 1.89 (1.18) | 4.54 (1.05)* | |
| Dietary behavior | Diet healthiness | −2.76 (1.26)* | −1.29 (1.01) | −1.03 (1.07) | −2.65 (0.96)* |
| Processed foods | 0.85 (1.28) | 1.20 (1.03) | 0.53 (1.10) | −0.04 (0.96) | |
| Vegetables | 0.24 (1.11) | −0.05 (0.88) | 0.37 (0.94) | 0.75 (0.83) | |
| Fruits | −0.19 (1.24) | −0.25 (0.99) | −0.91 (1.06) | −0.37 (0.93) | |
| Protein | −2.52 (1.13)* | −1.46 (0.92) | −0.76 (0.98) | −0.77 (0.87) | |
| Whole grains |
−1.22 (1.16) | 1.53 (0.93) | −0.67 (1.00) | −0.74 (0.88) | |
| Exercise behavior | Frequency | −0.49 (0.77) | 0.03 (0.63) | −0.48 (0.66) | −0.60 (0.58) |
| Intensity | 2.12 (1.29) | 1.77 (1.07) | 1.36 (1.14) | 1.42 (0.99) | |
Note. *Significant associations (P < .05) in bold.
Objective 3: Correlations Between Health Behaviours and the Gut Microbiota
Spearman’s rho correlation analysis for non-parametric data were used to examine relationships between bacterial taxonomic composition and dietary and exercise health behaviors in a subset of 17 survivors. Figure 2 illustrates correlations between antibiotic and probiotic use and specific taxa. Only antibiotic use significantly correlated with any of the microbial taxa. Specifically, Lachnospiraceae (ASV-1) (ρ = 0.55, P = .02), Bacteroides (ASV-9) (ρ = 0.75, P < .01), and Lachnospiraceae (ASV-26) (ρ = 0.60, P = .02) correlated positively with antibiotic use.
Figure 2.

Heatmap of correlations between antibiotic and probiotic use behaviors and ASV’s at the order (o), family (f), and genus (g) levels in cancer survivors. Spearman’s rho is presented. Values for n range from 10 to 17. Bolded correlations are statistically significant at the P < .01 level. All other correlations statistically significant at the P < .05 level.
As seen in Figure 3, for dietary behaviors, Lachnospiraceae (ASV-3) was positively correlated with self-rated diet health (ρ = 0.51, P = .05), while Bacteroides (ASV-14) correlated negatively (ρ = −0.62, P = .02) with diet healthiness. Fruit consumption was positively correlated with both Lachnospiraceae (ASV-12) (ρ = 0.80, P < .001) and Subdoligranulum (ASV-29) (ρ = 0.61, P = .02). Consumption of whole grains was positively correlated with Lachnospiraceae (ASV-3) (ρ = 0.63, P = .01), but negatively correlated with Anaerostipes (ASV-11) (ρ = −0.59, P = .02).
Figure 3.

Heatmap of correlations between dietary health behaviors and ASV’s at the order (o), family (f), and genus (g) levels in cancer survivors. Spearman’s rho is presented. Values for n range from 10 to 17. Bolded correlations are statistically significant at the P < .01 level. All other correlations statistically significant at the P < .05 level.
Figure 4 illustrates the correlations between exercise related health behaviors, specifically exercise frequency and intensity, and bacterial taxa. Exercise frequency was positively correlated with Lachnospiraceae (ASV-1) (ρ = 51, P = .04), Faecalibacterium (ASV-6) (ρ = 0.65, P = .01), Bacteroides (ASV-9) (ρ = 0.66, P = .01), Anaerostipes (ASV-11) (ρ = 0.53, P = .04), Alistipes (ASV-27) (ρ = 0.75, P = .01), and Subdoligranulum (ASV-29) (ρ = 0.59, P = .03). Meanwhile, only Lachnospiraceae (ASV-3) was negatively correlated with exercise intensity (ρ = −0.63, P = .01).
Figure 4.

