

ABSTRACT
AZD1222 (ChAdOx1 nCoV-19) is a replication-deficient adenoviral vectored coronavirus disease-19 (COVID-19) vaccine that is manufactured as SII-ChAdOx1 nCoV-19 by the Serum Institute of India Pvt Ltd following technology transfer from Oxford University/AstraZeneca. The non-inferiority of SII-ChAdOx1 nCoV-19 with AZD1222 was previously demonstrated in an observer-blind, phase 2/3 immuno-bridging study (trial registration: CTRI/2020/08/027170). In this analysis of immunogenicity and safety data 6 months post first vaccination (Day 180), 1,601 participants were randomized 3:1 to SII-ChAdOx1 nCoV-19 or AZD1222 (immunogenicity/reactogenicity cohort n = 401) and 3:1 to SII-ChAdOx1 nCoV-19 or placebo (safety cohort n = 1,200). Immunogenicity was measured by anti-severe acute respiratory syndrome coronavirus 2 spike (anti-S) binding immunoglobulin G and neutralizing antibody (nAb) titers. A decline in anti-S titers was observed in both vaccine groups, albeit with a greater decline in SII-ChAdOx1 nCoV-19 vaccinees (geometric mean titer [GMT] ratio [95% confidence interval (CI) of SII-ChAdOx1 nCoV-19 to AZD1222]: 0.60 [0.41–0.87]). Consistent similar decreases in nAb titers were observed between vaccine groups (GMT ratio [95% CI]: 0.88 [0.44–1.73]). No cases of severe COVID-19 were reported following vaccination, while one case was observed in the placebo group. No causally related serious adverse events were reported through 180 days. No thromboembolic or autoimmune adverse events of special interest were reported. Collectively, these data illustrate that SII-ChAdOx1 nCoV-19 maintained a high level of immunogenicity 6 months post-vaccination. SII-ChAdOx1 nCoV-19 was safe and well tolerated.
KEYWORDS: SARS-CoV-2, COVID-19 vaccine, SII-ChAdOx1 nCoV-19, AZD1222 (ChAdOx1 nCoV-19), safety, immunogenicity
Introduction
The coronavirus disease-19 (COVID-19) pandemic affected India severely, with > 44 million cases and > 0.5 million deaths due to COVID-19 reported as of January 31, 2023.1 Following technology transfer of AZD1222 (ChAdOx1 nCoV-19) from AstraZeneca in 2020, SII-ChAdOx1 nCoV-19 (COVID-19 vaccine) was manufactured in India by Serum Institute of India Pvt Ltd (SIIPL).2
A phase 2/3 immuno-bridging trial demonstrated that SII-ChAdOx1 nCoV-19 was non-inferior to AZD1222 in terms of geometric mean titer (GMT) ratios of anti-spike (anti-S) immunoglobulin G (IgG) antibodies, and was accompanied by an acceptable safety profile. Based on these results, SII-ChAdOx1 nCoV-19 was approved by the Indian regulatory authorities under the brand name of ‘COVISHIELDTM,’ and subsequently received an emergency use listing by the World Health Organization (WHO).3 SII-ChAdOx1 nCoV-19 has played an important role in mitigating the pandemic globally, with ~ 1.75 billion doses supplied across > 100 countries.
The immunogenicity and safety of SII-ChAdOx1 nCoV-19 at 1 month post second-dose primary series vaccination (Day 57) have previously been described.2 As observed with other studies of COVID-19 vaccines, serological monitoring over time is important to assess immunological waning after vaccination.4–6 AZD1222 has demonstrated durability of protection against symptomatic COVID-19 and immune responses for 6 months after the second dose.7 Here, we describe the immunogenicity and safety of SII-ChAdOx1 nCoV-19 6 months post first-dose primary series vaccination (Day 180) compared with AZD1222.
Methods
This was a phase 2/3 participant-blind, observer-blind, randomized, controlled study in healthy adults in India (trial registration: CTRI/2020/08/027170). The study was approved by the Indian regulatory authority and the ethics committee of each study site. The study was conducted in accordance with the International Council for Harmonization good clinical practice guidelines (2016), the Declaration of Helsinki (2013), as well as the guidelines of the Indian Council of Medical Research (2017), and the Government of India’s New Drugs and Clinical Trial Rules (2019). Participants provided written informed consent before study enrollment. An independent Data Safety Monitoring Board (DSMB) reviewed safety data during the course of the study. The study enrolled participants from 14 hospitals across India.
