

This cohort study assesses differences in donor heart acceptance by transplant center teams for Black and White men and women on the transplant waiting list in the US.
Abstract
Importance
Barriers to heart transplant must be overcome prior to listing. It is unclear why Black men and women remain less likely to receive a heart transplant after listing than White men and women.
Objective
To evaluate whether race or gender of a heart transplant candidate (ie, patient on the transplant waiting list) is associated with the probability of a donor heart being accepted by the transplant center team with each offer.
Design, Setting, and Participants
This cohort study used the United Network for Organ Sharing datasets to identify organ acceptance with each offer for US non-Hispanic Black (hereafter, Black) and non-Hispanic White (hereafter, White) adults listed for heart transplant from October 18, 2018, through March 31, 2023.
Exposures
Black or White race and gender (men, women) of a heart transplant candidate.
Main Outcomes and Measures
The main outcome was heart offer acceptance by the transplant center team. The number of offers to acceptance was assessed using discrete time-to-event analyses, nonparametrically (stratified by race and gender) and parametrically. The hazard probability of offer acceptance for each offer was modeled using generalized linear mixed models adjusted for candidate-, donor-, and offer-level variables.
Results
Among 159 177 heart offers with 13 760 donors, there were 14 890 candidates listed for heart transplant; 30.9% were Black, 69.1% were White, 73.6% were men, and 26.4% were women. The cumulative incidence of offer acceptance was highest for White women followed by Black women, White men, and Black men (P < .001). Odds of acceptance were less for Black candidates than for White candidates for the first offer (odds ratio [OR], 0.76; 95% CI, 0.69-0.84) through the 16th offer. Odds of acceptance were higher for women than for men for the first offer (OR, 1.53; 95% CI, 1.39-1.68) through the sixth offer and were lower for the 10th through 31st offers.
Conclusions and Relevance
The cumulative incidence of heart offer acceptance by a transplant center team was consistently lower for Black candidates than for White candidates of the same gender and higher for women than for men. These disparities persisted after adjusting for candidate-, donor-, and offer-level variables, possibly suggesting racial and gender bias in the decision-making process. Further investigation of site-level decision-making may reveal strategies for equitable donor heart acceptance.
Key Points
Question
Is the race or gender of a patient on the heart transplant waiting list associated with the probability of a donor heart being accepted by the transplant center team with each offer?
Findings
In this cohort study of 159 177 heart offers with 13 760 donors and 14 890 candidates, there was a statistically significant difference among the race and gender strata in the cumulative incidence functions, with the cumulative incidence of heart offer acceptance being consistently highest for White women followed by Black women, White men, and Black men.
Meaning
The findings suggest that race and gender are significantly associated with the probability of donor heart acceptance and that investigation is needed to change modifiable factors contributing to these disparities.
Introduction
Racial, ethnic, and gender disparities in heart transplant allocation have persisted in the US.1,2 Black patients and women have disproportionately lower rates of receipt of a heart transplant than White patients and men.1,2,3 Approximately 40% of heart transplant recipients are from minoritized racial and ethnic groups, and approximately 25% of heart transplant recipients are women.4 Meanwhile, Black patients have 2- to 3-times greater risk of developing heart failure than White patients and have the highest risk of dying from heart failure compared with all other racial and ethnic groups.5,6 Women have a modestly lower risk of heart failure than men.7 There are some caveats. Although women with the heart failure phenotype are often not eligible for heart transplant, when addressing the intersectionality of race and ethnicity with gender, minoritized groups such as Black women often have the appropriate clinical phenotype for heart transplant.8 Ultimately, Black patients and women are consistently less likely to be listed for heart transplant.4 Black patients are less likely to receive a heart transplant after listing and more likely to die while waiting for a heart transplant than their peers from other racial and ethnic groups.4
Reasons for racial, ethnic, and gender disparities in accessing heart transplant are becoming clearer, but some factors remain elusive. Multiple studies have identified significant contributors to inequitable allocation, such as variable referral patterns, inequitable transplant team decision-making during selection for listing (subjectivity in the assessment of social support systems and adherence, variability in the weight of social determinants of health, and poor group dynamics), and clinical factors.1,2,9,10,11,12,13,14,15 Bias against minoritized groups has also contributed to the inequitable allocation processes.9,10,14 It is unclear why minoritized racial and ethnic groups and women are less likely to receive a transplant after these barriers have been addressed to the point that the patient is deemed appropriate to be listed for heart transplant.
When a patient is listed for a heart transplant (ie, becomes a candidate for transplant), the matching process for candidates and donors is fairly standardized (a glossary of terms is given in the Box).16,17 A computer algorithm ranks and matches candidates and donors according to candidate characteristics (eg, severity of illness and urgency for transplant, location of the transplant center, and blood type) and prespecified donor characteristics (eg, blood type, donor hospital location). Then, a transplant center is notified with an offer when the candidate is next in line with a matching donor. The designated team members at a transplant center must then review donor data and decide whether to accept the organ donation. While the matching process follows an algorithm, the decision to accept an offer is more nuanced and subjective.
Box. Glossary of Termsa.
Bypassed offer: skipping rank due a transplant center’s filters for a suitable donation, directed donation, multiorgan placement, or natural disaster.
Candidate: patient listed for and awaiting transplant.
