

Abstract
Background
The use of electric scooters (e-scooters) continues to increase as a simple, inexpensive means of transport, resulting in a sharp increase in the incidence of scooter-related accidents. No study to date has closely examined the injury extent to the lower leg, joints, and extremities from e-scooter-related accidents. Here, we investigated the epidemiology and injury patterns of such accidents, focusing on injuries to the ankle and foot.
Methods
Based on data from a single tertiary hospital’s database, the demographics of 563 patients with scooter-associated injuries were analyzed retrospectively. Among the patients, 229 patients who were injured by e-scooter riding were further investigated. Based on the data, the general demographics of whole scooter-associated injuries and the injury characteristics and fracture cases of the lower leg, ankle, and foot were analyzed.
Results
During the 4-year study period, the number of patients injured by e-scooters increased every year. Lower extremities were the most common injury site (67.2%) among riders, whereas injuries to the head and neck (64.3%) were more common in riders of non-electric scooters. Among the lower leg, ankle, and foot injuries of riders (52 cases), the ankle joint (53.8%) was the most commonly injured site, followed by the foot (40.4%) and lower leg (21.2%). The fracture group scored significantly higher on the Abbreviated Injury Scale than the non-fracture group (p < 0.001). Among the fracture group (20 cases), ankle fractures (9 cases) were most common, including pronation external rotation type 4 injuries (4 cases) and pilon fractures (2 cases). Five patients (25%) had open fractures, and 12 patients (60%) underwent surgical treatment.
Conclusions
The ankle and foot are the most common injury sites in e-scooter-related accidents. Given the high frequency and severity of e-scooter-related ankle and foot injuries, we suggest that more attention be paid to preventing these types of injuries with greater public awareness of the dangers of using e-scooters.
Keywords: Ankle fracture, Lower extremity, Ankle, Foot, Motorized scooter
Electric scooters (e-scooters) are single-person vehicles powered by electricity. Social interest in e-scooters has increased rapidly due to the accessibility they offer, faster mobility than walking, and the eco-friendliness of using electricity.1) As the number of e-scooter users has steadily increased, the incidence of related accidents has continued to rise. Hence, research on these accidents is also actively conducted. Although previous studies have examined scooter-associated injuries, the studies reported to date have focused on the general characteristics of injuries or comparison analyses regarding riders of e-scooters versus those of non-electric-scooters (NES).2,3,4,5,6,7) Recently, Kobayashi et al.8) analyzed 103 patients with e-scooter-associated accidents and reported that extremity fractures were most frequently observed (42%), with lower extremity fractures of the tibia and fibula being most frequent (30%). Our practice sees a considerable number of patients with injuries to the lower leg, ankle, and foot from e-scooter riding. In some cases, the injuries are severe and include fractures and ligament tears that require operative treatment. However, no study to date has closely examined the injury extent to the lower leg, joints, and extremities from e-scooter-related accidents.
In this study, we investigated the epidemiology and injury patterns of e-scooter injuries, focusing on the lower leg, ankle, and foot to better understand and draw awareness to the potential dangers associated with this mode of transport and the need for proper treatment and implementation of the appropriate safety measures.