The study had two primary outcomes: incidence of causally related serious adverse events (SAEs) with SII-ChAdOx1 nCoV-19 compared with placebo, and the anti-S IgG GMT ratio at 1 month post second dose of SII-ChAdOx1 nCoV-19 compared with AZD1222. The study design, inclusion/exclusion criteria, protocol and safety and immunogenicity results 1 month post second dose (Day 57) have previously been published.2 Briefly, the study enrolled adults aged ≥18 years into immunogenicity/reactogenicity and safety cohorts between August 25 and October 31, 2020 (data cutoff June 2, 2021). Individuals who had controlled comorbid conditions, per investigator judgment based on medical history and clinical examination, were eligible for enrollment. Female participants were required to have a negative pregnancy test prior to each dose of vaccine and were required to use adequate contraception from 28 days before the first dose through 28 days after the second dose. Key exclusion criteria were acute illness, known prior severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, and prior diagnosis of an immunosuppressive condition or receipt of immunosuppressive therapy. Full eligibility criteria are listed in the protocol (appendix).
SII-ChAdOx1 nCoV-19 and AZD1222 consist of a replication-deficient simian adenovirus vector (ChAdOx1) containing genetic material encoding the spike protein for SARS-CoV-2.2 Each 0.5 mL dose contains 5 × 1010 viral particles and other excipients. Participants visited the study sites on Day 1, Day 29 (+14 days window period), Day 57 (+14 days), and Day 180 (+28 days). Two doses of the vaccine or placebo were given intramuscularly with a 4-week interval (Day 1 and Day 29). Participants were contacted by telephone on Day 90 for the safety assessment. All participants were tested for SARS-CoV-2 by reverse transcription polymerase chain reaction (RT-PCR) at baseline, Day 29, Day 180, and at any time during the study if they were suspected of having COVID-19, or had contact with confirmed COVID-19-positive cases.
In the immunogenicity/reactogenicity cohort, participants were randomly assigned in a 3:1 ratio to receive either SII-ChAdOx1 nCoV-19 or AZD1222, stratified by age (18–59 years and ≥60 years, to ensure ~ 25% of participants in the latter group). In the safety cohort, participants were randomly assigned in a 3:1 ratio to receive SII-ChAdOx1 nCoV-19 or placebo. An Interactive Web Response system was used for randomization and the randomization scheme was generated using SAS version 9.4. Personnel involved in administering vaccines were not blinded to treatment allocation and they did not conduct any study outcome evaluations. Participants and all other study personnel, including sponsor and laboratory personnel, were blinded to treatment.
Anti-S and anti-receptor binding domain (anti-RBD) IgG antibody titers were tested at baseline, Day 29, Day 57, and Day 180 using a validated electrochemiluminescence-based multiplex immunoassay. Antibody titers are expressed as Arbitrary Units (AU) per mL based on the reference standard provided by Mesoscale Discovery (MSD) and the assay was validated using the WHO International Reference Standard, with results expressed as binding antibody units per mL. Neutralizing antibodies (nAbs) at baseline, Day 29, Day 57, and Day 180 were tested using a validated pseudovirus-based microneutralization (MNT) assay, which is a fully quantitative assay fitted with a PPD®-developed reference standard. The assay was calibrated against the WHO International Reference Standard and results are expressed as relative to the International Standard in International Units (IU) per mL.2 Seroconversion was defined as a four-fold increase in antibody titer with respect to the baseline value.
The secondary outcome included immunogenicity at 180 days post-vaccination. The secondary outcome was not statistically powered and analyzed descriptively. The GMT and the geometric mean fold rise (GMFR) from baseline were compared between the groups. For the immunogenicity analysis, the log-transformed titers were used to construct the least squares mean (LSM) and its 95% confidence interval (CI) for each study group. The difference between the LSMs for the two vaccine groups (SII-ChAdOx1 nCoV-19 and AZD1222) and a two-sided 95% CI were calculated using the Mixed Model for Repeated Measures, which included vaccine group, log baseline titer, comorbidity, age group, sex, visits, and vaccine-by-visit interaction as covariates. The GMT and the corresponding 95% CI were calculated by using the antilog of the LSM of logarithmically transformed titers. Similarly, the GMT ratio and the corresponding 95% CI were calculated from the LSM difference. The odds ratio for the seroconversion rates between the SII-ChAdOx1 nCoV-19 and AZD1222 groups was estimated using a logistic regression model, with baseline titer value, comorbidity, and age group as covariates. Participants having positive RT-PCR for SAR CoV-2 (symptomatic or asymptomatic) were excluded from immunogenicity analysis from time point of positive result.