Donor: patient who has donated organs.
Match run: match of candidates to organ donors by rank.
Offer: a donor’s organ is offered or propositioned to a matching candidate. When an offer is made, the candidate’s transplant team must determine whether or not to accept the organ donation. If the offer is not accepted, it is offered to the next ranked candidate.
Rank: computer-generated order of candidates according to specified donor and candidate characteristics including clinical severity and urgency for transplant and waiting list time.
Recipient: patient who has received an organ transplant.
There is a need to reduce disparities in the transplant allocation process in the US. Since the 2022 National Academies of Sciences, Engineering, and Medicine recommendation to improve equitable distribution and reduce nonuse of donated organs in the US transplant system, multiple changes have been initiated by the United Network for Organ Sharing (UNOS), the US governing body for organ transplants.18 Over the next few years, all UNOS organ allocation programs will have a new method in place that uses a point system to calculate transplant candidate rank order for each organ donor and has additional changes for equity.19 Thus, we used the UNOS public use data sets to understand factors contributing to inequitable receipt of heart transplant by race and gender after a patient has been listed for transplant. Foremost, we aimed to investigate whether the race and gender of a heart transplant candidate are associated with likelihood of donor organ acceptance by the transplant center team after adjusting for clinical indications that support good outcomes. We hypothesized that Black candidates and women would have lower odds of donor organ acceptance for each offer compared with White candidates and men. This study is important given the need for more equitable allocation of heart transplants.
Methods
Data Source
This cohort study used publicly available, deidentified data obtained from the UNOS Standard Transplant Analysis and Research data set and the Potential Transplant Recipient dataset. As the governing body for transplant and organ donation in the US, UNOS collects data on all organ donors, transplant candidates, and transplant recipients (eTable 1 in Supplement 1). Data include demographics, clinical characteristics, and longitude and latitude of transplant centers. This study was deemed exempt from review and informed consent by the Indiana University institutional review board. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Study Population
Heart transplant candidates were included if they were on the waiting list for a single organ, aged at least 18 years on their listing date, and listed from October 18, 2018 (date of last UNOS heart transplant policy change), through March 31, 2023. We limited this analysis to patients with stated race and ethnicity of either non-Hispanic Black (hereafter, Black) or non-Hispanic White (hereafter, White). Other racial and ethnic groups were not included in initial analyses due to lower frequencies and added complexity of analyses and interpretation. Future work will address additional racial and ethnic groups. We limited match runs to those in which the donor heart was ultimately accepted and the donor was at least 16 years of age. Bypassed offers were excluded. This resulted in 14 890 candidates with 1 or more offers (eFigure 1 in Supplement 1). For a given candidate, we included offers up to the first accepted offer, resulting in a total of 171 974 offers. Offers were then numbered sequentially for each candidate.
Study Outcomes
The primary outcome was the number of offers for a candidate until the first acceptance of a donor heart, assessed using discrete time-to-event analyses. Each offer of a donor heart to a candidate was treated as a discrete trial in which the event (offer acceptance) could occur or not occur (success or failure, respectively). Discrete time-to-event analysis models the hazard, where the hazard at trial t is defined as the probability that the event occurs at trial t, conditional on the event not having occurred prior to trial t: h(t) = P(T = t | T ≥ t).
The independent variables of interest were candidate race (Black, White) and gender (men, women). Race and gender were identified by transplant sites and supplied to UNOS. UNOS relabeled the gender category to birth sex as of September 2023,20 which followed completion of this study. We describe the study using gender and sex interchangeably because both gender and sex may contribute to study findings as a social construct and biological variable.
Statistical Analysis
Kaplan-Meier estimates of survival, stratified by race and gender, were obtained using the survival package in R, version 4.2.3 (R Project for Statistical Computing).21,22 To calculate quantiles of the number of offers until acceptance, we included all offers up to the first accepted offer for each candidate (a total of 171 974 offers). To compare survival among strata using a log-rank test, we included only the first 50 offers for each candidate (a total of 159 177 offers; 90.6% of all candidates had an offer accepted by the 50th offer), which is equivalent to censoring candidates after the 50th offer. Estimates of survival were converted to cumulative incidence of offer acceptance for interpretability.
The hazard of offer acceptance for each offer was modeled using a generalized linear mixed model with logit-link in R package lme4.23 For this analysis, we also included only the first 50 offers for each candidate. The effect of time (offer number) was modeled using a cubic spline. We included effects of race (Black or White), gender (man or woman), and interactions of race with time and gender with time. We initially included a race-gender interaction and a race-gender-time interaction; however, these interactions were not statistically significant (P > .05), so we excluded them from the final model for the sake of interpretability. Other model covariates included those that may directly affect the decision to accept an organ: donor history of cancer, whether or not the candidate had a ventricular assist device (VAD) at listing (time to explant affects ischemic time), offer rank (the order in which an organ is offered to candidates, which addresses candidate’s severity of illness for status listing), the distance between the donor’s hospital and the candidate’s listing center (affects ischemic time), donor age, candidate age, donor ejection fraction, and percentage difference in donor and candidate predicted heart mass. Finally, we included a random intercept for donor that accounts for other donor characteristics that were constant across offers. We used multiple imputation to account for missing values. In all, 4039 of 159 177 offers (2.5%) had 1 or more missing values for variables used in the model. We performed additional sensitivity analyses with complete case variables that had too many missing data for inclusion in the original model. These included pulmonary vascular resistance (PVR; missing for 19.3% at listing) and calculated panel reactant antibody (cPRA) level (missing for 11.0% at listing). The recent changes in the availability of donated organs via donation after cardiac death rather than donation only after brain death were addressed in sensitivity analyses. Two-sided P < .05 was considered significant. The eMethods in Supplement 1 provide additional details.
