

Abstract
Objectives:
Mesonephric (MA) and mesonephric-like (MLA) adenocarcinomas are rare cancers, and data on clinical behavior and response to therapy are limited. We sought to report molecular features, treatment, and outcomes of MA/MLA from a single institution.
Methods:
Patients with MA (cervix) or MLA (uterus, ovary, other) treated at Memorial Sloan Kettering Cancer Center (MSK) from 1/2008–12/2021 underwent pathologic re-review. For patients with initial treatment at MSK, progression-free survival (PFS1) was calculated as time from initial surgery to progression or death; second PFS (PFS2) was calculated as time from start of treatment for recurrence to subsequent progression or death. Overall survival (OS) was calculated for all patients. Images were retrospectively reviewed to determine treatment response. Somatic genetic alterations were assessed by clinical tumor-normal sequencing (MSK-Integrated Mutation Profiling of Actionable Cancer Targets [MSK-IMPACT]).
Results:
Of 81 patients with confirmed gynecologic MA/MLA, 36 received initial treatment at MSK. Sites of origin included cervix (n=9, 11%), uterus (n=42, 52%), ovary (n=28, 35%), and other (n=2, 2%). Of the 36 patients who received initial treatment at MSK, 20 (56%) recurred; median PFS1 was 33 months (95% CI: 17-not evaluable), median PFS2 was 8.3 months (95% CI: 6.9–14), and median OS was 87 months (95% CI: 58.2-not evaluable). Twenty-six of the 36 patients underwent MSK-IMPACT testing, and 25 (96%) harbored MAPK pathway alterations.
Conclusion:
Most patients diagnosed with early-stage disease ultimately recurred. Somatic MAPK signaling pathway mutations appear to be highly prevalent in MA/MLA, and therapeutics that target this pathway are worthy of further study.
Keywords: mesonephric adenocarcinoma, mesonephric-like adenocarcinoma, MAPK, KRAS
Introduction
Mesonephric adenocarcinoma (MA) and mesonephric-like adenocarcinoma (MLA) of the gynecologic tract are rare cancers that frequently harbor alterations in mitogen-activated protein kinase (MAPK) pathway-related genes, most commonly in KRAS [1–4]. MA occurs in the uterine cervix, is not associated with human papillomavirus, and arises from mesonephric (Wolffian) duct remnants within the deep cervical wall [5–8]. MLA arises in the uterine corpus, ovary, para-adnexal soft tissue, or vagina [9–14], typically does not have identifiable Wolffian duct remnant origins, and is thought to arise from transdifferentiation of Mullerian epithelium, including endometriosis [15]. MA and MLA are histologically similar, often express GATA3, thyroid transcription factor-1 (TTF-1; particularly MLA), calretinin, and luminal CD10, and are generally estrogen receptor and progesterone receptor negative, or at most focally positive (Figure 1) [3].
Figure 1: Histologic features of mesonephric adenocarcinoma (MA) and mesonephric-like adenocarcinoma (MLA) of gynecologic origin.