In the immunogenicity/reactogenicity cohort, solicited adverse events (AEs) were collected for 7 days after each dose using diary cards. In all participants, unsolicited AEs were collected through 28 days after each vaccine dose. Additionally, serious AEs (SAEs) and AEs of special interest (AESIs, including all cases of COVID-19) were collected throughout the study period until the Day 180 (+28 days) visit. Participants were instructed to inform investigators/study staff about any SAEs or AESIs including COVID-19 or any other illness throughout 180 days in addition to assessments at scheduled study visits. The proportions of participants experiencing SAEs and AESIs were reported for each vaccine group as percentages. Based on the assumption that the true frequency of causally related SAEs is 0.25%, the study provided a 95% probability of detecting at least one causally related SAE among the 1,200 participants receiving SII-ChAdOx1 nCoV-19.2
Results
The study was initiated in August 2020 and last participant visit occurred in June 2021. A total of 1,601 participants were enrolled in the study (401 in the immunogenicity/reactogenicity cohort and 1,200 in the safety cohort) and were randomized 3:1 to SII-ChAdOx1 nCoV-19 and AZD1222/placebo. 1,600 participants received > 1 dose of vaccine or placebo, and 1,566 (97.6%), 1,573 (98.1%), and 1,549 (96.6%) participants completed the Day 57, Day 90, and Day 180 visits, respectively (Figure 1). Baseline characteristics between the groups were similar (Supplementary Table S1).
Figure 1.
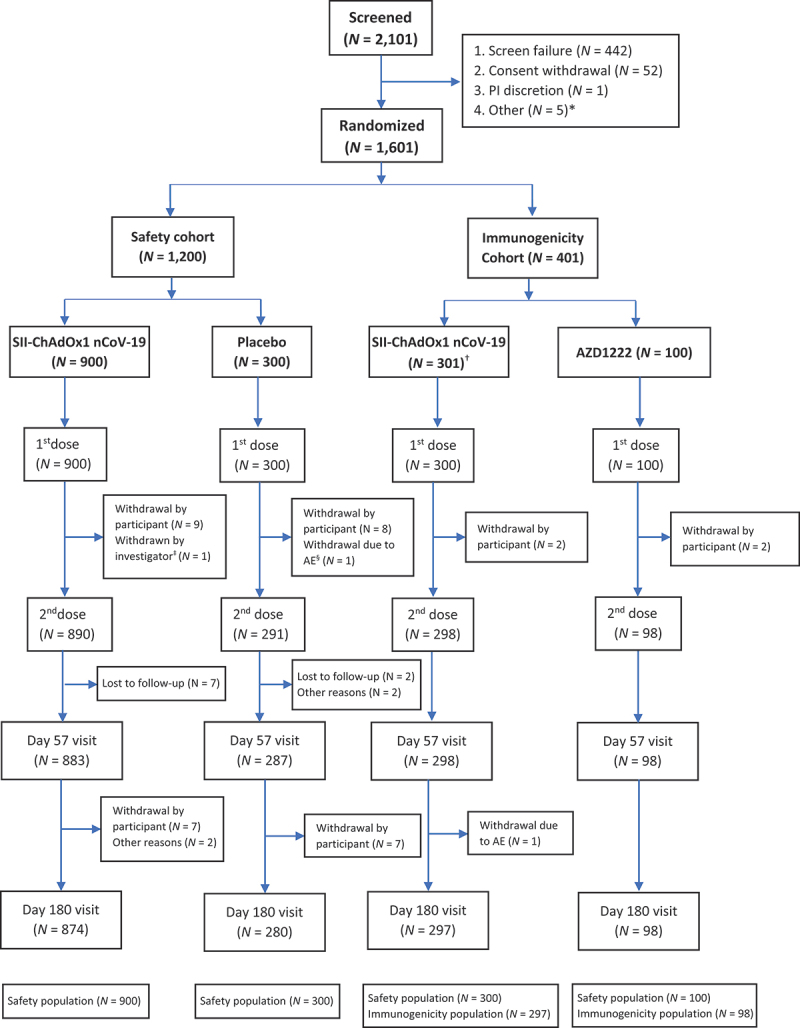
CONSORT flow chart.
*Participants did not go to their study site for the randomization visit within window period of 7 days after screening; †One participant withdrew consent before vaccination; ‡Participant was withdrawn by the investigator due to a neurological SAE; §Participant was withdrawn by the investigator on the Day 29 visit due to an AE of aggravation of hypertension. AE, adverse event; D, day; PI, principal investigator; SAE, serious adverse event.