Results
Transplant Candidates, Organ Donors, and Offers
After applying inclusion criteria, the final population included 14 890 candidates listed for heart transplant, including 4608 Black individuals (30.9%), 10 282 White individuals (69.1%), 10 956 men (73.6%), and 3934 women (26.4%) (Table 1). Among these candidates, the number of offers ranged from 1 to 243 (median, 6 [IQR, 2-14]). We observed an accepted offer for 72.5% of candidates. Overall, Black women and men and White women were younger at listing than White men. Predicted heart mass was lower for women than for men. A total of 3.8% of patients were receiving extracorporeal membrane oxygenation at listing. White men had the highest proportion of prior non-VAD cardiac surgeries, and Black men had the highest proportion of VADs at listing. The most common waiting list status across strata was 4 (a status of 1 indicates highest severity of illness, and 6 indicates lowest severity). Median cPRA level was less than 2% for all candidate groups, and median PVR was less than 3 millimeters of Hg × min/L for all candidate groups.
Table 1. Heart Transplant Candidate Characteristics.
| Characteristic | Candidates (N = 14 890)a | |||
|---|---|---|---|---|
| Black women (n = 1411 [9.5%]) | Black men (n = 3197 [21.5%]) | White women (n = 2523 [16.9%]) | White men (n = 7759 [52.1%]) | |
| Age at listing, median (IQR), y | 53 (41-61) | 54 (44-61) | 54 (42-62) | 59 (49-65) |
| Height, median (IQR), cm | 165 (160-170) | 180 (174-185) | 163 (159-168) | 178 (173-183) |
| Weight, median (IQR), kg [n] | 77.6 (65.8-89.8) [1409] | 91.0 (78.5-104.8) [3191] | 72.6 (61.2-84.8) [2521] | 89.0 (78.0-101.2) [7753] |
| Predicted heart mass, median (IQR), g [n] | 148 (134-162) [1409] | 203 (184-223) [3191] | 142 (129-156) [2521] | 199 (183-216) [7753] |
| PVR at listing, median (IQR), % [n] | 2.5 (1.7-3.5) [1169] | 2.3 (1.6-3.1) [2610] | 2.2 (1.5-3.2) [2004] | 2.0 (1.4-2.8) [6239] |
| cPRA at listing, median (IQR), mm of Hg × min/L [n] | 1 (0-49) [1261] | 0 (0-4) [2811] | 0 (0-30) [2253] | 0 (0-0) [6959] |
| Receiving ECMO at listing | 37 (2.6) | 107 (3.3) | 122 (4.8) | 295 (3.8) |
| History of tobacco use | 417/1397 (29.8) | 1267/3133 (40.4) | 881/2490 (35.4) | 3510/7642 (45.9) |
| VAD device at listing | ||||
| LVAD | 354 (25.1) | 1035 (32.4) | 438 (17.4) | 2037 (26.3) |
| LVAD and RVAD | 9 (0.6) | 40 (1.3) | 26 (1.0) | 92 (1.2) |
| RVAD | 1 (0.1) | 6 (0.2) | 6 (0.2) | 21 (0.3) |
| TAH | 1 (0.1) | 14 (0.4) | 5 (0.2) | 14 (0.2) |
| Prior non-VAD cardiac surgery at listing | 418/1349 (31.0) | 1061/3060 (34.7) | 889/2411 (36.9) | 3236/7412 (43.7) |
| Diagnosis at listing | ||||
| Dilated cardiomyopathy | 1060/1397 (75.9) | 2220/3133 (70.9) | 1265/2490 (50.8) | 3339/7642 (43.7) |
| Coronary artery disease | 124/1397 (8.9) | 515/3133 (16.4) | 464/2490 (18.6) | 2891/7642 (37.8) |
| Restrictive myopathy | 54/1397 (3.9) | 179/3133 (5.7) | 135/2490 (5.4) | 328/7642 (4.3) |
| Retransplant | 40/1397 (2.9) | 69/3133 (2.2) | 123/2490 (4.9) | 197/7642 (2.6) |
| Valvular heart disease | 20/1397 (1.4) | 18/3133 (0.6) | 32/2490 (1.3) | 90/7642 (1.2) |
| Otherb | 99/1397 (7.1) | 132/3133 (4.2) | 471/2490 (18.9) | 797/7642 (10.4) |
| Initial waiting list statusc | ||||
| 1 | 48 (3.4) | 147 (4.6) | 158 (6.3) | 422 (5.4) |
| 2 | 362 (25.7) | 909 (28.4) | 546 (21.6) | 1915 (24.7) |
| 3 | 179 (12.7) | 361 (11.3) | 238 (9.4) | 775 (10.0) |
| 4 | 513 (36.4) | 1180 (36.9) | 967 (38.3) | 2814 (36.3) |
| 5 | 50 (3.5) | 135 (4.2) | 45 (1.8) | 164 (2.1) |
| 6 | 249 (17.6) | 444 (13.9) | 549 (21.8) | 1608 (20.7) |
| Temporarily inactive | 10 (0.7) | 21 (0.7) | 20 (0.8) | 61 (0.8) |
Abbreviations: cPRA, calculated panel reactive antibody; ECMO, extracorporeal membrane oxygenation; LVAD, left ventricular assist device; PVR, pulmonary vascular resistance; RVAD, right VAD; TAH, total artificial heart.
