

Abstract
Aims
Economic burden of heart failure is attributed to hospital readmissions. Previous studies assessing risk factors for readmissions have focused on single group of risk factors, were limited to 30‐day readmissions, or did not account for competing risk of mortality. This study investigates the biological, socio‐economic, and behavioural risk factors predicting hospital readmissions while accounting for the competing risk of mortality.
Methods and results
In this prospective cohort study, we recruited 250 patients hospitalized with symptoms of advanced heart failure [New York Heart Association (NYHA) Class III and IV] between July 2017 and April 2019. We analysed their baseline survey data and their hospitalization records over the next 4.5 years (July 2017 to January 2022). We used a joint‐frailty model to determine the multifactorial risk factors for all‐cause and unplanned hospital readmissions and mortality. At the time of recruitment, patients' mean (SD) age was 66 (12) years, majority being male (72%) and NYHA class IV (68%) with reduced ejection fraction (72%). 87% of the patients had poor self‐care behaviours, 51% had diabetes and 56% had weak grip strength. Within 2 years of a hospital admission, 74% of the patients had at least one readmission. Among all readmissions during follow‐up, 68% were unplanned. Results from the multivariable regression analysis shows that the independent risk factors for hospital readmissions were biologic—weak grip strength [hazard ratio (95% CI): 1.59 (1.06, 2.13)], poor functional status [1.79 (0.98, 2.61)], diabetes [1.42 (0.97, 1.86)]; behavioural—poor self‐care [1.66 (0.84, 2.49)], and socio‐economic—preference for maximal life extension at high cost for those with high education [1.98 (1.17, 2.80)]. Risk factors for unplanned hospital readmissions were similar. A higher hospital readmission rate increased the risk of mortality [1.86 (1.23, 2.50)]. Other risk factors for mortality were biologic—weak grip strength [3.65 (0.57, 6.73)], diabetes [2.52 (0.62, 4.42)], socio‐economic—lower education [2.45 (0.37, 4.53)], and being married [2.53 (0.37, 4.69)]. Having a private health insurance [0.40 (0.08, 0.73)] lowered the risk for mortality.
Conclusions
Risk factors for hospital readmissions and mortality are multifactorial. Many of these factors, such as weak grip strength, diabetes, poor self‐care behaviours, are potentially modifiable and should be routinely assessed and managed in cardiac clinics and hospital admissions.
Keywords: Hospital readmissions, Heart failure, Functional status, Self‐care, Weak grip strength
Introduction
The prevalence of heart failure is increasing globally, 1 and has an economic cost of more than $100 billion per year. 2 More than 60% of this cost is attributable to direct health care expenditure including hospital readmissions. 2 Heart failure is also one of the most common causes of hospital readmissions among older adults. 1 Therefore, identification of patients at‐risk of hospital readmissions, especially those with preventable or reversible risk factors, is a priority for the health care systems in efforts to reduce health care costs.
Several studies over the last decade have assessed hospital readmissions among patients with heart failure. These studies have found that being older, 3 male, 3 unmarried, 4 having a health insurance, 5 cognitive impairment, 6 physical frailty, 7 diabetes, 7 , 8 poor self‐care behaviours, 9 and poor functional status 10 predict hospital readmissions. However, this literature has several gaps. First, most studies have focused on 30‐day hospital readmissions. 3 , 8 This was done as 30‐day hospital readmissions are believed to represent quality of hospital inpatient care and poor discharge planning. This approach, however, ignores the repeatability of hospital admissions beyond the arbitrary 30‐day period. Second, the current studies do not take into account the competing risk of mortality. Many patients may die during hospitalizations, thus making further readmissions impossible. Further, the same risk factors may affect both hospital readmissions and mortality. 7 Third, although the risk factors for hospital readmissions are likely to be multifactorial, existing studies have mostly focused on a single group of risk factors (e.g., biological or social). None has comprehensively assessed a range of biologic, social, economic and behavioural factors in predicting hospital readmissions. The role of patient preferences for life extension in predicting hospital readmissions has also been overlooked. This is despite studies suggesting that patients who prefer life extending treatments also receive more aggressive treatments. 11 The association between patient preferences for life extension and hospital readmissions may vary by patients' financial situation and healthcare affordability. Previous studies have showed that heart failure patients with lower socio‐economic status 12 and those with private health insurance 13 have low readmission rates. However, none has assessed whether patient preferences for life extension and hospital readmissions varies by healthcare affordability.
Recent trials have shown that self‐care interventions reduce patients' readmission and mortality risk. 14 , 15 However, a large proportion of patients with heart failure are physically frail. 16 As self‐care is a complex set of activities, physically frail patients may find it difficult to adhere to these activities and generally have poor self‐care behaviours. It is unclear whether improving self‐care behaviours among these patients can mitigate the effect of physical frailty on readmissions.
While several studies have assessed patterns of hospital readmissions globally, data from Asian populations is relatively scarce. 17 Studies show that Asian patients with symptomatic heart failure are younger, have more severe clinical features and higher rates of mechanical ventilation than those in the West. 18 Further, given the demographic transition in many Asian countries, 19 a high prevalence of diabetes 20 and other cardiovascular risk factors, 21 a better understanding of the multifactorial risk factors for hospital readmissions in Asian settings is warranted.