In both vaccine groups, the anti-S GMTs were < 100 AU/mL at baseline, and increased to > 6,000 AU/mL after the first dose, and > 25,900 AU/mL after the second dose. Day 180, anti-S titers were 8,222 (95% CI: 6,650.2–10,165.8) AU/mL and 13,790.5 (95% CI: 9,845.7–19,315.9) AU/mL in the SII-ChAdOx1 nCoV-19 and AZD1222 groups, respectively. As previously reported, the anti-S GMT ratio between SII-ChAdOx1 nCoV-19 and AZD1222 on Day 57 was 0.98 (95% CI: 0.78–1.23),2 and on Day 180 was 0.60 (95% CI: 0.41–0.87) (Table 1). Anti-S GMTs showed similar trends in the seronegative population at baseline (Supplementary Table S2). The anti-S GMFR from baseline was > 325 in both vaccine groups on Day 57. On Day 180, the GMFR from baseline was 106.9 (95% CI: 83.7–136.7) in the SII-ChAdOx1 nCoV-19 group and 175.9 (95% CI: 105.7–292.7) in the AZD1222 group. In both vaccine groups, the anti-S seroconversion rate was ≥ 98% after the second dose, and ≥ 94% on Day 180 (Table 2; Supplementary Table S3).
Table 1.
Statistical assessments of anti-S and anti-RBD IgG and nAbs (immunogenicity analysis population).
| Anti-S |
Anti-RBD |
nAbs |
|||||
|---|---|---|---|---|---|---|---|
| Timepoint | Statistic | SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
| Visit 4 – Day 57 (+14) | n | 293 | 95 | 293 | 95 | 291 | 95 |
| GMT (95% CI) | 25,928.5 (22,422.1–29,983.2) |
26,495.2 (21,416.0–32,779.0) |
33,259.1 (28,458.4–38,869.6) |
33,817.2 (26,876.5–42,550.2) |
60.2 (50.7–71.4) |
53.9 (41.9–69.3) |
|
| Ratio of GMTs* (95% CI) | 0.98 (0.78–1.22) | 0.98 (0.77–1.25) | 1.12 (0.86–1.46) | ||||
| Visit 6 – Day 180 (+28) | n | 258 | 88 | 258 | 88 | 83 | 29 |
| GMT (95% CI) | 8,222.2 (6,650.2– 10,165.8) |
13,790.5 (9,845.7– 19,315.9) |
9,472.7 (7,554.3– 11,878.2) |
16,939.3 (11,818.2–24,279.6) |
18.1 (12.6–26.0) |
20.7 (11.4–37.6) |
|
| Ratio of GMTs* (95% CI) | 0.60 (0.41–0.87) | 0.56 (0.37–0.84) | 0.88 (0.44–1.73) | ||||
*Ratio of GMTs for anti-S and anti-RBD IgG and nAbs between the two vaccine groups on Day 57 and Day 180 are presented.
Anti-RBD, anti-receptor binding domain; anti-S, anti-spike; CI, confidence interval; GMFR, geometric mean fold rise; GMT, geometric mean titer; IgG, immunoglobulin G; nAb, neutralizing antibody.
Table 2.
Proportion of participants with seroconversion (immunogenicity analysis population).
| Anti-S |
Anti-RBD |
nAbs |
|||||
|---|---|---|---|---|---|---|---|
| Timepoint | Statistic | SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
SII-ChAdOx1 nCoV-19 (N = 297) |
AZD1222 (N = 98) |
| Visit 4 – Day 57 (+14) | N evaluated | 293 | 95 | 293 | 95 | 291 | 95 |
| Seroconversion, n (%)* | 287 (98.0) | 94 (98.9) | 284 (96.9) | 93 (97.9) | 249 (85.6) | 80 (84.2) | |
| 95% CI | 95.6–99.2 | 94.3–100.0 | 94.2–98.6 | 92.6–99.7 | 81.0–89.4 | 75.3–90.9 | |
| Visit 6 – Day 180 (+28) | N evaluated | 258 | 88 | 258 | 88 | 83 | 29 |
| Seroconversion, n (%)* | 243 (94.2) | 85 (96.6) | 236 (91.5) | 82 (93.2) | 47 (56.6) | 15 (51.7) | |
| 95% CI | 90.6–96.7 | 90.4–99.3 | 87.4–94.6 | 85.7–97.5 | 45.3–67.5 | 32.5–70.6 | |
*Seroconversion is defined as 4-fold rise in titer from baseline. Anti-RBD, anti-receptor binding domain; anti-S, anti-spike; CI, confidence interval; nAb, neutralizing antibody.
In both vaccine groups, the anti-RBD GMTs were < 200 AU/mL at baseline, and increased to > 5,600 AU/mL after the first dose, and > 33,000 AU/mL after the second dose. Day 180 anti-RBD GMTs were 9,472.7 (95% CI: 7,554.3–11,878.2) and 16,939.3 (11,818.2–24,279.6) in the SII-ChAdOx1 nCoV-19 and AZD1222 groups, respectively (Table 1). Anti-RBD GMTs showed similar trends in the seronegative population at baseline (Supplementary Table S2). Compared with baseline, the anti-RBD GMFR was > 225 on Day 57 in both vaccine groups. On Day 180, the GMFR from baseline was 66.6 (95% CI: 53.0–83.6) and 114.3 (95% CI: 70.6–185.0) in the SII-ChAdOx1 nCoV-19 and AZD1222 groups, respectively. In both vaccine groups, the anti-RBD seroconversion rate ≥ 96% after the second dose, and ≥ 91% on Day 180 (Table 2; Supplementary Table S3).
