

Abstract
Introduction
In a multicenter, open-label randomized phase 3 clinical trial conducted in the Netherlands and Denmark, treatment with ex vivo-expanded tumor-infiltrating lymphocytes (TIL-NKI/CCIT) from autologous melanoma tumor compared with ipilimumab improved progression-free survival in patients with unresectable stage IIIC–IV melanoma after failure of first-line or second-line treatment. Based on this trial, we conducted a cost-utility analysis.
Methods
A Markov decision model was constructed to estimate expected costs (expressed in 2021€) and outcomes (quality-adjusted life years (QALYs)) of TIL-NKI/CCIT versus ipilimumab in the Netherlands. The Danish setting was assessed in a scenario analysis. A modified societal perspective was applied over a lifetime horizon. TIL-NKI/CCIT production costs were estimated via activity-based costing. Through sensitivity analyses, uncertainties and their impact on the incremental cost-effectiveness ratio (ICER) were assessed.
Results
Mean total undiscounted lifetime benefits were 4.47 life years (LYs) and 3.52 QALYs for TIL-NKI/CCIT and 3.33 LYs and 2.46 QALYs for ipilimumab. Total lifetime undiscounted costs in the Netherlands were €347,168 for TIL-NKI/CCIT (including €67,547 for production costs) compared with €433,634 for ipilimumab. Undiscounted lifetime cost in the Danish scenario were €337,309 and €436,135, respectively. This resulted in a dominant situation for TIL-NKI/CCIT compared with ipilimumab in both countries, meaning incremental QALYs were gained at lower costs. Survival probabilities, and utility in progressive disease affected the ICER most.
Conclusion
Based on the data of a randomized phase 3 trial, treatment with TIL-NKI/CCIT in patients with unresectable stage IIIC–IV melanoma is cost-effective and cost-saving, both in the current Dutch and Danish setting. These findings led to inclusion of TIL-NKI/CCIT as insured care and treatment guidelines. Publicly funded development of the TIL-NKI/CCIT cell therapy shows realistic promise to further explore development of effective personalized treatment while warranting economic sustainability of healthcare systems.
Keywords: Ipilimumab, Melanoma, Healthcare Economics and Organizations
WHAT IS ALREADY KNOWN ON THIS TOPIC.
This study is the first to assess cost-effectiveness in a multicenter, open-label randomized phase 3 clinical trial of an ex vivo-expanded tumor-infiltrating lymphocytes (TIL-NKI/CCIT) from autologous melanoma tumor compared with ipilimumab in patients with unresectable stage IIIC–IV melanoma after failed first-line or second-line treatment.
WHAT THIS STUDY ADDS
Treatment with TIL-NKI/CCIT in patients with unresectable stage IIIC–IV melanoma is cost-effective and cost-saving, both in the current Dutch and Danish setting. These findings led to inclusion of TIL-NKI/CCIT as insured care and treatment guidelines.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Publicly funded development of the TIL-NKI/CCIT cell therapy shows realistic promise to further explore development of effective personalized treatment while warranting economic sustainability of healthcare systems.
Introduction
Advanced melanoma is an aggressive malignant disease with high mortality as a hallmark. The introduction of targeted therapies and immune checkpoint inhibitors (ICI) has substantially improved clinical outcomes in patients with advanced melanoma.1 2 After failure of first-line ICI treatment with anti-PD-1 antibodies, such as nivolumab or pembrolizumab, in patients with unresectable stage IIIC–IV cutaneous melanoma, second-line treatment with ipilimumab (anti-CTLA-4 antibody) monotherapy or ipilimumab/nivolumab combined has shown modest objective response rates up to 13% and 31%, respectively.3 4 For patients harboring a BRAF mutation (approximately 50% of melanomas), second-line treatment with BRAF/MEK inhibitors has shown better objective response rates of 22%–57%, but this clinical benefit is often short-lived.5 6 As limited clinical benefit is observed for second-line treatment with the currently available immuno and targeted therapies, there is a clear unmet medical need for novel treatment modalities for patients with unresectable stage IIIC–IV melanoma after first-line treatment failure.
Adoptive cell therapy with ex vivo-expanded tumor-infiltrating lymphocytes (TIL) from autologous melanoma tumors has been one of the first cell therapies developed with public funding by hospitals reaching advanced development milestones. Over the past years, multiple non-randomized single institution phase 2 clinical trials have been conducted in the USA, Israel and Europe, representing TIL as a safe and effective strategy to treat patients with metastatic melanoma.7–12 Recently, we showed statistically significant and clinically relevant improved progression-free survival (PFS) in patients with unresectable stage IIIC–IV melanoma after failed first-line or second-line treatment with tumor-infiltrating lymphocytes (TIL-NKI/CCIT) compared with ipilimumab, in a multicenter, open-label, randomized phase 3 clinical trial.13
Ex vivo-expanded TIL-NKI/CCIT are regulated as advanced therapy medicinal product (ATMP).14 As a consequence, the product needs to comply with stringent medicinal product quality, safety and efficacy standards. Therefore, substantial upfront public investments were needed, for example a fully equipped ATMP production facility with Good Manufacturing Practice-manufacturing license, skilled technical staff and controlled (hospital) logistics. To assess (financial) challenges, clinical implementation scenarios and an early cost-utility analysis (CUA) were conducted.15–17 The early-CUA estimated that TIL-NKI/CCIT was expected to yield more quality-adjusted life years (QALYs) at lower costs, based on early phase 2 clinical trial data and expert opinion. However, due to high evidentiary and clinical uncertainty, the need was expressed to reassess cost-effectiveness when confirmative clinical and cost data were available.
Therefore, the objective was to conduct a CUA based on a multicenter, open-label, randomized phase 3 clinical trial, calculating the incremental cost-effectiveness ratio (ICER) of treatment with TIL-NKI/CCIT compared with standard of care with ipilimumab in patients with unresectable stage IIIC–IV melanoma after failed first-line or second-line treatment. The phase 3 trial with TIL-NKI/CCIT was conducted as part of a coverage with evidence development (CED) program in the Netherlands in collaboration with Denmark.9 18
Methods
Study design
A prospective CUA was conducted assessing life years (LYs), QALYs and costs for patients with unresectable stage IIIC–IV melanoma after failed of first-line or second-line treatment comparing TIL-NKI/CCIT to standard of care treatment with ipilimumab. The CUA was based on the multicenter, open-label, randomized phase 3 clinical trial (TIL-NKI/CCIT trial: NCT02278887) conducted at the Netherlands Cancer Institute (NKI), the Netherlands, and the National Center for Cancer Immune Therapy (CCIT-DK), Denmark.13 A modified societal perspective was used with a lifetime horizon. The Dutch setting is presented as the base case, the Danish setting was included in a scenario analysis. Differences between the scenarios were country-specific costs. Methods and results adhere to the Consolidated Health Economic Evaluation Reporting Standards guidelines for cost-effectiveness analysis.
