

Abstract
BACKGROUND:
Women require follow-up care and ongoing counseling after childbirth. The present study aimed to evaluate the effect of in-home supportive counseling on the maternal functioning and self-efficacy after CS among primiparous women.
MATERIALS AND METHODS:
This randomized controlled clinical trial was performed on 60 primiparous women aged 18–35 years following CS in Ardabil, Iran from April to November 2021. After convenience sampling, participants were randomly assigned into the intervention and control groups with a ratio of 1:1 by block randomization using Random Allocation Software with block sizes of 4 and 6. The intervention group received in-home supportive counseling during three sessions on days 3, 7, and one month after birth. The control group received only routine postpartum care. The data were collected using the demographic and obstetric characteristics, maternal self-efficacy questionnaire, and Barkin index of maternal functioning, completed by both groups 10–15 days, two, and four months after birth. Independent t-test and RMANOVA were used to analyze the data.
RESULTS:
The mean score of maternal functioning in the intervention group was significantly higher than that of the control group 10–15 days, 2 and 4 months after birth (AMD: 28.51, 95% CI: 24.91 to 32.10, P < 0.001). There was no significant difference in the mean (SD) score of maternal self-efficacy between the two groups 10–15 days after birth. However, this difference was statistically significant 2 and 4 months after birth and after adjusting the time effect (AMD: 10.56, 95% CI: 9.46 to 11.67, P < 0.001).
CONCLUSION:
In-home supportive counseling can be effective in improving maternal functioning and maternal self-efficacy after CS. Acquiring functional skills increases mothers’ self-confidence and self-efficacy in caring for the newborn.
Keywords: Counseling, maternal behavior, postnatal care, self-efficacy
Introduction
The postpartum period is influenced by changes in the personal relationships, social roles, and how to adapt to these changes, which significantly affect the mother’s health and child’s growth.[1] The functional status during the postpartum period is a multidimensional concept, encompassing personal care, infant care, family care, and social activities. A return to the prepregnancy functional status is achieved when a woman takes on the responsibilities of her maternal role and reorganizes her life by accepting the baby and fulfilling her responsibilities.[2]
Some factors that may affect the functional status of mothers in the postpartum period include the number of previous deliveries, perceived social support, type of delivery, maternal-neonatal complications, and fatigue.[3] Maternal self-efficacy is regarded as another factor affecting functional status.[4] Maternal self-efficacy refers to the mother’s belief in her own ability to be an effective and efficient mother, strongly influenced by maternal sense and the level of mother’s self-confidence and understanding of her competence.[5]
The prevalence of CS is about 48% in Iran.[6] Some complications, such as pain, weakness, disability, recovery period, and physical complications are more common in CS compared with vaginal delivery.[7,8] Mothers undergoing CS are discharged from the hospital 24–48 h after the surgery and spend the first days and weeks of motherhood without close support of health care providers.[9] Thus, the continuation of in-home support and care and the use of appropriate counseling approaches are necessary for the period after CS to adapt to new conditions for optimal maternal functioning, especially in primiparous mothers.[10] In this regard, in-home supportive counseling was used to acquire care skills and adapt to new condition by primiparous mothers after CS.
Supportive counseling uses direct measures to alleviate symptoms, restore or improve self-esteem, and acquire adaptive skills[11] and aims to strengthen women’s ability to cope with stress. In this approach, the counselor listens carefully to clients, encourages them to express their thoughts and feelings, and helps them to restore their self-confidence.[12] In the literature review, no study was found that uses the postpartum supportive counseling approach to improve maternal self-efficacy and functioning.
According to the needs assessment, women require follow-up care and ongoing counseling after childbirth.[13,14,15,16,17] Many primiparous women declare that they discharge from the hospital before having opportunity to talk about their worries.[18] Although postpartum home visit is common in the most developed countries, it is not considered as a routine program in developing countries, like Iran. Therefore, the present study aimed to determine the effect of in-home supportive counseling on maternal functioning and self-efficacy following CS among primiparous women.
Materials and Methods
Study design and setting
This randomized controlled clinical trial was conducted on postpartum women who gave birth in Alavi educational and treatment hospital in Ardabil from April to November 2021.