In both vaccine groups, the nAb GMTs were < 6 IU/mL at baseline, and increased to > 53 IU/mL after the second dose. Day 180 nAb GMTs were 18.1 (95% CI: 12.6–26.0) IU/mL and 20.7 (95% CI: 11.4–37.6) IU/mL in the SII-ChAdOx1 nCoV-19 and AZD1222 groups, respectively, with a GMT ratio of 0.88 (95% CI: 0.44–1.73) (Table 1). nAb GMTs showed similar trends in the seronegative population at baseline (Supplementary Table S2). Compared with baseline, the nAb GMFR was > 12 in both vaccine groups on Day 57. On Day 180, the nAb GMFR from baseline was 4.9 (95% CI: 3.4–7.1) in the SII-ChAdOx1 nCoV-19 group and 6.4 (95% CI: 2.8–14.9) in the AZD1222 group. The nAb seroconversion rate was ≥ 84% after the second dose; however, it declined to ≥ 51% on Day 180 in both vaccine groups (Table 2; Supplementary Table S3).
Among the 1,600 participants, a total of 27 SAEs were reported in 27 (1.7%) participants: 21 of the 1,200 participants who received SII-ChAdOx1 nCoV-19 (1.8%, 95% CI: 1.1–2.7), 4 of the 300 participants who received placebo (1.3%, 95% CI: 0.4–3.4), and 2 of the 100 participants who received AZD1222 (2.0%, 95% CI: 0.2–7.0) (Table 3). These SAEs included COVID-19 (n = 17), fracture/dislocation (n = 3), and one case each of malaria, megaloblastic anemia, cataract, liver cirrhosis, invasive ductal breast carcinoma, encephalopathy, and vocal cord cyst. All SAEs resolved without any sequalae, and none were adjudged to be causally related to the study vaccines. There were no thromboembolic or autoimmune AESIs. The incidence of COVID-19 was low in both vaccine groups during the study (Supplementary Table S4).
Table 3.
Summary of unsolicited AEs after any vaccination (overall safety population).
| SII-ChAdOx1 nCoV-19 (N = 1,200) n (%) [E] |
Placebo (N = 300) n (%) [E] |
AZD1222 (N = 100) n (%) [E] |
|
|---|---|---|---|
| Any AE within 30 minutes after vaccination | 15 (1.3) [16] | 4 (1.3) [5] | 0 |
| Any AE | 352 (29.3) [602] | 72 (24.0) [101] | 20 (20.0) [32] |
| Severe | 3 (0.3) [3] | 1 (0.3) [1] | 0 |
| Any treatment-related AE | 236 (19.7) [384] | 39 (13.0) [50] | 0 |
| Any SAE | 21 (1.8) [21] | 4 (1.3) [4] | 2 (2.0) [2] |
| Related SAE | 0 | 0 | 0 |
AE, adverse event; E, number of events; n, participants reporting at least one AE; N, total number of participants in a group; SAE, serious adverse event.
Discussion
Here, we present the immunogenicity and safety of the SII-ChAdOx1 nCoV-19 vaccine, as compared to AZD1222 and placebo, in Indian adults 6 months after first-dose primary series vaccination. Despite high antibody titers (anti-S, anti-RBD, and nAb) at Day 57 (i.e., 1 month after the second dose), a substantial decline in antibody titers was observed at Day 180; however, Day 180 titers remained higher than baseline titers. Our finding of waning antibody titers is consistent with previous studies illustrating significant reduction in antibody titers in the months following natural SARS-CoV-2 infection.8,9 Similar immunological waning of anti-S, and nAb titers has been reported with all available COVID-19 vaccines across mRNA, viral vector, inactivated, and subunit vaccine platforms.4–6
SARS-CoV-2 reinfections have been observed within a few months of initial infection, and increasing numbers of breakthrough cases have been reported in countries with early vaccine rollouts/deployment, indicating waning vaccine effectiveness after primary series COVID-19 vaccination.10–12 In a previous AZD1222 study with follow-up of vaccine effectiveness against symptomatic and severe COVID-19 over 20 weeks, protection against severe outcomes was shown to be sustained, while protection against non-severe COVID-19 declined to an estimated 44% by 20 weeks.13 Our findings with SII-ChAdOx1 nCoV-19 are consistent with these results. No case of severe COVID-19 was reported in either vaccine group despite the high prevalence of the SARS-CoV-2 Delta variant in India from March to June 2021.14 Longer term protection against other variants has not been characterized in India; however, waning of protection against severe disease due to SARS-CoV-2 Omicron infection has been reported after 6 months of primary vaccination in other geographical regions.15 Our current results indicate a decline in anti-S and nAb titers over 6 months post vaccination, underscoring the importance of using booster doses to restore waning antibody levels and maintain protection against symptomatic disease.16,17
SII-ChAdOx1 nCoV-19 has been shown to be non-inferior to AZD1222 in terms of anti-S antibodies at Day 572; while Day-180 results showed evidence of higher anti-S antibodylevels after AZD1222 than SII-ChAdOx1 nCoV-19, the difference in nAb levels was not as marked. The differences observed may be related to background heterogeneity in the context of a relatively limited overall sample size and different AZD1222 vs SII-ChAdOx1 nCoV-19 population sizes (3:1 randomization), at a time of very intense SARS-CoV-2 Delta variant community transmission (March – June 2021).14 Moreover, immunogenicity assessment at Day 180 timepoint was not statistically powered.