Model description
Treatment sequence was simulated by means of a Markov model. The Markov model included three mutually exclusive health states: PFS, progressive disease (PD) and death (all causes), see figure 1. In both treatment arms, all patients started in the PFS state. At the start of each cycle, patients could remain in the PFS state, could progress to PD or could progress to the absorbing death state. When progressed to PD, patients could remain in this state or progress to death. Cycle length was 3 months. Each cycle was associated with a health-state specific cost and utility, which accumulated over time. Base case model input parameters are reported in table 1, and a more detailed overview of input parameters is included in online supplemental table S1. PFS and PD probabilities over time per treatment arm are shown in online supplemental figure S1.
Figure 1.

Model structure. Structure of the decision tree presented as a flow-diagram of treatment with ex vivo-expanded tumor infiltrating lymphocytes from autologous melanoma tumor (TIL-NKI/CCIT) and ipilimimab-arm combined with the Markov decision-model with three mutually exclusive health states: progression-free survival (PFS), progressive disease (PD) and the absorbing state death.
Table 1.
Base case input parameters in Markov decision model for the Netherlands
| Costs tumor infiltrating lymphocytes (TIL-NKI/CCIT) | |||||
| Healthcare cost (progression free survival) | Base case | Unit | Source | ||
| Screening | € 3 822 | Per patient | 13 44 | ||
| Physical examination | € 2 917 | Per patient | 13 44 | ||
| Lab tests | € 607 | Per patient | 13 44 | ||
| Consultations | € 298 | Per patient | 13 44 | ||
| TIL-NKI/CCIT isolation | € 2,043 | Per patient | 13 44 | ||
| Surgery | € 1 583 | Per patient | 13 44 | ||
| Hospital admission | € 420 | Per patient | 13 44 | ||
| Consultations | € 40 | Per patient | 13 44 | ||
| TIL-NKI/CCIT production | € 67 547 | Per product | 13 44 | ||
| Hospital admission and follow-up | € 44 528 | Per patient | 13 44 | ||
| Hospital admission | € 20 706 | Per patient | 13 44 | ||
| Medications | € 12 190 | Per patient | 13 44 | ||
| Laboratory tests | € 5 004 | Per patient | 13 44 | ||
| Blood products | € 1 926 | Per patient | 13 44 | ||
| Consultations | € 205 | Per patient | 13 44 | ||
|
Specialized nurse Others (eg, ECG, CT, chest X-ray, supportive care) |
€ 2 429 € 2 069 |
Per patient Per patient |
13 44 | ||
| Total costs TIL-NKI/CCIT treatment | € 117 940 | Per patient | |||
| Healthcare costs (progressive disease)* | Base case | Unit | Source | ||
| Ipilimumab monotherapy | € 66 388 | 0.20 | 13 44 | ||
| BRAF/MEK inhibitor | € 101 224 | 0.20 | 13 44 | ||
| Ipilimumab/nivolumab combination therapy | € 72 514 | 0.11 | 13 44 | ||
| Pembrolizumab | € 54 571 | 0.01 | 13 44 | ||
| No treatment | € 0 | 0.43 | 13 44 | ||
| Other (temozolomide, ipilimumab/pembrolizumab) | € 96 448 | 0.05 | 13 44 | ||
| Death | Base case | Unit | Source | ||
| Costs associated with (3 months prior to) death | € 1 516 | Per patient | 13 44 | ||
| Societal costs | Base case | Unit | Source | ||
| Direct patient costs (medication, homecare, travel) | € 227 | First cycle | 13 44 | ||
| Direct patient costs (medication, homecare, travel) | € 82 | >First cycle | 13 44 | ||
| Direct patient costs (copay) | € 385 | Per year | 13 44 | ||
| Informal care | € 710 | First cycle | 13 38 44 | ||
| Informal care | € 99 | >First cycle | 13 38 44 | ||
| Productivity loss | € 3 539 | First cycle | 13 38 44 | ||
| Productivity loss | € 75 | >First cycle | 13 38 44 | ||
| Costs ipilimumab | |||||
| Healthcare costs (progression-free survival) | Base case | Unit | Source | ||
| Screening | € 2 507 | Per patient | 13 44 | ||
| Physical examination and lab tests | € 2 507 | Per patient | 13 44 | ||
| Ipilimumab treatment | € 75 316 | Per patient | 13 44 | ||
| Hospital admission | € 3 200 | Per patient | 13 44 | ||
| Ipilimumab, including supportive medicines | € 66 388 | Per patient | 13 44 | ||
| Lab tests | € 2 103 | Per patient | 13 44 | ||
| Blood products | € 105 | Per patient | 13 44 | ||
| Consultations | € 648 | Per patient | 13 44 | ||
| Others (eg, ECG, CT, chest X-ray, supportive care) | € 2 872 | Per patient | 13 44 | ||
| Total costs ipilimumab treatment | € 77 823 | Per patient | |||
| Healthcare costs (progressive disease)* | Base case | Unit | Source | ||
| Ipilimumab rechallenge | € 66 388 | 0.02 | 13 44 | ||
| BRAF/MEK inhibitor | € 101 224 | 0.29 | 13 44 | ||
| Pembrolizumab | € 54 571 | 0.10 | 13 44 | ||
| No treatment/other trial | € 0 | 0.57 | 13 44 | ||
| Other (dacarbazine, temozolomide) | € 6 814 | 0.02 | 13 44 | ||
| Death | Base case | Unit | Source | ||
| Costs associated with (3 months prior to) death | € 1 516 | Per patient | 13 44 | ||
| Societal costs | Base case | Unit | Source | ||
| Direct patient costs (medication, homecare, travel) | € 210 | First cycle | 13 44 | ||
| Direct patient costs (medication, homecare, travel) | € 27 | >First cycle | 13 44 | ||
| Direct patient costs (copay) | € 385 | Per year | 13 44 | ||
| Informal care | € 916 | First cycle | 13 38 44 | ||
| Informal care | € 99 | >First cycle | 13 38 44 | ||
| Productivity loss | € 3 539 | First cycle | 13 38 44 | ||
| Productivity loss | € 75 | >First cycle | 13 38 44 | ||
| Survival (probabilities) | |||||
| TIL | Ipilimumab | ||||
|
Modeled
PFS† |
Modeled
OS† |
Modeled PFS† |
Modeled
OS† |
Source | |
| Baseline | 1.000 | 1.000 | 1.000 | 1.000 | 13 44 |
| Month 3 | 0.792 | 0.942 | 0.635 | 0.936 | 13 44 |
| Month 6 | 0.612 | 0.871 | 0.269 | 0.847 | 13 44 |
| Month 9 | 0.485 | 0.801 | 0.129 | 0.759 | 13 44 |
| Month 12† | 0.395 | 0.735 | 0.072 | 0.679 | 13 44 |
| Utilities | |||||