METHODS
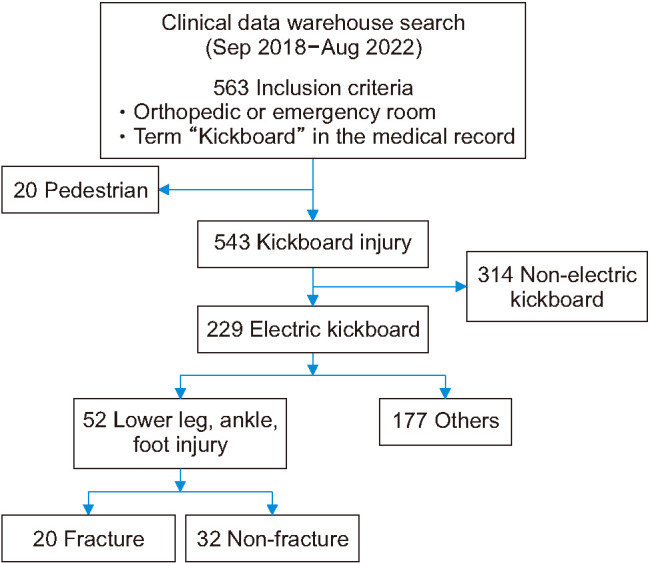
This study was approved by the Institutional Review Board of Konyang University Hospital (No. 2022-10-001). Written consent was not needed due to its retrospective nature. A retrospective analysis was performed based on data collected from the clinical data warehouse (CDW) of our single tertiary hospital from September 2018 to August 2022. The inclusion criteria were as follows: patients who visited an orthopedic outpatient clinic or emergency room and patients of whom the term “kickboard” was included in the electronic medical record (n = 563). In South Korea, the word for scooter is “kickboard”; thus, we searched all records containing this word. The annual number of accidents that occurred from the use of e-scooters and NES was analyzed, and the general demographic data of scooter-associated injuries were collected. Among them, pedestrian accident patients were excluded (n = 20). Among the cases of scooter riders (n = 543), e-scooter riders (n = 229) were further classified into patients with injuries of the lower leg, ankle, and foot (n = 52) and patients with injuries to other parts of the body (n = 177). The “lower leg” was defined as the part between the proximal tibia below the knee joint and the 1/3 of the distal tibia. The lower leg, ankle, and foot injury group was further divided into fracture (n = 20) and non-fracture (n = 32) groups (Fig. 1).
Fig. 1. Flow diagram of participant eligibility.
An investigator who was not involved in any of the clinical or operative treatments (JGC) retrospectively reviewed the electronic medical charts and evaluated all radiographic data. After investigating the general demographics of the scooter-associated injuries, lower leg, ankle, and foot injuries of e-scooter riders were evaluated in terms of sex, laterality, age, injury mechanism, and severity. Among the injury mechanisms, “car accidents” refer to the accidents in which e-scooter riders are hit by cars. For the criteria of injury severity, the Abbreviated Injury Scale (AIS) was used, with the following grades: grade 1, strains, lacerations, contusions, and simple sprains; grade 2, sprains of major joints and non-displaced fractures of long bones; grade 3, displaced fractures; grade 4, multiple closed fractures; grade 5, multiple open fractures; and grade 6, fracture leading to death.9) The patients were further divided into fracture and non-fracture groups, and we investigated whether there were significant differences between the 2 groups with respect to sex, injury site, age, injury mechanism, and severity. Each case of the fracture group was evaluated with respect to demographics, diagnosis, and treatment. Ankle fractures were classified using the Lauge-Hansen classification system and tibial fractures were classified using the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification.10,11) If the ankle joint presented with epiphysis, the Salter-Harris (S-H) classification was used.12)
Statistical Analysis
Statistical analyses were performed using IBM SPSS ver. 28.0 (IBM Corp.). The chi-square test or Fisher’s exact test was performed to analyze categorical data. Continuous data were compared between the 2 groups using Student t-test (parametric data) or the Mann-Whitney U-test (nonparametric data). For all analyses, a p-value of less than 0.05 was considered statistically significant.
RESULTS
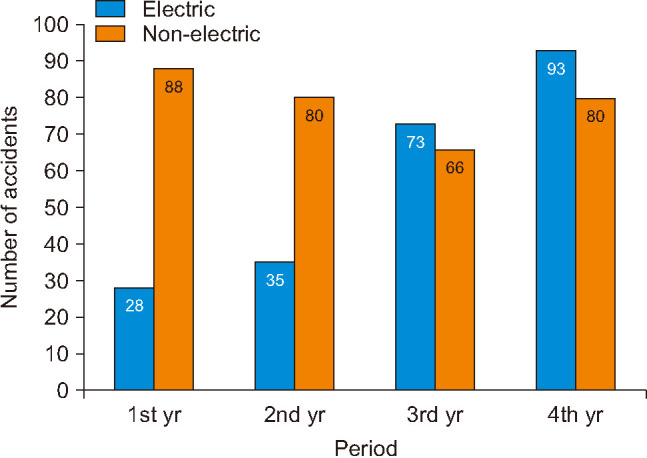
From September 2018 to August 2022, a total of 229 injury cases occurred due to e-scooter riding and the number of e-scooter-associated accidents increased each year over the 4-year study period (Fig. 2). Among the cases, 93 (40.6%) occurred in the last year of the study. During the first and second years, the frequency of NES injury was higher than that from an e-scooter; however, e-scooter injuries outpaced NES injuries in the third and fourth years.