Study participants and sampling
The inclusion criteria were primiparous women undergoing emergency CS, aged 18–35 years, term singleton birth with gestational age over 37 weeks with birth weight more than 2,500 g. The exclusion criteria included having systemic disease or exacerbated disorders during pregnancy, such as overt or gestational diabetes, hypertensive disorders, heart disease, the hospitalized neonate, the mother’s inability to care for the baby, a history of depression according to the medical record, cases of abnormalities, death of the baby, and unplanned pregnancy.
The sample size was calculated using G-Power software. According to the study of Barkin et al.[19] and based on the variable of maternal functioning, by considering m1 = 80, with the default increase of 25% in the mean score of maternal functioning due to the intervention (m2 = 100), sd1 = sd2 = 17, power = 80%, and two-sided testing, a sample size of 13 was obtained per group. Furthermore, according to the study of Chamgordani et al.[20] and based on the maternal self-efficacy variable and regarding m1 = 33.6, m2 = 35.6, sd1 = 3.2, sd2 = 2.9, power = 80% and one-sided testing, sample size was estimated 30 in each group. Therefore, the final sample size was considered 30 by taking into account the larger sample size.
After registering the study in the clinical trial site (IRCT20170506033834N6, registration date: 10.08.2021), Convenience sampling was done at Alavi educational and treatment hospital in Ardabil. The researcher (first author) attended the selected hospital, identified the eligible mothers, and after explaining the objectives and method of the study, invited individuals who had desire to take part in the study. Then, they were evaluated in terms of the inclusion and the exclusion criteria. After obtaining the written informed consent form and completing the demographic and obstetrics characteristics, participants were randomly assigned into the intervention and control groups with a ratio of 1:1 by block randomization using Random Allocation Software with block sizes of 4 and 6. The allocation type was written on paper and placed in opaque envelopes numbered in consecutive order for the allocation concealment. The envelopes were opened sequentially by a noninvolved person in the sampling. The outcome assessor (the sixth author) was blinded.
Data collection tools and technique
Demographic and obstetric characteristics questionnaire
The demographic and obstetric characteristics included the variables of age, level of education, occupation, family income level, gender of neonate, type of pregnancy, etc.
Barkin Index of Maternal functioning (BIMF)
The tool was developed by Barkin et al.[2] to evaluate postpartum maternal functioning. The BIMF consists of 20 items addressing 7 domains, including self-care (items 2, 11, 13), infant care (items 12 and 14), mother-child interaction (items 4, 5, and 15), maternal psychological well-being (items 1, 2, 3, 5, 7, 10, 11, 16, 18, and 20), social support (items 6, 8, and 9), management (items 7, 11, 13, 14 and 18), and adjustment (items 17 and 19). Each item is scored between 0 and 6 and the total score ranges from 0 to 120. A higher score indicates better maternal functioning. The Cronbach’s alpha coefficient and Intra Class Correlation Coefficient (ICC) of the instrument in the study of Chamgordani et al.[20] were reported 0.88 and 0.85, respectively.
Maternal Self-Efficacy Questionnaire (MSQ)
The developed questionnaire by Teti and Gelfand was used to measure maternal self-efficacy, focusing more on the mother’s tasks in caring for her baby. This tool consists of 10-item, 9 of which are related to mother’s activity and one is a general item. The responses are scored based on a 4-point Likert scale (1 = worse than others, 2 = relatively worse than others, 3 = as good as the others, 4 = better than others), and the higher score represents the higher maternal self-efficacy.[21] The Cronbach’s alpha coefficient and ICC of the instrument in the Persian version were 0.82 and 0.89, respectively.[22]
Intervention
The researcher attended the hospital the day after the CS and after introductory session, trained postpartum care for both intervention and control groups. Then, the intervention group received in-home supportive counseling during three sessions on days 3 and 7 after delivery and one month after birth for 45–60 min. The timing of consultation was determined in coordination with the participants. Based on the supportive counseling strategies, including alliance between the counselor and the client (empathy), accepting the client’s perception and supporting her in expressing feelings, meeting needs and resolving ambiguities, establishing a relationship between the client’s condition and behaviors, strengthening and promoting social support, strengthening positive thoughts and helping the client to find a solution,[11,23] the content of the in-home counseling sessions was as follows:
First session: (3 days after birth): The session included encouraging clients to talk about the questions and problems experienced during their self-care and baby care, training breastfeeding, and talking about maternal nutrition, breast hygiene, CS wound care, pain management, and caring for neonate’s umbilical cord.