Heatmap of correlations between exercise health behaviors and ASV’s at the order (o), family (f), and genus (g) levels in cancer survivors. Spearman’s rho is presented. Values for n range from 10 to 17. Bolded correlations are statistically significant at the P < .01 level. All other correlations statistically significant at the P < .05 level.
Discussion
Among the 334 post-treatment survivors of cancer who participated in this study, 55.7% rated their diet as moderately healthy, while 53.9% reported engaging in low intensity exercise for ≤5 hours/week. Consistent with previous research on antibiotics and GI symptoms, antibiotic use was associated with more belly pain, constipation, and diarrhea. Importantly, those who consumed a healthier diet had fewer symptoms of belly pain and gas/bloating, while higher protein consumption was associated with less belly pain. Better diet health was also positively correlated with Lachnospiraceae abundance, and negatively correlated with Bacteroides abundance. Greater exercise frequency positively correlated with abundance of Lachnospiraceae, Faecalibacterium, Bacteroides, Anaerostipes, Alistipes, and Subdoligranulum. Results provide novel evidence for associations between antibiotic use, probiotic use, dietary and exercise health behaviors and GI symptoms and the gut microbiota.
Health Behaviours in Survivors of Cancer
In this cohort of cancer survivors, self-rated diet healthiness was reported by over half of the participants as being moderately healthy. Participants indicated that they consumed no, or few processed foods or meals per week, which is consistent with recommendations from the American Cancer Society. 1 These data provide new evidence describing specific dietary health behaviors in a diverse sample of cancer survivors. Considering the established link between diet and good health, previous studies have investigated the effects of various dietary interventions in survivors of cancer, 38 yet there is limited information regarding specific dietary behaviors in cancer cohorts. Further research is needed to characterize a comprehensive range of dietary behaviors in cancer survivors that may impact health outcomes.
Participants’ daily consumption of different food groups, and particularly vegetables and fruits, which are known to beneficially support gut microbial health and overall health more generally, was concerningly low. Over one-third (38.6%) of survivors reported consuming 2 or fewer servings of vegetables per day, while about half (52.1%) reported consuming 2 or fewer servings of fruit per day. Canada’s Food Guide recommends 7 to 10 daily servings of fruits and vegetables for adults, 39 indicating that survivors’ in our study do not meet the guidelines for healthy fruit and vegetable consumption. Vegetables contain crucial vitamins and nutrients to support cancer prevention and recovery, in addition to fiber necessary for optimal gut microbial function. For instance, cruciferous vegetables like broccoli and cabbage contain isothiocyanates and a potent phytochemical called sulforaphane, which evidence suggests is effective in the prevention and treatment of several cancers including breast, colorectal, bladder, prostate, and oropharyngeal cancers. 40 Studies have also shown that diets characterized by higher vegetable and fruit intake are associated with reduced risk and incidence of chronic diseases, such as diabetes and cancer. 41 Higher consumption of vegetables has also been associated with an attenuated white blood cell profile, suggesting reduced markers of systemic inflammation. 42
Most survivors reported engaging in exercise at a frequency of 2 or fewer (32.3%) or 3 to 5 (36.8%) hours per week, with low exercise intensity (ie, vacuuming, walking) most frequently reported by over half (53.9%) of participants. This is consistent with previous research suggesting that in general survivors tend to engage in physical activity of lower intensity such as walking, 43 and that engagement in exercise post-treatment tends to be lower relative to pre-diagnosis. 17 However, it must be noted that these data were collected during the COVID pandemic, when frequent closures of gyms and other exercise facilities occurred. As such, survivors may have reported engaging in less physical activity than they normally would do to the challenging circumstances brought on by the pandemic.
