

Every week in 2022, the equivalent of a highschool classroom’s worth of students — an average of 22 adolescents — died of drug overdoses in the United States, according to data from the Centers for Disease Control and Prevention (CDC). Drug overdoses and poisonings are now the third-leading cause of pediatric deaths in this country, after firearm-related injuries and motor vehicle crashes.1 Although drug-related mortality among adults has risen steadily for multiple decades, adolescents had been largely insulated from these increases until the second half of 2019.2 After more than a decade of holding relatively steady, overdose deaths among adolescents 14 to 18 years of age more than doubled between August 2019 and March 2020 (see graph). Since then, this crisis has further intensified, with 5.2 deaths per 100,000 adolescents in 2022.
This increase in mortality has occurred despite adolescent drug use becoming less common. Reported use of various types of illicit drugs has decreased in recent years. In 2002, 20.9% of U.S. 12th graders reported having used an illicit drug besides cannabis in the previous year; by 2022, the percentage had fallen to 8.0%.
An important driver of increasing risk is the widespread availability of counterfeit pills containing illicit fentanyl. Fentanyl is now involved in at least 75% of adolescent overdose deaths (see Supplementary Material). Although fentanyl-associated deaths in the general population began to rise sharply in 2013, adolescent deaths weren’t substantially affected until 2019.2 Fentanyl was initially predominantly found in powder forms, as a replacement for heroin. More recently, however, fentanyl has increasingly been pressed into counterfeit pills resembling oxycodone, benzodiazepines, and other prescription-drug tablets, which are far more likely to be used by adolescents for experimentation.3,4 In 2022, for example, 0.3% of 12th graders reported previous year heroin use, whereas 5.0% reported nonmedical use of prescription drugs. Many adolescents may be unaware of the proliferation of counterfeit pills.
To stem the rising tide of adolescent overdose deaths, we believe clinicians, parents, educators, and policymakers must act quickly. To help guide interventions, three groups of adolescents at potential risk for overdose can be identified: adolescents who experiment with substances and don’t have an opioid use disorder (OUD), who may be unaware of the risk associated with fentanyl; adolescents with mental illness or trauma, who may seek substances (including pills) to manage their symptoms; and adolescents with an OUD, some of whom may be knowingly using fentanyl. Overlaps and shifts among these groups can occur, but a key conclusion is that many adolescents who experience an overdose don’t have a known OUD. A recent study found that 41% of adolescents who died of an overdose between July 2019 and December 2021 had a known mental health problem or history of receiving mental health care, whereas only 11% had a history of receiving substance-use treatment.3
Since many adolescents may use fentanyl unknowingly, widespread implementation of up-to-date overdose-prevention education is essential. Most overdose deaths in adolescents (84%) are categorized as unintentional deaths. Pediatricians, other primary care clinicians, and mental health practitioners who see adolescents could routinely ask their patients whether they or their peers have been approached about purchasing pills, including on social media, or have used pills that weren’t prescribed to them. Many pediatricians already universally screen adolescents for substance use, which can serve as an introduction to a conversation about fentanyl. Clinicians can provide adolescents and family members with anticipatory guidance about counterfeit pills, signs of an overdose, and how to intervene in the event of an overdose.
Educators and parents can convey clear messages about the risk associated with fentanyl and counterfeit pills. Alcohol, nicotine, and cannabis remain the substances most commonly used by adolescents — and therefore deserve to be a focus of home- and school-based substance-use prevention programming — but are rarely implicated in drug-poisoning deaths. The focus of programming could be expanded to include education on fentanyl, counterfeit pills, naloxone, and techniques for reducing risk. Such programming should avoid using fear-based tactics and instead promote adolescents’ strengths, including their capacity for careful decision-making, desire for safety, and resilience.
Clinicians, educators, and parents can draw inspiration from the Safety First curriculum, which presents abstinence from drugs as the safest choice for adolescents but also provides information about risk reduction for those who choose to experiment with drugs. Messaging should include the recommendation to never use drugs alone, so that someone is available to intervene in the event of an overdose; information about where to find and how to use the overdose-reversal agent naloxone, which recently became available over the counter; and guidance to call emergency services in the event of an overdose, including reassurance that doing so won’t result in criminal penalties (in states that have Good Samaritan laws providing such protections).
