

Abstract
Background: Opioid-induced constipation (OIC) is a pervasive and distressing side effect of chronic opioid therapy in patients with cancer pain, significantly impacting their quality of life. Peripherally acting μ-opioid receptor antagonists (PAMORAS) were developed for treatment-resistant OIC but most studies were conducted with non-cancer patients. Objective: to discuss two oral formulations of PAMORAs, naldemedine and naloxegol, and to review available evidence of the effectiveness of these drugs for OIC in cancer patients. Methods: a comprehensive search to identify primary literature for either naldemedine or naloxegol for OIC in cancer patients. Results: Only three prospective randomized, double-blind, placebo-controlled clinical trials for naldemedine enrolling cancer patients were identified; the results of a subgroup analysis of two of those studies and two non-interventional post marketing surveillance studies of these trials are also reported here. For naloxegol, only two randomized controlled trials were identified; both were unsuccessful in enrolling sufficient patients. An additional four prospective non-interventional observational studies with naloxegol were found that enrolled cancer patients. There were significantly higher rates of responders in the PAMORA groups than in the placebo groups. The most common side effect for both PAMORAs was diarrhea. Limitations: All studies were industry-funded, and given that only three trials were randomized controlled studies, the overall quality of the studies was lacking. Conclusion: Naldemedine or naloxegol appeared safe and useful in the treatment of OIC in cancer patients and may improve their quality of life. Larger-scale randomized placebo-controlled studies of PAMORAs in cancer patients would strengthen existing evidence.
Keywords: naldemedine, naloxegol, opioid-induced constipation, obstipation, cancer patients
1. Introduction
Opioid-induced constipation (OIC) is a disabling symptom which 60–90 percent of cancer patients with chronic opioid use experience [1,2,3,4]. Opioids bring about analgesia largely by binding to μ-receptors in the central nervous system, but they also bind to the μ-receptor in the myenteric plexus in the gastrointestinal tract, leading to the adverse side effect of constipation by decreasing intestinal motility, increasing fluid and electrolyte absorption in the small intestine and the colon, while also increasing the anal sphincter tone [1,2,3,4]. This can lead to more water absorption from the feces resulting in hard and dry stool. OIC has been defined by the Rome IV criteria as worsening symptoms of constipation when initiating, changing, or increasing opioid therapy, and it must include at least two of the following: fewer than three spontaneous bowel movements per week, straining during more than one-fourth of defecations, lumpy or hard stools in more than one-fourth of defecations, sensation of incomplete evacuation in more than one-fourth of defecations, or manual maneuvers to facilitate more than one-fourth of defecations (e.g., digital evacuation, support of the pelvic floor) [5,6].
Peripherally acting μ-opioid receptor antagonists (PAMORAs) are a class of medications aiming to reverse opioids’ adverse effects on the gut by interacting with opioid receptors in the gastrointestinal tract without significantly crossing the blood–brain barrier, and therefore they are not affecting the analgesic opioid effects in the central nervous system [7,8,9,10,11,12]. They are different from classic laxatives as, by their mechanism, they are targeted therapies for OIC. PAMORAs have been approved in the US by the Federal Drug Administration for OIC in patients with chronic non-cancer pain [13,14], and in Europe by the European Medicines Agency for use in patients with or without cancer [15,16]. In the US, naloxegol [12.5, 25 mg] was approved in September 2014, and naldemedine [0.1, 0.2 mg] was approved in March 2017 [13,14]. Patients with OIC can suffer greatly from reduced quality of life, as some may reduce their opioid dose in attempts to ease the OIC, leading to inadequate analgesia and a vicious circle without adequate relief of OIC. The American Gastroenterological Association published guidelines for the management of OIC [17], and other societies have published guidelines for the management of constipation in patients with cancer which specifically target OIC by including PAMORAs [18,19].
The objective of this review was to describe available primary literature on the use of oral naldemedine (sold as Symproic® in the US or Rizmoic® in the European Union) and oral naloxegol (sold as Movantik® or Moventig®), specifically in cancer patients.
1.1. Mechanism of Action
PAMORAs are used in the treatment of opioid-induced constipation because they block and competitively prevent the binding of opioid agonists to μ-opioid receptors in the gastrointestinal tract [7]. PAMORAs act on gut motility, gut secretion and sphincter function [8]. Opioid agonists induce decreased cyclic adenosine monophosphate (cAMP) formation, and this effect is reversed by PAMORAs, leading to normalized chloride secretion. PAMORAs’ effect on gut motility leads to decreased transit time. This reduces the passive absorption of water from the stool, thus allowing for less dry and hard stools [9]. PAMORAs can also prevent sphincter of Oddi dysfunction and anal sphincter dysfunction caused by opioids, reducing straining and incomplete emptying.
1.2. Structure
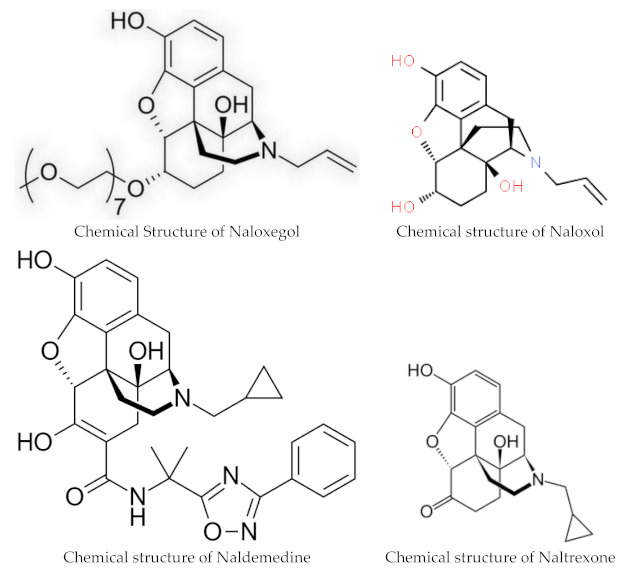
Naloxegol and naldemedine are structurally similar to morphine and other μ-opioid receptor agonists. They both have a pentacyclic structure with a benzene ring, tetrahydrofuran ring, two cyclohexane rings, and a piperidine ring. The phenolic ring and its 3-hydroxyl group play a central role in the analgesic effects of opioids, as removal of the OH group reduces analgesic activity significantly. Naldemedine, with a chemical formula of C32H34N4O6, is a peripherally acting μ-opioid receptor antagonist derived from naltrexone. It blocks opioid receptors of the μ, δ, and κ types in the gastrointestinal tract. Patents for naldemedine tosylate are expected to expire between 2026 and 2031. Unlike naltrexone, which can cross the blood–brain barrier and is used to treat opioid dependence, naldemedine has a large hydrophilic side chain and affinity to P-glycoprotein, resulting in minimal concentrations in the central nervous system. Due to its low abuse potential, the Drug Enforcement Administration removed naldemedine from Class II scheduling in September 2017 [20]. Naloxegol oxalate (chemical formula C34H53NO11) is another peripherally acting μ-opioid receptor antagonist (PAMORA) and a PEGylated derivative of naloxol, a derivative of naloxone (chemical formula C19H23NO4) [21]. It also does not cross the blood–brain barrier and is not a Class II schedule drug [22].