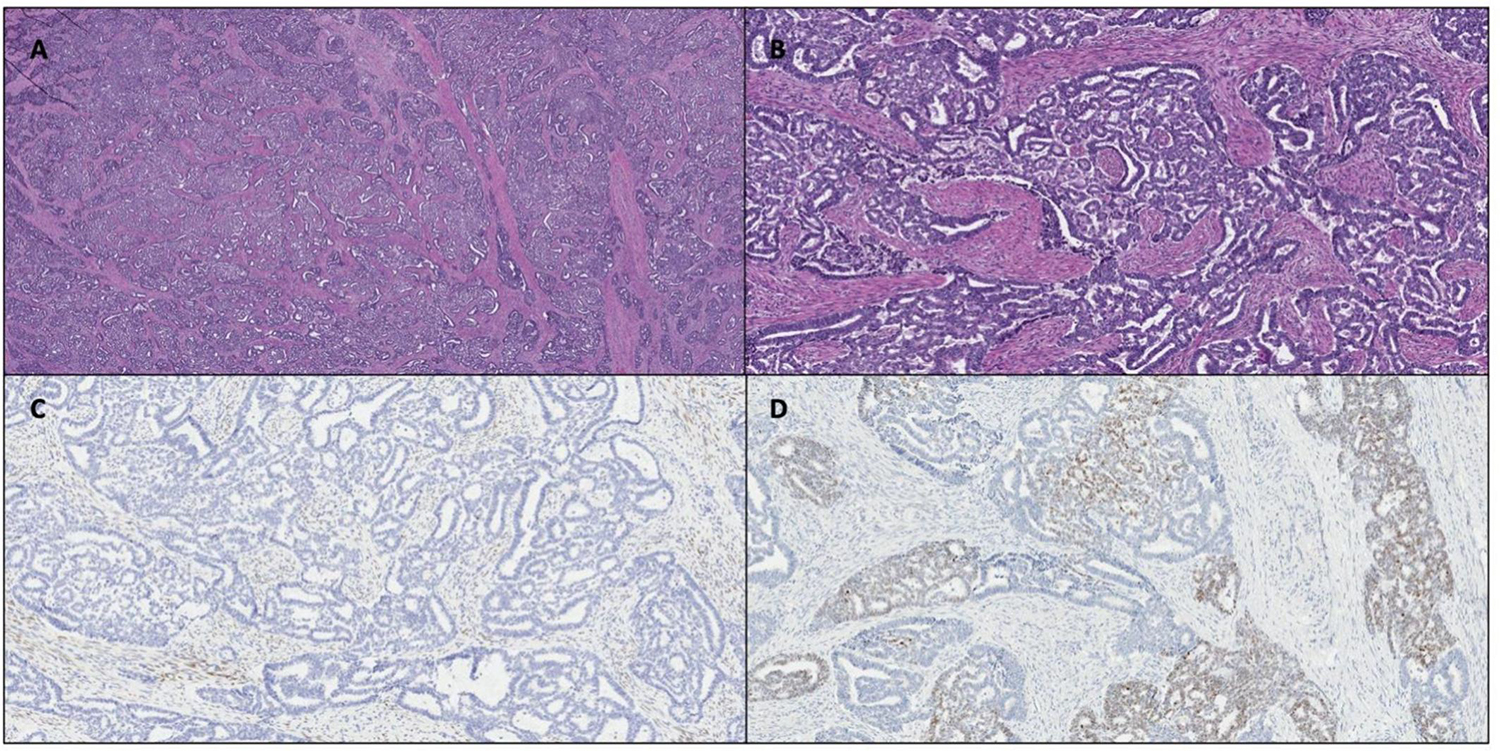
Representative hematoxylin-and-eosin photomicrographs of MA and MLA of gynecologic origin. A) MLA of the endometrium, 2X magnification. B) MLA of the endometrium, 10X magnification. C) Progesterone receptor completely negative in tumor with positive internal control of myometrium. D) Thyroid transcription factor 1 (TTF1) positive in tumor cell nuclei.
To date, no prospective therapeutic studies have been completed in patients with MA or MLA of gynecologic origin. We aim to describe the molecular features, response to treatment, and oncologic outcomes for patients with MA or MLA of gynecologic origin who were treated at a single institution.
Methods
Case selection
Patients with MA (cervix) or MLA (uterus, ovary, other) treated at Memorial Sloan Kettering Cancer Center (MSK) from January 1, 2008, to December 31, 2021, were retrospectively identified using a natural language search in the institutional pathology database, as well as a review of the institutional clinical database using the keywords “mesonephric” and “mesonephric-like.” Cases were only included if the tumors had typical mesonephric morphology with supporting immunohistochemical expression patterns (ie, hormone receptor-negative status, or at most focal/weak, and positive GATA3 or TTF1 status). Slides or digitally scanned images underwent histologic re-review and confirmation of pathology by an expert gynecologic pathologist (KP), and clinical characteristics, treatment regimens, and oncologic outcomes were obtained from medical records. The prior Pors et al publication [3] included 48 cases from MSK, and this analysis included 39 cases not previously published.