Fig. 2. Frequency of electric and non-electric scooter-related injuries during the study period.
The general demographic data of scooter-associated injuries are shown in Table 1. In both e-scooter and NES patients, male patients were more common than female patients. The most common age groups of patients in the e-scooter and NES groups were those in their 20s and those under 10 years of age, respectively. The mean age of patients in the e-scooter group was significantly higher than that in the NES group (p < 0.001). The majority of patients in both groups initially visited the emergency room for treatment. The e-scooter group showed significantly more cases with multiple injuries (42.8%) compared to the NES group (15.6%) (p < 0.001). With respect to the injury site, lower extremity (67.2%) was the most common in the e-scooter group, and head and face (64.3%) were most frequently observed in the NES group. The lower extremity injuries were significantly more common in the e-scooter group than in the NES group (p < 0.001).
Table 1. Demographic Data on Scooter-Associated Injuries.
| Variable | Total (n = 543) | Electric (n = 229) | Non-electric (n = 314) | p-value | ||
|---|---|---|---|---|---|---|
| Sex | 0.335* | |||||
| Male | 343 (63.2) | 150 (65.5) | 193 (61.5) | |||
| Female | 200 (36.8) | 79 (34.5) | 121 (38.5) | |||
| Age (yr) | < 0.001†,‡ | |||||
| < 10 | 232 (42.7) | 5 (2.2) | 227 (72.3) | |||
| 10–19 | 105 (19.3) | 71 (31.0) | 34 (10.8) | |||
| 20–29 | 125 (23.0) | 100 (43.7) | 25 (8.0) | |||
| 30–39 | 40 (7.4) | 25 (10.9) | 15 (4.8) | |||
| 40–49 | 28 (5.2) | 16 (7) | 12 (3.8) | |||
| 50–59 | 7 (1.3) | 7 (3.1) | 0 | |||
| ≥ 60 | 6 (1.1) | 5 (2.2) | 1 (0.3) | |||
| Mean | 16.92 | 25.38 | 10.75 | |||
| Care unit | 0.098* | |||||
| Emergency room | 500 (92.1) | 216 (94.3) | 284 (90.4) | |||
| Orthopedic clinic | 43 (7.9) | 13 (5.7) | 30 (9.6) | |||
| Injury site | < 0.001*,‡ | |||||
| Single | 396 (72.9) | 131 (57.2) | 265 (84.4) | |||
| Multiple | 147 (27.1) | 98 (42.8) | 49 (15.6) | |||
| 2 | 89 (16.4) | 57 (24.9) | 32 (10.2) | |||
| 3 | 37 (6.8) | 27 (11.8) | 10 (3.2) | |||
| ≥ 4 | 21 (3.9) | 14 (6.1) | 7 (2.2) | |||
| Affected body part | ||||||
| Head and face | 333 (61.3) | 131 (57.2) | 202 (64.3) | 0.092* | ||
| Head | 91 (16.8) | 30 (13.1) | 61 (19.4) | |||
| Face and teeth | 242 (44.6) | 101 (44.1) | 141 (44.9) | |||
| Upper extremity | 225 (41.4) | 118 (51.5) | 107 (34.1) | < 0.001*,‡ | ||
| Shoulder | 34 (6.2) | 21 (9.2) | 13 (4.1) | |||
| Elbow | 64 (11.8) | 31 (13.5) | 33 (10.5) | |||
| Forearm and hand | 127 (23.4) | 66 (28.8) | 61 (19.4) | |||
| Lower extremity | 223 (41.1) | 154 (67.2) | 69 (22.0) | < 0.001*,‡ | ||
| Hip and pelvis | 34 (6.2) | 20 (8.7) | 14 (4.5) | |||
| Thigh | 8 (1.5) | 5 (2.1) | 3 (1.0) | |||
| Knee and lower leg | 121 (22.3) | 88 (38.4) | 33 (10.5) | |||
| Foot and ankle | 60 (11.0) | 41 (18.0) | 19 (6.1) | |||
| Others | 32 (5.9) | 19 (8.3) | 13 (4.1) | 0.042*,‡ | ||
| Vertebral column | 14 (2.6) | 8 (3.5) | 6 (1.9) | |||
| Abdomen and chest | 18 (3.3) | 11 (4.8) | 7 (2.2) | |||
Values are presented as number (%).