To address the above gaps in knowledge, we used survey data and medical records from a prospective cohort of patients with heart failure in Singapore, a South‐East Asian country with a rapidly aging population. 22 We first aimed to assess pattern of hospital readmissions over the study period, and characterize them based on their type (planned vs. unplanned). Second, we aimed to assess multifactorial risk factors for all‐cause hospital readmissions, while accounting for the competing risk of mortality. We hypothesized that biologic (muscle weakness, poor functional limitations, cognitive impairment, diabetes), socio‐economic (poor social well‐being, private health insurance, unmarried, lower education), behavioural (poor self‐care behaviours, preference for life‐extension) and demographic (older age, men) factors will be associated with greater risk of hospital readmissions and mortality. Third, we aimed to assess whether patient preferences for life extension as a risk factor for hospital readmissions varied by patients' education and private health insurance, indicators of their healthcare affordability. We hypothesized that readmissions will be higher among patients who prefer life extension and are more educated/have a private health insurance. Fourth, we aimed to assess whether better self‐care behaviours among physically frail patients, as measured by their grip strength and functional status, may reduce their risk of hospital readmission.
Methods
Participants and study setting
This study utilized baseline survey data from the Singapore Cohort of Patients with Advanced Heart Failure (SCOPAH) study, a prospective cohort of patients with heart failure recruited when they were hospitalized between July 2017 and April 2019. Their hospital readmissions through January 2022 were ascertained from their hospital medical records.
Patients were recruited from two public hospitals; those eligible included Singapore citizens or Permanent Residents aged ≥21 years hospitalized with heart failure and symptoms classified as New York Heart Association (NYHA) class III or IV. Patients with major psychiatric disorders, as stated in their electronic medical records, were excluded from participation. Patients were screened for cognitive impairment with the Montreal Cognitive Assessment 23 ; those with scores less than 10 indicating severe cognitive impairment were excluded. Written informed consent was obtained from all eligible patients who agreed to participate in the study. The study protocol has been published. 24 The study was approved by the SingHealth Centralised Institutional Review Board (2016/3046).
Study measures
Outcomes
All‐cause hospital readmissions: Patients' hospital admission and discharge dates, length of stay, and type (unplanned vs. planned, based on linkage with admissions data from emergency department) of each hospital readmission were ascertained using medical records from study enrolment through January 2022 or until death.
Date of death: Data were extracted from patients' medical records.
Independent variables
The variables include potential risk factors measured at baseline.
Biologic factors
Weak hand grip strength: Hand grip strength was assessed using Smedley spring‐type dynamometer. After demonstration, study personnel asked patients to remove rings or other hand jewellery and sit straight upright with their elbow extended at their side, not touching the bed or chair. Patients were instructed to squeeze the dynamometer as hard as possible and then let go. The process was conducted twice for each hand. Measurements were recorded to the nearest 0.5 kg. Hand dominance was also recorded for each patient. We calculated the grip strength as the average of two measurements for patient's dominant hand. If only one measurement was recorded for the dominant hand, that value was used. If measurements were only recorded for one hand, those values were averaged and used. If patients reported both hands were equally dominant, the average of the two measurements for the hand with greater grip strength was used. Participants were classified as having weak grip strength if their dominant hand grip strength value fell at or below the 20th percentile of Singapore normative grip strength values for sex and age. 25 If valid hand grip strength value was not available at baseline, we used the next earliest available grip strength value within 1 year of follow‐up.
Poor functional status: We assessed activities of daily living (ADLs) in patients using the Physical ADL section of the Older American Resources and Services. 26 This is a 7‐item scale, assessing patient's ability to eat, dress/undress, take care of own appearance, walk, get in/out of bed, take a bath and use the bathroom. Patients showing limitation (responded as ‘completely unable to do’ or ‘do with some help’) in any of these 7 items were categorized as having poor functional status.
Cognitive impairment: Cognitive impairment was assessed using Montreal Cognitive Assessment 23 , 24 (score range: 10–30) and categorized as none (score ≥26), mild (score ≥18 & ≤25) and moderate (score ≥10 & ≤17). Those with severe cognitive impairment (<10) did not take part in the survey.
Diabetes: Patients self‐reported whether they had a history of diabetes (yes or no).
Socio‐economic factors
Poor social well‐being: Patients' social well‐being was measured through the Functional Assessment of Cancer Therapy‐General (FACT‐G). 27 Social well‐being subscale comprised of 7 items ranging from 0 to 4 (not at all, a little bit, somewhat, quite a bit and very much). Total score ranged from 0 to 28 with a higher score representing higher social well‐being. Poor social well‐being was defined as below 25th percentile of social well‐being score.
Private health insurance: Patients were asked if they had any private health insurance to help cover the cost of their medical care. In Singapore, while all residents have access to a basic public health insurance (MediShield Life), 28 some may choose to top‐up their coverage by purchasing an additional private health care insurance.
Education and marital status: Data were assessed in the survey and categorized as primary or below versus secondary and above (for education) and married versus not married (for marital status).