Data are presented as number or number/total number (percentage) of candidates unless otherwise indicated.
Cancer, muscular dystrophy, and United Network for Organ Sharing category of “other” diagnosis.
A status of 1 indicates highest severity of illness, and 6 indicates lowest severity.
There was a total of 159 177 offers in the analysis set, with 13 760 donors (donor characteristics are shown in Table 2). Of these offers, rank ranged from 1 to 1468 (median, 25 [IQR, 8-79]), distance ranged from 0 to 2967 miles (median, 300 miles [IQR, 157-496 miles]), and the percentage difference in predicted heart mass ranged from −61% to 176% (median, −8% [IQR, −21% to 8%]).
Table 2. Heart Donor Characteristics.
| Characteristic | Donors (N = 13 760)a |
|---|---|
| Gender | |
| Female | 4062 (29.5) |
| Male | 9698 (70.5) |
| Age, median (IQR), y | 32 (25-40) |
| Ejection fraction, median (IQR), % [n] | 60 (55-65) [13 751] |
| Height, median (IQR), cm | 175 (168-180) |
| Weight, median (IQR), kg [n] | 81.7 (70.7-95.7) [13 756] |
| Predicted heart mass, median (IQR), g [n] | 186 (163-207) [13 756] |
| History of cancer | 177/13 593 (1.3) |
| Infection type | |
| Pulmonary | 9953 (72.3) |
| Blood | 1601 (11.6) |
| Urinary | 1580 (11.5) |
| Other | 1073/10 806 (9.9) |
| History of cocaine use | 3824/13 120 (29.1) |
| Risk of bloodborne disease transmission | 4178 (30.4) |
| History of diabetes, y | |
| >10 | 130/13 579 (1.0) |
| 6-10 | 77/13 579 (0.6) |
| 0-5 | 267/13 579 (2.0) |
| Cause of death | |
| Anoxia | 6388 (46.4) |
| Head trauma | 5244 (38.0) |
| Cerebrovascular or stroke | 1773 (12.9) |
| CNS tumor | 51 (0.4) |
| Other | 324 (2.4) |
Abbreviation: CNS, central nervous system.
Data are presented as number or number/total number (percentage) of donors unless otherwise indicated.
Outcomes
Overall, 11.4% (95% CI, 10.8%-11.9%) of first offers were accepted. After the first offer, the hazard rate (the probability that the ith offer was accepted given offers 1 to i − 1 were not) declined before leveling off around the 25th offer (eFigure 2 in Supplement 1).
Cumulative incidence curves differed by race and gender combination (log-rank test, P < .001), and there was notable separation even at the first offer. White women had the highest proportion of first offers accepted (17.5%; 95% CI, 16.0%-18.9%) followed by Black women (14.0%; 95% CI, 12.1%-15.8%), White men (10.3%; 95% CI, 9.6%-11.0%), and Black men (7.9%; 95% CI, 7.0%-8.8%), for whom the rate was less than half that for White women. This ordering was consistent up to the 50th offer (Figure 1 and eFigure 3 in Supplement 1 with confidence bands). By the tenth offer, more than two-thirds of White women had an offer accepted (68.4%; 95% CI, 66.3%-70.3%) but less than half of Black men had an offer accepted (48.0%; 95% CI, 46.0%-49.8%). The median number of offers until an offer was accepted was lowest for White women (5; 95% CI, 5-6) followed by Black women (7; 95% CI, 6-8), White men (9; 95% CI, 9-9), and Black men (11; 95% CI, 11-12) (eTable 2 in Supplement 1 gives additional quantiles and 95% CIs). Most candidates had an offer accepted by the 50th offer (eFigure 4 in Supplement 1).
Figure 1. Cumulative Incidence Function of Accepting a Donor Organ With Each Offer Stratified by Candidate Race and Gender.

The unadjusted cumulative incidence of offer acceptance is provided by candidate race and gender for each matching offer up to the 50th offer.
After adjusting for patient-, donor-, and offer-level variables, the odds of acceptance for a Black candidate were 24% less than for a White candidate for the first offer (odds ratio [OR], 0.76; 95% CI, 0.69-0.84) and remained significantly lower than those for a White candidate up to the 16th offer (Figure 2). The odds of acceptance for a female candidate were 53% higher than for a male candidate at the first offer (OR, 1.53; 95% CI, 1.39-1.68) and remained significantly higher for the first 6 offers. The odds were significantly lower for women than for men for the 10th to 31st offers; however, most female candidates (53%; 95% CI, 52%-55%) already had an offer accepted by the sixth offer. The tendency for the hazard probability to decline with offer number seen with empirical results (eFigure 2 in Supplement 1) was also observed after adjusting for patient-, donor-, and offer-level covariates (eFigure 5 in Supplement 1). eFigures 6 to 10 illustrate the estimated hazard probability with each of the remaining quantitative variables. Sensitivity analyses including PVR, cPRA level, and donation after cardiac death revealed no change in the overall findings with the exception of the OR of accepting an offer shifting modestly higher for female candidates compared with male candidates (eFigures 11-15 in Supplement 1).