Second session (7 days after birth): Some issues, such as mother-neonate interaction, reasons for the baby crying, adjustment of sleep and wake time with the infant, perceived social support, and adjustment to responsibilities were discussed. This session generally aimed to look for functional disturbance, symptoms, like stress, and incorrect adaptive skills for explaining how to deal with them using training relaxation techniques, seeking and attracting social support, developing communication skills for relationships with others, especially the infant and spouse.
Third session (one month after birth):The overall purpose of this session was to examine the physical and psychological symptoms experienced by the woman. Furthermore, the postpartum resumption of sexual activity and contraceptive methods were discussed and acquired adaptive skills were summarized.
In terms of ethical considerations, consultant (first author) attended the client’s home by submitting a letter of introduction from health deputy of Ardabil University of Medical Sciences, and she commuted by an agency which was responsible for waiting and returning the consultant from clients’ homes.
In this study, the control group received only routine postpartum care. According to the national guideline,[24] the first postpartum care was in the hospital before discharge, and subsequent cares were in public health centers on days 10–15 and 42–60 after delivery.
The maternal functioning and maternal self-efficacy questionnaires were completed by both groups 10–15 days and 2 and 4 mo after birth, while referring to health centers for postpartum care and vaccination of the infant.
Ethical consideration
The study was approved by the ethics committee of Tabriz University of Medical Sciences, Iran (IR.TBZMED.REC.1399.781). The study complies with the World Medical Association Helsinki Declaration regarding the ethical conduct of research involving human subjects. The study protocol was developed following the Consort guidelines for clinical trials and included a completed CONSORT checklist. Written informed consent was obtained from each individual participant. The principles of anonymity and confidentiality were applied, and the participants were provided with the results upon their request.
Data analysis
The data were analyzed using SPSS24 software. The Kolmogorov–Smirnov test was employed to determine the normality of data distribution and independent t-test and RMANOVA were applied to compare the maternal functioning and maternal self-efficiency scores during 10–15 days, 2 and 4 mo after birth.
Results
The present study was conducted from April to July 2021 and followed to November 2021. Among 100 primiparous women undergoing CS, 60 were eligible and were randomly assigned to two groups. There was no loss to follow-up during the study and the data of all participants were analyzed [Figure 1].
Figure 1.
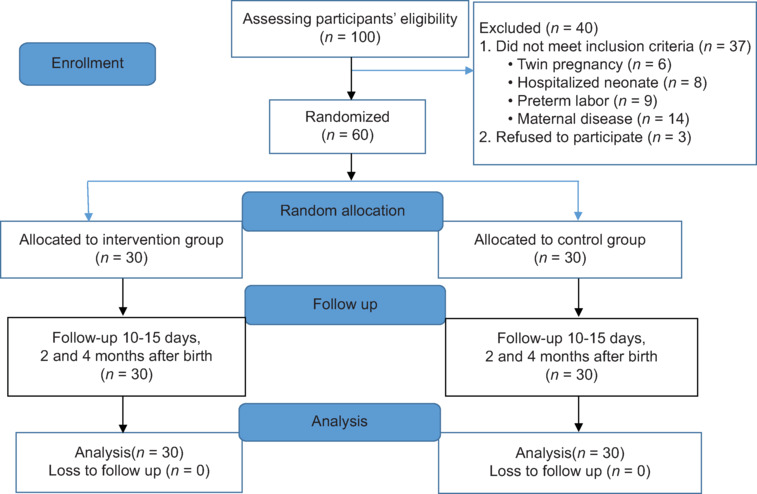
Flowchart of the study
The mean (SD) of age was 24.20 (4.90) years in the intervention group and 26.13 (5.46) in the control group (P = 0.15). The majority of participants in both groups (100% in the intervention group and 96.7% in the control group) were housekeeper. About 50% of women in the intervention group and 40% in the control group had diploma. Most of women in both groups had moderate economic status. Gender of 50% of infants in the intervention group and 60% in the control group was female. In general, there was no statistically significant difference between the demographic and obstetric characteristics of the intervention and control groups [Table 1].
Table 1.