Behavioural factors
Poor self‐care behaviour: Self‐care behaviour was assessed through Self‐Care of Heart Failure Index (SCHFI) V6.2., 29 which comprised 15 items across 3 subscales – self‐care maintenance, self‐care management and self‐care confidence. Items were rated on a 4‐point response scale and higher score indicated better self‐care. The total score for each subscale was transformed into 0 to 100; overall score ranged from 0 to 300 and <210 was considered poor self‐care behaviour. 17
Preference for life‐extension: We asked patients to trade‐off life extension with health care cost‐ “If you had to make a choice now, would you prefer treatment that extends life as much as possible, or would you want treatment that costs you less?” Patients responded on scale of 1 to 9, with 1 representing extend life as much as possible at high cost and 9 representing no life extension at less cost. Responses were classified as maximal life extension (score 1 to 4) and moderate or minimal life extension (score 5 to 9).
Demographic factors
Age and gender were assessed in the survey. We also reported the ejection fraction classified as depressed (<50%) or preserved (≥50%) 30 based on left ventricular function performed at the time of hospital admission.
Statistical analysis
We described baseline patient characteristics and number and characteristics of hospitalizations during the follow‐up period. Among the sub‐group of patients who died, we described time to death from enrolment. We then used joint‐frailty model to investigate potential baseline risk factors for all‐cause hospital readmissions and mortality. We also tested, using separate models, whether patients' education and private health insurance (indicator for their socio‐economic status) modified the association between their preference for life extension and hospital readmissions. Further, we tested whether self‐care behaviours modified the association of weak grip strength and poor functional status (indicator of frailty) with hospital readmissions. Lastly, we also investigated the potential baseline risk factors for unplanned hospital readmissions. A joint‐frailty model is a time‐to‐event model to jointly model both recurrent (hospital readmissions) and terminal events (mortality), both models linked through a shared random effect (patient identification number). 31 Jointly modelling the two events was relevant as hospital readmissions increase the risk of mortality and hospital readmissions cannot occur after death. Thus, an appropriate analysis of hospital readmissions required censoring due to death. In contrast, other commonly used methods, such as Cox models only consider the time to first hospital readmission, count models such as Poisson or negative binomial do not take into account the timing of the readmissions, and the recurrent event models such as Anderson‐Gill regression do not take into account the competing risk of mortality. We used Stata's merlin package 32 to implement the joint frailty model. We used Stata M/P 16.1 for all analyses.
Results
We analysed data from 250 patients (excluding one extreme outlier); of these 41 (16%) died within 1 year of enrolment and 94 (38%) died during a total of 4.5‐year follow‐up (Figure S1 ). The average follow‐up period per patient was 1 year and 10 months.
Patient baseline characteristics
Patients' mean age was 66 ± 12 years; majority being male (72%), married (69%), NYHA class IV (68%), with reduced ejection fraction (72%), with mild or moderate cognitive impairment (74%), and having poor self‐care behaviours (87%). Over half had primary or below education (52%), diabetes (51%) and weak grip strength (56%). 12% experienced poor functional status and 24% had poor social well‐being. More than one‐third had a private health insurance (37%) and 32% preferred maximal life extension at high cost (Table 1 ). Among patients with low education, 28% preferred life extension at high cost and among those with high education 37% preferred life extension at high cost.
Table 1.
Baseline patient characteristics, n = 250
| Age, mean (SD) (range: 29–91) | 66.0 (12.0) |
| Gender, n (%) | |
| Male | 179 (71.6) |
| Female | 71 (28.4) |
| New York Heart Association (NYHA) Functional Classification | |
| Class III | 80 (32.0) |
| Class IV | 170 (68.0) |
| Ejection fraction <50%, n (%) (n = 200) | 145 (72.5) |
| Biologic risk factors | |
| Weak grip strength, n (%) (n = 230) | 128 (55.9) |
| Limitations in activities of daily living, yes, n (%), n = 242 | 30 (12.4) |
| Cognitive impairment, n (%) range (0–30) | |
| Normal (≥26) | 66 (26.4) |
| Mild 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 | 138 (55.2) |
| Moderate (≤17–>10) | 46 (18.4) |
| Diabetes, n (%) | 128 (51.2) |
| Socio‐economic risk factors | |
| Poor social well‐being, n (%) | 59 (23.6%) |
| Private health insurance, n (%), n = 242 | 90 (37.2) |
| Education, n (%) | |
| Primary or below | 130 (52.0) |
| Above primary | 120 (48.0) |
| Married, n (%) | 173 (69.2) |
| Behavioural risk factors | |
| Poor self‐care behaviour, n (%), n = 244 | 213 (87.3) |
| Preference for life extension, n (%), n = 230 | |
| Minimal or moderate life extension | 156 (67.8) |
| Maximal life extension | 74 (32.2) |
Hospital readmission characteristics and mortality
Within 1 month, 6 months, 1 year and 2 years of the index hospital admission, 22%, 53%, 66% and 74% of the patients had at least one hospital readmission (Figure 1 ). Median number of hospital readmissions per patient during the follow‐up period was 3 (IQR: 1, 5). Among all readmissions in the follow‐up period, 68% were unplanned. Median (IQR) length of stay for all hospital readmissions was 4 days (2, 7) [planned – 2 days (0, 5), unplanned – 4 days]. 2 , 8
Figure 1.