Figure 2. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender.
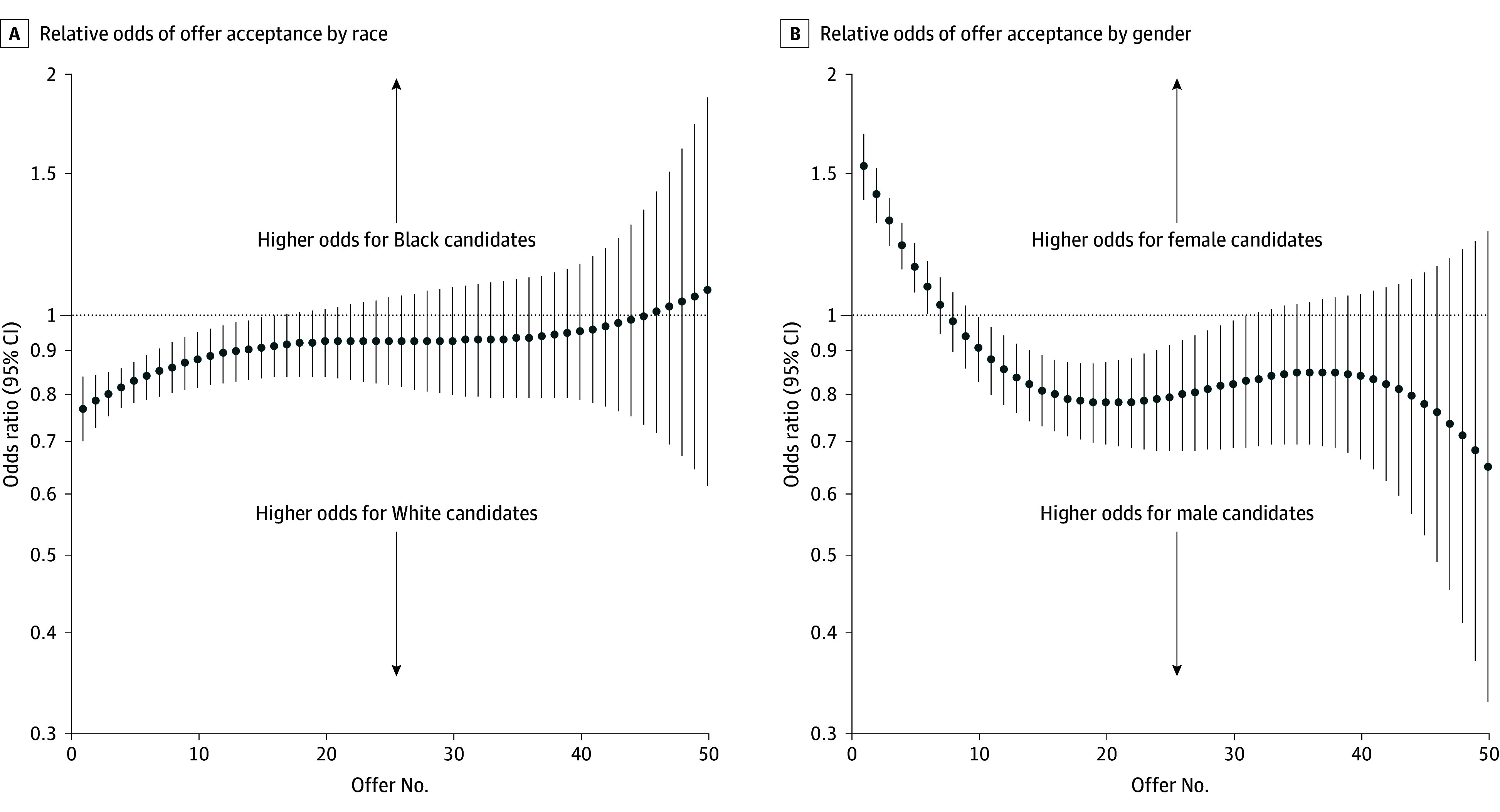
The adjusted odds ratios of offer acceptance are provided as the odds for Black candidates compared with the odds for White candidates and the odds for women compared with the odds for men for each matching offer up to the 50th offer, with 95% CIs per the model.
Discussion
Among Black and White patients listed for heart transplant in the US, the cumulative incidence of donor heart offer acceptance for female candidates was consistently higher than that for male candidates and the cumulative incidence for Black candidates was consistently lower than that for White candidates of the same gender for up to at least the 50th organ offer. Black candidates generally had to wait for more offers until an offer was accepted for transplant. The decisions to accept donor hearts were made by designated health care team members—generally a combination of cardiothoracic surgeons and/or heart transplant cardiologists—at each transplant center. These disparities existed after adjusting for the pertinent donor-, patient-, and offer-level characteristics that may impact the decision to accept a donor heart. This finding suggests racial and gender bias as a potential contributor to the organ acceptance decision-making process.