The demographic and obstetric characteristics of the participants
| Variable | Intervention group (n=30) n (%) | Control group (n=30) n (%) | P |
|---|---|---|---|
| Age (years)† | 24.20 (4.90) | 26.13 (5.46) | *0.15 |
| Occupation | |||
| Housekeeper | 30 (100) | 29 (96.7) | **1.00 |
| Employed | 0 | 1 (3.3) | |
| Level of Education | |||
| Illiterate | 0 | 1 (3.3) | ***0.91 |
| Elementary/guidance | 10 (33.3) | 13 (43.3) | |
| High school/diploma | 15 (50) | 12 (40) | |
| Academic | 5 (16.7) | 4 (13.3) | |
| Household income level | |||
| Inadequate/Not enough | 5 (16.7) | 6 (20) | ***0.52 |
| Somewhat enough | 24 (80) | 21 (70) | |
| Enough | 1 (3.3) | 3 (10) | |
| Housing status | |||
| Private | 22 (73.3) | 22 (73.3) | **1.00 |
| Rental | 8 (26.7) | 8 (26.7) | |
| Type of delivery | |||
| Emergency cesarean section | 30 (100) | 30 (100) | **1.00 |
| Elective cesarean section | 0 | 0 | |
| Gender of the baby | |||
| Female | 15 (50) | 18 (60) | **0.43 |
| Male | 15 (50) | 12 (40) | |
| History of infertility | |||
| Yes | 2 (6.7) | 5 (16.7) | **0.42 |
| No | 28 (93.3) | 25 (83.3) |
†Mean (Standard deviation); *Independent t-test; **Fisher’s exact test; *** Trend Chi-square
The total mean (SD) score of maternal functioning 10–15 days after birth was 102.16 (5.06) in the intervention group and 78.70 (9.18) in the control group (P < 0.001). Two months after delivery, the total mean (SD) score of maternal functioning was 105.56 (2.80) in the intervention group and 77.26 (11.14) in the control group. Four months after delivery and after adjusting the time effect, the total mean score of maternal functioning in the intervention group was significantly higher than that in the control group (MD: 28.51, 95% CI = 24.91 to 32.10, P < 0.001). A significant difference was observed between the two groups in all seven domains of maternal functioning [Table 2].
Table 2.
The comparison of maternal functioning and its subdomains in the intervention and control groups
| Variables | Counseling (n=30) (SD) Mean | Control (n=30) (SD) Mean | P | Adjusted mean difference confidence interval) 95%) |
|---|---|---|---|---|
| Total score of Barkin Index of Maternal functioning (0-120) | ||||
| 10-15 days after birth | 102.16 (5.06) | 78.70 (9.18) | <0.001* | - |
| Two months after birth | 105.56 (2.80) | 77.26 (11.14) | - | |
| Four months after birth | 107.26 (1.76) | 73.50 (10.93) | <0.001** | 28.51 (24.91-32.10) |
| Self-care (0-18) | ||||
| 10-15 days after birth | 16.16 (1.36) | 9.80 (2.74) | <0.001* | - |
| Two months after birth | 17.20 (0.88) | 10.16 (2.74) | - | |
| Four months after birth | 17.63 (0.76) | 9.90 (2.25) | <0.001** | 7.04 (6.14-7.94) |
| Infant care (0-12) | ||||
| 10-15 days after birth | 11.93 (0.25) | 9.90 (1.44) | <0.001* | - |
| Two months after birth | 12 (0.21) | 9.96 (1.60) | - | |
| Four months after birth | 12 (0.21) | 9.86 (1.81) | <0.001** | 2.06 (1.51-2.62) |
| Mother-child interaction (0-18) | ||||
| 10-15 days after birth | 15.76 (1.33) | 10.60 (2.35) | <0.001* | - |
| Two months after birth | 17.36 (0.88) | 11.16 (2.60) | - | |
| Four months after birth | 17.90 (0.40) | 10.76 (2.31) | <0.001** | 6.16 (5.33-6.99) |
| Maternal psychological well-being (0-60) | ||||
| 10-15 days after birth | 47.50 (2.89) | 37.10 (5.25) | <0.001* | - |
| Two months after birth | 48.50 (1.71) | 37.23 (5.93) | - | |
| Four months after birth | 48.60 (1.22) | 36.26 (5.65) | <0.001** | 11.33 (9.37-13.29) |
| Social support (0-18) | ||||
| 10-15 days after birth | 15.83 (1.93) | 12.60 (3.26) | <0.001* | - |
| Two months after birth | 15.96 (1.56) | 9.93 (3.53) | - | |
| Four months after birth | 16.90 (0.99) | 7.90 (3.18) | <0.001** | 6.08 (4.91-7.26) |
| Management (0-36) | ||||
| 10-15 days after birth | 23.53 (1.65) | 18.90 (3.63) | <0.001* | - |
| Two months after birth | 23.73 (1.33) | 18.16 (3.24) | - | |
| Four months after birth | 24.03 (0.96) | 17.06 (2.91) | <0.001** | 5.72 (4.54-6.89) |
| Adjustment (0-12) | ||||