Health Behaviours Are Associated With Specific GI Symptoms
The data revealed that antibiotic use within the past 2 years was associated with more severe belly pain, constipation, and diarrhea GI symptoms. These findings are consistent with research suggesting that antibiotic treatment is frequently associated with a myriad of GI symptoms and functional GI disorders. 44 Additionally, it is estimated that between 40% and 100% cancer patients who have been treated with chemotherapy experience GI toxicity, referred to as chemotherapy-induced intestinal mucositis, which results in painful ulceration of the GI tract, greater severity of GI symptoms such as abdominal pain and diarrhea, and compromised quality of life and treatment adherence. 45 Hence, in alignment with the pathobiological model of mucositis it is possible that some of the more severe GI symptoms reported by participants may also result from chemotherapy-induced mucositis. Addressing the pathobiology of GI mucositis could be an appropriate target for future diet-related interventions. Interestingly, probiotic use was associated with more symptoms of belly pain and gas/bloating. Although probiotic use has sometimes been associated with GI symptoms, such as gas or flatulence, it is also possible that survivors are consuming probiotics to help address these pre-existing GI symptoms. Further research is needed to understand the context within which survivors of cancer decide to use probiotic supplements.
About half (48.8%) of the participants reporting consuming 2 to 4 servings of protein per day. Our regression analysis found that lower protein consumption at 2 or fewer servings daily was actually predictive of more belly pain symptoms, suggesting that adequate protein consumption may be important for supporting gut health. However, the types of protein (eg, milk, whey, poultry, plant sources, etc.) consumed by participants in our study are unknown and could be an important factor mediating the effects of protein consumption on GI symptomology. Better self-rated diet healthiness was predictably associated with fewer GI symptoms of belly pain and gas/bloating. Specifically, we found that higher-rated diet healthiness was associated with lower symptoms of belly pain (B = −2.76, SE = 1.26, P < .03), and gas/bloating (B = −2.65, SE = 0.96, P < .01). These data provide needed evidence regarding specific dietary behaviors and the implications for survivors in experiencing, and potentially managing, GI symptoms after treatments for cancer.
Gut Microbiota Are Associated With Health Behaviours
In our small sample of participants who provided stool for gut microbiota analyses, only 3 bacterial taxa were significantly positively correlated with antibiotic use. Specifically, Lachnospiraceae (ASV-1 and 26) and Bacteroides correlated positively with antibiotic use, such that a higher abundance of taxa was present in participants who had taken antibiotics. Although Bacteroides species are abundant within the human gut microbiota and can be symbiotic with the host, under certain conditions Bacteroides can also become opportunistic pathogens. For instance, overabundance of Bacteroides vulgatus has been associated with Crohn’s disease, while Bacteroides fragilis is implicated in appendicitis and inflammatory bowel disease. 46 Considering that antibiotic treatment was identified as a predictor of GI symptoms in the present study, it is possible that antibiotic-associated changes in the gut microbiota may be a contributing factor to GI symptomology.
Concerning dietary behaviors, Lachnospiraceae was positively correlated with self-rated diet health, while Bacteroides correlated negatively with diet healthiness. Those who reported better diet health had a higher abundance of Lachnospiraceae, which is among the main producers of short-chain fatty acids 47 and a lower abundance of Bacteroides. Fruit consumption was positively correlated with both Lachnospiraceae and Subdoligranulum, such that those reporting a higher (3 -5 servings) consumption of fruit per day had a higher abundance of these bacterium. Subdoligranulum is an important species that in humans with overweight or obesity has been correlated with reduced fat mass, insulin resistance, leptin, and insulin levels, as well as attenuated levels of proinflammatory biomarkers including C-reactive protein and Interleukin-6. 48 Higher consumption (3 -5 servings per day) of whole grains was positively correlated with a higher abundance of Lachnospiraceae, while fewer servings (2 or less) of whole grains per day was associated with greater Anaerostipes abundance. This is consistent with previous studies reporting higher abundances of Anaerostipes among Chinese adults who consumed a lower intake of refined grains. 49
Regarding exercise behavior, our data suggest that it may be the frequency, rather than the intensity, impacting the gut microbiota the most. Specifically, correlation analyses found that higher exercise frequency was significantly correlated with a greater abundance of Lachnospiraceae, Faecalibacterium, Bacteroides, Anaerostipes, Alistipes, and Subdoligranulum. Previous studies suggest that Faecalibacterium prausnitzii has beneficial effects in the human microbiome and may be a novel probiotic bacterium to treat functional GI disorders, like irritable bowel syndrome. 50 Genus Alistipes is another example of a bacterium that may be symbiotic, or pathogenic, depending on the gut microbial conditions. Previous studies suggested that Alistipes may have potential protective effects against colitis, but when pathogenic it has also been associated colorectal cancer and depression. 51 While our associations between specific microbial taxa and health behaviors are intriguing, further research is needed to contextualize these findings, clarify the direction of causality, and understand the implications for cancer survivors’ health.