Multiple studies have previously demonstrated how barriers to heart transplant prevent equitable listing for heart transplant by race and gender,1,2,9,10,11,12,13,14 but the barriers to equitable heart transplant after listing are not clear. Annual US data reports for heart candidates have demonstrated a lower likelihood of transplant for Black patients listed for heart transplant compared with White patients and a higher likelihood of transplant for women listed for heart transplant than for men; these trends have persisted for years.4 In general, a transplant center cannot control the following key criteria for matching a candidate with a donor: severity of candidate illness, availability of a matching donor, and matching donor blood type. However, the decision pathway to accept a matched donor organ may be modifiable.
Our study differs from others by examining the odds of donor heart acceptance after a donor match. We accounted for pertinent factors that impact the decision to accept a donor organ. We adjusted for the likelihood of organ viability during transplant (donor age, donor ejection fraction, percentage difference in donor and candidate predicted heart mass, PVR, and cPRA level), ischemic time (distance between the donor’s hospital and the candidate’s listing center and whether the candidate had a VAD at listing, which would require a longer operative time to explant), perceived ability for the patient to continue safely waiting for better offers (candidate age, offer rank [greater likelihood of increased frequency of offers with low rank numbers, urgency, and clinical severity]), and a possible contraindication (donor history of cancer).24 We limited this study to the period of the last UNOS policy change, which altered waiting list status coding and the distance for which a candidate might match with a donor.25 After adjustment for all of these dynamic factors, racial and gender disparities persisted in the acceptance of donor organs.
Several factors are worth considering as potential contributors to our study findings. First, high levels of cPRA were unlikely to contribute to lower acceptance of an organ by gender or race despite other studies revealing higher levels in women (related to higher likelihood of prior pregnancies) and in Black patients (due to higher ratio of a prior VAD from blood transfusion, sensitization from biomaterials, or infection related to a VAD).26,27,28 Although high cPRA levels result in greater sensitization to donors, centers can screen for unacceptable antigens that would prevent an offer from ever taking place. A high level of concern may warrant a crossmatch test between the donor and the candidate that would be completed after tentative acceptance of a donor organ. Thus, cPRA level would impact availability of a donor match rather than acceptance. In addition, cPRA levels were similar across race and gender and did not change overall findings in the sensitivity analyses.
Second, center-level culture and practice may contribute to decisions to accept an offer more consistently. A prior study demonstrated center-level variability in acceptance of the first-rank offer for heart transplant centers that was not related to center volume.29 That study also found that sites accepting first-rank offers had better 1-year survival outcomes than did centers that declined first-rank offers. Although our study differed by considering each offer up to the 50th offer, it is worth investigating the qualities of centers that accept offers earlier for patients and identifying whether these centers are less likely to have disparate acceptance of offers by candidate race and gender in future work.
Last, unconscious bias and structural racism are known contributors in clinical decision-making30,31 and have been shown to influence heart transplant allocation processes.9,10,14 It is possible that bias and structural racism may also influence the decision to accept an organ. These issues could be generated from a false security that Black patients and/or men can wait longer for a better offer or from greater fear of a bad outcome with selecting an “imperfect” donor for a particular race and/or gender. Unconscious bias and structural racism may be studied and perhaps remedied by providing transplant center–level acceptance and waiting list survival data by race, ethnicity, and gender to centers and incentivizing (1) examination of center-level causes and (2) implementation of strategies resulting in equitable offer acceptance (ie, annual incentives for quality,32 evidence-based bias reduction and antiracism training33).
Limitations
This study has limitations. There were no adjustments for qualitative donor data. For example, presence or absence of coronary artery disease in the donor was not available categorically or not consistently assessed, or assessment was not recommended for donors 40 years or younger without risk factors.24 However, we adjusted for donor age in the models. In addition, centers can create donor filters (ie, donor-candidate heart mass, donor ejection fraction, and donor antigens) for each candidate, which may result in differing quality of offers. While the donor filters for each candidate were not available, we were able to adjust for the most pertinent variables that may contribute to accepting a donor offer.
Conclusions
In this cohort study, the cumulative incidence of donor heart offer acceptance by a transplant center team was consistently highest for White women followed by Black women, White men, and Black men. Further investigation is needed of the hospital-level decision-making process. Changes in the decision pathway to accept a donor organ are needed.
eMethods.
eTable 1. Representativeness of Study Participants
eTable 2. Estimates (95% CI) of Numbers of Offers Until Offer Is Accepted by Candidate Race and Gender
eFigure 1. Definition of Study Cohort
eFigure 2. Observed Hazard of Offer Acceptance by Offer Number
eFigure 3. Cumulative Incidence Function of Accepting a Donor Organ With Each Offer Stratified by Candidate Race and Gender with 95% Confidence Interval Bands
eFigure 4. Cumulative Incidence Function of Accepting a Donor Organ With Each Offer Stratified by Candidate Race and Gender Including All Offers
eFigure 5. Predicted Hazard of Offer Acceptance by Offer Number
eFigure 6. Predicted Hazard of Offer Acceptance by Distance from Donor to Candidate Center
eFigure 7. Predicted Hazard of Offer Acceptance by Percent Difference in Predicted Heart Mass
eFigure 8. Predicted Hazard of Offer Acceptance by Donor Ejection Fraction
eFigure 9. Predicted Hazard of Offer Acceptance by Candidate Age at Match
eFigure 10. Predicted Hazard of Offer Acceptance by Rank
eFigure 11. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender from Version 1 of PVR Sensitivity Analysis Compared to Computed From the Same Data but Without PVR at Listing
eFigure 12. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From Version 2 of PVR Sensitivity Analysis Compared to Computed From the Same Data but Without PVR at Listing
eFigure 13. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From cPRA Sensitivity Analysis Compared to Those Computed From the Same Data but a Model Without cPRA
eFigure 14. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From DCD Sensitivity Analysis With an Indicator Variable for DCD Donors Compared to Those Without the Indicator for DCD Donors
eFigure 15. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From DCD Sensitivity Analysis Omitting Observations With DCD Donors Compared to Those Computed From the Complete Data
eReferences.