| Stable disease | Base case | Unit | Source | ||
| TIL-NKI/CCIT: baseline | 0.874 | Per cycle | 13 24 45 | ||
| TIL-NKI/CCIT: month 3 | 0.879 | Per cycle | 13 24 45 | ||
| TIL-NKI/CCIT: month 6 | 0.885 | Per cycle | 13 24 45 | ||
| TIL-NKI/CCIT: month 9 | 0.881 | Per cycle | 13 24 45 | ||
| TIL-NKI/CCIT: month 12† | 0.887 | Per cycle | 13 24 45 | ||
| Ipilimumab: baseline | 0.838 | Per cycle | 13 24 45 | ||
| Ipilimumab: month 3 | 0.840 | Per cycle | 13 24 45 | ||
| Ipilimumab: month 6 | 0.841 | Per cycle | 13 24 45 | ||
| Ipilimumab: month 9 | 0.849 | Per cycle | 13 24 45 | ||
| Ipilimumab: month 12‡ | 0.828 | Per cycle | 13 24 45 | ||
| Progressive disease | Base case | Unit | Source | ||
| Ipilimumab (rechallenge) | 0.764 | Per cycle | 32 | ||
| Ipilimumab/nivolumab combination therapy | 0.695 | Per cycle | 46 | ||
| BRAF/MEK inhibitor | 0.844 | Per cycle | 47 | ||
| Pembrolizumab | 0.707 | Per cycle | 48 | ||
| Temozolomide | 0.730 | Per cycle | 49 | ||
| Dacarbazine | 0.791 | Per cycle | 50 | ||
| No treatment after TIL-NKI/CCIT | 0.832 | Per cycle | 13 | ||
| No treatment after ipilimumab | 0.764 | Per cycle | 13 | ||
| Death (applied to 3 months prior to death) | 0.665 | Per cycle | 40 | ||
*Healthcare costs progressive disease: costs for nivolumab and ipilimumab were based on the schedule 1 mg/kg nivolumab+3 mg/kg ipilimumab every 3 weeks for four cycles, followed by 240 mg/2 weeks per model cycle until progression or death. Costs for BRAF/MEK were based on the regimen dabrafenib (150 mg/2dd)/trametinib (2 mg/1dd). Pembrolizumab was based on 200 mg intravenous every 3 weeks cycle until progression or death. Temozolomide regimen was based on 150 mg/m2 two times a day for 7 days for four cycles and dacarbazine 850 mg/m2 for three cycles. ±PFS and OS estimates are derived from the TIL-NKI/CCIT-study and modeled to fit and extrapolated beyond the trial time horizon using a log-logistic distribution.
†PFS and OS estimates are derived from the TIL-NKI/CCIT-study and modeled to fit and extrapolated beyond the trial time horizon using a log-logistic distribution.
‡PFS, OS and utility values are beyond 12 months and reported in more detail elsewhere.13 A formal data request can be directed to the NKI/AvL. For terms and procedure, we refer to the data sharing agreement in the initial publication.13
BRAF/MEK, v-Raf murine sarcoma viral oncogene homolog B1/mitogen activated protein kinase; OS, overall survival; PFS, progression-free survival; TIL-NKI/CCIT, ex vivo-expanded tumor infiltrating lymphocytes from autologous melanoma tumor.
jitc-2023-008372supp001.pdf (4.2MB, pdf)
Patients
After eligibility screening for the TIL-NKI/CCIT-trial, 168 patients were randomly assigned to receive either TIL-NKI/CCIT treatment (84 patients) or standard ipilimumab treatment (84 patients). Of 168 patients, 132 were treated in the Netherlands and 36 in Denmark, with an even distribution between treatments arms. Baseline characteristics were well-balanced in both study groups.13 The primary trial endpoint was PFS, as defined by Response Evaluation Criteria In Solid Tumors (RECIST), version 1.1.
Intervention and comparator
The intervention of interest was TIL-NKI/CCIT cell therapy. After randomization to the TIL-NKI/CCIT treatment arm, patients underwent surgical resection of a melanoma metastasis for TIL-NKI/CCIT production according to the TIL-NKI/CCIT-treatment protocol (figure 1). This was followed by TIL-NKI/CCIT infusion, preceded by non-myeloablative lymphodepleting chemotherapy.13 TIL-NKI/CCIT infusion consisted of the single intravenous adoptive transfer of at least 5×109 autologous TILs, followed by administration of high-dose bolus interleukin 2 (600.000 IU/kg/dose every 8 hours intravenous with a maximum of 15 doses). Supportive care comprised thrombocyte and erythrocyte transfusions until spontaneous hematopoietic recovery. The trial showed that after disease progression on TIL-NKI/CCIT therapy, 20% of patients switched to ipilimumab monotherapy, 20% to BRAF/MEK combination therapy, 11% to ipilimumab/nivolumab combination therapy, 1% to pembrolizumab, 5% to other treatments (25% temozolomide, 75% ipilimumab/pembrolizumab) and the remaining 43% received no further treatment (table 1 and online supplemental table S1).
TIL-NKI/CCIT treatment was compared with ipilimumab, which was standard of care for this population at time of trial initiation. Ipilimumab was administered according to the standard regimen of 3 mg/kg intravenous once every 3 weeks, for maximum of four cycles.19–21 After progression on ipilimumab treatment, 29% of patients continued on BRAF/MEK combination therapy, 10% on pembrolizumab, 2% on ipilimumab (rechallenge), 2% on other treatments (50% dacarbazine, 50% temozolomide) and the remaining 57% of patients continued to participate in another clinical trial (20%) or received no further treatment (37%), see table 1 and online supplemental table S1.
Health effects
Survival
Health state transition probabilities were informed by PFS and overall survival (OS) data from the TIL-NKI/CCIT trial.13 The cut-off for clinical data collection was June 9, 2022. Of the survival curves, log-cumulative hazard plots were compared for initial model selection and extrapolated beyond trial duration by fitting individual parametric survival curves. Best fit was assessed according to the Akaike Information Criterion, Bayesian Information Criterion and visual (expert) inspection.22 23 This resulted in the selection of the log-logistic, see online supplemental table S2. Online supplemental fi gure S1 includes PFS and PD probabilities over time and best fitted parametric survival curves. The model was cut-off if patients reached the age of 100 years or 99.9% of patients were deceased.