Molecular features
Somatic mutation and copy number alteration status were obtained from the clinical US Food and Drug Administration (FDA)-authorized tumor-normal sequencing panel, MSK-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) [16].
Radiologic assessment of treatment response
Computed tomography images were retrospectively reviewed by an expert radiologist (JG) using Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 to determine response to therapy for patients with available radiology images [17]. Waterfall plots of percent change in tumor size following first-line treatment for recurrence were generated for each origin of MA and MLA (uterus, cervix, ovary).
Statistical analysis
For the entire cohort (including patients who received initial treatment at MSK), progression-free survival (PFS1) was calculated as the time from initial surgery to progression (as determined by the treating physician) or death. Second PFS (PFS2) was calculated as the time from start of treatment for recurrence to subsequent progression (as determined by the treating physician) or death. Overall survival (OS) was calculated as the time from surgery to the date of last follow-up or death. Median PFS1, PFS2, and OS were estimated using the Kaplan-Meier method, and the 95% confidence intervals were reported. Median follow-up was estimated using the reverse Kaplan-Meier method, which is calculated by reversing the censor and event status of patients. All analyses were performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinicopathologic features and treatment of patients with gynecologic MA or MLA
A total of 81 patients were confirmed to have gynecologic MA or MLA, 36 (44%) of whom received initial surgical management and treatment at our institution. Table 1 describes the demographic and clinicopathologic characteristics of the entire cohort. For the overall cohort, median age at MA/MLA diagnosis was 60 years (IQR, 53–67 years). MA in the cervix was diagnosed in 9 patients (11%) and MLA in 72 patients (89%). Gynecologic site of origin for MLA was most commonly the uterus (n=42, 52%), followed by the ovary (n=28, 35%), and other (Mullerian not otherwise specified; n=2, 2%). Among the 42 cases of uterine MLA, 29 had mixed histology noted on the pathology report. Of these mixed histology tumors, 20 included endometrioid, 8 carcinosarcoma, and 1 clear cell. Among the 28 cases of ovarian MLA, 20 had mixed histology noted on the pathology report. Of these mixed histology tumors, 10 included endometrioid, 4 mucinous features or mucinous borderline, 3 carcinosarcoma, 2 serous borderline, and 1 low-grade serous.
Table 1:
Characteristics of patients with mesonephric or mesonephric-like adenocarcinoma of the gynecologic tract.
| Characteristic | N = 81 n (%) |
|||
|---|---|---|---|---|
| Median age at diagnosis (interquartile range), years | 60 (53, 67) | |||
| Type of adenocarcinoma | ||||
| Mesonephric | 9 (11%) | |||
| Mesonephric-like | 72 (89%) | |||
| Site of origin | ||||
| Cervix | 9 (11%) | |||
| Uterus | 42 (52%) | |||
| Ovary | 28 (35%) | |||
| Other | 2 (2%) | |||
| Surgical stage at diagnosis | All | Cervix | Uterus | Ovary |
| I | 38 (47.5%) | 4 (11%) | 19 (50%) | 15 (39%) |
| II | 10 (12.5%) | 3 (30%) | 5 (50%) | 2 (20%) |
| III | 21 (26%) | 2 (10%) | 11 (52%) | 8 (38%) |
| Characteristic | N = 81 n (%) |
|||
| IV | 11 (14%)* | 0 | 6 (55%) | 3 (27%) |
| Unknown | 1 | 0 | 1 (100%) | 0 |
| Intent of first systemic treatment | ||||
| No treatment | 15 (19%) | |||
| Adjuvant | 57 (70%) | |||
| Palliative | 6 (7%) | |||
| Neoadjuvant | 3 (4%) | |||
| Residual disease after primary surgery | ||||
| No | 72 (97%) | |||
| Yes | 2 (3%) | |||
| Unknown | 7 | |||
| Radiation as part of initial treatment | ||||
| No | 46 (58%) | |||
| Yes | 34 (42%) | |||
| Unknown | 1 | |||
2 cases are of other Mullerian origin not otherwise specified.