| 10-15 days after birth | 11.13 (0.68) | 8.33 (1.51) | <0.001* | - |
| Two months after birth | 11.83 (0.37) | 8.93 (1.38) | - | |
| Four months after birth | 11.96 (0.18) | 8.76 (1.52) | <0.001** | 2.96 (2.52-3.40) |
*Independent t-test, **RMANOVA
The total mean (SD) score of maternal self-efficacy 10–15 days after delivery was 25.06 (1.38) in the intervention group and 26.23 (2.90) in the control group (P = 0.9). Two months after delivery, the total mean (SD) score of maternal self-efficacy in the intervention and control groups was 38.10 (1.42) and 27.40 (3.43), respectively. Furthermore, the total mean (SD) score of maternal self-efficacy 4 mo after delivery was 37.57 (0.81) in the intervention group and 27.011 (3.37) in the control group. Following the control of time effect, the total mean score of maternal self-efficacy in the intervention group was significantly higher than that in the control group (MD: 10.56, 95%CI: 9.46 to 11.67, P < 0.001) [Table 3].
Table 3.
The comparison of maternal self-efficacy in the intervention and control groups
| Variables | Intervention Group n=30 Mean (SD) | Control group n=30 Mean (SD) | AMD (95% CI)† | P |
|---|---|---|---|---|
| 10-15 days after birth | 25.06 (1.38) | 26.23 (2.90) | - | 0.9* |
| Two months after birth | 38.10 (1.42) | 27.40 (3.43) | - | |
| Four months after birth | 37.57 (0.81) | 27.011 (3.37) | 10.56 (9.46-11.67) | <0.001** |
†Adjusted Mean difference) 95% Confidence interval); *Independent t-test; ** RMANOVA
Discussion
This was the first Iranian study investigated the effect of in-home supportive counseling on the maternal functioning and self-efficacy of primiparous mothers after CS. The results indicated a significant increase in the maternal functioning in the intervention group compared with the control group.
In line with the findings of the present study, Chamgordani et al.[20] reported that the maternal functioning in the intervention group was significantly higher than that in the control group, after 4-session of counseling with skill training approach starting from the third week after vaginal delivery or CS. In addition, in a study by Bagherinia et al.,[25] the training package, including face-to-face, telephone, and booklet, had a positive effect on postpartum self-confidence and maternal functional status six weeks after intervention. In another study, Kordi et al.[26] revealed that maternal role training among nulliparous women with unplanned pregnancy during pregnancy and after birth led to increased maternal competence.
However, in a study conducted by Bashour et al.[27] on primiparous mothers in Syria, there was no significant difference in maternal and neonatal outcomes between groups receiving four sessions of home visits, one session of home visits, and no home visits as control group. In other study in Istanbul, antenatal education did not improve postpartum functional status, which may be due to the difference in the type and time of interventions.[28]
The findings of the present study indicated that following in-home supportive counseling, maternal self-efficacy was not significant between the two groups 10–15 days after childbirth.
However, maternal self-efficacy significantly increased in the intervention group compared with the control group 2 and 4 mo after birth. Although a significant increase was observed in the maternal functioning of the intervention group 10–15 days after delivery, there was still no significant difference in the maternal self-efficacy between the two groups. Considering the relationship between maternal self-efficacy and maternal functioning following childbirth in previous studies, which provided the basis for suggesting interventions to improve maternal self-efficacy for enhancing their functioning in the postpartum period,[29,30,31] the findings of the present study demonstrated that gaining functional skills in mothers lead to improved self-confidence and self-efficacy in caring for the baby over time.