Health state utilities
For each treatment arm, QALYs were calculated based on utilities. A utility is a standardized score between 0 and 1, with 0 reflecting death and 1 perfect health, measured via the EuroQol 5D-3L (EQ-5D) questionnaire. When utility is multiplied by length of survival, it yields a QALY. To derive utilities from the EQ-5D questionnaire, country-specific Dutch and Danish EQ-5D tariffs were applied to the appropriate cohorts.24 25 After disease progression, QALY measurements were discontinued as per study protocol. For patients continuing to a next line of treatment, a treatment-specific utility was extracted from literature (table 1 and online supplemental table S1).26–29
Resource use and costs
Treatment costs
For the Dutch study population, the TIL-NKI/CCIT products were developed and manufactured at the NKI and Sanquin Bloodbank, therefore no formal list price was available. The costs per TIL-NKI/CCIT product were therefore calculated via the cell therapy manufacturing cost framework using activity-based costing.30 31 A detailed cost calculation was conducted in each center, more detail is included in online supplemental methods.
Ipilimumab treatment costs comprised drug costs, patient hospital admission for treatment and supportive medication (ie, infliximab for adverse events). Base cases were calculated by matching trial informed population mean dosage, patient weight and admission frequency to Dutch 2021 drug list tariffs, see table 1 and online supplemental table S1.
Healthcare resources
Healthcare utilization included physical examinations, hospital admissions, laboratory tests, blood products, imaging and (surgical) interventions (table 1 and online supplemental table S1). Occurrence and frequency of consumed resources was informed by the TIL-NKI/CCIT-trial and extracted from hospital records. In the base case, resource use was multiplied with Dutch 2021 unit costs in Euros (€), in adherence with the Dutch guideline on costing research in healthcare. As per trial protocol, post-treatment follow-up was modeled concurrently with clinical and health-related quality of life questionnaire follow-up. These follow-ups were assumed to stop after 5 years, as ongoing medical insight reports that patients without signs of PD after 5 years are considered cured.32
Non-healthcare related costs
In adherence to the modified societal perspective, non-hospital related healthcare costs, out-of-pocket expenses and treatment-related travel costs were also included. In the first health-related quality of life follow-up questionnaire, patients were asked once to report costs related to travel, medication and homecare. It was assumed these were representative of the preceding years. In addition, costs of productivity loss (absenteeism) were included for patients who reported employment (42%, average 0.52 fte) for the 2021 friction period (78.9 days).33 34 In addition, productivity loss and travel expenses were included for family and friends, assuming that in 50% of hospital visits a patient was accompanied by someone who had to take half a day off.
Statistical analysis
The model was constructed in Microsoft Excel, 2010 (Microsoft, Redmond, WA). Incremental benefits and costs between treatment arms were expressed using the ICER and were calculated based on the intention-to-treat analysis of the TIL-NKI/CCIT-trial.13 The ICER captures the incremental costs per full QALY gained of an intervention compared with another: ICER=(Costsintervention–CostsStandardOfCare)/(QALYintervention–QALYStandardOfCare).
Further statistical analyses were performed using R statistical computing V.4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). QALYs over time were modeled via generalized estimating equations.35 36 Missing items from the EQ-5D were imputed according to the EQ-5D scoring guidelines by using R multivariate imputation via chained equation package, using baseline characteristics, treatment outcome, EQ-5D-questionnaires and costs as predictors.37 Dutch discount rates were applied in the base case; 4.0% on costs and 1.5% on benefits (LYs and QALYs).38 Discounting was applied to convert future costs and effects to their present value.39
Sensitivity analyses
Uncertainty around parameter estimates were explored via deterministic (DSA) and probabilistic sensitivity analyses (PSA). The DSA explores the impact of individual parameters by alternately varying input values between pre-set minimum and maximum values and can be considered parameter-specific best-case and worst-case scenarios. Minimum and maximum values were informed by 95% CIs or variance of the mean by ±20% (table 1 and online supplemental table S1).
A PSA provides a more comprehensive uncertainty estimate by simultaneously sampling all parameters. This was done by sampling 10,000 iterations of all model input parameters according to their individual appropriate minimum, maximum and distributions. In addition, here the PSA was presented with a relative density plot to better visualize uncertainty and clustering of ICER-estimates. With the PSA output, the probability of a treatment being cost-effective for a given willingness-to-pay (WTP) threshold was estimated, which is presented as a cost-effectiveness acceptability curve (CEAC). The Dutch informal WTP of €80,000/incremental QALY was applied.40
Scenario analysis
In addition to the Dutch base case analysis, a scenario analysis was conducted in which costs for the Danish setting were included, see online supplemental table S3. The survival and quality of life input parameters in the scenario were the same as in the Dutch base case setting (table 1 and online supplemental table S1). Costs were estimated by multiplying mean population used drug and healthcare utilization with Danish 2021 tariffs and converted from Danish kroner (DKK) to Euros (€). Also, country specific discount rates of 3.5% for both costs and (QA)LYs were applied in line with methods of the Danish Medicines Council, and an adjusted friction period (75.4 days) was applied to estimate productivity loss.33 34 38 41 In Denmark, no WTP-threshold has been reported. Therefore, The WHO’s Choosing Interventions that are Cost-Effective recommendation was adopted, which states that an intervention with a cost/QALY of less than the national annual gross domestic product (GDP) per capita, is considered cost-effective. This translates to an informal threshold of €50,000/incremental QALY based on the Danish GDP per capital as of December 2021.
Results
Benefits and costs of treatments
Higher total LYs, QALYs and lower total costs for the TIL-NKI/CCIT treatment compared with treatment with ipilimumab were observed in both the Dutch base case and Danish scenario analysis. Treatment with TIL-NKI/CCIT resulted in mean undiscounted LYs of 4.47 (95% credibility interval (CrI) 3.88–5.29) and QALYs of 3.52 (95% CrI 3.30–4.59) compared with 3.33 (95% CrI 2.88–4.00) LY and 2.46 (95% CrI 1.47–3.41) QALYs for patients treated with ipilimumab (table 2 and online supplemental table S4).
Table 2.