*Fisher’s exact test. †Student t-test. ‡Statistically significant values.
The characteristics of lower leg, ankle, and foot injury in e-scooter riders and their subgroups of fracture and non-fracture groups are shown in Table 2. The most common age group of patients was between 10 and 20 years of age (42.3%), followed by those in their 20s (34.6%). Slipdown injury (76.9%) was more common than car accidents (23.1%). Regarding injury severity by AIS, grade 1 injury (61.5%) was most frequently observed, followed by grade 3 injury (19.2%). The ankle joint was the most frequently injured site (53.8%), followed by foot (40.4%) and lower leg (21.2%) injuries. Among these patients, 20 patients (38.5%) had fracture injury. In a comparative study of fracture and non-fracture groups, sex, laterality, age, injury mechanism, and injury site revealed no significant difference between the 2 groups (p > 0.05). The fracture group exhibited significantly higher injury severity by AIS (grade 3: 50%; grade 4: 25%; and grade 5: 25%) than the non-fracture group (all grade 1) (p < 0.001). In terms of the injured part, the ankle joint was the most common site in both the fracture (45.0%) and non-fracture groups (59.4%).
Table 2. Comparison of Characteristics between Fracture Group and Non-fracture Group in the Lower Leg, Ankle, and Foot Injury Associated with Electric Scooter Riding.
| Variable | Total (n = 52) | Fracture group (n = 20) | Non-fracture group (n = 32) | p-value | |
|---|---|---|---|---|---|
| Sex | 0.890* | ||||
| Male | 29 (55.8) | 11 (55.0) | 18 (56.3) | ||
| Female | 23 (44.2) | 9 (45.0) | 14 (43.7) | ||
| Injury side | 0.680* | ||||
| Right | 17 (32.7) | 9 (45.0) | 8 (25.0) | ||
| Left | 29 (55.8) | 10 (50.0) | 19 (59.4) | ||
| Both | 6 (11.5) | 1 (5.0) | 5 (15.6) | ||
| Age (yr) | 0.178† | ||||
| < 10 | 0 | 0 | 0 | ||
| 10–19 | 22 (42.3) | 8 (40.0) | 14 (43.8) | ||
| 20–29 | 18 (34.6) | 6 (30.0) | 12 (37.5) | ||
| 30–39 | 7 (13.5) | 3 (15.0) | 4 (12.5) | ||
| 40–49 | 2 (3.8) | 1 (5.0) | 1 (3.1) | ||
| 50–59 | 0 | 0 | 0 | ||
| ≥ 60 | 3 (5.8) | 2 (10.0) | 1 (3.1) | ||
| Mean | 25.2 | 26.6 | 24.3 | ||
| Injury mechanism | 0.383* | ||||
| Slip down | 40 (76.9) | 16 (80.0) | 24 (75.0) | ||
| Car accident | 12 (23.1) | 4 (20.0) | 8 (25.0) | ||
| Abbreviated Injury Scale | < 0.001†,‡ | ||||
| 1 | 32 (61.5) | 0 | 32 (100.0) | ||
| 2 | 0 | 0 | 0 | ||
| 3 | 10 (19.2) | 10 (50.0) | 0 | ||
| 4 | 5 (9.6) | 5 (25.0) | 0 | ||
| 5 | 5 (9.6) | 5 (25.0) | 0 | ||
| Mean | 2.1 | 3.8 | 1 | ||
| Injury site | |||||
| Lower leg | 11 (21.2) | 6 (30.0) | 5 (15.6) | 0.299* | |
| Ankle | 28 (53.8) | 9 (45.0) | 19 (59.4) | 0.395* | |
| Foot | 21 (40.4) | 7 (35.0) | 14 (43.8) | 0.575* | |
Values are presented as number (%).
*Fisher’s exact test method. †Student t-test. ‡Statistically significant values.