Limitations and Future Directions
One of the main limitations of this study is that it relied primarily on participants’ self-report measures, which tend to be subjective and prone to bias. Participants may have over or underestimated certain health behaviors, such as self-rated diet healthiness or the amount or type of whole grains consumed daily. The cross-sectional design is another limitation, since we are not able to evaluate outcomes over a period of time or to establish long-term trends, and cross-sectional designs can be prone to selection bias and confounding. Further, while some participants reported taking both a probiotic and antibiotic within the past 2 years, we are unable to determine whether these were taken at the same time points and for how long, which are factors that may affect GI symptoms. The data collected regarding daily consumption of different food groups also lacked specificity regarding the exact sources of proteins, grains, vegetables, and fruits participants consumed, which is a major limitation of this study and an important area for future research. For objective 3, a small sub-sample that provided stool samples was used. Due to the small sample size, no control for multiple comparisons was applied. Hence, there is an elevated risk for potential Type I errors. Additionally, as 16 seconds rRNA gene sequencing analysis was used, only the composition of the gut microbiota could be quantified, limiting our understanding of the potential functional capacity of the gut microbiota and how this may relate to health behaviors. Our study was also limited in terms of design. Specifically, as we did not include a control group, we were unable to compare the results of our dietary and exercise behavior outcomes to healthy peers, with the exception of PROMIS GI measures which could be compared to the PROMIS healthy population reference mean score of 50. As well, the data used for this study was collected during the COVID pandemic between December 2019 to April 2021, which may have affected diet and exercise behaviors, especially during periods where lockdowns were implemented. Participants may have been engaging in less exercise due to inaccessibility to the gym and other fitness activities they would typically engage in. Moreover, this affected our ability to collect a larger sample at multiple time points. Notably, participants experienced diverse types of cancer diagnoses and anti-cancer treatments. This heterogeneity presents challenges with determining which potential aspects of cancer diagnosis and treatments may contribute to changes in GI symptoms and the gut microbiota. Given this, our results must be interpreted with caution and future trials with larger samples and a control group for comparison are warranted.
Despite the limitations of this study, our findings provide context regarding dietary and exercise health behaviors in a diverse group of cancer survivors, and how these behaviors relate to GI symptoms. Moreover, associations between specific dietary behaviors, exercise frequency, and the gut microbiota are revealed. Our findings can inform future research aimed at using dietary or exercise-based interventions to improve GI symptoms in survivors of cancer, potentially via modulation of the microbiota-gut-brain axis. Moreover, results can be used by clinicians to support recommendations for diet and exercise in survivorship care plans, and to educate patients on the importance of healthy nutrition and the integration of physical activity. Survivors of cancer can use this information to make informed decisions about their health, in conjunction with numerous other evidence-based resources and recommendations for safe and effective use of dietary strategies and exercise after cancer.15,16,52,53
Conclusions
Overall, most survivors in this study reported consuming a moderately healthy diet and engaging in low intensity exercise a few times a week. Moreover, results provide evidence for associations between antibiotic use and more severe symptoms of belly pain, constipation, and diarrhea. Dietary behaviors including self-rated diet health, and average daily servings of protein were associated with GI symptoms. Antibiotic use, self-rated diet healthiness, fruit, whole grain consumption, and exercise frequency behaviors correlated with specific types of bacterial taxa, but the direction of causality cannot be determined by our analysis and requires further research. Behavioral and dietary-based interventions may be optimally suited to address survivors’ adverse GI symptoms by influencing the gut microbiota. However, larger, prospective trials are needed.
Acknowledgments
We wish to acknowledge and thank the participants who took the time to participate in this study and research staff in the Reimer lab for assisting with sample processing procedures.