Despite the observed decay in antibody levels, there was no case of severe COVID-19 in either vaccine group. No safety concerns were observed at 6 months after the first dose, with no reports of vaccine-related SAEs or AESIs. AZD1222 has also previously shown an acceptable safety profile in a large phase 3 efficacy trial.18 There was only one case of severe COVID-19 in the placebo group, which required prolonged hospitalization, including intensive care and mechanical ventilation, and no deaths due to COVID-19 occurred in the study.
Our study had a few limitations. Firstly, we did not assess AZD1222 vaccine effectiveness, as this has already been established in previous analyses of multiple Phase 2/3 clinical trials (66.7%, 95% CI 57.4–74.019 and 74%, 95% CI 65.3–80.5).18 Secondly, although our findings underline the need for booster dosing following primary series vaccination, we did not assess the booster response of SII-ChAdOx1 nCoV-19/ AZD1222 in this study; this has however been assessed in other studies.20–22 Finally, our study population was relatively healthy (i.e.,~23% of participants had comorbidities), which somewhat limited our insight into immunogenicity/safety outcomes among people with comorbidities who are known to be at high risk of severe COVID-19; however, previous reports have demonstrated no difference in AZD1222 efficacy based on comorbidity status.18
To conclude, SII-ChAdOx1 nCoV-19 is highly immunogenic and has an acceptable long-term safety profile, but booster doses are likely to be needed due to immunological waning 6 months after primary series vaccination. These data support the continued use of SII-ChAdOx1 nCoV-19 to mitigate the COVID-19 pandemic.
Supplementary Material
Acknowledgments
We sincerely thank all the study participants and all the study team members. Medical editing assistance was provided by Laura Winton, BSc, and Craig O’Hare, PhD, of Ashfield MedComms, an Inizio company, which was in accordance with Good Publication Practice (GPP) 2022 guidelines (https://www.ismpp.org/gpp-2022; Ann Intern Med 2022 doi:10.7326/M22-1460) and funded by AstraZeneca.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Funding Statement
The study was funded by SIIPL and the Indian Council of Medical Research. SIIPL funded the contract research organization and laboratory costs, while the site costs were funded by the Indian Council of Medical Research. The study vaccines were supplied by SIIPL and AstraZeneca.
Contributor Information
Collaborators: Anand Kawade, Arunkumar Gondhali, Mini P. Singh, Ritin Mohindra, Pratibha Pereiera, M R Narayana Murthy, Abhishek V. Raut, Chetna Maliye, Ashwini Kalantri, Vijaya L L Chaudhari, Charuta J Godbole, Malangori Parande, Nandakumar Salunke, Sonali Palkar, Neeta Hanumante, Piyush Chaudhari, Shilpa Karande, Dipti Kumbhar, Shilpa Gupta, Sajal Mitra, S Sudharshini, Prakash Venkatesan, Madhukar -, Abhik Sen, Sunita Sreegiri, Venkata Durga Prasad Vithanala, Tamilanbu Panneerselvam, Aiswarya M Nair, Atul Chaudhari, and Silvester Patil
Disclosure statement
The authors declare the following financial interests/personal relationships, which may be considered as potential competing interests: Cyrus S. Poonawalla is Chairman and Managing Director of Serum Institute of India Pvt. Ltd. Prasad S. Kulkarni, Chetanraj Bhamare, Abhijeet Dharmadhikari, Manish Gautam, Umesh Shaligram, Dhananjay Kapse, and Bhagwat Gunale are employed by Serum Institute of India Pvt. Ltd, which manufactures SII-ChAdOx1 nCoV-19 (COVID-19) vaccine. Chandrasekaran Padmapriyadarsini, Madhuri Thakar, Swarali N. Kurle, Nivedita Gupta, Samiran Panda, and Balram Bhargava are employed by ICMR. Johan Vekemans and Elizabeth J. Kelly are former employees of AstraZeneca and may hold AstraZeneca stock or stock options. Ashish Bavdekar, Madhu Gupta, Praveen Kulkarni, B.S. Garg, Nithya J. Gogtay, Muralidhar Tambe, Sanjay Lalwani, Kiranjit Singh, Renuka Munshi, Sushant Meshram, T.S. Selvavinayagam, Krishna Pandey, Devi Madhavi Bhimarasetty, S.R. Ramakrishnan, Chandrashekhar Budhawant, and Cyrille J. Bonhomme declare no potential conflicts of interest.