The 20 fracture cases of the lower leg, ankle, and foot in e-scooter riders are shown in Table 3. Among the 20 cases, 9 cases had ankle fractures: 4 cases of pronation external rotation (PER) type 4 (Figs. 3 and 4), 1 case of supination external rotation type 4, 2 cases of AO/OTA 43B pilon fracture, 1 case of S-H type 2, and 1 case of S-H type 4 epiphysial injury. Among the PER type 4 cases, 2 cases were diagnosed as Maisonneuve fracture. There were 7 cases of foot fractures, including 4 cases of midfoot Lisfranc joint injury and 3 cases of forefoot injury. Among the 20 patients, 5 patients (25.0%) had open fracture injuries, and 12 patients (60.0%) needed surgical treatment. Among the 12 patients who underwent surgical treatment, 9 patients underwent open reduction and internal fixation, 2 patients had closed reduction and internal fixation, and 1 patient had open reduction surgery.
Table 3. Fracture Cases of the Lower Leg, Ankle, and Foot Associated with Electric Scooter Riding.
| Patient no. | Sex | Age (yr) | Injury mechanism | Injury site | Diagnosis | Treatment | Combined injury |
|---|---|---|---|---|---|---|---|
| 1 | F | 34 | Slip down | Ankle (AO 43B) | Fracture, distal tibiofibular, left (pilon) | ORIF with plate | |
| 2 | F | 67 | TA | Foot | Fracture, base, 3rd and 4th metatarsal bones, left Fracture, medial cuneiform, left | Short leg splint | Brain concussion |
| FU loss | |||||||
| 3 | M | 39 | Slip down | Lower leg (AO 42C) | Fracture, open, tibia shaft, right | ORIF with plate | |
| Fracture, proximal fibula, right | |||||||
| 4 | F | 23 | Slip down | Ankle (PER 4) | Fracture, posterior malleolus, ankle, left | ORIF with plate | |
| Fracture, medial malleolus, ankle, left | |||||||
| Fracture, fibula shaft, left | |||||||
| 5 | M | 11 | Slip down | Foot | Fracture, proximal phalange, 5th toe, right | Short leg splint | |
| 6 | F | 30 | Slip down | Foot | Fracture, base, 2nd, 3rd, and 4th metatarsal bones, left Injury, lisfranc joint, left | ORIF with plate | |
| 7 | M | 25 | Slip down | Foot | Fracture, base, 2nd, 3rd, and 4th metatarsal bones, right Injury, Lisfranc joint, right | Short leg splint | |
| 8 | M | 61 | TA | Lower leg | Fracture, fibula shaft, right | Long leg splint | L-spine Fx |
| 9 | M | 14 | Slip down | Ankle (S-H 4) | Fracture, triplane, right | Short leg splint | |
| FU loss | |||||||
| 10 | F | 17 | Slip down | Lower leg/Ankle (PER 4) | Fracture, medial, posterior malleolar, ankle, right | ORIF with screw | Facial Fx |
| Injury, syndesmosis, ankle, right | Syndesmosis fixation | ||||||
| Fracture, proximal fibula, right (Maisonneuve Fx) | |||||||
| 11 | F | 16 | Slip down | Ankle (SER 4) | Fracture, trimalleolar, ankle, left | ORIF with plate and screw | |
| 12 | F | 12 | TA | Lower leg (AO 42C) | Fracture, open, tibiofibular shaft, left | ORIF with nail | Phalanx Fx |
| 13 | M | 29 | Slip down | Ankle (PER 4) | Fracture, open, medial malleolar, ankle, right | ORIF with plate and screw | |
| Fracture, posterior malleolar, ankle, right | |||||||
| Fracture, fibula shaft, right | Syndesmosis fixation | ||||||
| Injury, syndesmosis, ankle, right | |||||||
| 14 | M | 21 | TA | Lower leg (AO 42C) | Fracture, open, shaft, tibiofibular, right | CRIF with IM nailing | Patella Fx |
| Fracture, proximal fibula, right | Femur Fx | ||||||
| 15 | F | 21 | Slip down | Lower leg/Ankle (PER 4) | Fracture, medial malleolar, ankle, right | ORIF with tension band wiring | |