Footnotes
List of Abbreviations: Gastrointestinal (GI); Remote Electronic Data Capture (REDCap); Electronic Data Capture (EDC); High intensity interval training (HIIT); National Institutes for Health (NIH); Patient-Reported Outcomes Measurement Information System (PROMIS); Amplicon sequence variants (ASV); Statistical Package for the Social Sciences (SPSS); Mean (M); Standard Deviation (SD); Standard Error (SE); Unstandardized Beta Coefficient (Unstd.B).
Author Contributions: Study conceptualization and methodology was completed by J.D., L.C., and R.R. Administrative and recruitment support was provided by M.B. and K.A.P. All data collection was completed by J.D., while sample processing was done by J.D., F.C., and D.L. Data analysis was completed by J.D. and O.L., while all bioinformatics were completed by F.C. The original manuscript draft preparation was done by J.D. All other authors contributed to review and revision of the final manuscript and intellectual content. L.C. was responsible for supervision and funding acquisition.
Data Availability Statement: Data is available upon reasonable written request to the corresponding author.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Enbridge Research Chair in Psychosocial Oncology, co-funded by the Canadian Cancer Society Alberta/NWT Division and the Alberta Cancer Foundation, awarded to L.E. Carlson, and by the Killam Foundation in the form of a scholarship awarded to J.M. Deleemans.
ORCID iDs: Julie M. Deleemans  https://orcid.org/0000-0001-8645-0990
https://orcid.org/0000-0001-8645-0990
Raylene A. Reimer
https://orcid.org/0000-0001-5088-7947
References
- 1. Rock CL, Thomson CA, Sullivan KR, et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J Clin. 2022;72:230-262. [DOI] [PubMed] [Google Scholar]
- 2. Canadian Cancer Society. Reduce your risk. Published 2023. Accessed February 25, 2023. https://cancer.ca/en/cancer-information/reduce-your-risk.
- 3. Canadian Cancer Society. Canadian Cancer Statistics special report 2022. Published 2023. Accessed February 27, 2023. https://cancer.ca/en/about-us/media-releases/2022/canadian-cancer-statistics-special-report-2022#:~:text=Today%2C%20it%20is%20estimated%20that,the%20importance%20of%20cancer%20prevention.
- 4. American Cancer Society. Cancer facts & figures 2022. Published 2023. Accessed February 27, 2023. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html.
- 5. Suriano F, Nyström EEL, Sergi D, Gustafsson JK. Diet, microbiota, and the mucus layer: the guardians of our health. Front Immunol. 2022;13:1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Monda V, Villano I, Messina A, et al. Exercise modifies the gut microbiota with positive health effects. Oxid Med Cell Longev. 2017;2017:1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry. 2005;18:189-193. [DOI] [PubMed] [Google Scholar]
- 8. Ding D, Van Buskirk J, Nguyen B, et al. Physical activity, diet quality and all-cause cardiovascular disease and cancer mortality: a prospective study of 346 627 UK Biobank participants. Br J Sports Med. 2022;56:1148-1156. [DOI] [PubMed] [Google Scholar]
- 9. Moazzen S, Cortes-Ibañez FO, van der Vegt B, Alizadeh BZ, de Bock GH. Diet quality indices and gastrointestinal cancer risk: results from the Lifelines study. Eur J Nutr. 2022;61:317-327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Neufeld L, Hendriks M, Hugas M. Healthy diet: a definition for the United Nations food systems summit 2021. In: von Braun J, Afsana K, Fresco LO, et al. eds. Science and Innovations for Food Systems Transformation. Springer; 2023. doi: 10.1007/978-3-031-15703-5_3 [DOI] [PubMed] [Google Scholar]
- 11. Domingo JL, Nadal M. Carcinogenicity of consumption of red meat and processed meat: A review of scientific news since the IARC decision. Food Chem Toxicol. 2017;105:256-261. [DOI] [PubMed] [Google Scholar]
- 12. Epner M, Yang P, Wagner RW, Cohen L. Understanding the link between sugar and cancer: an examination of the preclinical and clinical evidence. Cancers. 2022;14:1-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Campaniello D, Corbo MR, Sinigaglia M, et al. How diet and physical activity modulate gut microbiota: evidence, and perspectives. Nutrients. 2022;14:1-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Li Y, Lv MR, Wei YJ, et al. Dietary patterns and depression risk: a meta-analysis. Psychiatry Res. 2017;253:373-382. [DOI] [PubMed] [Google Scholar]
- 15. AIfC Research. Cancer survival. Published 2023. Accessed February 26, 2023. https://www.aicr.org/cancer-survival/.