1.3. Pharmacokinetics
The oral bioavailability of Naldemedine ranges from 20% to 56%, with peak blood plasma levels achieved after 45 min on an empty stomach and 150 min when taken with a high-fat meal. The substance is highly bound to plasma proteins, primarily albumin, in the blood. The recommended dosage is 0.2 mg once daily with or without food [13,15]. Naldemedine is primarily metabolized by CYP3A to nor-naldemedine, and to a lesser extent by UDP-glucuronosyltransferase 1A3 to naldemedine 3-Glucuronide. Both metabolites are opioid receptor antagonists, but they are less potent than the original drug [23]. The drug is excreted in urine and feces, with an elimination half-life of 11 h. Patients with severe hepatic impairment should avoid naloxegol or naldemedine, although both drugs have been found to be safe and effective for those with mild to moderate hepatic impairments [24,25].
Naldemidine requires no adjustment for renal impairment [13,24,26]. For naloxegol, it is recommended that patients with a creatinine clearance <60 mL/min start with the lower naloxegol dose of 12.5 mg once daily and then, if tolerated, can increase the dose to 25 mg once daily [14,27].
Naloxegol clears mostly via hepatic metabolism (P450-CYP3A) with unknown actions of the metabolites. Naloxegol is excreted mostly in feces (and to some degree in urine), and its elimination half-life is 6–11 h [14]. Like naldemedine, when naloxegol is given with a fatty meal, absorption increases. Naloxegol is given as a once daily 12.5 or 25 mg tablet daily, and it should be taken on an empty stomach 1 h before or 2 h after the first meal of the day. Naloxegol may be crushed and can be given via nasogastric tube [14]. Maintenance laxatives should be discontinued prior to starting PAMORA therapy but may be resumed if OIC persists after 3 days of daily treatment. Decreased need for other laxatives may significantly reduce pill burden as, in many studies, PAMORAs alone were sufficient for relief of OIC.
1.4. Interactions
Even though PAMORAs in the US were approved for treatment of OIC in adults with noncancer pain, they have also been approved in other countries for both cancer and non-cancer pain [15,16], and are often prescribed off-label for OIC in cancer patients in the US. A very low risk of opioid withdrawal exists, so patients starting PAMORAs should be monitored for withdrawal symptoms such as hyperhidrosis, rhinorrhea, anxiety, and chills, though this was not commonly observed in clinical real-world practice. Opioid antagonists such as naloxone and naltrexone should not be used in conjunction with PAMORAs because of the potential increased risk of withdrawal. Both Naldemidine and naloxegol are no longer considered Schedule II controlled substances [20,22].
Naldemedine undergoes primary metabolism by the liver enzyme CYP3A4. Inhibitors of this enzyme can elevate naldemedine levels in the body, potentially leading to more side effects (see Table 1). Drugs like itraconazole, ketoconazole, clarithromycin, and grapefruit juice are examples of such inhibitors. In contrast, substances such as rifampicin and St John’s wort, which induce CYP3A4 activity, can significantly decrease naldemedine concentrations.
Table 1.
Inhibitors and inducers of CYP3A4 which potentially increase or decrease naldemedine concentrations.
| Strong Inhibitors of CYP3A4: Increase Naldemedine Concentration | Inducers of CYP3A4: Decrease Naldemedine Concentration |
|---|---|
| Itraconazole | Rifampine |
| Ketoconaxole | St. John’s wort |
| Clarithromycin | |
| Grapefruit juice | |
|
Moderate Inhibitors of CYP3A4: Diltiazem Erythromycin Verapamil |
Potent inhibitors of the P-glycoprotein pump, like ciclosporin, have the potential to elevate naldemedine blood levels.
1.5. Contraindications
Both naloxego and naldemidine are contraindicated in patients with gastrointestinal obstruction or patients with hypersensitivity to the medication. Naloxegol should be avoided with strong CYP3A4 inhibitors like clarithromycin and ketoconazole, as they can raise Naloxegol levels and increase the risk of side effects. If taking moderate CYP3A4 inhibitors, such as diltiazem, erythromycin, or verapamil, the dosage of Naloxegol needs to be reduced. Grapefruit and grapefruit juice may also increase Naloxegol levels. Rifampin, a CYP3A4 inducer, may reduce the effectiveness of Naloxegol.
1.6. Side Effects
The most common side effects of PAMORAs are diarrhea, abdominal pain, nausea, flatulence, vomiting and headache [7]. As pure opioid antagonists, Naloxegol and Naldemedine have no potential for abuse. During subgroup analysis of the COMPOSE trials I–III, no increase in adverse events (45.9%) for patients aged ≥65 years (N = 344) were found for naldemedine 0.2 mg compared to the overall group (47.1%) or compared to the placebo (51.6%), nor was there a difference in proportion of responders between older adults compared to the overall group [28]. Other subgroup analyses also found no increase in adverse events for naldemedine users with renal impairments [26] or in patients with hepatobiliary impairments from pancreatic cancer [29]. Moderate and strong CYP3A4 inhibitors and P-glycoprotein inhibitors may increase naldemedine concentrations; therefore, monitoring for adverse reactions is recommended in patients taking these medications. PAMORAs can improve quality of life, are generally safe and well tolerated, and offer a good response without reducing opioid-mediated analgesia.