| Injury, syndesmosis, ankle, right | |||||||
| Fracture, proximal fibula, right (Maisonneuve Fx) | Syndesmosis fixation | ||||||
| 16 | M | 16 | Slip down | Foot | Fracture, base, 3rd and 4th metatarsal bones, left | ORIF with plate | |
| 17 | M | 11 | Slip down | Ankle (S-H 2) | Fracture, lateral malleolar, left | Short leg splint | |
| 18 | M | 21 | Slip down | Foot | Fracture, open, distal phalange, 5th toe, right | Short leg splint | |
| Injury, nail bed, 5th toe, right | FU loss | ||||||
| 19 | M | 18 | Slip down | Ankle (AO 43B) | Fracture, distal tibiofibular, left (pilon) | Short leg splint | |
| Dislocation, ankle, left | FU loss | ||||||
| 20 | F | 45 | Slip down | Foot | Dislocation, 1st and 2nd MTPJs, left | Open reduction | |
| Fracture, head, 3rd and 4th metatarsal bones, left |
ORIF: open reduction and internal fixation, TA: traffic accident, FU: follow-up, PER: pronation external rotation, Fx: fracture, S-H: Salter-Harris, SER: supination external rotation, IM: intramedullary, CRIF: closed reduction and internal fixation, MTPJ: metatarsophalangeal joint.
Fig. 3. Images showing a right ankle fracture of a 29-year-old male patient. Preoperative gross image (A), simple radiographs (B, C), and computed tomography (CT) images (D, E) showing the open fracture of a pronation external rotation type 4 trimalleolar ankle fracture. (F) Intraoperative gross image of a posterior tibialis tendon rupture. Postoperative simple radiographs (G-I) and axial CT image (J) of the operated ankle.

Fig. 4. Images showing the preoperative and postoperative radiographic results of a 21-year-old female patient. (A-C) Preoperative simple radiographs showing the Maisonneuve fracture. Postoperative simple radiographs (D, E) and 1-year follow-up radiographs (F, G) of the operated ankle.

DISCUSSION
In this study, we revealed that the ankle and foot were the most common injury sites in e-scooter-related accidents. The most important finding of the present study is that e-scooter-related accidents resulted in high-frequency and high-severity foot and ankle injuries, including fractures that frequently required surgical treatment.
E-scooters were introduced in an effort to address difficult and congested transportation issues.6) In the case of South Korea, a scooter service started ianalyzed 103 patients withn 2018. The number of related accidents has increased sharply since then, as the popularity and availability of scooters increased. Our data (Fig. 2) support previous studies from several countries that have reported an increasing number of injuries resulting from e-scooter use.6,8) Blomberg et al.6) researched e-scooter-associated accidents in Copenhagen, Denmark, and reported that the number of accidents had increased since 2018 when public service of the e-scooter began. Kobayashi et al.8) also reported that the number of e-scooter accidents in San Diego, California, had increased since 2017 when the e-scooter rental service began. We presume that the number of e-scooter users continues to increase because the scooters are easy to use, inexpensive, fast, and eco-friendly. Particularly in South Korea, many middle, high school, and university students use them to commute between home and school. In the present study, the most common age groups of patients that used scooters were those in their 20s (43.7%) and those between 10 and 19 years of age (31.0%).