Undiscounted and discounted base case life years, quality adjusted life years, costs and incremental cost-effectiveness ratios of TIL-NKI/CCIT-treatment compared with Ipilimumab in the Netherlands
| Undiscounted | Discounted* | |||||
| TIL-NKI/CCIT | Ipilimumab | Incremental | TIL-NKI/CCIT | Ipilimumab | Incremental | |
| 5 years | Mean | |||||
| Life years | 2.46 | 2.11 | 0.35 | 2.40 | 2.06 | 0.34 |
| QALYs | 1.94 | 1.53 | 0.41 | 1.89 | 1.49 | 0.40 |
| Costs | € 224,502 | € 283,100 | € −58,599 | € 214,089 | € 266,455 | € −52,366 |
| ICER | Dominant | Dominant | ||||
| 10 years | ||||||
| Life years | 3.38 | 2.72 | 0.66 | 3.23 | 2.61 | 0.62 |
| QALYs | 2.66 | 1.99 | 0.67 | 2.55 | 1.91 | 0.64 |
| Costs | € 279,683 | € 358,242 | € −78,559 | € 255,931 | € 323,591 | € −67,660 |
| ICER | Dominant | Dominant | ||||
| Lifetime | ||||||
| Total LYs | 4.47 | 3.33 | 1.14 | 4.09 | 3.10 | 0.99 |
| Total QALYs | 3.52 | 2.46 | 1.06 | 3.22 | 2.28 | 0.94 |
| Total costs | € 347,168 | € 433,634 | € −86,467 | € 292,369 | € 365,068 | € −72,699 |
| ICER | Dominant | Dominant | ||||
Calculated ICER=(Costsintervention–CostsStandardOfCare)/(QALYintervention–QALYStandardOfCare).
*Costs are discounted with 4% per year and effects (life years and QALYs) with 1.5% per year in line with Dutch guidelines for economic evaluations. Discounting is applied to adjust future costs and effects to their present value.
ICER, incremental cost-effectiveness ratio; QALYs, quality-adjusted life years; TIL-NKI/CCIT, ex vivo-expanded tumor infiltrating lymphocytes from autologous melanoma tumor.
In the Netherlands, mean lifetime undiscounted societal costs per patient were €347,168 (95% CrI €269,889–447,100) for TIL-NKI/CCIT compared with €433,634 (95% CrI €329,255–571,253) for ipilimumab, and in the Danish scenario €337,309 (95% CrI €264,324–438,132) versus €436,135 (95% CrI €331,304–€572,222), respectively (table 2 and online supplemental table S4). Adjusted benefits and costs with country-specific discount rates are presented in table 2 and online supplemental table S4.
Although initial costs of TIL-NKI/CCIT production and treatment-related healthcare costs were higher in the base case and scenario than ipilimumab costs, the cost savings seem to be driven by longer observed and modeled PFS in the TIL-NKI/CCIT cohort. Prolonged PFS consequently delayed or prevented the need for additional care and switching to (more costly) next-line oncological treatments.
Deterministic and probabilistic sensitivity analyses
The result of the base case DSA is shown in the tornado diagram (figure 2). The parameters with the biggest impact on the ICER were survival probabilities, quality of life in PD and next-line treatment cost in PD. The DSA for the Danish scenario is included in online supplemental figure S2 and shows similar results.
Figure 2.

Deterministic (univariate) sensitivity analysis. Results of the deterministic (univariate) sensitivity analysis visualized in a tornado diagram. The diagram shows the impact of discounted individual parameters on the incremental cost-effectiveness ratio by alternately varying input values one by one between pre-set minimum and maximum values (see table 1). BRAF/MEK, V-Raf murine sarcoma viral oncogene homolog B1/mitogen activated protein kinase; ipi, ipilimumab; OS, overall survival; PFS, progression-free survival; Prob, probability; QALY, quality-adjusted life year; TIL-NKI/CCIT, ex vivo-expanded tumor infiltrating lymphocytes from autologous melanoma tumor; Tx, treatment; #, number.
The probability of TIL-NKI/CCIT being cost-effective compared with ipilimumab, at a WTP-threshold of €80,000 per QALY, was >99% in the Dutch base case, as can be seen in the CEAC (online supplemental figure S3). The PSA results are visualized in figure 3. This plot shows that almost all simulated ICER estimates are located in the south-east quadrant of the cost-effectiveness plane, and no ICER-estimates are located above the WTP-threshold. The CEAC for the Danish setting is shown in online supplemental figure S4 and shows that, in line with the PSA in online supplemental figure S5, at a WTP of €50,000, the chance of TIL-NKI/CCIT being cost-effective in comparison to ipilimumab, is 99%. Despite the uncertainty quantified in the input parameters, the likelihood of treatment with TIL-NKI-CCIT compared with ipilimumab being cost-effective is ≥99% in both the Danish and Dutch situation. Moreso, in the base case as well as in a large proportion of estimates it is even cost-saving, while providing additional health benefits as treatment with more expensive oncological agents is avoided or postponed.
Figure 3.
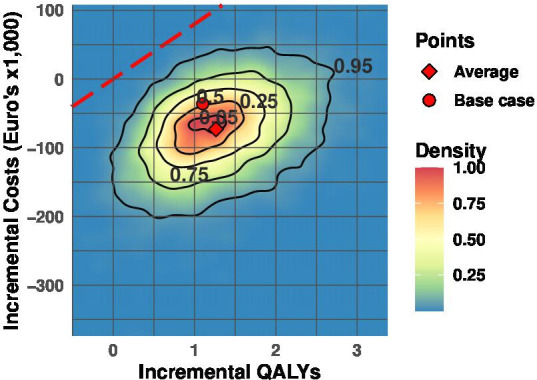
Probabilistic sensitivity analysis. Results of the probabilistic sensitivity analysis (PSA) visualized in cost-effectiveness plane. The PSA shows uncertainty of estimated discounted base case incremental cost-effectiveness ratio over a lifetime horizon by simultaneously sampling uncertainty across all parameters by 10,000 iterations. All model input parameters are sampled randomly, according to their individual appropriate distributions between pre-set minimum and maximum values (table 1). QALYs, quality-adjusted life years; WTP, willingness to pay.
Discussion
Based on the multicenter, randomized phase 3 trial, treatment with TIL-NKI/CCIT for patients with unresectable stage IIIC–IV melanoma, with the majority of patients with failed first-line treatment, is accompanied by a substantial gain in QALYs and by cost-savings in both a Dutch and Danish setting compared with treatment with standard of care ipilimumab.13 This indicates that TIL-NKI/CCIT therapy is cost-effective compared with standard ICI immunotherapy with ipilimumab for this patient population. In addition, to the best of our knowledge, this is the first cost-effectiveness analysis of a novel cell therapy developed by public funds, based on data from a randomized clinical phase 3 trial.
The CUA in this study was performed as part of a CED program.18 Within this program, a comprehensive Health Technology Assessment (HTA) was performed to identify challenges and to support timely access to the promising innovation. This HTA included a qualitative study assessing aspects that play a role in the implementation of cell therapies, where we found that public financing and a multidisciplinary approach was conditional.19 (30) Furthermore, an early CUA was performed, followed by a scenario study where several future development scenarios were incorporated.16 17 The results from the early CUA, which estimated that TIL-NKI/CCIT therapy could be cost-effective compared with treatment with ipilimumab, hold in the current trial-based CUA. Herewith, we demonstrated that conducting early economic evaluations—including scenarios—was informative and can support the design of product development strategies.