Among the entire cohort, 58 patients (72%) had recurrent disease, most commonly in the lung (n=28, 48%) (Table 2). Among the 36 patients who were initially treated at our institution, 20 (56%) recurred (Table 2). Initial recurrence rates (PFS1) were high regardless of stage at presentation. Median PFS1 rate at 24 months for the 36 patients who underwent initial treatment at MSK, by stage, was 71% (95% CI: 52%–96%) for stage I, 67% (95% CI: 30%–100%) for stage II, 27% (95% CI: 8.9%–80%) for stage III, and 50% (95% CI: 19%–100%) for stage IV disease (Figure 2). For the 20 patients with recurrent disease who received initial treatment at MSK, 11 (55%) received platinum-based systemic treatment, 2 (10%) received liposomal doxorubicin with or without bevacizumab, 2 (10%) underwent secondary cytoreductive surgery, 1 (5%) received immunotherapy, 1 (5%) enrolled on a clinical trial, 1 (5%) received hormonal treatment, 1 (5%) received targeted therapy (temsirolimus), and 1 (5%) received unknown treatment (Table 2). One patient received an MEK inhibitor.
Table 2:
Characteristics of patients with recurrent mesonephric or mesonephric-like adenocarcinoma of the gynecologic tract.
| Characteristic | n (%) |
|---|---|
| Site of first recurrence, all patients (N=58) | |
| Vagina | 5 (9%) |
| Abdomen/pelvis | 24 (41%) |
| Lung | 28 (48%) |
| Bone | 1 (2%) |
| Treatment regimen for first recurrence, patients with initial care at MSK (N=20) | |
| Platinum-based systemic treatment | 11 (55%) |
| Liposomal doxorubicin with or without bevacizumab | 2 (10%) |
| Immunotherapy | 1 (5%) |
| Clinical trial | 1 (5%) |
| Hormonal treatment | 1 (5%) |
| Targeted therapy (temsirolimus) | 1 (5%) |
| Secondary cytoreductive surgery | 2 (10%) |
| Unknown | 1 |
MSK, Memorial Sloan Kettering Cancer Center
Figure 2: Kaplan-Meier curve demonstrating progression-free survival for first recurrence (PFS1) for patients with mesonephric and mesonephric-like adenocarcinoma of gynecologic origin who received initial care at Memorial Sloan Kettering Cancer Center (MSK), by initial stage.

PFS1 was calculated as the time from surgery to progression (as determined by treating physician) or death.
Outcomes for patients initially treated at our institution
Median follow-up for the entire cohort was 64.9 months (95% CI: 56.5–98.5 months). Among all 81 patients, median OS was 83.8 months (95% CI: 73-not evaluable [NE]). For the 36 patients who received initial treatment at MSK, median follow-up was 55.8 months (95% CI: 46.8–73.3 months). Median PFS1 and PFS2 were 33 months (95% CI: 17-NE) and 8.3 months (95% CI: 6.9–14 months), respectively (Figures 3A and 3B). Median OS was 87 months (95% CI: 58-NE) (Figure 3C).
Figure 3: Kaplan-Meier curves demonstrating A) progression-free survival (PFS1), B) second PFS (PFS2), and C) overall survival (OS) for all patients with mesonephric or mesonephric-like adenocarcinoma of gynecologic origin who received initial care at Memorial Sloan Kettering Cancer Center (MSK).

PFS1 was calculated as the time from surgery to progression (as determined by treating physician) or death. PFS2 was calculated as the time from start of treatment for recurrence to progression (as determined by treating physician) or death. OS was calculated as the time from surgery to death or last follow-up.
Treatment response in patients initially treated at our institution
Response to systemic therapy at time of first recurrence is displayed in the waterfall plots shown in Supplementary Figure S1.