Data Sharing Statement
Footnotes
References
- 1.Breathett K, Knapp SM, Carnes M, Calhoun E, Sweitzer NK. Imbalance in heart transplant to heart failure mortality ratio among African American, Hispanic, and White patients. Circulation. 2021;143(24):2412-2414. doi: 10.1161/CIRCULATIONAHA.120.052254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Breathett K, Knapp SM, Carnes M, Calhoun E, Sweitzer NK. Imbalance in heart transplant to heart failure mortality ratio by sex. J Am Heart Assoc. 2021;10(17):e020146. doi: 10.1161/JAHA.120.020146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chouairi F, Fuery M, Clark KA, et al. Evaluation of racial and ethnic disparities in cardiac transplantation. J Am Heart Assoc. 2021;10(17):e021067. doi: 10.1161/JAHA.120.021067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Colvin MM, Smith JM, Ahn YS, et al. OPTN/SRTR 2021 annual data report: heart. Am J Transplant. 2023;23(2)(suppl 1):S300-S378. doi: 10.1016/j.ajt.2023.02.008 [DOI] [PubMed] [Google Scholar]
- 5.Bahrami H, Kronmal R, Bluemke DA, et al. Differences in the incidence of congestive heart failure by ethnicity: the Multi-Ethnic Study of Atherosclerosis. Arch Intern Med. 2008;168(19):2138-2145. doi: 10.1001/archinte.168.19.2138 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063 [DOI] [PubMed] [Google Scholar]
- 7.Bozkurt B, Ahmad T, Alexander KM, et al. ; Writing Committee Members . Heart failure epidemiology and outcomes statistics: a report of the Heart Failure Society of America. J Card Fail. 2023;29(10):1412-1451. doi: 10.1016/j.cardfail.2023.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chang PP, Chambless LE, Shahar E, et al. Incidence and survival of hospitalized acute decompensated heart failure in four US communities (from the Atherosclerosis Risk in Communities Study). Am J Cardiol. 2014;113(3):504-510. doi: 10.1016/j.amjcard.2013.10.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Breathett K, Yee E, Pool N, et al. Does race influence decision making for advanced heart failure therapies? J Am Heart Assoc. 2019;8(22):e013592. doi: 10.1161/JAHA.119.013592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Breathett K, Yee E, Pool N, et al. Association of gender and race with allocation of advanced heart failure therapies. JAMA Netw Open. 2020;3(7):e2011044. doi: 10.1001/jamanetworkopen.2020.11044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Breathett K, Yee R, Pool N, et al. Group dynamics and allocation of advanced heart failure therapies—heart transplants and ventricular assist devices—by gender, racial, and ethnic group. J Am Heart Assoc. 2023;12(5):e027701. doi: 10.1161/JAHA.122.027701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nayak A, Hicks AJ, Morris AA. Understanding the complexity of heart failure risk and treatment in Black patients. Circ Heart Fail. 2020;13(8):e007264. doi: 10.1161/CIRCHEARTFAILURE.120.007264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lewsey SC, Breathett K. Equity in heart transplant allocation: intended progress up the hill or an impossibility? J Am Heart Assoc. 2021;10(17):e022817. doi: 10.1161/JAHA.121.022817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cascino TM, Colvin MM, Lanfear DE, et al. ; REVIVAL Investigators . Racial inequities in access to ventricular assist device and transplant persist after consideration for preferences for care: a report from the REVIVAL Study. Circ Heart Fail. 2023;16(1):e009745. doi: 10.1161/CIRCHEARTFAILURE.122.009745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Morris AA, Khazanie P, Drazner MH, et al. ; American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Hypertension . Guidance for timely and appropriate referral of patients with advanced heart failure: a scientific statement from the American Heart Association. Circulation. 2021;144(15):e238-e250. doi: 10.1161/CIR.0000000000001016 [DOI] [PubMed] [Google Scholar]
- 16.How we match organs. UNOS. Accessed December 21, 2023. https://unos.org/transplant/how-we-match-organs/
- 17.Glossary. Organ Procurement & Transplantation Network. Accessed December 23, 2023. https://optn.transplant.hrsa.gov/patients/glossary/#R
- 18.A fairer and more equitable cost effective and transparent system of donor organ procurement allocation and distribution. National Academies of Sciences, Engineering, and Medicine. Accessed September 9, 2023. https://www.nationalacademies.org/our-work/a-fairer-and-more-equitable-cost-effective-and-transparent-system-of-donor-organ-procurement-allocation-and-distribution
- 19.Continuous distribution. Organ Procurement & Transplantation Network. Accessed September 9, 2023. https://hrsa.unos.org/policies-bylaws/a-closer-look/continuous-distribution/
- 20.Data label change: “gender” to “birth sex.” UNOS. June 30, 2023. Accessed September 22, 2023. https://unos.org/unet-system-changes/data-label-change-gender-to-birth-sex/