In line with the results of the present study about maternal self-efficacy, Chaves & Ximenes reported that following three-session of motivational phone counseling after birth, maternal self-efficacy significantly improved 4 mo after delivery.[32] Furthermore, Perez-Blasco et al.[33] indicated a significant increase in the maternal self-efficacy of postpartum mothers after 8 sessions of mindfulness-based counseling. In another study, after postpartum home visit and phone call follow up, a significant increase was observed in the maternal self-efficacy of primiparous mothers.[34] Moreover, in a study by Fasanghari et al.,[35] a maternal role training program based on Mercer theory during pregnancy and after birth increased maternal self-confidence in primiparous women with unplanned pregnancy. In another study, prenatal education based on the health belief model enhanced improved self-efficacy in primiparous women.[36]
However, the results of a study conducted by Jaafarnejad et al.[37] showed that infant care training package based on Bandura’s self-efficacy theory did not affect maternal self-confidence of primiparous women, which may be due to the difference in the content of intervention, and maternal self-confidence measurement tool. In that study, maternal self-confidence was measured by Lips questionnaire. Furthermore, Salonen et al.[38] examined the effect of online educational intervention on maternal self-efficacy. The women in the intervention group had access to an educational site with infant care training from 21st week of pregnancy and the control group received only the routine antenatal care. The results revealed no significant difference in the maternal self-efficacy between two groups six to eight weeks after birth, which was not consistent with the results of the present study. The reason for the discrepancy between the findings was related to the time of intervention and the study population. On the other hand, some of the women in the intervention group used the Internet to a small extent, and probably the internet nature of the intervention influenced the outcome.
Limitations and recommendation
The limitations of this study were small sample size and self-reported data. Furthermore, it was not possible to blind the participants, due to the nature of the study.
It is recommended to use in-home supportive counseling approach in primiparous mothers underwent CS, and it is suggested to assess the effect of in-home supportive counseling on the mental health and neonatal outcomes following CS in the future studies.
Conclusion
The in-home supportive counseling provides a valuable opportunity for mothers to express their concerns and stresses along with acquiring care skills, leading to the improvement of maternal functioning and maternal self-efficacy in the postpartum period. The findings of this study demonstrated that the acquisition of functional skills in mothers leads to increased self-confidence and improved self-efficacy in caring for the baby over time.
Financial support and sponsorship
Research deputy of Tabriz University of Medical sciences financed this work (grant ID: IR.TBZMED.REC.1399.781).
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
This is a report of database from MSc thesis registered in Tabriz University of Medical sciences with ID: IR.TBZMED.REC.1399.781. The cooperation of the Research Deputy and the officials and staff of Tabriz and Ardabil University of Medical sciences, as well as all women who participated in the study, is gratefully acknowledged.
References
- 1.Bahari S, Nourizadeh R, Esmailpour K, Hakimi S. The Effect of supportive counseling on mother psychological reactions and mother-infant bonding following traumatic childbirth. Issues Ment Health Nurs. 2022;43:447–54. doi: 10.1080/01612840.2021.1993388. [DOI] [PubMed] [Google Scholar]
- 2.Barkin JL, Wisner KL, Bromberger JT, Beach SR, Terry MA, Wisniewski SR. Development of the Barkin index of maternal functioning. J Womens Health (Larchmt) 2010;19:2239–46. doi: 10.1089/jwh.2009.1893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rychnovsky JD. Postpartum fatigue in the active-duty military woman. J Obstet Gynecol Neonatal Nurs. 2007;36:38–46. doi: 10.1111/j.1552-6909.2006.00112.x. [DOI] [PubMed] [Google Scholar]