To estimate the costs per TIL-NKI/CCIT product, activity-based costing was applied. Production costs between small facilities differ greatly and are highly facility dependent.31 The costs per TIL-NKI/CCIT product presented here reflect true production costs during the clinical trial without marketing costs, (profit) margins, costs for obtaining and maintaining marketing authorization or early investments and will certainly be an underestimation compared with a more commercial setting.31 This means that if changes occur in organization or demand, it directly impacts the here presented production cost estimates. A TIL-NKI/CCIT adoption scenario analysis based on expert opinion, conducted as part of the CED, assumed commercial costs of TIL-NKI/CCIT would be at least three times higher.17 According to DSA results, if this assumption is applied, TIL-NKI/CCIT still remains the most cost-effective option compared with ipilimumab. However, in the context of increased interest in public funded cell therapy development, further research on efficiency, organization, upscaling of manufacturing and costing is needed.
The trial-based CUA design of this study provides a direct comparison between treatment arms and allows to take into account real-world (cost) data. This affected our analysis as guidelines describe four cycles of ipilimumab treatment in this population.20 Our data showed that patients received on average three cycles of ipilimumab due to ipilimumab-induced toxicity or rapid PD.13 This observation is in line with previous reports of real-world use of ipilimumab.42 Given the high costs of ipilimumab, the estimated cost-saving in this study might be an underestimation in populations that more often receive four cycles of ipilimumab. Although a trial-based analysis has numerous advantages, a limitation is its limited time horizon. To extrapolate trial data beyond trial duration to a lifetime horizon, assumptions were made regarding future follow-up activities. In addition, the optimal time to determine OS of both treatment modalities was not yet reached.13 Although a positive trend is visible in OS for TIL-NKI/CCIT therapy compared with ipilimumab, this difference did not (yet) reach statistical significance, despite profound differences in PFS.13 Consequently, the beneficial effect on survival on TIL-NKI/CCIT treatment reflected in the (QA)LYs might currently be underestimated. Furthermore, information on third and following treatment lines were available on a patient level, but associated costs and utilities were literature-derived due to the trial design. Also, indirect costs were not collected in line with current HTA-guidelines (the trial was designed under the 2010 Dutch guideline for costing studies), therefore assumptions were made to adhere to the societal perspective. Additionally, as often seen with clinical trials, the standard of care for patients with melanoma has moved from ipilimumab monotherapy to ipilimumab/nivolumab combination therapy for a specific patient population during the course of the trial.19 As there is no head-to-head comparisons yet available of ipilimumab/nivolumab versus TIL-NKI/CCIT, the cost-effectiveness of this comparator was not included in this study. As the price of ipilimumab/nivolumab is substantial, a large difference in survival is necessary to change the conclusion of this study. Whether our hypothesis stands will need to be clinically confirmed. Research is ongoing and results of a head-to-head trial comparing ipilimumab and ipilimumab/nivolumab in a similar population are expected in 2024/2025.43
Clinical interpretation
Although the mean costs of TIL-NKI/CCIT treatment (including TIL-NKI/CCIT production and hospital admission) itself were higher compared with ipilimumab in patients with metastatic melanoma, the considerable increase in observed and modeled survival, delayed or forgone need for additional care, and (more costly) next-line treatment led to overall cost savings. This demonstrates the need to assess clinical and economic impact of new therapies not just based on its initial costs, but also on their impact on the healthcare and care pathways as a whole.
Even though advancements of metastatic melanoma treatment move towards ipilimumab/nivolumab combination therapy for a part of the population, the results of the phase 3 trials and this cost-effectiveness analysis have demonstrated impact on treatment guidelines in the Netherlands and Denmark. However, large scale implementation of TIL-NKI/CCIT treatment may still be associated with production and logistical challenges due to its personalized nature. Therefore, continued efforts are needed to address these challenges. This is emphasized, as TIL-NKI/CCIT therapy is one of the first cell therapies developed by two hospitals using public financing and is moving towards European market access.
To conclude, TIL-NKI/CCIT treatment for patients with unresectable stage IIIC–IV cutaneous melanoma failed first-line or second-line treatment showed gained QALYs against less costs, both in a Dutch and Danish setting in comparison to treatment with standard ipilimumab. This supported reimbursement of TIL-NKI/CCIT as well as impacted treatment guidelines in this patient population. In addition, development of cell therapies by research institutes and hospitals funded by public money show realistic promise to further explore effective personalized treatment while warranting the economic sustainability of healthcare systems.
Acknowledgments
We would like to thank all patients and their families for their contribution and for making this trial possible. Additionally, we thank all co-workers from the Netherlands Cancer Institute (NKI) and National Center for Cancer Immune Therapy (CCIT-DK) for making this trial run successfully. We would especially like to acknowledge the nursing staff/ward and the departments of surgery, radiology, pulmonology, dermatology, cardiology, intensive care unit, clinical laboratory and ophthalmology (external centers). In addition, we would like to thank dr. Miriam van de Meulen for her methodological input.
Footnotes
Twitter: @tenham2, @doniamarco
Presented at: Work was partly presented at the European Society for Medical Oncology Congress, September 10, 2022.
Contributors: VR, WvH, RMTtH, MR and JH designed the study. MR, RK, WS, WS, BN, CN, ML, TM, MD, IMS gathered and analyzed data. ML, RMTtH and VR performed the analyses and simulations. VR and RMTtH took the lead in writing the manuscript. VR is acting as guarantor. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Funding: This trial was supported by the Dutch Cancer Society (KWF Kankerbestrijding), the Netherlands Organization for Health Research and Development (837004011), the Dutch Ministry of Health, Stichting Avento, the Danish Cancer Society and Capital Region of Denmark Research Foundation.
Competing interests: THB: Bristol-Myers Squibb(speaker engagement). MD: Achiles Therapeutics (consulting), Astra Zeneca (teaching), Bristol-Myers Squibb (consulting and teaching), F. Hoffman-La Roche (speaker engagement), Genentech (consulting), Merck (speaker engagement), Novartis (speaker engagement). JH: Achilles Therapeutics (Scientific Advisory Board), Amgen (funding), Asher Bio (funding), Bayer (consulting), BioNtech US (Scientific Advisory Board, funding), Bristol-Myers Squibb (consulting, funding, teaching), Eisai (consulting), ESMO IOTECH (Editor-in-chief), Gadeta (Scientific Advisory Board), Immunocore (Scientific Advisory Board), Instil Bio (consulting, teaching), Iovance Biotherapeutics (consulting, teaching), Ipsen Bioscience Inc (consulting), Merck Serono (consulting, teaching), Merck Sharp & Dohme Corporation (funding, consulting, teaching), Molecular Partners (consulting), Neogene Therapeutics (Scientific Advisory Board, shareholder), Novartis (funding, consulting, teaching), Pfizer (consulting, teaching), PokeAcel (Scientific Advisory Board), Roche/Genentech (consulting, teaching), Sanofi (consulting, teaching), Scenic (Scientific Advisory Board), Seattle Genetics (consulting), T-Knife (Scientific Advisory Board), Vaximm (Scientific Advisory Board). IMS: Adaptimmune (funding), Bristol-Myers Squibb (speaking engagement), Enara Bio (funding), Evaxion (funding), IO biotech (funding, stock, consulting), Lytix Biopharma (funding), Merck (speaking engagement and funding), Novartis (consulting), Pierre Fabre Pharmaceuticals, Inc (speaking engagement and consulting), Sanofi Pasteur Inc (speaking engagement), TILT Biotherapeutics (funding). Other authors declare to have no competing interests.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
This study involves human participants and was approved by the Dutch Central Committee on Research Involving Human Subjects and the Danish competent authority (NCT02278887). All the patients provided written informed consent prior to receiving treatment.