Education would ideally be coupled with the provision of naloxone in schools — an approach recently implemented by numerous districts and recommended broadly by the Biden administration. Schools could also adopt “no questions asked” pill-disposal programs and provide students with anonymous mechanisms — such as messaging services — to ask questions about counterfeit pills and other substance use without risking punishment or shame.
Social media contributes to risk — but also offers opportunities — in this area. Counterfeit pills are commonly marketed to adolescents on social media platforms. These platforms are also sources of health information for adolescents, however, and therefore places where overdose-prevention education can occur. Public health agencies are often unsuccessful at building large followings of adolescents on social media, but they can partner with social media users who already have large followings (many of whom are adolescents) to disseminate accurate information. Social media platforms should strive to verify accounts that provide high-quality educational information and elevate their posts in their algorithms. Many recent overdose-prevention efforts, including efforts to expand access to naloxone in schools, have been spurred by activism among adolescents, often after the deaths of their peers. Adolescents should be recognized and empowered as agents who can drive change.
In addition, any long-term, sustainable strategy for addressing the adolescent overdose crisis will require the widespread availability of high-quality mental health care and addiction treatment. Mental health problems among adolescents have become considerably more common over the past decade — particularly depressive symptoms and suicidal ideation, according to CDC data, both of which can intensify substance use. Access to mental health care and substance-use treatment is often hampered by long wait times and high costs, and adolescents may be reluctant to seek care because of stigma. Mental health services should be available at minimal cost to families and with little or no wait, including in schools and other places that adolescents frequent.
Similarly, low-barrier and evidence-based addiction treatment should be available to adolescents, and steps should be taken to reduce the stigma associated with seeking treatment. Recent data suggest that only one in four residential addiction-treatment facilities for adolescents offers buprenorphine, the standard-of-care medication for OUD treatment in this age group.5 The recent elimination of the X-waiver requirement for prescribing buprenorphine creates new treatment opportunities; primary care clinicians can now more easily offer evidence-based buprenorphine treatment to adolescents in general medical settings.
Throughout, interventions will need to address disparities in overdose deaths based on race and ethnicity. Such mortality among non-Hispanic American Indian or Alaska Native adolescents was 1.82 times as high as that among non-Hispanic White adolescents between 2020 and 2022. Investment in Native-led, culturally appropriate substance-use prevention and treatment approaches will therefore be essential.
There are also geographic hotspots of adolescent overdose deaths, many of which are in the western United States. Arizona, Colorado, and Washington State had mortality nearly twice the national average or higher in 2020–2022. An assessment of hotspot counties — defined as those that had at least 20 overdose deaths and mortality higher than the national average during this period — revealed 19 counties of high concern. Maricopa County, Arizona, and Los Angeles County, California, had the highest number of fatal overdoses, with 117 and 111 deaths, respectively. School-based interventions could be prioritized in these counties.
The U.S. overdose crisis is affecting Americans at younger ages — even as adolescent substance use is decreasing. In response, parents, physicians, and educators must equip adolescents with the knowledge and tools they need to keep themselves safe, and adolescents must be supported with stronger mental health and addiction services.
Supplementary Material
Figure: Drug-Overdose Mortality and Previous-Year Illicit-Drug Use among High-School–Aged Adolescents in the United States.