- 21.Therneau TM. Survival: survival analysis. August 14, 2023. Accessed September 9, 2023. https://cran.r-project.org/web/packages/survival/index.html
- 22.Borgan Ø. Modeling survival data: extending the Cox model.. Stat Med. 2001;20(13):2053-2054. doi: 10.1002/sim.956 [DOI] [Google Scholar]
- 23.Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67:1-48. doi: 10.18637/jss.v067.i01 [DOI] [Google Scholar]
- 24.Copeland H, Knezevic I, Baran DA, et al. Donor heart selection: evidence-based guidelines for providers. J Heart Lung Transplant. 2023;42(1):7-29. doi: 10.1016/j.healun.2022.08.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Guidance and policy addressing adult heart allocation. Organ Procurement & Transplantation Network. Accessed February 16, 2024. https://optn.transplant.hrsa.gov/policies-bylaws/public-comment/guidance-and-policy-addressing-adult-heart-allocation
- 26.Colvin MM, Cook JL, Chang PP, et al. ; American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Surgery and Anesthesia . Sensitization in heart transplantation: emerging knowledge: a scientific statement from the American Heart Association. Circulation. 2019;139(12):e553-e578. doi: 10.1161/CIR.0000000000000598 [DOI] [PubMed] [Google Scholar]
- 27.Nunoda S. Impact of pretransplant antibodies on outcomes after heart transplantation. Curr Opin Organ Transplant. 2019;24(3):220-226. doi: 10.1097/MOT.0000000000000629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Morris AA, Cole RT, Veledar E, et al. Influence of race/ethnic differences in pre-transplantation panel reactive antibody on outcomes in heart transplant recipients. J Am Coll Cardiol. 2013;62(24):2308-2315. doi: 10.1016/j.jacc.2013.06.054 [DOI] [PubMed] [Google Scholar]
- 29.Choi AY, Mulvihill MS, Lee HJ, et al. Transplant center variability in organ offer acceptance and mortality among US patients on the heart transplant waitlist. JAMA Cardiol. 2020;5(6):660-668. doi: 10.1001/jamacardio.2020.0659 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Breathett K, Jones J, Lum HD, et al. Factors related to physician clinical decision-making for African-American and Hispanic patients: a qualitative meta-synthesis. J Racial Ethn Health Disparities. 2018;5(6):1215-1229. doi: 10.1007/s40615-018-0468-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care; Smedley BD, Stith AY, Nelson AR, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. National Academies Press; 2003.. [PubMed] [Google Scholar]
- 32.Emanuel EJ, Ubel PA, Kessler JB, et al. Using behavioral economics to design physician incentives that deliver high-value care. Ann Intern Med. 2016;164(2):114-119. doi: 10.7326/M15-1330 [DOI] [PubMed] [Google Scholar]
- 33.Breathett K, Yee RH, Pool N, et al. Pilot test of a multicomponent implementation strategy for equity in advanced heart failure allocation. Am J Transplant. 2023;23(6):805-814. doi: 10.1016/j.ajt.2023.03.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods.
eTable 1. Representativeness of Study Participants
eTable 2. Estimates (95% CI) of Numbers of Offers Until Offer Is Accepted by Candidate Race and Gender
eFigure 1. Definition of Study Cohort
eFigure 2. Observed Hazard of Offer Acceptance by Offer Number
eFigure 3. Cumulative Incidence Function of Accepting a Donor Organ With Each Offer Stratified by Candidate Race and Gender with 95% Confidence Interval Bands
eFigure 4. Cumulative Incidence Function of Accepting a Donor Organ With Each Offer Stratified by Candidate Race and Gender Including All Offers
eFigure 5. Predicted Hazard of Offer Acceptance by Offer Number
eFigure 6. Predicted Hazard of Offer Acceptance by Distance from Donor to Candidate Center
eFigure 7. Predicted Hazard of Offer Acceptance by Percent Difference in Predicted Heart Mass
eFigure 8. Predicted Hazard of Offer Acceptance by Donor Ejection Fraction
eFigure 9. Predicted Hazard of Offer Acceptance by Candidate Age at Match
eFigure 10. Predicted Hazard of Offer Acceptance by Rank
eFigure 11. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender from Version 1 of PVR Sensitivity Analysis Compared to Computed From the Same Data but Without PVR at Listing
eFigure 12. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From Version 2 of PVR Sensitivity Analysis Compared to Computed From the Same Data but Without PVR at Listing
eFigure 13. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From cPRA Sensitivity Analysis Compared to Those Computed From the Same Data but a Model Without cPRA
eFigure 14. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From DCD Sensitivity Analysis With an Indicator Variable for DCD Donors Compared to Those Without the Indicator for DCD Donors
eFigure 15. Adjusted Odds Ratio of Accepting a Donor Organ With Each Offer by Candidate Race and Gender From DCD Sensitivity Analysis Omitting Observations With DCD Donors Compared to Those Computed From the Complete Data
eReferences.
Data Sharing Statement