1.7. Clinical Trials
Naldemedine was approved based on the results of the Japanese-led COMPOSE trials, which were phase three clinical studies in adult outpatients with chronic non-cancer pain and opioid-induced constipation. COMPOSE-I and COMPOSE-II were 12-week double-blind multi-country randomized controlled trials comparing 0.2 mg oral once daily naldemedine with a placebo between 2013–2015 [30]. Responders had to have at least three spontaneous bowel movements per week, with an increase of one spontaneous bowel movement for nine of the twelve weeks; the proportion of responders were significantly higher in the naldemedine group in both trials. COMPOSE-III tested the long term safety of naldemedine in patients with non-cancer chronic pain over 52 weeks, finding a statistically significant increase in weekly bowel movements without any evidence of opioid withdrawal symptoms [31].
While there is ample literature on the use of PAMORAs in patients with non-cancer pain, recruiting seriously ill patients with cancer into clinical research trials outside of cancer-directed treatment trials is difficult due to the patients’ short life expectancy, impaired functional status, and high symptom burden [32,33].
The objective of this systematic review was to search for high quality prospective interventional trials of either naldemedine or naloxegol for OIC in patients with cancer.
2. Materials and Methods
2.1. Focal Question
This (unregistered) literature search identified all primary literature (original research articles, reports, conference papers) using either naldemedine or naloxegol for opioid-induced constipation in cancer patients.
2.2. Search and Information Sources
The MESH search terms ‘naldemedine’, ‘naloxegol’, ‘constipation’, ‘obstipation’, ‘opioid-induced constipation’, and ‘cancer’ were used to search PubMed, Cochrane Library, Medline (Ovid), Scopus, Embase, ClinicalKey, and CINAHL Plus databases, as mentioned in the articles’ title, abstract, or body, from 2000 to 2023. The search terms were entered into each database using the Boolean operator ‘AND’ in several combinations: ‘naldemedine’ AND ‘constipation, ‘naldemedine’ AND ‘opioid-induced constipation’, and ‘naldemedine’ AND ‘obstipation’. The same search was completed using the word ‘naloxegol’ rather than ‘naldemidine’. Additional searches were conducted through Google Scholar and reviewing of references of the discovered studies. The literature search was conducted between October and early December of 2023.
2.3. Eligibility Criteria and Study Selection
There was no restriction on article types screened, but only prospective clinical trials using naldemidine or naloxegol for the treatment of OIC were eligible for review. There also was no restriction on language used, though our search was conducted in English and would likely not have found articles in other languages if they did not have at least an abstract written in English. Each article’s title and abstract were reviewed for relevance, and only studies conducted with cancer patients were included.
2.4. Outcomes Assessed
All studies used the ROME-IV criteria to define opioid-induced constipation, i.e., participants had to experience new or worsening constipation symptoms when starting or increasing opioid therapy and were straining during more than 25% of time spent passing stools, or had hard or lumpy stools more than 25% of the time [5,6]. Studies assessed changes in spontaneous bowel movement (SBM) frequency/week from baseline, SBM with complete bowel evacuation/week, and SBMs without significant straining/week for both intervention and placebo groups. Some studies also looked at the median time to first SBM after drug administration. Quality of life outcomes were assessed using the PAC–SYM stool domain and PAC–QOL dissatisfaction domain. All studies recorded adverse events and the seriousness of adverse events.
2.5. Quality Assessment
Due to the paucity of studies meeting all our inclusion criteria (being prospective controlled studies of either naldemedine or naloxegol enrolling cancer patients with OIC), we also report results of prospective post-marketing surveillance extension studies, which obviously were of much lower quality due to lack of a comparison group. We used the Critical Appraisal Skills Programme (CASP) [34] to assess the studies, which is appropriate for randomized controlled trials.
3. Results
Figure 1 shows a flowchart describing how the articles were chosen for inclusion in this review.
Figure 1.

Description of identification of studies included in this review (Von Roenn et al., 2013) [32].
Retrospective Studies Excluded
We excluded retrospective studies; many were conducted in patients with non-cancer, but several were conducted in special populations of cancer patients. One multi-center study evaluated the efficacy and safety of naldemedine in 40 hospitalized thoracic cancer patients with opioid-induced constipation in Japan where 65% of patients were responders [35]. Diarrhea was the most common adverse event and occurred in 27.5% (11 patients) but was mild for most of them (9 patients). Another Japanese multi-center retrospective study examined 33 hospitalized patients with gastrointestinal cancers (esophageal, gastric, small bowel, and colorectal cancers) of which, again, 63.6% were considered responders, i.e., they had a significant increase in bowel movement frequency of at least three times per week or at least once per week above the baseline after initiation of naldemedine [36]. Mild diarrhea was again the most common adverse event and occurred in 39.45% (13 patients). Additionally, 34 hospitalized patients with hepatobiliary pancreatic cancer (liver, biliary tract, and pancreatic cancers) who were taking opioids and received naldemedine during hospitalization were the focus of another retrospective multicenter Japanese study and were assessed for frequency of bowel movements before and after starting naldemedine [29]. In this group, 21 were responders (61.7%), defined as having ≥3 bowel movements/week, or with an increase from a baseline of ≥1 bowel movement/week over seven days after beginning daily naldemedine administration. The median number of weekly bowel movements before and after naldemedine treatment was two (range: 0–9) and six (range: 1–17), respectively; the increase in the number of bowel movements following naldemedine administration was statistically significant (Wilcoxon signed-rank test, p < 0.0001). Almost one third of patients experienced diarrhea as the most common side effect.
Cancer patients with a poor performance status are a particularly vulnerable group whose quality of life can be significantly impaired by constipation. Another retrospective multi-center Japanese study evaluated 71 cancer patients with ECOG performance status, 3 or 4 of whom received naldemedine [37]. Of these, 66.1% responded, i.e., bowel movement frequency increased to ≥3 times/week over 7 days after naldemedine administration., and grade 1 or 2 diarrhea was again the most common adverse event (38%). All of these retrospective studies in different types of cancer patients showed that naldemedine seemed safe and effective in clinical real-world practice, regardless of type of cancer and the performance status of patients.