Uterine MLA
Fourteen patients with uterine MLA were evaluable; 9 received platinum-doublet chemotherapy, 3 received immunotherapy, 1 received hormonal therapy, and 1 received targeted therapy. The response rate among the 9 patients treated with platinum-doublet chemotherapy was 77.8% (n=7; 1 complete and 6 partial responses). Patients who received both targeted (temsirolimus) and hormonal therapies had a best response of stable disease. The 3 patients who received immunotherapy demonstrated a best response of progression of disease (POD), though notably all had mismatch repair-proficient disease and/or had a low tumor mutational burden. For the patients with uterine MLA and initial treatment at MSK, median PFS2 was 8.4 months (95% CI: 6.9-NE).
Ovarian MLA
Among the 7 patients with ovarian MLA who were evaluable, 4 received platinum-doublet chemotherapy, 1 received platinum-doublet therapy with bevacizumab, 1 received chemotherapy with bevacizumab, and 1 received immunotherapy. No patients had a CR. Of the 4 patients who received platinum-doublet chemotherapy, 1 (25%) had a PR, 2 (50%) had SD, and 1 (25%) had POD. The remaining 3 patients had SD on platinum-doublet therapy with bevacizumab treatment, chemotherapy and bevacizumab, and immunotherapy, respectively. For the patients with ovarian MLA who received initial treatment at MSK, the median PFS2 was 7.9 months (95% CI: 3.9-NE).
Cervical MA
Three patients with cervical MA were evaluable. No patients had a CR or PR. The patient who received platinum-doublet therapy and the patient who received immunotherapy (and notably had programmed death-ligand 1 [PD-L1]-positive immunohistochemistry [IHC]) had SD. The patient on platinum-doublet therapy progressed after 5 months on treatment, and the patient on immunotherapy progressed after 22 months on treatment. The patient who enrolled on a clinical trial demonstrated a best response of POD.
Molecular features of MA and MLA
Twenty-six (72%) of the 36 patients who were initially treated at our institution underwent clinical molecular profiling via MSK-IMPACT. All but 1 MA/MLA harbored MAPK pathway alterations (n=25, 96%), including KRAS (n=20, 77%) or NRAS (n=3, 11%) hotspot missense mutations, HRAS amplification (n=1, 4%), or a NF1 truncating mutation (n=1, 4%) (Figure 4). MAPK pathway alterations were generally mutually exclusive, except for 1 ovarian MLA that harbored both a hotspot KRAS and a hotspot NRAS mutation. PIK3CA hotspot mutations were found in 5 (30%) of 15 uterine MLAs and in 3 (30%) of 9 ovarian MLAs (Figure 4).
Figure 4: Oncoprint showing recurrent somatic genetic alterations and gene copy number alterations in mesonephric adenocarcinoma (MA) and mesonephric-like adenocarcinoma (MLA) of gynecologic origin.

Cases are sorted in columns by site of origin, genes in rows, color coded by the legend. Information on mesonephric type, surgical stage, and tissue type (primary/recurrence) are shown in the phenobar on top.
*Case harbors a POLE hotspot mutation.
MAPK, mitogen-activated protein kinase; SNV, single-nucleotide variant
Discussion
Here, we report on the molecular features, recurrent treatment paradigms, and oncologic outcomes of patients with MA or MLA of gynecologic origin from a single institution. Our data demonstrate that 96% of these tumors harbored an MAPK pathway alteration. Recurrent disease most commonly occurred in the lung (48%), and once recurrent, median PFS2 was 8.3 months.
A large retrospective study of 99 patients with MA or MLA of gynecologic origin found similarly poor oncologic outcomes as our study [3]. While our institution contributed cases to this large retrospective study, in the current study, we focused on patients who underwent initial treatment at MSK and expanded upon systemic therapy response and molecular findings. Consistent with our results, Pors et al demonstrated a high rate of patients who presented with advanced-stage disease (II-IV); 60% of patients had cervical MA, 58% had uterine MLA, and 39% had ovarian MLA [3]. Pors et al also demonstrated a high recurrence rate of 52% among the entire cohort, which is consistent with our finding of a 56% recurrence rate in the cohort of patients who received initial treatment at MSK. Importantly, congruent with Pors et al and other retrospective studies, our data demonstrate a propensity of recurrences in the lung [1–3, 9]. Our finding of a median PFS2 of 8.3 months for patients who underwent initial treatment at MSK supports prior analyses showing PFS is limited in the setting of recurrence [3, 10–12].