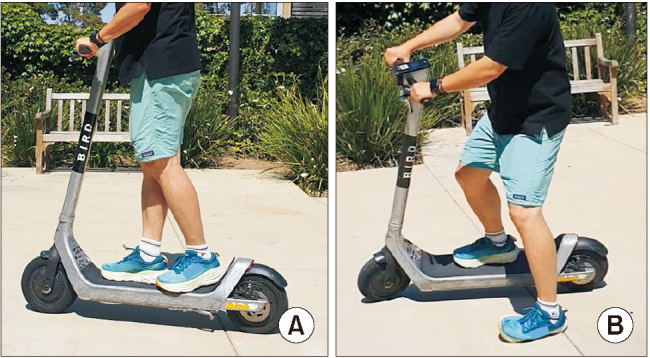
Kobayashi et al.8) analyzed 103 patients with e-scooter-associated accidents and reported that extremity fractures were the most frequent injury, occurring in 43 patients (42%). In the study, lower extremity fractures of the tibia, fibula (13 cases, 30%), and medial and lateral malleoli (6 cases, 14%) were the most frequent, which are in line with our data. However, in the present study, NES riders presented most often with injuries of the head and face (202 cases, 64.3%), followed by upper extremities (107 cases, 34.1%) and lower extremities (69 cases, 22.0%). The reasons why lower leg, ankle, and foot injuries commonly occur in e-scooter users have not been investigated. We presume that the ages of drivers and the driving methods of scooters are important factors that determine the site of the injuries. E-scooter users, whose mean age (25.4 years) was significantly higher than NES users (10.8 years) (p < 0.001), may have superior motor ability such that they are more likely to land on the ground with the foot, resulting in injury in the form of contusion, sprain, and/or fracture of the ankle and foot (Fig. 5). Particularly, ankle sprain and fracture are most likely to occur. On the other hand, NES users are mainly children with a mean age of 10.8 years; this group may have seen more injuries to the head and face as opposed to the upper or lower extremities, as they may lack sufficient motor ability and reflexes for protection by the foot landing during slip down. In addition, they must continuously use 1 leg to ride the scooter, which may make it more difficult to use their legs for landing. It is also worth noting that multiple injuries were more common in e-scooter users (42.8%) than in NES users (15.6%) (p < 0.001). Although the speed during the injuries was not evaluated, we presume higher speed and the force of the e-scooter induced higher energy trauma with more multiple injuries than the NES.
Fig. 5. Images showing electric scooter riding (A) and ankle injury during riding (B).
Regarding injury characteristics in the lower leg, ankle, and foot, only the injury severity by AIS showed a significant difference between the fracture and non-fracture groups. The AIS showed significantly higher severity in the fracture group than in the non-fracture group (p < 0.001). It is worth noting that all fracture groups had > grade 3 injury. These results may have occurred because the fracture group had considerably severe trauma in the ankle and foot during e-scooter riding, which induced a displaced fracture (grade 3), multiple closed displaced fractures (grade 4), and multiple open fractures (grade 5). Among the 16 patients followed up with foot and ankle fractures, 12 patients (75.0%) required surgical treatment. A previous study also reported that extremity fracture induced by e-scooter use was associated with a higher risk for treatment requiring surgical procedures.8)
In terms of the injured part, the ankle joint was the most common injury site in both the fracture group (45.0%) and non-fracture group (59.4%). The ankle fractures were surgically reduced and stabilized by a plate and screw according to the injury mechanism. As explained above, e-scooter users might have instantly landed on the ground with the foot to prevent an accident, which may have resulted in an ankle fracture by ankle eversion or inversion. Among the 9 cases with ankle fractures, PER type 4 was the most common injury (4 cases, 44.4%), and 2 cases among them were diagnosed as Maisonneuve fractures. Three cases of PER type 4 ankle fracture needed syndesmosis fixation. In addition, there were 2 cases of AO/OTA 43B pilon fracture and 1 case of triplane fracture. We believe that these high-energy ankle trauma injuries are relatively frequent in e-scooter riders, as they involve both slip down and fall from height injuries of the foot from the deck of the running e-scooter at high speed (Fig. 5). The exact mechanism of ankle injury in relation to e-scooter riding needs to be demonstrated in further experimental research.
The strength of the present study is that this is the first study to investigate the epidemiology and characteristics of e-scooter injuries focusing on the lower leg, ankle, and foot. Although previous studies have analyzed scooter-associated injuries, they have reported data mainly regarding the general characteristics of e-scooter injuries,4,8) without focusing on injuries of specific body parts. We investigated injury types focusing on the lower extremities, particularly the ankle, which showed the highest frequency of injury in the study. In addition, patients with ankle and foot injuries were further divided into fracture and non-fracture groups and were evaluated as to whether there were significant differences in variables between them.