- 16. Frenkel M, Sapire KJ, Lacey J, Zollman C, Sierpina VS. “What should I eat?”-Addressing questions and challenges related to nutrition in the Integrative Oncology Setting. Curr Oncol Rep. 2022;24:1557-1567. [DOI] [PubMed] [Google Scholar]
- 17. Murnane A, Gough K, Thompson K, Holland L, Conyers R. Adolescents and young adult cancer survivors: exercise habits, quality of life and physical activity preferences. Support Care Cancer. 2015;23:501-510. [DOI] [PubMed] [Google Scholar]
- 18. Capozzi LC, Nishimura KC, McNeely ML, Lau H, Culos-Reed SN. The impact of physical activity on health-related fitness and quality of life for patients with head and neck cancer: a systematic review. Br J Sports Med. 2016;50:325-338. [DOI] [PubMed] [Google Scholar]
- 19. Rinninella E, Raoul P, Cintoni M, et al. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms. 2019;7:1-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Berding K, Vlckova K, Marx W, et al. Diet and the microbiota-gut-brain axis: Sowing the seeds of good mental health. Adv Nutr. 2021;12:1239-1285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Zmora N, Suez J, Elinav E. You are what you eat: diet, health and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16:35-56. [DOI] [PubMed] [Google Scholar]
- 22. Bajic JE, Johnston IN, Howarth GS, Hutchinson MR. From the bottom-up: chemotherapy and gut-brain axis dysregulation. Front Behav Neurosci. 2018;12:104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Loman BR, Jordan KR, Haynes B, Bailey MT, Pyter LM. Chemotherapy-induced neuroinflammation is associated with disrupted colonic and bacterial homeostasis in female mice. Sci Rep. 2019;9:16490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Bull MJ, Plummer NT. Part 1: the human gut microbiome in health and disease. Integr Med. 2014;13:17-22. [PMC free article] [PubMed] [Google Scholar]
- 25. Sonis ST. The pathobiology of mucositis. Nat Rev Cancer. 2004;4:277-284. [DOI] [PubMed] [Google Scholar]
- 26. Deleemans JM, Chleilat F, Reimer RA, et al. The chemo-gut pilot study: associations between gut Microbiota, gastrointestinal symptoms, and psychosocial health outcomes in a cross-sectional sample of young adult cancer survivors. Curr Oncol. 2022;29:2973-2994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Deleemans JM, Toivonen K, Reimer RA, Carlson LE. The chemo-gut study: a cross-sectional survey exploring physical, mental, and gastrointestinal health outcomes in cancer survivors. Glob Adv Health Med. 2022;11:1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Deleemans JM, Chleilat F, Reimer RA, et al. The chemo-gut study: investigating the long-term effects of chemotherapy on gut microbiota, metabolic, immune, psychological and cognitive parameters in young adult cancer survivors; study protocol. BMC Cancer. 2019;19:1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. PROMIS Health Organization. PROMIS® patient-reported outcomes measurement information system®. Published 2022. https://www.promishealth.org/57461-2/, 2018-2022.