Beyond clinicopathologic characteristics and oncologic outcomes, we assessed response to systemic treatment in the recurrent setting for this rare histology. Immunotherapy, even in 1 patient with cervical MA and positive PD-L1 IHC, did not result in tumor regression. In a case report, Montagut et al reported on a patient with recurrent uterine MLA as well as a review of the available literature on systemic treatment response in mesonephric gynecologic cancer [18]. The patient was diagnosed with recurrence (in the lungs and peritoneum) 10 months after initial surgical management and demonstrated a durable response to carboplatin and paclitaxel. Though limited by a small sample, our data support the use of platinum-based chemotherapy for patients with uterine MLA. The limited PFS observed, however, indicates a need for improved therapeutics in this rare subset of gynecologic cancers.
MA and MLA of gynecologic origin demonstrate nearly ubiquitous somatic alterations in the MAPK signaling pathway. In our study, 96% of patients with MA or MLA of gynecologic origin had a somatic alteration in the MAPK signaling pathway, with most having a somatic KRAS mutation. Similarly, da Silva et al found a high prevalence of somatic alterations in the MAPK signaling pathway in patients with MA or MLA of gynecologic origin; 89% of patients had alterations in KRAS, 7% in NRAS, and 4% in BRAF [2]. Importantly, da Silva et al demonstrated that mutations affecting the RAS/MAPK family of genes were clonal throughout the metastatic process when comparing primary and paired metastatic samples [2]. This evidence, which is concordant with our results demonstrating poor PFS in the recurrent setting, suggests patients with MA or MLA may benefit from therapy targeting the MAPK signaling pathway.
Low-grade serous ovarian carcinoma (LGSOC) is a rare type of ovarian cancer characterized by a high prevalence of somatic MAPK pathway alterations, most commonly in KRAS, which is altered in one-third of LGSOC tumors [19–21]. Multiple recent studies of single-agent MEK inhibitors in LGSOC have shown promising results, particularly in patients with a KRAS mutation, in whom the response rate to treatment with binimetinib was 44% [22, 23]. A similar strategy may be beneficial for patients with MA or MLA. Combination strategies have also shown promising results in patients with LGSOC, particularly in those harboring a KRAS mutation [24]. The combination of VS-6766 and defactinib showed encouraging response with durability across patients with LGSOC, with response rates of 46% in all patients and 64% in patients with KRAS-mutated LGSOC [24].
Strengths of this study include the large cohort of 81 patients, including 36 patients who underwent initial treatment at our institution. Despite this being one of the largest retrospective studies of this rare histology, the sample included in this analysis was small, which makes it difficult to interpret oncologic outcomes and tumor responses to systemic treatments. This study is also limited by its retrospective nature, specifically the retrospective radiologic image review to determine tumor response to treatment. Moreover, the treatment regimen was at the discretion of the treating physician, and therefore it was likely focused on the gynecologic organ of origin rather than mesonephric histology.
Ultimately, prospective data on response to systemic therapy for patients with MA or MLA of gynecologic origin are limited. In our study, 56% of patients who received initial treatment at our institution demonstrated recurrence, most commonly involving the lung. Importantly, there appears to be a high prevalence of MAPK pathway alterations in MA and MLA tumors. Therapies targeting the MAPK pathway recently have shown promising results in other rare gynecologic cancers with a high prevalence of KRAS mutations and are worthy of further study in MA and MLA of gynecologic origin. Toward this end, a single-institution study (NCT05787561) of the dual MEK/RAF inhibitor avutometinib in combination with the FAK inhibitor defactinib in patients with recurrent MA or MLA of gynecologic origin is currently accruing patients.
Supplementary Material
Highlights.