References
- 1. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with Ipilimumab in patients with metastatic Melanoma. N Engl J Med 2010;363:711–23. 10.1056/NEJMoa1003466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Luke JJ, Flaherty KT, Ribas A, et al. Targeted agents and Immunotherapies: optimizing outcomes in Melanoma. Nat Rev Clin Oncol 2017;14:463–82. 10.1038/nrclinonc.2017.43 [DOI] [PubMed] [Google Scholar]
- 3. Pires da Silva I, Ahmed T, Reijers ILM, et al. Ipilimumab alone or Ipilimumab plus anti-PD-1 therapy in patients with metastatic melanoma resistant to anti-PD-(L)1 monotherapy: a multicentre, retrospective, cohort study. Lancet Oncol 2021;22:836–47. 10.1016/S1470-2045(21)00097-8 [DOI] [PubMed] [Google Scholar]
- 4. Vanderwalde AM, Moon J, Kendra K, et al. S1616: Ipilimumab plus nivolumab versus Ipilimumab alone in patients with metastatic or unresectable melanoma that did not respond to anti-PD-1 therapy [abstract]. Cancer Res 2022;82:CT013. 10.1158/1538-7445.AM2022-CT013 [DOI] [Google Scholar]
- 5. Ackerman A, Klein O, McDermott DF, et al. Outcomes of patients with metastatic melanoma treated with immunotherapy prior to or after BRAF inhibitors. Cancer 2014;120:1695–701. 10.1002/cncr.28620 [DOI] [PubMed] [Google Scholar]
- 6. Weichenthal M, Ugurel S, Leiter UM, et al. Salvage therapy after failure from anti-PD-1 single agent treatment: a study by the German adoreg melanoma registry. JCO 2019;37:9505. 10.1200/JCO.2019.37.15_suppl.9505 [DOI] [Google Scholar]
- 7. Besser MJ, Shapira-Frommer R, Treves AJ, et al. Clinical responses in a phase II study using adoptive transfer of short-term cultured tumor infiltration lymphocytes in metastatic Melanoma patients. Clin Cancer Res 2010;16:2646–55. 10.1158/1078-0432.CCR-10-0041 [DOI] [PubMed] [Google Scholar]
- 8. Radvanyi LG, Bernatchez C, Zhang M, et al. Specific lymphocyte subsets predict response to adoptive cell therapy using expanded autologous tumor-infiltrating lymphocytes in metastatic melanoma patients. Clin Cancer Res 2012;18:6758–70. 10.1158/1078-0432.CCR-12-1177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. van den Berg JH, Heemskerk B, van Rooij N, et al. Tumor infiltrating lymphocytes (TIL) therapy in metastatic melanoma: boosting of neoantigen-specific T cell reactivity and long-term follow-up. J Immunother Cancer 2020;8:e000848. 10.1136/jitc-2020-000848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Goff SL, Dudley ME, Citrin DE, et al. Randomized, prospective evaluation comparing intensity of Lymphodepletion before adoptive transfer of tumor-infiltrating lymphocytes for patients with metastatic Melanoma. J Clin Oncol 2016;34:2389–97. 10.1200/JCO.2016.66.7220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Seitter SJ, Sherry RM, Yang JC, et al. Impact of prior treatment on the efficacy of adoptive transfer of tumor-infiltrating lymphocytes in patients with metastatic melanoma. Clin Cancer Res 2021;27:5289–98. 10.1158/1078-0432.CCR-21-1171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rosenberg SA, Yang JC, Sherry RM, et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using t-cell transfer immunotherapy. Clinical Cancer Research 2011;17:4550–7. 10.1158/1078-0432.CCR-11-0116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Rohaan MW, Borch TH, van den Berg JH, et al. Tumor-infiltrating lymphocyte therapy or Ipilimumab in advanced Melanoma. N Engl J Med 2022;387:2113–25. 10.1056/NEJMoa2210233 [DOI] [PubMed] [Google Scholar]
- 14. The European Parliament and the Council of the European Union . Regulation (EC) no 1394/2007 of the European Parliament and of the Council. The Official Journal of the European Union 2007:121–38. [Google Scholar]
- 15. Retèl VP, Steuten LMG, Geukes Foppen MH, et al. Early cost-effectiveness of tumor infiltrating lymphocytes (TIL) for second line treatment in advanced melanoma: a model-based economic evaluation 14 economics 1402 applied economics. BMC Cancer 2018;18:895. 10.1186/s12885-018-4788-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Lindenberg MA, Retèl VP, van den Berg JH, et al. Treatment with tumor-infiltrating lymphocytes in advanced Melanoma: evaluation of early clinical implementation of an advanced therapy medicinal product. J Immunother 2018;41:413–25. 10.1097/CJI.0000000000000245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Lindenberg M, Retèl V, Rohaan M, et al. Evaluating different adoption scenarios for TIL-therapy and the influence on its (early) cost-effectiveness. BMC Cancer 2020;20:712. 10.1186/s12885-020-07166-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Dutch National Healthcare Institute (ZIN) . Dutch National Healthcare Institute (ZIN) Voorwaardelijke toelating behandeling met tumor infiltrerende lymfocyten (TIL) bij uitgezaaid melanoom irresectabel stadium IIIc en stadium IV, Available: https://www.zorginstituutnederland.nl/werkagenda/kanker/voorwaardelijke-toelating-behandeling-met-tumor-infiltrerende-lymfocyten-til-van-uitgezaaid-melanoom-irresectabel-stadium-iiic-en-stadium-iv [Accessed 5 May 2022].
- 19. (FMS)" FMS . Melanoma - adjuvant systemic Tretamnet after Inital treatment [in Dutch]. 2019.