We used the Critical Appraisal Skills Programme (CASP) [34] to assess the studies we included in our review, which is an appropriate tool for randomized controlled trials. All of the studies we found were industry-sponsored, with authors having conflicts of interest, making them prone to bias. Only five of the studies were randomized blinded placebo-controlled studies [32,33,38,39,40], two of which were unable to enroll sufficient participants [32,33]. The other seven studies were all non-interventional prospective open label extension/post-marketing surveillance studies [41,42,43,44,45,46,47], and therefore the quality of most of the discussed studies was not very high.
Table 2 describes the three randomized placebo-controlled trials included in this review for naldemedine [38,39,40], as well as results from a pooled subgroup analysis of patients from both 2017 Katakami studies [14] and two post-marketing surveillance studies of naldemidine [42,43]. It also details the six studies included for nalexogol, of which two were unsuccessful randomized controlled clinical studies due to insufficient enrollment [32,33], and four were non-interventional prospective observational studies in cancer patients lasting between 4 weeks and 1 year [44,45,46,47]. Studies described safety and efficacy, and the naloxegol studies included outcomes on quality of life. Table 2 describes the study design, medication regimen, inclusion criteria, outcomes assessed, and the results of each trial in detail.
Table 2.
Primary literature related to naldemedine or naloxegol for opioid-induced constipation in cancer patients.
| Authors | Study Design | Medication Regimen | Inclusion Criteria | Outcomes Assessed | Results |
|---|---|---|---|---|---|
| Katakami N et al., J Clin Onc, June 2017, Japan [38] |
Phase II b randomized double-blind placebo-controlled study | Naldemedine 1:1:1:1:1 assigned to either 0.1 mg, 0.2 mg, 0.4 mg, or placebo oral daily for 14 days | Adults 18 years or older with OIC and cancer, ECOG ≤ 2, on stable opioid regimen for ≥2 weeks | Primary: Change in spontaneous bowel movement frequency/week from baseline Secondary:
|
|
| |||||
| Katakami N et al., J Clin Onc, December 2017, Japan [39] |
COMPOSE-4: randomized Phase III placebo-controlled double-blind study COMPOSE-5: open-label extension study |
COMPOSE-4: 1:1 random assignment to Naldemedine 0.2 mg vs. placebo daily for 14 days COMPOSE-5: open-label 12-week extension |
Adults 20 years or older with OIC and cancer, ECOG ≤ 2, on stable opioid regimen for ≥2 weeks | COMPOSE-4 Primary endpoint: Proportion of SBM responders (≥3 SBMs/week and increase ≥1 SBM/week from baseline) COMPOSE-5 primary end point: safety. |
COMPOSE-4: N = 193 (97 naldemedine, 96 placebo); COMPOSE-5: N = 131
|
| |||||
| Katakami N et al., Ann Onc, 2018, Japan [40] |
COMPOSE-4: randomized Phase III placebo-controlled double-blind study COMPOSE-5: open-label extension study |
COMPOSE-4: 1:1 random assignment to Naldemedine 0.2 mg vs. placebo daily for 14 days COMPOSE-5: open-label 12-week extension study of Naldemedine 0.2 mg |
Adults 20 years or older with OIC and cancer, ECOG ≤ 2, on stable opioid regimen for ≥2 weeks | Secondary endpoints:
|
|
| |||||
| Osaka I et al., Esmo Open 2019, Japan [41] |
Subgroup analysis of pooled data from both Katakami 2017 studies | Naldemedine 0.2 mg vs. placebo | Adults 18 years or older with OIC and cancer, ECOG ≤ 2, on stable opioid regimen for ≥2 weeks | Proportions of SBM responders and patients with diarrhea. For patient subgroups with or without possible blood–brain barrier (BBB) disruptions, changes in Numerical Rating Scale (NRS) and Clinical Opioid Withdrawal Scale (COWS) scores. |
|
| |||||
| Takata K et al., Support Care Cancer 2022, Japan [42] | Non-interventional multi-center prospective post-marketing surveillance | Naldemedine 0.2 mg, for up to 12 weeks | Adult patients with opioid-induced constipation (OIC) and cancer pain | Safety & effectiveness | Effectiveness analysis set (N = 953): Improved frequency (75.0% and 83.2%) and condition of bowel movement (80.0% and 88.0%) at 2 and 12 weeks, respectively |
| Safety analysis set (N = 1177), 145 ADRs occurred in 133 (11.3%) patients, diarrhea was the most frequent event (n = 107, 9.09%) but most cases of diarrhea were non-serious (98.1%). Most ADRs were non-serious (93.8%) and resolved within 2 weeks (75.9%). | |||||
| Naya N, 2023, Cureus, Japan [43] | Non-interventional exploratory post hoc subgroup analysis of post-marketing surveillance, same dataset as [42] | naldemedine 0.2 mg, for up to 12 weeks | Adult patients with opioid-induced constipation (OIC) and cancer pain | Safety & effectiveness with subgroup analysis by:
|
|
| Incidence of AE, including diarrhea, among subgroups ranged from 7.74% to 16.08% (diarrhea: 5.95% to 13.19%), compared to 11.30% (diarrhoea: 9.09%) in the total population. | |||||
| Von Roenn JH et al., 2013, USA, published as poster only [32] |
KODIAC-06, planned as a randomized, placebo-controlled, double-blind, multicenter, phase 3 trial | Naloxegol 12.5 or 25 mg | Adult cancer patients with OIC |
|
Study was closed early due to inability to enroll sufficient patients. No further details available, no response from author received by date of submission. |
| Bull J et al., J Pain Sym Man, 2019, USA [33] | Feasibility study, planned as 3-center randomized, placebo-controlled trial | Naloxegol 25 mg, with or without concomitant use of laxatives, (14 days of double-blind naloxegol vs. placebo followed by 14-day open-label naloxegol daily) | Adult advanced cancer patients aged ≥ 18 years, with life expectancy > 8 weeks, PPS ≥ 30, on at least 20 Morphine equivalents/d for >1 week, with OIC on laxatives |
|
Study closed early after 24 months due to inability to enroll sufficient patients:
|
| Cobo Dols M et al., BMJ Support Palliat Care, 2020, Spain [44] | Non-interventional, 3-month follow-up observational cohortstudy | Naloxegol 12.5 or 25 mg, with or without concomitant use of laxatives | Adult cancer patients ≥ 18 years, on opioids for pain with OIC on laxatives, Karnofsky ≥ 50 |
|
|
| Lemaire A. et al., Supp Care Cancer, 2021, France [45] |
Non-interventional “real life” outpatient multi-center, 4-week follow-up observational study | Naloxegol 12.5 or 25 mg, with or without concomitant use of laxatives | Adult cancer patients aged 18–70 years old with OIC on laxatives, any ECOG, on any opioid regimen |
|
N = 124 cancer patients of which 79% had ECOG ≤ 2, metastatic stage, 80%. At inclusion, the median opioid dosage was 60 mg of oral morphine or equivalent.