- 30. Cessna JM, Jim HS, Sutton SK, et al. Evaluation of the psychometric properties of the PROMIS Cancer fatigue short form with cancer patients. J Psychosom Res. 2016;81:9-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kochar B, Martin CF, Kappelman MD, et al. Evaluation of gastrointestinal patient reported outcomes measurement information system (GI-PROMIS) symptom scales in subjects with inflammatory bowel diseases. Am J Gastroenterol. 2018;113:72-79. [DOI] [PubMed] [Google Scholar]
- 32. Spiegel BMR, Hays RD, Bolus R, et al. Development of the NIH patient-reported outcomes measurement information system (PROMIS) gastrointestinal symptom scales. Am J Gastroenterol. 2014;109:1804-1814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Callahan BJ, McMurdie PJ, Rosen MJ, et al. DADA2: high-resolution sample inference from illumina amplicon data. Nat Methods. 2016;13:581-583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Quast C, Pruesse E, Yilmaz P, et al. The SILVA ribosomal RNA gene database project: improved data processing and web-based tools. Nucleic Acids Res. 2013;41:D590-D596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. May J, Looney SW. Sample size charts for Spearman and Kendall coefficients. Biometrics & Biostatistics. 2020;11:1-7. [Google Scholar]
- 36. PHMN University. PROMIS® score cut points. Published 2023. Accessed February 24, 2023. https://www.healthmeasures.net/score-and-interpret/interpret-scores/promis/promis-score-cut-points.
- 37. Hays RD, Spritzer KL, Thompson WW, Cella D. U.S. General population estimate for "Excellent" to "poor" self-rated Health Item. J Gen Intern Med. 2015;30:1511-1516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Pekmezi DW, Demark-Wahnefried W. Updated evidence in support of diet and exercise interventions in cancer survivors. Acta Oncol. 2011;50:167-178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Canada H. Eating well with Canada food guide. Ottawa, Canada. 2023. [Google Scholar]
- 40. Nandini DB, Rao RS, Deepak BS, Reddy PB. Sulforaphane in broccoli: the green chemoprevention!! Role in cancer prevention and therapy. J Oral Maxillofac Pathol. 2020;24:405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. van der Merwe M. Gut microbiome changes induced by a diet rich in fruits and vegetables. Int J Food Sci Nutr. 2021;72:665-669. [DOI] [PubMed] [Google Scholar]
- 42. Menni C, Louca P, Berry SE, et al. High intake of vegetables is linked to lower white blood cell profile and the effect is mediated by the gut microbiome. BMC Med. 2021;19:37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Wong JN, McAuley E, Trinh L. Physical activity programming and counseling preferences among cancer survivors: a systematic review. Int J Behav Nutr Phys Act. 2018;15:48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Karakan T, Ozkul C, Küpeli Akkol E, et al. Gut-brain-microbiota axis: antibiotics and functional gastrointestinal disorders. Nutrients. 2021;13:1-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Dahlgren D, Sjöblom M, Hellström PM, Lennernäs H. Chemotherapeutics-induced intestinal mucositis: pathophysiology and potential treatment strategies. Front Pharmacol. 2021;12:1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Zafar H, Saier Mh, Jr. Gut bacteroides species in health and disease. Gut Microbes. 2021;13:1-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Vacca M, Celano G, Calabrese FM, et al. The controversial role of human gut lachnospiraceae. Microorganisms. 2020;8:1-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Van Hul M, Le Roy T, Prifti E, et al. From correlation to causality: the case of subdoligranulum. Gut Microbes. 2020;12:1-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Zhang Y, Chen H, Lu M, et al. Habitual diet pattern associations with gut microbiome diversity and composition: results from a Chinese adult cohort. Nutrients. 2022;14:1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Miquel S, Martín R, Rossi O, et al. Faecalibacterium prausnitzii and human intestinal health. Curr Opin Microbiol. 2013;16:255-261. [DOI] [PubMed] [Google Scholar]
- 51. Parker BJ, Wearsch PA, Veloo ACM, Rodriguez-Palacios A. The genus Alistipes: gut bacteria with emerging implications to inflammation, cancer, and Mental Health. Front Immunol. 2020;11:906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. FHC Center. Cook for your life. Published 2023. Accessed February 26, 2023. https://www.cookforyourlife.org/.
- 53. WCRF International. Diet, activity | cancer. Published 2023. Accessed February 26, 2023. https://www.wcrf.org/diet-activity-and-cancer/.