This study also has several limitations. The primary limitation is the lack of external validity due to the relatively small size of the study population from 1 general hospital. Due to this limitation, a risk of selection bias remains. Our data cannot be generalized to the whole population. For example, the frequency of ages and the injury site may differ according to the different traffic laws and transportation systems of certain regions and countries. Additional studies with a larger sample size and primary data-based prospective and multicenter studies are warranted. However, compared to other studies, we analyzed a larger number of patients injured by e-scooter riding (n = 229). We searched the eligible patients using the CDW system, as opposed to the number code or surgical code, which allowed for more participants to be included from the electronic medical records of both the emergency room and outpatient clinic. Second, there was no investigation regarding alcohol/drug history or wearing of protective gear, which were reported to be important risk factors in other studies.6,8) Blomberg et al.6) investigated helmet use and alcohol/drug intoxication in e-scooter-associated accidents and reported that only 3.6% of patients wore protective gear, and 36.6% of patients had been drinking before using the scooter. Additional studies regarding the effects of protective gear (i.e., helmet use, ankle brace, and so forth) and drunk riding are needed in the near future.
E-scooter use continues to increase each year worldwide. Our results indicate that the ankle and foot are the most common injury sites in e-scooter-related accidents. Among the fracture group, ankle fractures were the most common, including PER type 4 injury and pilon fractures. Given the high frequency and severity of e-scooter-related ankle and foot injuries, we suggest that more attention be paid to preventing these types of injuries with greater public awareness of the dangers of using e-scooters.
ACKNOWLEDGEMENTS
This work was supported by the Konyang University Myunggok Research Fund of 2020.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Trivedi TK, Liu C, Antonio AL, et al. Injuries associated with standing electric scooter use. JAMA Netw Open. 2019;2(1):e187381. doi: 10.1001/jamanetworkopen.2018.7381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Toofany M, Mohsenian S, Shum LK, Chan H, Brubacher JR. Injury patterns and circumstances associated with electric scooter collisions: a scoping review. Inj Prev. 2021;27(5):490–499. doi: 10.1136/injuryprev-2020-044085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hennocq Q, Schouman T, Khonsari RH, et al. Evaluation of electric scooter head and neck injuries in Paris, 2017-2019. JAMA Netw Open. 2020;3(11):e2026698. doi: 10.1001/jamanetworkopen.2020.26698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Graef F, Doll C, Niemann M, et al. Epidemiology, injury severity, and pattern of standing e-scooter accidents: 6-month experience from a German level I trauma center. Clin Orthop Surg. 2021;13(4):443–448. doi: 10.4055/cios20275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brownson AB, Fagan PV, Dickson S, Civil ID. Electric scooter injuries at Auckland City Hospital. N Z Med J. 2019;132(1505):62–72. [PubMed] [Google Scholar]
- 6.Blomberg SN, Rosenkrantz OC, Lippert F, Collatz Christensen H. Injury from electric scooters in Copenhagen: a retrospective cohort study. BMJ Open. 2019;9(12):e033988. doi: 10.1136/bmjopen-2019-033988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Badeau A, Carman C, Newman M, Steenblik J, Carlson M, Madsen T. Emergency department visits for electric scooter-related injuries after introduction of an urban rental program. Am J Emerg Med. 2019;37(8):1531–1533. doi: 10.1016/j.ajem.2019.05.003. [DOI] [PubMed] [Google Scholar]
- 8.Kobayashi LM, Williams E, Brown CV, et al. The e-merging e-pidemic of e-scooters. Trauma Surg Acute Care Open. 2019;4(1):e000337. doi: 10.1136/tsaco-2019-000337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gennarelli TA, Wodzin E. AIS 2005: a contemporary injury scale. Injury. 2006;37(12):1083–1091. doi: 10.1016/j.injury.2006.07.009. [DOI] [PubMed] [Google Scholar]
- 10.Sanders R. New … and improved. J Orthop Trauma. 2012;26(7):385. doi: 10.1097/BOT.0b013e31825fb3ff. [DOI] [PubMed] [Google Scholar]
- 11.Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg (1920) 1950;60(5):957–985. [PubMed] [Google Scholar]
- 12.Cepela DJ, Tartaglione JP, Dooley TP, Patel PN. Classifications in brief: Salter-Harris classification of pediatric physeal fractures. Clin Orthop Relat Res. 2016;474(11):2531–2537. doi: 10.1007/s11999-016-4891-3. [DOI] [PMC free article] [PubMed] [Google Scholar]