|
| Davies A et. al., Cancers, 2022, 26 European countries [46] |
Non-interventional, prospective “real world” singles arm open label multi-national 4-wek study | Naloxegol 12.5 or 25 mg (−50 mg), with or without concomitant use of laxatives | Adult cancer patients ≥ 18 years old who had been on opioids for at least 4 weeks and had OIC, any ECOG, on any opioid regimen. Colorectal cancer pts were excluded |
|
|
| Cobo Dols M et al., BMJ Support Palliat Care, 2023, Spain [47] |
Non-interventional, 1-year prospective observational “real-world” study (continuation of Cobo 2020 study) | Naloxegol 12.5 or 25 mg, with or without concomitant laxative use | Adult cancer patients ≥ 18 years, on opioids for pain with OIC on laxatives, Karnofsky ≥ 50 | Long-term efficacy, quality of life (QOL) and safety of naloxegol. Assessed by the patient assessment of constipation QOL questionnaire (PAC-QOL), the PAC symptoms (PAC-SYM), the response rate at day 15, and months 1-3-6-12, and global QOL (EuroQoL-5D-5L) |
|
OIC = opioid-induced constipation, SBM = spontaneous bowel movement, CBSM = complete spontaneous bowel movement, AE = adverse events, TEAE = treatment emergent adverse events, NRS = numerical rating scale, COWS = clinical opioid withdrawal scale, ECOG = Eastern Cooperative Oncology Group (assessment of functional status), PAC-SYM stool domain = patient assessment of constipation-symptoms, PAC-QOL dissatisfaction domain = patient assessment of constipation-quality of life, QoL = quality of life.
The most common side effects described with both nalexogol and naldemedine were diarrhea, abdominal pain, abdominal bloating, nausea, and dysesthesia; almost all adverse effects were of a mild degree.
4. Discussion
Our literature search revealed three randomized placebo controlled double-blind trials in patients with cancer using naldemedine to treat OIC, as well as two unsuccessful randomized placebo-controlled double-blind trials using naloxegol for OIC in patients with advanced cancer and cancer-related pain that were closed early due to poor patient enrollment. Additionally, three non-interventional studies of naldemidine and four non-interventional studies of naloxegol in cancer patients were found. Large interventional studies with cancer patients were absent, reflecting the enormous recruiting difficulties in this population; thus, higher quality studies are only available for naldemidine but not for naloxegol. All naldemidine studies were conducted in Japan, whereas all naloxegol studies were non-interventional and conducted in Europe. Attempts at high-quality randomized controlled trials with naloxegol failed due to enormous recruiting difficulties in the US.
The usual medication doses studied were 0.2 mg for naldemedine and 12.5 or 25 mg for naloxegol, and, at these doses, treatment emergent adverse events were usually relatively minor. Cancer patients with OIC seem to be ideal candidates for treatment with PAMORAs as they block the constipating effects of opioids at the myenteric plexus without affecting analgesia in the central nervous system. Ongoing treatment for the disabling opioid side effect of constipation with PAMORAs seems to be safe, even if given for prolonged periods of times of up to one year based on the open label extension studies. No particular monitoring for toxicity is required, and even patients with renal or hepatic impairment up to CHILD class B are good candidates for PAMORAs without a need for dose adjustment [24,25,26,27].
While conducting studies on symptom management in cancer patients seems difficult and fraught with recruitment challenges, head-to-head comparisons of laxatives versus PAMORAs or different PAMORASs against each other are even rarer, even in patients with non-cancer pain who are easier to recruit. We only found one retrospective study comparing oral naloxegol with subcutaneous methylnaltrexone [48]; however, this study was conducted in seriously ill patients in an intensive care unit setting and included only 30 cancer patients (15% of patients in the naloxegol group and 28% in the naltrexone group had cancer). They found that both drugs increased SBMs and that naloxegol was non-inferior to subcutaneous methylnaltrexone at a significantly reduced cost.
4.1. Limitations and Study Quality
We reviewed all prospective studies using either naldemidine or naloxegol in patients with OIC and cancer; all these studies were funded by industry, and investigators were either employees of the drug companies or received royalties from the drug companies sponsoring the studies, making them prone to bias. However, the three RCTs by Katakami [38,39,40] were conducted according to generally accepted standards with appropriate randomization and blinding, following a well-described study protocol and reporting results comprehensively, including confidence intervals and reporting of adverse events (these RCTs were also comparable since the outcome measures used were similar for these trials). Of the 12 studies reviewed, only 5 were RCTs, and of those only 3 (naldemidine studies) [38,39,40] had results, as the other 2 (naloxegol studies) [32,33] were unable to recruit enough patients. The other studies reviewed were various non-interventional open label extension studies of the primary Katakami studies (for naldemidine) or non-interventional observational studies (for naloxegol) [44,45,46,47], and thus of much lower quality. However, we reviewed all in the absence of any better evidence, as our clinical question was about use of PAMORAs specificially in cancer patients with OIC. The ‘real world’ studies were also the only studies able to follow patients taking PAMORAs over a longer period of time, While the RCTs only administered the study drug for two weeks [33,38,39,40], the ‘real world’ open label extension studies were either up to four weeks [45,46], three months [39,40,41,42,43,44] or even up to one year [47] long.
Most studies were conducted in Japan [38,39,40,41,42,43], and some in Europe [44,45,46,47], while the few studies conducted in the US [32,33] were unable to recruit enough participants; therefore, it is not clear if results would be fully applicable to patients in North America.