Mesonephric adenocarcinoma (MA) and mesonephric-like adenocarcinoma (MLA) of gynecologic origin are rare cancers.
The majority of patients who presented with early-stage disease ultimately recurred, typically in the lung.
Somatic MAPK signaling pathway mutations are highly prevalent in MA and MLA.
Therapeutics that target the MAPK signaling pathway are worthy of further study in MA and MLA of gynecologic origin.
Funding
This research was funded in part by the National Institutes of Health/National Cancer Institute Cancer Center Support Grant P30 CA008748.
Footnotes
Conflicts of Interest
B. Weigelt reports research funding by Repare Therapeutics, outside the current work. N. R. Abu-Rustum reports grant funding from GRAIL paid to the institution. A. Iasonos reports consulting fees from Mylan. C. Aghajanian reports clinical trial funding paid to the institution from AstraZeneca; consulting fees (advisory board) from Eisai/Merck, Roche/Genentech, Abbvie, AstraZeneca/Merck, and Repare Therapeutics; advisory board participation (no fee) for Blueprint Medicine; and leadership/fiduciary roles for the GOG Foundation Board of Directors (travel cost reimbursement) and NRG Oncology Board of Directors (unpaid). D. Chi reports personal fees from Apyx Medical, Verthermia Inc., Biom ‘Up, and AstraZeneca, as well as recent or current stock/options ownership of Apyx Medical, Verthemia, Intuitive Surgical, Inc., TransEnterix, Inc., Doximity, Moderna, and BioNTech SE. R.N. Grisham reports honoraria from GSK, AstraZeneca, Natera, Springworks, Corcept, MJH, and PER. The other authors do not have potential conflicts of interest to declare.
Accepted as a poster presentation at the Society of Gynecologic Oncology Annual Meeting, March 2023, Tampa, FL, USA
Consent Statement
This retrospective study was approved by the Institutional Review Board at Memorial Sloan Kettering Cancer Center, and all patients provided written consent.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Anagnostopoulos A, Ruthven S, and Kingston R, Mesonephric adenocarcinoma of the uterine cervix and literature review. BMJ Case Rep, 2012. 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.da Silva EM, et al. , Mesonephric and mesonephric-like carcinomas of the female genital tract: molecular characterization including cases with mixed histology and matched metastases. Mod Pathol, 2021. 34(8): p. 1570–1587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pors J, et al. , Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study. Am J Surg Pathol, 2021. 45(4): p. 498–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mirkovic J, et al. , Targeted Genomic Profiling Reveals Recurrent KRAS Mutations in Mesonephric-like Adenocarcinomas of the Female Genital Tract. Am J Surg Pathol, 2018. 42(2): p. 227–233. [DOI] [PubMed] [Google Scholar]
- 5.Clement PB, et al. , Malignant mesonephric neoplasms of the uterine cervix. A report of eight cases, including four with a malignant spindle cell component. Am J Surg Pathol, 1995. 19(10): p. 1158–71. [DOI] [PubMed] [Google Scholar]
- 6.Dierickx A, et al. , Mesonephric adenocarcinoma of the cervix: Case report and literature review. Gynecol Oncol Rep, 2016. 17: p. 7–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ferry JA and Scully RE, Carcinoma in mesonephric remnants. Am J Surg Pathol, 1995. 19(10): p. 1218–9. [DOI] [PubMed] [Google Scholar]
- 8.Kenny SL, et al. , Mesonephric adenocarcinomas of the uterine cervix and corpus: HPV-negative neoplasms that are commonly PAX8, CA125, and HMGA2 positive and that may be immunoreactive with TTF1 and hepatocyte nuclear factor 1-beta. Am J Surg Pathol, 2012. 36(6): p. 799–807. [DOI] [PubMed] [Google Scholar]
- 9.Bague S, Rodriguez IM, and Prat J, Malignant mesonephric tumors of the female genital tract: a clinicopathologic study of 9 cases. Am J Surg Pathol, 2004. 28(5): p. 601–7. [DOI] [PubMed] [Google Scholar]