- 4.Fathi F, Mohammad-Alizadeh-Charandabi S, Mirghafourvand M. Maternal self-efficacy, postpartum depression, and their relationship with functional status in Iranian mothers. Women Health. 2018;58:188–203. doi: 10.1080/03630242.2017.1292340. [DOI] [PubMed] [Google Scholar]
- 5.Azmoude E, Jafarnejade F, Mazlom SR. The predictors for maternal self-efficacy in early parenthood. J Midwifery Reprod Health. 2015;3:368–76. [Google Scholar]
- 6.Rafiei M, Saei Ghare M, Akbari M, Kiani F, Sayehmiri F, Sayehmiri K, et al. Prevalence, causes, and complications of cesarean delivery in Iran: A systematic review and meta-analysis. Int J Reprod Bio Med. 2018;16:221–34. [PMC free article] [PubMed] [Google Scholar]
- 7.Jansen AJ, Duvekot JJ, Hop WC, Essink-Bot ML, Beckers EA, Karsdorp VH, et al. New insights intofatigue and health-related quality of life after delivery. Acta Obstet Gynecol Scand. 2007;86:579–84. doi: 10.1080/00016340701275424. [DOI] [PubMed] [Google Scholar]
- 8.Ahmad-Nia S, Delavar B, Eini-Zinab H, Kazemipour S, Mehryar AH, Naghavi M. Caesarean section in the Islamic Republic of Iran: Prevalence and some sociodemographic correlates. East Mediterr Health J. 2009;15:1389–98. [PubMed] [Google Scholar]
- 9.Elmir R, Schmied V, Wilkes L, Jackson D. Women’s perceptions and experiences of a traumatic birth: A meta-ethnography. J Adv Nurs. 2010;66:2142–53. doi: 10.1111/j.1365-2648.2010.05391.x. [DOI] [PubMed] [Google Scholar]
- 10.Shaw RJ, St John N, Lilo EA, Jo B, Benitz W, Stevenson DK, et al. Prevention of traumatic stress in mothers with preterm infants: A randomized controlled trial. Pediatrics. 2013;132:e886–94. doi: 10.1542/peds.2013-1331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Winston A, Rosenthal RN, Pinsker H. American Psychiatric Publishing, Inc.; 2012. Learning Supportive Psychotherapy: An Illustrated Guide. Available from: https://psycnet.apa.org/record/2011-27479-000 . [Google Scholar]
- 12.Grover S, Avasthi A, Jagiwala M. Clinical practice guidelines for practice of supportive psychotherapy. Indian J Psychiatry. 2020;62:S173–82. doi: 10.4103/psychiatry.IndianJPsychiatry_768_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Almalik MM. Understanding maternal postpartum needs: A descriptive survey of current maternal health services. J Clin Nurs. 2017;26:4654–63. doi: 10.1111/jocn.13812. [DOI] [PubMed] [Google Scholar]
- 14.Madray C, Richardson J, Hornsby P, Grello C, Drake E, Kellams A. Exploring the unmet needs of postpartum mothers: A qualitative study. J Perinat Educ. 2022;31:71–81. doi: 10.1891/JPE-2021-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rotich E, Wolvaardt L. A descriptive study of the health information needs of Kenyan women in the first 6 weeks postpartum. BMC Pregnancy Childbirth. 2017;17:385. doi: 10.1186/s12884-017-1576-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Xiao X, Ngai FW, Zhu SN, Loke AY. The experiences of early postpartum Shenzhen mothers and their need for home visit services: A qualitative exploratory study. BMC Pregnancy Childbirth. 2019;20:5. doi: 10.1186/s12884-019-2686-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ong SF, Chan WC, Shorey S, Chong YS, Klainin-Yobas P, He HG. Postnatal experiences and support needs of first-time mothers in Singapore: A descriptive qualitative study. Midwifery. 2014;30:772–8. doi: 10.1016/j.midw.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 18.Park EJ. Telehealth technology in case/disease management. Lippincott’s Case Manag. 2006;11:175–82. doi: 10.1097/00129234-200605000-00010. [DOI] [PubMed] [Google Scholar]
- 19.Barkin JL, Willis GB, Hawkins KC, Stanfill-Thomas T, Beals L, Bloch JR. Semantic assessment of the Barkin index of maternal functioning in a medically underserved obstetric population. Perspect Psychiatr Care. 2017;53:95–103. doi: 10.1111/ppc.12141. [DOI] [PubMed] [Google Scholar]
- 20.Chamgordani FK, Barkin JL, Esmaeilpour K, Malakouti J, Buoli M, Mirghafourvand M. The effect of counseling with a skills training approach on maternal functioning: A randomized controlled clinical trial. BMC Womens Health. 2020;20:51. doi: 10.1186/s12905-020-00914-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Teti DM, Gelfand DM. Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child Dev. 1991;62:918–29. doi: 10.1111/j.1467-8624.1991.tb01580.x. [DOI] [PubMed] [Google Scholar]
- 22.Jamalivand S, Mirghafourvand M, Mohammad-Alizadeh Charandabi S. Comparison of the effects of educational software and training booklet on maternal self-efficacy and infant care behavior in Iranian mothers: A randomized controlled trial. Int J Pediatr. 2017;5:5923–34. [Google Scholar]