4.2. Implications for Pharmacy Practice
Pharmacists need to take an active role in counseling patients who are taking opioid medications for cancer pain and who will invariably experience OIC. OIC significantly impairs the quality of life of patients requiring opioids for pain control, which makes prevention, identification, and treatment of OIC, as well as counseling on available medications and their proper use, critical areas for pharmacist involvement. It is important to note that the usual first line counseling techniques by clinical pharmacists, like increasing hydration and physical activity, even if necessary in a global cancer context, is not effective in OIC. Similarly, traditional laxatives may not be effective in OIC but can be responsible for side effects, enormous pill burden, and, in some cases, patients reducing their opioids, which then leads to increased suffering due to inadequate pain control. Therefore, being knowledgable about PAMORAs to treat OIC is crucial for clinical pharmacists who assist cancer patients. Due to their increased cost, large health care systems like the Veteran Health Administration have developed criteria for the use of both Naldemedine [49] and naloxegol [50] t by theVA Pharmacy Benefits Management Services.
5. Conclusions
Naldemedine at 0.2 mg or naloxegol at 12–25 mg once daily were useful in the treatment of OIC in cancer patients, improving their quality of life while producing relatively minor side effects. Both drugs have high potential in palliative and hospice care due to the debilitating effects of treatment-resistant OIC and non-responsiveness to traditional laxatives. Clinical pharmacists take an active role in counseling patients on the appropriate use of PAMORAs, which can have a tremendous impact on cancer patients’ well-being. Few high quality trials were found for naldemidine and none for naloxegol, and the trials for the former were of short duration (14 days). Further longer-lasting larger-scale randomized placebo-controlled or comparative studies with standard laxative medications and PAMORAs in cancer patients would strengthen existing evidence but are wrought with significant recruitment challenges.
Author Contributions
Conceptualization, methodology, and writing—original draft preparation: U.K.B.; writing—review and editing: U.K.B., L.K.J., M.A.G. and S.N.I. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
This material is the result of work supported with resources and the use of facilities at the Michael E. DeBakey VA medical center in Houston, TX. The content is solely the authors’ responsibility and does not necessarily represent the Department of Veteran Affairs’ official views.
Footnotes
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
References
- 1.Rang H.P., Dale M.M., Ritter J.M. Analgesic drugs. Pharmacology. 1999;13:579–603. [Google Scholar]
- 2.Kurz A., Sessler D.I. Opioid-induced bowel dysfunction: Pathophysiology and potential new therapies. Drugs. 2003;63:649–671. doi: 10.2165/00003495-200363070-00003. [DOI] [PubMed] [Google Scholar]
- 3.Sykes N.P. The relationship between opioid use and laxative use in terminally ill cancer patients. Palliat. Med. 1998;12:375–382. doi: 10.1191/026921698674125048. [DOI] [PubMed] [Google Scholar]
- 4.Bell T.J., Panchal S.J., Miaskowski C., Bolge S.C., Milanova T., Williamson R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: Results of a US and European Patient Survey (PROBE 1) Pain Med. 2009;10:35–42. doi: 10.1111/j.1526-4637.2008.00495.x. [DOI] [PubMed] [Google Scholar]
- 5.Drossman D.A., Hasler W.L. Rome IV-Functional GI disorders: Disorders of gut-brain interaction. Gastroenterology. 2016;150:1257–1261. doi: 10.1053/j.gastro.2016.03.035. [DOI] [PubMed] [Google Scholar]
- 6.Schmulson M.J., Drossman D.A. What is New in Rome IV. J. Neurogastroenterol. Motil. 2017;23:151–163. doi: 10.5056/jnm16214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Streicher J.M., Bilsky E.J. Peripherally Acting μ-Opioid Receptor Antagonists for the Treatment of Opioid-Related Side Effects: Mechanism of Action and Clinical Implications. J. Pharm. Pract. 2017;31:658–669. doi: 10.1177/0897190017732263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brock C., Olesen S.S., Olesen A.E., Frøkjaer J.B., Andresen T., Drewes A.M. Opioid Induced Bowel Dysfunction. Drugs. 2012;72:1847–1865. doi: 10.2165/11634970-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 9.Floettmann E., Bui K., Sostek M., Payza K., Eldon M. Pharmacologic Profile of Naloxegol, a Peripherally Acting µ-Opioid Receptor Antagonist, for the Treatment of Opioid-Induced Constipation. J. Pharmacol. Exp. Ther. 2017;361:280–291. doi: 10.1124/jpet.116.239061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hu K., Bridgeman M.B. Naldemedine (Symproic) for the Treatment of Opioid-Induced Constipation. Pharm. Ther. 2018;43:601–627. [PMC free article] [PubMed] [Google Scholar]
- 11.Garnock-Jones K.P. Naloxegol: A review of its use in patients with opioid-induced constipation. Drugs. 2015;75:419–425. doi: 10.1007/s40265-015-0357-2. [DOI] [PubMed] [Google Scholar]
- 12.Essmat N., Karádi D.Á., Zádor F., Király K., Fürst S., Al-Khrasani M. Insights into the Current and Possible Future Use of Opioid Antagonists in Relation to Opioid-Induced Constipation and Dysbiosis. Molecules. 2023;28:7766. doi: 10.3390/molecules28237766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.FDA Symproic (Naldemedine) Tablets. [(accessed on 28 November 2023)]; Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208854Orig1s000TOC.cfm.
- 14.FDA Movantik (Naloxegol) Prescribing Information Highlights (PDF) [(accessed on 28 November 2023)]; Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/204760s000lbl.pdf.
- 15.European Medicines Agency (EMA) “Rizmoic: EPAR—Product Information” (PDF) 2019. [(accessed on 7 February 2024)]. Available online: https://www.ema.europa.eu/en/documents/product-information/rizmoic-epar-product-information_en.pdf.
- 16.European Medicines Agency (EMA) “Moventig”: EPAR—Product Information (PDF) 2014. [(accessed on 31 January 2024)]. Available online: https://www.ema.europa.eu/en/documents/product-information/moventig-epar-product-information_en.pdf.