Author contributors
PSK, DK, BG, JV, US, CP, NG, SP, and CSP contributed to the study design and protocol development. PSK, DK, and BG accessed and verified the data. CJB, MT, and SNK led the immunogenicity experiments. CB contributed to the analysis. PSK, DK, and BG contributed to the manuscript preparation. The manuscript was finalized with considerable input from all authors. AB, MG, PK, BSG, NJG, MT, SL, KS, RM, SM, TSS, KP, DMB, and SRR contributed to data collection. EJK, US, and MG contributed to immunogenicity experiment oversight and supervision.
Data availability statement
Individual-level participant data will not be made available to others due to privacy concerns.
supplementary data
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2024.2304974.
References
- 1.Ministry of Health and Family Welfare. Government of India. Coronavirus Dashboard. National Informatics Centre . 2023. [accessed 2023 Feb 1]. https://www.mohfw.gov.in/.
- 2.Kulkarni PS, Padmapriyadarsini C, Vekemans J, Bavdekar A, Gupta M, Kulkarni P, Garg BS, Gogtay NJ, Tambe M, Lalwani S, et al. A phase 2/3, participant-blind, observer-blind, randomised, controlled study to assess the safety and immunogenicity of SII-ChAdOx1 nCoV-19 (COVID-19 vaccine) in adults in India. EClinicalMedicine. 2021;42:101218. doi: 10.1016/j.eclinm.2021.101218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization . WHO lists two additional COVID-19 vaccines for emergency use and COVAX roll-out. WHO; 2021. [accessed 2023 Feb 1]. https://www.who.int/news/item/15-02-2021-who-lists-two-additional-covid-19-vaccines-for-emergency-use-and-covax-roll-out. [Google Scholar]
- 4.Jo DH, Minn D, Lim J, Lee KD, Kang YM, Choe KW, Kim K-N.. Rapidly declining SARS-CoV-2 antibody titers within 4 months after BNT162b2 vaccination. Vaccines (Basel). 2021;9(10):1145. doi: 10.3390/vaccines9101145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Favresse J, Bayart JL, Mullier F, Elsen M, Eucher C, Van Eeckhoudt S, Roy T, Wieers G, Laurent C, Dogné J-M, et al. Antibody titres decline 3-month post-vaccination with BNT162b2. Emerg Microbes Infect. 2021;10(1):1495–8. doi: 10.1080/22221751.2021.1953403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barouch DH, Stephenson KE, Sadoff J, Yu J, Chang A, Gebre M, McMahan K, Liu J, Chandrashekar A, Patel S, et al. Durable humoral and cellular immune responses 8 months after Ad26.COV2.S vaccination. N Engl J Med. 2021;385(10):951–3. doi: 10.1056/NEJMc2108829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sobieszczyk ME, Maaske J, Falsey AR, Sproule S, Robb ML, Frenck RW, Tieu H-V, Mayer KH, Corey L, Neuzil KM, et al. Durability of protection and immunogenicity of AZD1222 (ChAdox1 nCoV-19) COVID-19 vaccine over 6 months. J Clin Invest. 2022 Sep 15;132(18):e160565. doi: 10.1172/JCI160565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhu L, Xu X, Zhu B, Guo X, Xu K, Song C, Fu J, Yu H, Kong X, Peng J, et al. Kinetics of SARS-CoV-2 specific and neutralizing antibodies over seven months after symptom onset in COVID-19 patients. Microbiol Spectr. 2021;9(2):e0059021. doi: 10.1128/Spectrum.00590-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Griffante G, Chandel S, Ferrante D, Caneparo V, Capello D, Bettio V, Borgogna C, Aleni C, Esposito S, Sarro A, et al. Persistence of neutralizing antibodies to SARS-CoV-2 in first wave infected individuals at ten months post-infection: the UnIRSA cohort study. Viruses. 