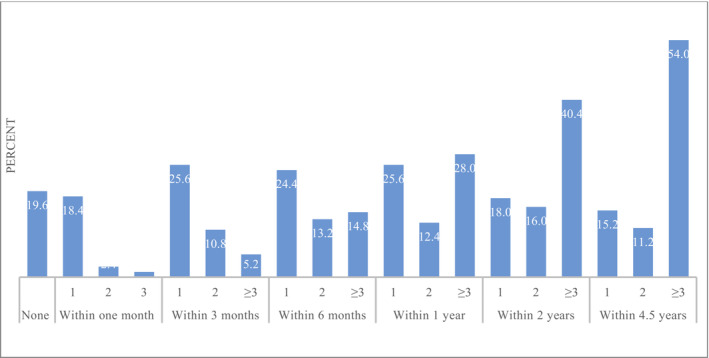
No. of hospital readmissions per person, n = 250.
Mortality rate in 1 month, 3 months, 6 months, 1 year and 2 years of the index hospital admission were 2%, 6%, 9%, 16% and 23%, respectively.
Risk factors for hospital readmissions and mortality
In the multivariable analysis, patients with weak grip strength were 59% more likely [hazard ratio (95% CI): 1.59 (1.06, 2.13)] and those with poor functional health were 79% more likely [1.79 (0.98, 2.61)] to have a hospital readmission (Table 1 ). Patients with poor self‐care behaviour had a 66% greater risk [1.66 (0.84, 2.49)], and those with diabetes had 42% greater risk [1.42 (0.97, 1.86)] of a hospital readmission. Among patients with high education, those who preferred maximal life extension had a 98% greater risk [1.98 (1.17, 2.80)] of a hospital readmission compared with those with preference for minimal or moderate life extension. Among patients with preference for minimal or moderate life extension, those with low education had a 92% greater risk [1.92 (1.15, 2.68)] of a hospital readmission compared with those with those with a high education (Table 2 ). Similar results were noted for unplanned readmissions (Table 3 ).
Table 2.
Risk factors for hospital readmissions and mortality among patients with advanced heart failure, n = 211
| Hazard ratio (95% CI) | ||
|---|---|---|
| Hospital readmissions | Mortality | |
| Biologic factors | ||
| Weak hand grip strength | 1.59 (1.06, 2.13)*** | 3.65 (0.57, 6.73)*** |
| Poor functional status | 1.79 (0.98, 2.61)** | 2.13 (−0.06, 4.3) |
| Cognitive impairment (ref: none) | ||
| Mild | 0.83 (0.51, 1.15) | 0.78 (0.09, 1.46) |
| Moderate | 1.17 (0.55, 1.80) | 0.50 (−0.12, 1.12) |
| Diabetes | 1.42 (0.97, 1.86)** | 2.52 (0.62, 4.29)** |
| Behavioural factors | ||
| Poor self‐care behaviour | 1.66 (0.84, 2.49)** | 0.89 (−0.04, 1.63) |
| Preference for maximal life extension at high cost | ‐ | 1.60 (0.39, 2.82) |
| Socio‐economic factors | ||
| Poor social support | 0.94 (0.60, 1.28) | 1.05 (0.22, 1.88) |
| Private health insurance | 0.84 (0.57, 1.11) | 0.43 (0.10, 0.76)** |
| Married (vs. not married) | 1.19 (0.78, 1.60) | 2.53 (0.37, 4.69)** |
| Low education (vs. high) | ‐ | 2.45 (0.37, 4.53)** |
| Preference for maximal life extension at high cost among those with low (primary or below) education (vs. high) | 1.02 (0.58, 1.45) | ‐ |
| Preference for maximal life extension at high cost among those with high education (vs. preference for minimum or moderate life extension) | 1.98 (1.17, 2.80)*** | ‐ |
| Preference for minimal or moderate life extension among those with low education (vs. high education) | 1.92 (1.15, 2.68)*** | ‐ |
| Demographics | ||
| Age | 1.00 (0.99, 1.02) | 1.05 (1.01, 1.09)** |
| Female (vs. males) | 1.05 (0.68, 1.42) | 0.99 (0.17, 1.81) |
P‐value < 0.05.
P‐value < 0.01.
Table 3.