- 10.Euscher ED, et al. , Mesonephric-like Carcinoma of the Endometrium: A Subset of Endometrial Carcinoma With an Aggressive Behavior. Am J Surg Pathol, 2020. 44(4): p. 429–443. [DOI] [PubMed] [Google Scholar]
- 11.Horn LC, et al. , Mesonephric-like adenocarcinomas of the uterine corpus: report of a case series and review of the literature indicating poor prognosis for this subtype of endometrial adenocarcinoma. J Cancer Res Clin Oncol, 2020. 146(4): p. 971–983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kim HG, et al. , Mesonephric-like Adenocarcinoma of the Uterine Corpus: Comprehensive Analyses of Clinicopathological, Molecular, and Prognostic Characteristics With Retrospective Review of 237 Endometrial Carcinoma Cases. Cancer Genomics Proteomics, 2022. 19(4): p. 526–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Na K and Kim HS, Clinicopathologic and Molecular Characteristics of Mesonephric Adenocarcinoma Arising From the Uterine Body. Am J Surg Pathol, 2019. 43(1): p. 12–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wu H, et al. , Mesonephric adenocarcinoma of the uterine corpus. Int J Clin Exp Pathol, 2014. 7(10): p. 7012–9. [PMC free article] [PubMed] [Google Scholar]
- 15.Chang CS, Carney ME, and Killeen JL, Two Cases of Mesonephric-like Carcinoma Arising From Endometriosis: Case Report and Review of the Literature. Int J Gynecol Pathol, 2023. 42(1): p. 101–107. [DOI] [PubMed] [Google Scholar]
- 16.Zehir A, et al. , Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat Med, 2017. 23(6): p. 703–713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eisenhauer EA, et al. , New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer, 2009. 45(2): p. 228–47. [DOI] [PubMed] [Google Scholar]
- 18.Montagut C, et al. , Activity of chemotherapy with carboplatin plus paclitaxel in a recurrent mesonephric adenocarcinoma of the uterine corpus. Gynecol Oncol, 2003. 90(2): p. 458–61. [DOI] [PubMed] [Google Scholar]
- 19.Grisham R, Garg K, Zhou Q, Iasonos A, Berger M, Dao F, Hyman D, Levine D, Solit D, Aghajanian C, Iyer G, A comprehensive analysis of BRAF and KRAS mutation status in low-grade serous (LGS) and serous borderline (SB) ovarian cancer J Clin Oncol 2012. suppl; abstr 5030 [Google Scholar]
- 20.Grisham RN, et al. , BRAF mutation is associated with early stage disease and improved outcome in patients with low-grade serous ovarian cancer. Cancer, 2013. 119(3): p. 548–554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Grisham RN, et al. , Extreme Outlier Analysis Identifies Occult Mitogen-Activated Protein Kinase Pathway Mutations in Patients With Low-Grade Serous Ovarian Cancer. J Clin Oncol, 2015. 33(34): p. 4099–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gershenson DM, et al. , Trametinib versus standard of care in patients with recurrent low-grade serous ovarian cancer (GOG 281/LOGS): an international, randomised, open-label, multicentre, phase 2/3 trial. Lancet, 2022. 399(10324): p. 541–553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Monk BJ, et al. , MILO/ENGOT-ov11: Binimetinib Versus Physician’s Choice Chemotherapy in Recurrent or Persistent Low-Grade Serous Carcinomas of the Ovary, Fallopian Tube, or Primary Peritoneum. J Clin Oncol, 2020. 38(32): p. 3753–3762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.S Banerjee RG, Shinde R, Lima J, Krebs M, Rahman R, Little M, Tunariu N, Curcean A, Badham H, Mahmud M, Turner A, Parmar M, Yap C, Minchom A, Lopez J, de Bono J, Banerji U, Phase I study of the combination of the dual RAF/MEK inhibitor VS-6766 and the FAK inhibitor defactinib: Results of efficacy in low grade serous ovarian cancer. Annals of Oncology, 2021. 32: p. S725–S772. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.