- 20. Keilholz U, Ascierto PA, Dummer R, et al. ESMO consensus conference recommendations on the management of metastatic melanoma: under the auspices of the ESMO guidelines committee. Ann Oncol 2020;31:1435–48. 10.1016/j.annonc.2020.07.004 [DOI] [PubMed] [Google Scholar]
- 21. Dansk Melanom Gruppe . Onkologisk Behandling Af Inoperabel Metastatisk Melanom. 2020. Available: https://www.melanoma.dk/assets/files/Melanoma_Guidelines_Onkologisk_behandling_af_inoperabel_metastatisk_melanom.pdf
- 22. Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making 2013;33:743–54. 10.1177/0272989X12472398 [DOI] [PubMed] [Google Scholar]
- 23. Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation.2nd edn. Oxford University Press, 2006. 10.1093/oso/9780198526629.001.0001 [DOI] [Google Scholar]
- 24. M. Versteegh M, M. Vermeulen K, M. A. A. Evers S, et al. Dutch tariff for the five-level version of EQ-5D. Value in Health 2016;19:343–52. 10.1016/j.jval.2016.01.003 [DOI] [PubMed] [Google Scholar]
- 25. Jensen CE, Sørensen SS, Gudex C, et al. The Danish EQ-5D-5L value set: a hybrid model using cTTO and DCE data. Appl Health Econ Health Policy 2021;19:579–91. 10.1007/s40258-021-00639-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Dutch National Health Care Institute . Package advice Dabrafenib/Trametinib [in Dutch]. Ref: 2020021411. 2020.
- 27. Dutch National Health Care Institute . Package advice ipilimumab/nivolumab [in Dutch]. 2021: 117. [Google Scholar]
- 28. Dutch National Health Care Institute . Package advice pembrolizumab [in Dutch]. 2016: 125. [Google Scholar]
- 29. Dutch National Health Care Institute . Farmacotherapeutisch Kompas [in Dutch], Available: https://www.farmacotherapeutischkompas.nl/
- 30. Arjmand MD M MM, Ellis M, Hillegeist SA, et al. Cost allocation can be as simple as A-B-C. Physician Leadersh J 2018;5:34–8. [Google Scholar]
- 31. Ten Ham RMT, Hövels AM, Hoekman J, et al. What does cell therapy manufacturing cost? A framework and methodology to facilitate academic and other small-scale cell therapy manufacturing costings. Cytotherapy 2020;22:388–97. 10.1016/j.jcyt.2020.03.432 [DOI] [PubMed] [Google Scholar]
- 32. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med 2019;381:1535–46. 10.1056/NEJMoa1910836 [DOI] [PubMed] [Google Scholar]
- 33. Garrison LP, Mansley EC, Abbott TA, et al. Good research practices for measuring drug costs in cost-effectiveness analyses: a societal perspective: the ISPOR drug cost task force report - part II. Value Health 2010;13:8–13. 10.1111/j.1524-4733.2009.00660.x [DOI] [PubMed] [Google Scholar]
- 34. Hanly P, Ortega-Ortega M, Sharp L. Friction costs and the chain of vacancies problem: a novel vacancy Multiplier solution. Value Health 2021;24:548–55. 10.1016/j.jval.2020.10.026 [DOI] [PubMed] [Google Scholar]
- 35. Hardin JW, Hilbe JM. Generalized estimating equations.2nd edn. Chapman & Hall/CRC, 2003. 10.1201/9781420035285 [DOI] [Google Scholar]
- 36. Liang K-Y, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika 1986;73:13–22. 10.1093/biomet/73.1.13 [DOI] [Google Scholar]
- 37. He Y. Missing data analysis using multiple imputation: getting to the heart of the matter. Circ Cardiovasc Qual Outcomes 2010;3:98–105. 10.1161/CIRCOUTCOMES.109.875658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Tan SS, Bouwmans CAM, Rutten FFH, et al. Update of the Dutch manual for costing in economic evaluations. Int J Technol Assess Health Care 2012;28:152–8. 10.1017/S0266462312000062 [DOI] [PubMed] [Google Scholar]
- 39. Williams AO, Rojanasarot S, McGovern AM, et al. A systematic review of discounting in national health economic evaluation guidelines: Healthcare value implications. J Comp Eff Res 2023;12:e220167. 10.2217/cer-2022-0167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Hatswell AJ, Pennington B, Pericleous L, et al. Patient-reported utilities in advanced or metastatic melanoma, including analysis of utilities by time to death. Health Qual Life Outcomes 2014;12:140. 10.1186/s12955-014-0140-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Medicinrådet . The Danish Medicines Council methods guide for assessing new pharmaceuticals. 2021. [Google Scholar]
- 42. Jochems A, Leeneman B, Franken MG, et al. Real-world use, safety, and survival of Ipilimumab in metastatic cutaneous Melanoma in the Netherlands. Anticancer Drugs 2018;29:572–8. 10.1097/CAD.0000000000000629 [DOI] [PubMed] [Google Scholar]
- 43. United States National Library of Medicine . Phase 3 study of nivolumab or nivolumab plus ipilimumab versus ipilimumab alone in previously untreated advanced melanoma (CheckMate 067;NCT01844505), Available: https://classic.clinicaltrials.gov/ct2/show/NCT01844505 [Accessed 25 Aug 2023].
- 44. Dutch Healthcare Authority (NZa) . NZa tarieven via NZa zorgproducten applicatie [Dutch]. 2023. [Google Scholar]
- 45. Wittrup-Jensen KU, Lauridsen J, Gudex C, et al. Generation of a Danish TTO value set for EQ-5D health States. Scand J Public Health 2009;37:459–66. 10.1177/1403494809105287 [DOI] [PubMed] [Google Scholar]
- 46. Dutch National Health Care Institute. . Pakketadvies Ipilimumab (Yervoy®) in Combinatie met Nivolumab (Opdivo®) Voor de Behandeling Van Asbestkanker. 2021. [Google Scholar]
- 47. Dutch National Health Care Institute. . Dabrafenib/trametinib (Tafinlar®/Mekinist®) for the adjuvant treatment of adult patients with stage III melanoma. 2019. [Google Scholar]
- 48. Dutch National Health Care Institute. . Farmaco-Economisch rapport voor pembrolizumab (Keytruda®) bij de behandeling van gevorderd NSCLC met PD-L1 expressie. 2016. [Google Scholar]
- 49. Gregory F G, Erqi L P, Volker W S, et al. Tumor treating fields and maintenance temozolomide for newly-diagnosed glioblastoma: a cost-effectiveness study. J Med Econ 2019:1006–13. 10.1080/13696998.2019.1614933 [DOI] [PubMed] [Google Scholar]
- 50. Dutch National Health Care Institute . Package advice vemurafenib (Zelboraf(R)) [In Dutch]. 2014. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
jitc-2023-008372supp001.pdf (4.2MB, pdf)
Data Availability Statement
Data are available upon reasonable request.