2021;13(11):2270. doi: 10.3390/v13112270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.To KK, Hung IF, Ip JD, Chu AW, Chan WM, Tam AR, Fong CHY, Yuan S, Tsoi H-W, Ng ACK, et al. Coronavirus disease 2019 (COVID-19) re-infection by a phylogenetically distinct severe acute respiratory syndrome coronavirus 2 strain confirmed by whole genome sequencing. Clin Infect Dis. 2021;73(9):e2946–e51. doi: 10.1093/cid/ciaa1275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chan PKS, Lui G, Hachim A, RLW K, Boon SS, Li T, Kavian N, Luk F, Chen Z, Yau EM, et al. Serologic responses in healthy adult with SARS-CoV-2 reinfection, Hong Kong, August 2020. Emerg Infect Dis. 2020;26(12):3076–8. doi: 10.3201/eid2612.203833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gopinath S, Ishak A, Dhawan N, Poudel S, Shrestha PS, Singh P, Xie E, Tahir P, Marzaban S, Michel J, et al. Characteristics of COVID-19 breakthrough infections among vaccinated individuals and associated risk factors: a systematic review. Trop Med Infect Dis. 2022;7(5):81. doi: 10.3390/tropicalmed7050081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Andrews N, Tessier E, Stowe J, Gower C, Kirsebom F, Simmons R, Gallagher E, Thelwall S, Groves N, Dabrera G, et al. Duration of protection against mild and severe disease by COVID-19 vaccines. N Engl J Med. 2022;386(4):340–50. doi: 10.1056/NEJMoa2115481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yang W, Shaman J. COVID-19 pandemic dynamics in India, the SARS-CoV-2 delta variant and implications for vaccination. J R Soc Interface. 2022;19(191):20210900. doi: 10.1098/rsif.2021.0900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Feikin DR, Abu-Raddad LJ, Andrews N, Davies MA, Higdon MM, Orenstein WA, Patel MK. Assessing vaccine effectiveness against severe COVID-19 disease caused by omicron variant. Report from a meeting of the World Health Organization. Vaccine. 2022;40(26):3516–27. doi: 10.1016/j.vaccine.2022.04.069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Feng S, Phillips DJ, White T, Sayal H, Aley PK, Bibi S, Dold C, Fuskova M, Gilbert SC, Hirsch I, et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat Med. 2021;27(11):2032–40. doi: 10.1038/s41591-021-01540-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, Subbarao K, Kent SJ, Triccas JA, Davenport MP, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med. 2021;27(7):1205–11. doi: 10.1038/s41591-021-01377-8. [DOI] [PubMed] [Google Scholar]
- 18.Falsey AR, Sobieszczyk ME, Hirsch I, Sproule S, Robb ML, Corey L, Neuzil KM, Hahn W, Hunt J, Mulligan MJ, et al. Phase 3 safety and efficacy of AZD1222 (ChAdox1 nCoV-19) COVID-19 vaccine. N Engl J Med. 2021;385(25):2348–60. doi: 10.1056/NEJMoa2105290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Voysey M, Costa Clemens SA, Madhi SA, Weckx LY, Folegatti PM, Aley PK, Angus B, Baillie VL, Barnabas SL, Bhorat QE, et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: a pooled analysis of four randomised trials. Lancet. 2021. Mar 6;397(10277):881–91. doi: 10.1016/S0140-6736(21)00432-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kulkarni PS, Gunale B, Kohli S, Lalwani S, Tripathy S, Kar S, Raut S, Kulkarni P, Apte A, Bavdekar A, et al. A phase 3, randomized, non-inferiority study of a heterologous booster dose of SARS CoV-2 recombinant spike protein vaccine in adults. Sci Rep. 2023;13(1):16579. doi: 10.1038/s41598-023-43578-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Munro APS, Janani L, Cornelius V, Aley PK, Babbage G, Baxter D, Bula M, Cathie K, Chatterjee K, Dodd K, et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): a blinded, multicentre, randomised, controlled, phase 2 trial. Lancet. 2021;398(10318):2258–76. doi: 10.1016/S0140-6736(21)02717-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rose W, Raju R, Babji S, George A, Madhavan R, Leander Xavier JV, David Chelladurai JS, Nikitha OS, Deborah AA, Vijayakumar S, et al. Immunogenicity and safety of homologous and heterologous booster vaccination of ChAdOx1 nCoV-19 (COVISHIELD™) and BBV152 (COVAXIN®): a non-inferiority phase 4, participant and observer-blinded, randomised study. Lancet Reg Health Southeast Asia. 2023;12:100141. doi: 10.1016/j.lansea.2023.100141. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Individual-level participant data will not be made available to others due to privacy concerns.