- 23.Buckley L, Maayan N, Soares-Weiser K. Supportive therapy for schizophrenia. Cochrane Database Syst Rev. 2015;4:CD004716. doi: 10.1002/14651858.CD004716.pub4. doi: 10.1002/14651858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Torkestani F, Abedini M, Radpouyan L, Rahimi Ghasbeh S, Hadipour Jahromi L, Bakhshandeh M, et al. 4th. Tehran: Iran Ministry of Health; 2017. National Guideline of Midwifery and Birth Services. [Google Scholar]
- 25.Bagherinia M, Mirghafourvand M, Shafaie FS. The effect of educational package on functional status and maternal self-confidence of primiparous women in postpartum period A randomized controlled clinical trial. J Matern Fetal Neonatal Med. 2017;30:2469–75. doi: 10.1080/14767058.2016.1253061. [DOI] [PubMed] [Google Scholar]
- 26.Kordi M, Fasanghari M, Asgharipour N, Esmaily H. The effect of maternal role training program on role attainment and maternal role satisfaction in nulliparous women with unplanned pregnancy. J Educ Health Promot. 2017;6:61. doi: 10.4103/jehp.jehp_113_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bashour HN, Kharouf MH, Abdulsalam AA, AsmarKh El, Tabba MA, Cheikha SA. Effect of postnatal home visits on maternal/infant outcomes in Syria: A randomized controlled trial. Public Health Nurs. 2008;25:115–25. doi: 10.1111/j.1525-1446.2008.00688.x. [DOI] [PubMed] [Google Scholar]
- 28.Gürkan ÖC, Ekşi Z. Effects of antenatal education program on postpartum functional status and depression. Clin Exp Neurol Sci. 2017;7:133–8. [Google Scholar]
- 29.Aktan NM. Functional status after childbirth and related concepts. Clin Nurs Res. 2010;19:165–80. doi: 10.1177/1054773810369372. [DOI] [PubMed] [Google Scholar]
- 30.Salarkia N, Omidvar N, Zaeri F, Zeinab HE, Neyestani TR. Mother’s self-efficacy mediates the relationship between household food insecurity and maternal Infant Feeding Styles. Matern Child Health J. 2016;20:602–12. doi: 10.1007/s10995-015-1859-y. [DOI] [PubMed] [Google Scholar]
- 31.Mirghafourvand M, Bagherinia M. Relationship between maternal self-efficacy and functional status four months after delivery in Iranian primiparous women. J Psychosom Obstet Gynaecol. 2018;39:321–8. doi: 10.1080/0167482X.2017.1394290. [DOI] [PubMed] [Google Scholar]
- 32.Chaves AFL, Ximenes LB, Rodrigues DP, Vasconcelos CTM, Monteiro JCDS, Oriá MOB. Telephone intervention in the promotion of self-efficacy, duration and exclusivity of breastfeeding: Randomized controlled trial. Rev Lat Am Enfermagem. 2019;27:e3140. doi: 10.1590/1518-8345.2777-3140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Perez-Blasco J, Viguer P, Rodrigo MF. Effects of a mindfulness-based intervention on psychological distress, well-being, and maternal self-efficacy in breast-feeding mothers: Results of a pilot study. Arch Womens Ment Health. 2013;16:227–36. doi: 10.1007/s00737-013-0337-z. [DOI] [PubMed] [Google Scholar]
- 34.Shorey S, Chan SW, Chong YS, He HG. A randomized controlled trial of the effectiveness of a postnatal psychoeducation programme on self-efficacy, social support and postnatal depression among primiparas. J Adv Nurs. 2015;71:1260–73. doi: 10.1111/jan.12590. [DOI] [PubMed] [Google Scholar]
- 35.Fasanghari M, Kordi M, Asgharipour N. Effect of maternal role training program based on Mercer theory on maternal self-confidence of primiparous women with unplanned pregnancy. J Educ Health Promot. 2019;8:4. doi: 10.4103/jehp.jehp_202_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kamran A, Shrifirad G, Mirkarimi SK, Farahani A. Effectiveness of breastfeeding education on the weight of child and self-efficacy of mothers-2011. J Educ Health Promot. 2012;1:11. doi: 10.4103/2277-9531.98569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Jaafarnejad F, Azmoude E, Mazlom SR, Reyhani T. The effect of self-efficacy training package on maternal self-confidence of primiparous women in infant care. Iran J Obstet Gynecol Infertil. 2014;17:18–28. [Google Scholar]
- 38.Salonen AH, Kaunonen M, Astedt-Kurki P, Jarvenpaa AL, Isoaho H, Tarkka MT. Effectiveness of an internet-based intervention enhancing finish parents’ parenting satisfaction and parenting self-efficacy during the postpartum period. Midwifery. 2011;27:832–41. doi: 10.1016/j.midw.2010.08.010. [DOI] [PubMed] [Google Scholar]