Risk factors for unplanned hospital readmissions
| Hazard ratio (95% CI) | ||
|---|---|---|
| Unplanned hospital readmissions | Mortality | |
| Biologic factors | ||
| Weak hand grip strength | 1.64 (0.97, 2.31)** | 3.47 (0.68, 6.24)*** |
| Poor functional status | 2.10 (0.95, 3.26)*** | 2.36 (0.01, 4.70) |
| Cognitive impairment (ref: none) | ||
| Mild | 0.93 (0.49, 1.37) | 0.88 (0.13, 1.63) |
| Moderate | 1.34 (0.47, 2.22) | 0.50 (−0.10, 1.11) |
| Diabetes | 2.01 (1.23, 2.79)*** | 2.65 (0.70, 4.60)*** |
| Behavioural factors | ||
| Poor self‐care behaviour | 1.45 (0.58, 2.33) | 0.78 (−0.01, 1.57) |
| Preference for maximal life extension at high cost (vs. preference for minimal or moderate life extension) | ‐ | 1.60 (0.43, 2.77) |
| Socio‐economic factors | ||
| Poor social well‐being | 1.02 (0.58, 1.47) | 0.98 (0.21, 1.75) |
| Private health insurance | 0.81 (0.48, 1.13) | 0.40 (0.09, 0.71)** |
| Married (vs. not married) | 1.09 (0.63, 1.55) | 2.53 (0.46, 4.59)** |
| Low education (vs. high) | ‐ | 2.76 (0.47, 5.05)** |
| Preference for maximal life extension at high cost among those with low (primary or below) education (vs. high education) | 1.16 (0.57, 1.75) | ‐ |
| Preference for maximal life extension at high cost among those with high education (vs. preference for minimum or moderate life extension) | 2.01 (0.96, 3.05)*** | ‐ |
| Preference for minimal or moderate life extension among those with low education (vs. high education) | 2.53 (1.27, 3.80)*** | ‐ |
| Demographics | ||
| Age | 1.00 (0.98, 1.02) | 1.04 (1.00, 1.08)** |
| Female (vs. males) | 0.98 (0.56, 1.41) | 0.94 (0.19, 1.69) |
P‐value < 0.05.
P‐value < 0.01.
Risk factors for mortality were weak grip strength [3.65 (0.57, 6.73)], diabetes [2.52 (0.62, 4.42)], age [1.05 (1.01, 1.09)], lower education [primary or below (vs. above primary)] [2.45 (0.37, 4.53)] and being married [2.53 (0.37, 4.69)]. Having private health insurance [0.40 (0.08, 0.73)] was associated with a lower risk for mortality (Table 2 ). The coefficient for random effect showed a positive association between hospital readmissions and mortality, that is, a higher rate of hospital readmissions was associated with increased mortality [1.86 (1.23, 2.50)].
Contrary to our hypothesis, we did not find that private health insurance modified the association between patient's preference for life extension and all hospital and unplanned readmissions. Similarly, self‐care behaviour did not modify the association of weak‐grip strength and poor functional status with all hospital and unplanned readmissions (Tables S1 and S2 ).
Discussion
In this prospective cohort of patients with heart failure, 74% had at least one hospital readmission within 2 years of the index hospital admission. All‐cause hospital readmissions were mainly unplanned. The 30‐day hospital readmission rate and mortality rates were similar to those previously reported from the United States. 33 We identified multi‐factorial risk factors for hospital readmissions including weak grip strength (muscle weakness), poor functional status, diabetes, poor self‐care, preference for life‐extension among those with high education.
Our results showed weak grip strength to be a risk factor for all‐cause and unplanned hospital readmissions and mortality. Prior studies have reported an increased risk of mortality among heart failure patients with lower grip strength. 7 Weak grip strength is an indicator of weak physiological reserve, 34 and a single‐item marker of frailty that is included in most frailty scoring systems. 35 Studies show that cardiac frailty is reversible through interventions such as a left ventricular assist device and cardiac rehabilitation. 36 These studies, taken together with our results, indicate that timely identification of cardiac frailty through grip strength and its subsequent management provides an avenue for reducing patients' risk of hospital readmissions. Grip strength measurements are easy‐to‐do and can be conducted for patients with limited functional status, and would thus be easy to implement in busy cardiac clinics.
Our results showed that patients with poor functional status were at a greater risk for all‐cause and unplanned hospital readmissions. Previous studies also show functional impairment to be associated with 30‐day and 90‐day hospital readmissions. 10 As patients are at the greatest risk of functional decline during and after hospitalizations, rehabilitation interventions during this time to maintain function and to prevent further functional decline may also prevent hospital readmissions. 10
Our results are consistent with previous studies that indicate that heart failure patients with diabetes are at an increased risk of hospital readmissions and mortality. 37 Results are notable given the high prevalence of diabetes in Singapore and other Asian populations, 20 , 37 and that heart failure and diabetes frequently co‐exist 38 as demonstrated in our sample in which about half of the patients had diabetes. Hyperglycaemia and insulin resistance are linked to inefficient myocardial fuel metabolism, diabetic cardiomyopathy, impaired immune function and risk of infections 39 ; and an improvement in glycaemic control has been shown to be associated with improved cardiac function. 40
Singapore is a high‐income Asian economy. Approximately 30% of health expenditure in the country is out‐of‐pocket, greater than the average for high‐income countries. 41 A mandatory low‐cost public health insurance with high deductibles partially meets patients' healthcare cost. Individuals who wish to obtain additional healthcare coverage for private hospitals or want to be cared for in private wards in public hospitals can opt for an additional private health insurance. 42 In our sample, about 62% of patients had some form of private health insurance. Findings shows that lack of private health insurance was associated with increased risk of mortality, indicating a marker of poor socio‐economic status, 43 which is generally associated with poorer outcomes in heart failure patients. 44
Literature regarding the association between hospital readmissions and patient preference for life extension is sparse. Few have shown that patients with do‐not‐resuscitate orders are less likely to be readmitted to hospital within 30 days. 45 Findings showed that among patients with a high education, those preferring maximal life extension had a higher risk of hospital readmission than those preferring minimal life extension. It suggests that among patients with a higher socio‐economic status, hospital readmissions may be triggered by a desire to extend life and seek aggressive treatments and interventions. However, among patients with a preference for minimal or moderate life extension, those with low education had a higher risk of hospital readmission compared with those with a high education. Past studies have also shown that socio‐economic deprivation among patients with heart failure is associated with increased risk of all‐cause hospitalization likely due to excessive cardiovascular 46 and non‐cardiovascular events. 47 Thus, the higher propensity for these events, rather than a preference for life extension, may be driving all‐cause hospitalizations among patients with low education levels. We found poor self‐care to be one of the most important risk factors for hospital readmissions. Self‐care is a vital component of heart failure management. Heart failure patients are typically asked to adhere to a regimen of medications, low‐sodium diet, regular exercise, monitoring of signs, symptoms and weight, fluid intake restriction and smoking cessation. 48 Engaging in these self‐care behaviours can lower the risk of heart failure exacerbations and thereby hospital readmissions. 9 Thus, improving self‐care through education and continual monitoring of their behaviours may reduce patients' risk of hospital readmissions.