- 17.Crockett S.D., Greer K.B., Heidelbaugh J.J., Falck-Ytter Y., Hanson B.J., Sultan S., American Gastroenterological Association Institute Clinical Guidelines Committee American Gastroenterological Association Institute Guideline on the Medical Management of Opioid-Induced Constipation. Gastroenterology. 2019;156:218–226. doi: 10.1053/j.gastro.2018.07.016. [DOI] [PubMed] [Google Scholar]
- 18.Larkin P.J., Cherny N.I., La Carpia D., Guglielmo M., Ostgathe C., Scotté F., Ripamonti C.I. ESMO Guidelines Committee. Diagnosis, assessment and management of constipation in advanced cancer: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018;29((Suppl. S4)):iv111–iv125. doi: 10.1093/annonc/mdy148. [DOI] [PubMed] [Google Scholar]
- 19.Farmer A.D., Drewes A.M., Chiarioni G., De Giorgio R., O’Brien T., Morlion B., Tack J. Pathophysiology and management of opioid-induced constipation: European expert consensus statement. United Eur. Gastroenterol. J. 2019;7:7–20. doi: 10.1177/2050640618818305. Erratum in: United Eur. Gastroenterol. J. 2019, 7, 178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schedules of Controlled Substances: Removal Of Naldemedine from Control (PDF). Federal Register. [(accessed on 28 November 2023)]; Available online: https://www.govinfo.gov/content/pkg/FR-2017-07-12/pdf/2017-14482.pdf.
- 21.Bui K., Zhou D., Xu H., Floettmann E., Al-Huniti N. Clinical Pharmacokinetics and Pharmacodynamics of Naloxegol, a Peripherally Acting µ-Opioid Receptor Antagonist. Clin. Pharmacokinet. 2017;56:573–582. doi: 10.1007/s40262-016-0479-z. [DOI] [PubMed] [Google Scholar]
- 22.Federal Register. [(accessed on 28 November 2023)]; Available online: https://www.federalregister.gov/documents/2015/01/23/2015-01172/schedules-of-controlled-substances-removal-of-naloxegol-from-control.
- 23.Kanemasa T., Koike K., Arai T., Ono H., Horita N., Chiba H., Nakamura A., Morioka Y., Kihara T., Hasegawa M. Pharmacologic effects of naldemedine, a peripherally acting μ-opioid receptor antagonist, in in vitro and in vivo models of opioid-induced constipation. Neurogastroenterol. Motil. 2019;31:e13563. doi: 10.1111/nmo.13563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fukumura K., Yamada T., Yokota T., Kawasaki A. The Influence of Renal or Hepatic Impairment on the Pharmacokinetics, Safety, and Tolerability of Naldemedine. Clin. Pharmacol. Drug Dev. 2020;9:162–174. doi: 10.1002/cpdd.690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bui K., She F., Sostek M. The effects of mild or moderate hepatic impairment on the pharmacokinetics, safety, and tolerability of naloxegol. J. Clin. Pharmacol. 2014;54:1368–1374. doi: 10.1002/jcph.348. [DOI] [PubMed] [Google Scholar]
- 26.Webster L.R., Hale M.E., Yamada T., Wild J.E. A Renal Impairment Subgroup Analysis of the Safety and Efficacy of Naldemedine for the Treatment of Opioid-Induced Constipation in Patients with Chronic Non-Cancer Pain Receiving Opioid Therapy. J. Pain Res. 2020;13:605–612. doi: 10.2147/JPR.S237833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bui K., She F., Sostek M. The effects of renal impairment on the pharmacokinetics, safety, and tolerability of naloxegol. J. Clin. Pharmacol. 2014;54:1375–1382. doi: 10.1002/jcph.349. [DOI] [PubMed] [Google Scholar]
- 28.Wild J., Webster L., Yamada T., Hale M. Safety and Efficacy of Naldemedine for the Treatment of Opioid-Induced Constipation in Patients with Chronic Non-Cancer Pain Receiving Opioid Therapy: A Subgroup Analysis of Patients ≥ 65 Years of Age. Drugs Aging. 2020;37:271–279. doi: 10.1007/s40266-020-00753-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kamiya T., Imai H., Fujita Y., Hiruta E., Masuno T., Yamazaki S., Tanaka H., Sandoh M., Takei S., Arai K., et al. A Retrospective Study of the Efficacy and Safety of Naldemedine for Treatment of Opioid-Induced Constipation in Patients with Hepatobiliary Pancreatic Cancer. Medicina. 2023;59:492. doi: 10.3390/medicina59030492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hale M., Wild J., Reddy J., Yamada T., Arjona Ferreira J.C. Naldemedine versus placebo for opioid-induced constipation (COMPOSE-1 and COMPOSE-2): Two multicentre, phase 3, double-blind, randomised, parallel-group trials. Lancet Gastroenterol. Hepatol. 2017;2:555–564. doi: 10.1016/S2468-1253(17)30105-X. [DOI] [PubMed] [Google Scholar]
- 31.Camilleri M., Hale M., Morlion B., Tack J., Webster L., Wild J. Naldemedine Improves Patient-Reported Outcomes of Opioid-Induced Constipation in Patients with Chronic Non-Cancer Pain in the COMPOSE Phase 3 Studies. J. Pain Res. 2021;14:2179–2189. doi: 10.2147/JPR.S282738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.von Roenn J.H., Tack J., Barker P.N., Lowe E.S., Fleischmann C., Sostek M. Multinational Association of Supportive Care in Cancer, Proceedings of the MASCC/ISOO International Symposium on Supportive Care in Cancer, Berlin, Germany, 27–29 June 2013. John Wiley & Sons; Hoboken, NJ, USA: 2013. Challenges in patient recruitment during KODIAC-06, a randomized, placebo-controlled, double-blind, multicenter, phase 3 trial of naloxegol in patients with neoplasia and opioid-induced constipation (OIC) [Google Scholar]
- 33.Bull J., Bonsignore L., Massie L., Riggs A., Knotkova H., Wellman C., Portenoy R. Challenges in Recruiting Patients to a Controlled Feasibility Study of a Drug for Opioid-Induced Constipation: Lessons from the Population With Advanced Cancer. J. Pain Symptom Manag. 2019;57:e5–e8. doi: 10.1016/j.jpainsymman.2018.09.024. [DOI] [PubMed] [Google Scholar]
- 34.Critical Appraisal Skills Programme CASP Randomised Controlled Trial Checklist. 2020. [(accessed on 7 February 2024)]. Available online: https://casp-uk.net/checklists/casp-rct-randomised-controlled-trial-checklist-fillable.pdf.