The study has several strengths. Its findings provide valuable information about the multifactorial risk factors for hospital readmissions, while accounting for the competing risk of mortality. Such comprehensive analyses of risk factors including, biologic, socio‐economic and behavioural, is not available in previous heart failure studies. Availability of detailed medical records along with information on baseline risk factors from a comprehensive survey facilitated the analyses. The study also has limitations. First, our sample size is smaller compared with many studies relying solely on administrative or medical records to assess readmissions. Second, although patients were recruited from two major hospitals in Singapore, the generalizability of our results to other countries/settings needs to be confirmed.
Conclusion
Findings indicate that risk factors for hospital readmissions are not just biologic, but also socio‐economic and behavioural. Further, most of these factors are potentially reversible or modifiable, and should be routinely assessed and managed in cardiac clinics and hospital admissions.
Funding
The study is funded by Health Services Research Competitive Research Grant, Ministry of Health, Singapore (NMRC/HSRG/0053/2016).
Conflict of interest
The authors do not have any conflicts of interest to declare.
Supporting information
Table S1. Risk factors for hospital readmissions among patients with advanced heart failure, n = 211.
Table S2. Risk factors for unplanned hospital readmissions.
Figure S1. Mortality since enrolment, n = 250.
Malhotra, C. , Chaudhry, I. , Keong, Y. K. , and Sim, K. L. D. (2024) Multifactorial risk factors for hospital readmissions among patients with symptoms of advanced heart failure. ESC Heart Failure, 11: 1144–1152. 10.1002/ehf2.14670.
References
- 1. Dokainish H, Teo K, Zhu J, Roy A, AlHabib KF, ElSayed A, et al. Global mortality variations in patients with heart failure: results from the International Congestive Heart Failure (INTER‐CHF) prospective cohort study. Lancet Glob Health 2017;5:e665‐e672. doi: 10.1016/S2214-109X(17)30196-1 [DOI] [PubMed] [Google Scholar]
- 2. Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart failure. Int J Cardiol 2014;171:368‐376. doi: 10.1016/j.ijcard.2013.12.028 [DOI] [PubMed] [Google Scholar]
- 3. Lim YMF, Ong SM, Koudstaal S, Hwong WY, Liew HB, Rajadurai J, et al. Trends for readmission and mortality after heart failure hospitalisation in Malaysia, 2007 to 2016. Global. Heart 2022;17:20. doi: 10.5334/gh.1108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Damiani G, Salvatori E, Silvestrini G, Ivanova I, Bojovic L, Iodice L, et al. Influence of socioeconomic factors on hospital readmissions for heart failure and acute myocardial infarction in patients 65 years and older: Evidence from a systematic review. Clin Interv Aging 2015;10:237. doi: 10.2147/CIA.S71165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Takahashi K, Saito M, Inaba S, Morofuji T, Aisu H, Sumimoto T, et al. Contribution of the long‐term care insurance certificate for predicting 1‐year all‐cause readmission compared with validated risk scores in elderly patients with heart failure. Open heart 2016;3:e000501. doi: 10.1136/openhrt-2016-000501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Holm H, Bachus E, Jujic A, Nilsson ED, Wadström B, Molvin J, et al. Cognitive test results are associated with mortality and rehospitalization in heart failure: Swedish prospective cohort study. ESC Heart Fail 2020;7:2948‐2955. doi: 10.1002/ehf2.12909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Chaudhry SI, McAvay G, Chen S, Whitson H, Newman AB, Krumholz HM, et al. Risk factors for hospital admission among older persons with newly diagnosed heart failure: Findings from the cardiovascular health study. J Am Coll Cardiol 2013;61:635‐642. doi: 10.1016/j.jacc.2012.11.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Madanat L, Saleh M, Maraskine M, Halalau A, Bukovec F. Congestive heart failure 30‐day readmission: Descriptive study of demographics, co‐morbidities, heart failure knowledge, and self‐care. Cureus 2021;13: doi: 10.7759/cureus.18661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Sahebi A, Mohammad‐Aliha J, Ansari‐Ramandi M, Naderi N. Investigation the relationship between self‐care and readmission in patients with chronic heart failure. Res Cardiovasc Med 2015;4:5. doi: 10.5812/cardiovascmed.25472 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Van Nguyen T, Dang HT, Burns MJ, Dao HH, Nguyen TN. Impairment in activities of daily living and readmission in older patients with heart failure: A cohort study. BMJ Open 2021;11:e044416. doi: 10.1136/bmjopen-2020-044416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Malhotra C, Bundoc F, Chaudhry I, Teo I, Ozdemir S, Finkelstein E, et al. A prospective cohort study assessing aggressive interventions at the end‐of‐life among patients with solid metastatic cancer. BMC Palliat Care 2022;21:73. doi: 10.1186/s12904-022-00970-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Philbin EF, Dec GW, Jenkins PL, DiSalvo TG. Socioeconomic status as an independent risk factor for hospital readmission for heart failure. Am J Cardiol 2001;87:1367‐1371. doi: 10.1016/S0002-9149(01)01554-5 [DOI] [PubMed] [Google Scholar]
- 13. Ferro EG, Secemsky EA, Wadhera RK, Choi E, Strom JB, Wasfy JH, et al. Patient readmission rates for all insurance types after implementation of the hospital readmissions reduction program. Health Aff 2019;38:585‐593. doi: 10.1377/hlthaff.2018.05412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ades PA, Keteyian SJ, Balady GJ, Houston‐Miller N, Kitzman DW, Mancini DM, et al. Cardiac rehabilitation exercise and self‐care for chronic heart failure. JACC: Heart Fail 2013;1:540‐547. doi: 10.1016/j.jchf.2013.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Heran BS, Chen JM, Ebrahim S, et al. Exercise‐based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2011;7:CD001800. doi: 10.1002/14651858.CD001800.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dai K, Laber E, Chen H, Mentz R, Malhotra C. Hand grip strength predicts mortality and quality of life in heart failure: Insights from the Singapore cohort of patients with advanced heart failure. J Card Fail 2022;29:911‐918. doi: 10.1016/j.cardfail.2022.11.009 [DOI] [PubMed] [Google Scholar]
- 17. Ma C. Rehospitalisation rates and associated factors within 6 months after hospital discharge for patients with chronic heart failure: A longitudinal observational study. J Clin Nurs 2019;28:2526‐2536. doi: 10.1111/jocn.14830 [DOI] [PubMed] [Google Scholar]
- 18. Lam CS. Heart failure in Southeast Asia: Facts and numbers. In: Heart failure in Southeast Asia: Facts and numbers. Wiley Online Library; 2015:46‐49. doi: 10.1002/ehf2.12036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Zaidi B, Morgan SP. The second demographic transition theory: A review and appraisal. Annu Rev Sociol 2017;43:473‐492. doi: 10.1146/annurev-soc-060116-053442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Rhee E‐J. Diabetes in Asians. Endocrinol Metab 2015;30:263‐269. doi: 10.3803/EnM.2015.30.3.263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Nguyen HN, Fujiyoshi A, Abbott RD, Miura K. Epidemiology of cardiovascular risk factors in Asian countries. Circ J 2013;77:2851‐2859. doi: 10.1253/circj.CJ-13-1292 [DOI] [PubMed] [Google Scholar]
- 22. Chung CF, Mansur K. A literature review on ageing population in selected Asian countries. Malay J Bus Econ (MJBE) 2018; doi: 10.1253/circj.CJ-13-1292 [DOI] [Google Scholar]
- 23. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695‐699. doi: 10.1111/j.1532-5415.2005.53221.x [DOI] [PubMed] [Google Scholar]
- 24. Malhotra C, Foo R, Singh R, Ozdemir S, Teo I, Sim D, et al. Study protocol for a cohort study of patients with advanced heart failure in Singapore. BMJ Open 2018;8:e022248. doi: 10.1136/bmjopen-2018-022248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Malhotra R, Ang S, Allen JC, Tan NC, Østbye T, Saito Y, et al. Normative values of hand grip strength for elderly Singaporeans aged 60 to 89 years: A cross‐sectional study. J Am Med Dir Assoc 2016;17:864.e1‐864.e7. doi: 10.1016/j.jamda.2016.06.013 [DOI] [PubMed] [Google Scholar]
- 26. Fillenbaum GG. Multidimensional functional assessment of older adults: The Duke Older Americans Resources and Services procedures. Psychology Press; 2013. doi: 10.4324/9780203771563 [DOI] [Google Scholar]
- 27. Webster K, Cella D, Yost K. The F unctional a ssessment of C hronic I llness T herapy (FACIT) measurement system: Properties, applications, and interpretation. Health Qual Life Outcomes 2003;1:1‐7. doi: 10.1186/1477-7525-1-79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Earn LC. The Singaporean health care system. Int Prof Health Care Syst 2020;169: doi: 10.1186/1477-7525-1-79 [DOI] [Google Scholar]
- 29. Riegel B, Carlson B, Moser DK, Sebern M, Hicks FD, Roland V. Psychometric testing of the self‐care of heart failure index. J Card Fail 2004;10:350‐360. doi: 10.1016/j.cardfail.2003.12.001 [DOI] [PubMed] [Google Scholar]