- 35.Imai H., Fujita Y., Hiruta E., Masuno T., Yamazaki S., Tanaka H., Kamiya T., Sandoh M., Takei S., Arai K., et al. A retrospective study of the efficacy and safety of naldemedine for opioid-induced constipation in thoracic cancer patients. Thorac. Cancer. 2022;13:2301–2308. doi: 10.1111/1759-7714.14557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nishiba H., Imai H., Fujita Y., Hiruta E., Masuno T., Yamazaki S., Tanaka H., Kamiya T., Ito M., Takei S., et al. Efficacy and safety of naldemedine treatment for opioid-induced constipation in gastrointestinal cancer: A retrospective analysis. Ann. Palliat. Med. 2023;12:697–707. doi: 10.21037/apm-22-1130. [DOI] [PubMed] [Google Scholar]
- 37.Fujita Y., Imai H., Hiruta E., Masuno T., Yamazaki S., Tanaka H., Kamiya T., Sandoh M., Takei S., Arai K., et al. Efficacy and Safety of Naldemedine Administration for Opioid-Induced Constipation in Cancer Patients with Poor Performance Status. J. Palliat. Med. 2023;26:548–553. doi: 10.1089/jpm.2022.0495. [DOI] [PubMed] [Google Scholar]
- 38.Katakami N., Oda K., Tauchi K., Nakata K., Shinozaki K., Yokota T., Suzuki Y., Narabayashi M., Boku N. Phase IIb, Randomized, Double-Blind, Placebo-Controlled Study of Naldemedine for the Treatment of Opioid-Induced Constipation in Patients with Cancer. J. Clin. Oncol. 2017;35:1921–1928. doi: 10.1200/JCO.2016.70.8453. [DOI] [PubMed] [Google Scholar]
- 39.Katakami N., Harada T., Murata T., Shinozaki K., Tsutsumi M., Yokota T., Arai M., Tada Y., Narabayashi M., Boku N. Randomized Phase III and Extension Studies of Naldemedine in Patients with Opioid-Induced Constipation and Cancer. J. Clin. Oncol. 2017;35:3859–3866. doi: 10.1200/JCO.2017.73.0853. [DOI] [PubMed] [Google Scholar]
- 40.Katakami N., Harada T., Murata T., Shinozaki K., Tsutsumi M., Yokota T., Arai M., Tada Y., Narabayashi M., Boku N. Randomized phase III and extension studies: Efficacy and impacts on quality of life of naldemedine in subjects with opioid-induced constipation and cancer. Ann. Oncol. 2018;29:1461–1467. doi: 10.1093/annonc/mdy118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Osaka I., Ishiki H., Yokota T., Tada Y., Sato H., Okamoto M., Satomi E. Safety and efficacy of naldemedine in cancer patients with opioid-induced constipation: A pooled, subgroup analysis of two randomised controlled studies. ESMO Open. 2019;4:e000527. doi: 10.1136/esmoopen-2019-000527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Takata K., Nakazawa M., Honda K., Hashimoto S. Post-marketing surveillance of the safety and effectiveness of naldemedine in the management of opioid-induced constipation in patients with cancer pain in Japan. Support. Care Cancer. 2022;30:3943–3954. doi: 10.1007/s00520-022-06807-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Naya N., Oka H., Hashimoto S., Morioka Y., Kizawa Y. Real-World Evidence for the Safety and Effectiveness of Naldemedine in the Management of Opioid-Induced Constipation in Patients with Cancer Pain: Post-hoc Subgroup Analysis of Post-marketing Surveillance in Japan. Cureus. 2023;15:e46090. doi: 10.7759/cureus.46090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cobo Dols M., Beato Zambrano C., Cabezón Gutiérrez L., Chicas Sett R., Blancas López-Barajas M.I., García Navalón F., Fírvida Pérez J.L., Serrano Bermúdez G., Togores Torres P., Delgado Mingorance I., et al. Efficacy of naloxegol on symptoms and quality of life related to opioid-induced constipation in patients with cancer: A 3-month follow-up analysis. BMJ Support. Palliat. Care. 2021;11:25–31. doi: 10.1136/bmjspcare-2020-002249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lemaire A., Pointreau Y., Narciso B., Piloquet F.X., Braniste V., Sabaté J.M. Effectiveness of naloxegol in patients with cancer pain suffering from opioid-induced constipation. Support. Care Cancer. 2021;29:7577–7586. doi: 10.1007/s00520-021-06299-2. Erratum in: Support. Care Cancer 2021, 29, 7587–7589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Davies A., Cinieri S., Dupoiron D., España Fernandez S., Leclerc J., Montesarchio V., Mystakidou K., Serna J., Tack J., on Behalf of the Nacasy Study Group A Prospective, Real-World, Multinational Study of Naloxegol for Patients with Cancer Pain Diagnosed with Opioid-Induced Constipation-The NACASY Study. Cancers. 2022;14:1128. doi: 10.3390/cancers14051128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cobo Dols M., Beato Zambrano C., Cabezón-Gutiérrez L., Chicas-Sett R., Blancas López-Barajas M.I., García Navalón F.J., Fírvida Pérez J.L., Serrano Bermúdez G., Togores Torres P., Delgado Mingorance I., et al. One-year efficacy and safety of naloxegol on symptoms and quality of life related to opioid-induced constipation in patients with cancer: KYONAL study. BMJ Support Palliat. Care. 2023;13:e318–e326. doi: 10.1136/bmjspcare-2020-002816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tobben D., Carpenter S., Kolar R., Merritt T., Young T., Hauser P., Collier T. Naloxegol versus Methylnaltrexone for Opioid-Induced Constipation in Critically Ill Patients. Ann. Pharmacother. 2023:10600280231205023. doi: 10.1177/10600280231205023. [DOI] [PubMed] [Google Scholar]
- 49.Naldemedine (SYMPROIC) Criteria for Use, February 2019 VA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. [(accessed on 1 December 2023)]; Available online: https://www.va.gov/formularyadvisor/DOC_PDF/Naldemedine_SYMPROIC.pdf.
- 50.Naloxegol (MOVANTIK) Criteria for Use March 2018 VA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. [(accessed on 1 December 2023)]; Available online: https://www.pbm.va.gov/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.