- 30. Pfeffer MA, Shah AM, Borlaug BA. Heart failure with preserved ejection fraction in perspective. Circ Res 2019;124:1598‐1617. doi: 10.1161/CIRCRESAHA.119.313572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Rondeau V, Mathoulin‐Pelissier S, Jacqmin‐Gadda H, Brouste V, Soubeyran P. Joint frailty models for recurring events and death using maximum penalized likelihood estimation: Application on cancer events. Biostatistics 2007;8:708‐721. doi: 10.1093/biostatistics/kxl043 [DOI] [PubMed] [Google Scholar]
- 32. Crowther MJ. Merlin—A unified modeling framework for data analysis and methods development in Stata. Stat J 2020;20:763‐784. doi: 10.1177/1536867X20976311 [DOI] [Google Scholar]
- 33. Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol 2013;61:391‐403. doi: 10.1016/j.jacc.2012.09.038 [DOI] [PubMed] [Google Scholar]
- 34. Saraiva WS, Prestes J, Funghetto SS, et al. Relation between relative handgrip strength, chronological age and physiological age with lower functional capacity in older women. Open Access J Sports Med 2019;10:185‐190. doi: 10.2147/OAJSM.S227720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146‐M156. doi: 10.1093/gerona/56.3.m146 [DOI] [PubMed] [Google Scholar]
- 36. Aili SR, Lo P, Villanueva JE, Joshi Y, Emmanuel S, Macdonald PS. Prevention and reversal of frailty in heart failure―A systematic review. Circ J 2021;86:14–22. doi: 10.1253/circj.CJ-21-0819 [DOI] [PubMed] [Google Scholar]
- 37. Tay WT, Teng THK, Simon O, Ouwerkerk W, Tromp J, Doughty RN, et al. Readmissions, death and its associated predictors in heart failure with preserved versus reduced ejection fraction. J Am Heart Assoc 2021;10:e021414. doi: 10.1161/JAHA.121.021414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Tousoulis D, Oikonomou E, Siasos G, Stefanadis C. Diabetes mellitus and heart failure. Eur Cardiol Rev 2014;9:37‐42. doi: 10.15420/ecr.2014.9.1.37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Dungan KM. The effect of diabetes on hospital readmissions. J Diabetes Sci Technol 2012;6:1045‐1052. doi: 10.1177/193229681200600508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Leung M, Wong VW, Hudson M, Leung DY. Impact of improved glycemic control on cardiac function in type 2 diabetes mellitus. Circulation. Cardiovasc Imag 2016;9:e003643. doi: 10.1161/CIRCIMAGING.115.003643 [DOI] [PubMed] [Google Scholar]
- 41. The World Bank . World Health Organization Global Health Expenditure database: The World Bank; 2018. https://data.worldbank.org/indicator/SH.XPD.OOPC.CH.ZS?locations=SG. Accessed 4 June 2023.
- 42. Central Provident Fund Board . https://www.cpf.gov.sg/member/healthcare‐financing/medishield‐life. Accessed 4 June 2023.
- 43. Braveman PA, Cubbin C, Egerter S, Williams DR, Pamuk E. Socioeconomic disparities in health in the United States: What the patterns tell us. Am J Public Health 2010;100:S186‐S196. doi: 10.2105/AJPH.2009.166082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Havranek EP, Mujahid MS, Barr DA, Blair IV, Cohen MS, Cruz‐Flores S, et al. Social determinants of risk and outcomes for cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2015;132:873‐898. doi: 10.1161/CIR.0000000000000228 [DOI] [PubMed] [Google Scholar]
- 45. Callahan K, Kitko L, Van Scoy LJ, Hollenbeak CS. Do‐not‐resuscitate orders and readmission among elderly patients with heart failure in Pennsylvania: An observational study, 2011‐2014. Heart Lung 2020;49:812‐816. doi: 10.1016/j.hrtlng.2020.09.012 [DOI] [PubMed] [Google Scholar]
- 46. Noori A, Shokoohi M, Baneshi MR, Naderi N, Bakhshandeh H, Haghdoost AA. Impact of socio‐economic status on the hospital readmission of congestive heart failure patients: A prospective cohort study. Int J Health Policy Manag 2014;3:251‐257. doi: 10.15171/ijhpm.2014.94 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Witte KK, Patel PA, Walker AM, et al. Socioeconomic deprivation and mode‐specific outcomes in patients with chronic heart failure. Heart 2018;104:993‐998. doi: 10.1136/heartjnl-2017-312539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Lainscak M, Blue L, Clark AL, Dahlström U, Dickstein K, Ekman I, et al. Self‐care management of heart failure: practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2011;13:115‐126. doi: 10.1093/eurjhf/hfq219 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Risk factors for hospital readmissions among patients with advanced heart failure, n = 211.
Table S2. Risk factors for unplanned hospital readmissions.
Figure S1. Mortality since enrolment, n = 250.