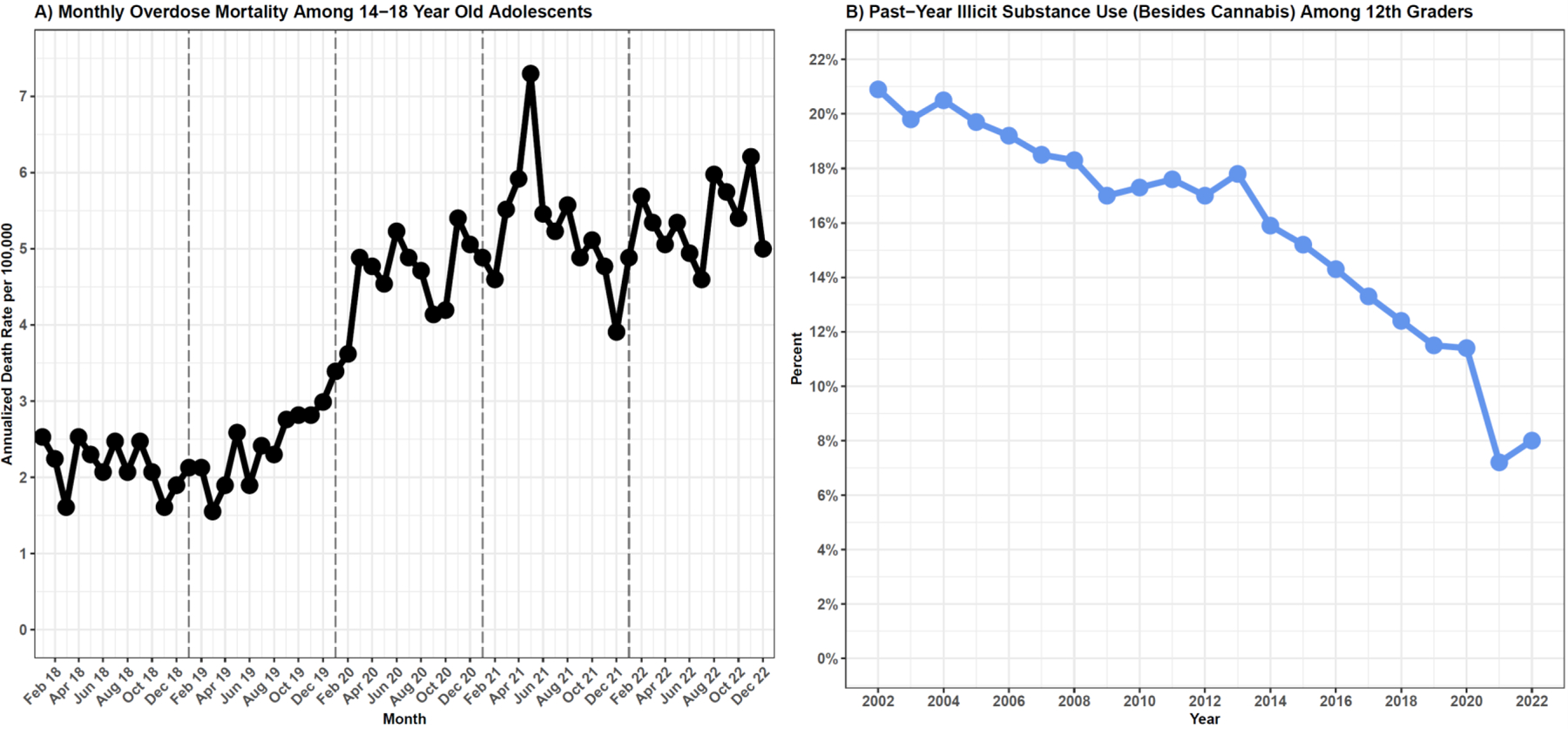
Panel A shows annualized monthly overdose deaths among adolescents 14 to 18 years of age between January 2018 and December 2022. Data are from the Centers for Disease Control and Prevention WONDER system. Data from 2022 are provisional. Panel B shows the percentage of 12th graders reporting use of illicit substances (besides cannabis) in the previous 12 months, between 2002 and 2022. Adapted from the Monitoring the Future survey (https://monitoringthefuture.org/data/). Specific question wording has shifted in minor ways over time.
Contributor Information
Joseph Friedman, Center for Social Medicine and Humanities, University of California, Los Angeles, Los Angeles in Boston
Scott E. Hadland, Division of Adolescent and Young Adult Medicine, Mass General for Children, and the Department of Pediatrics, Harvard Medical School Boston
References
- 1.Goldstick JE, Cunningham RM, Carter PM. Current causes of death in children and adolescents in the United States. N Engl J Med 2022;386:1955–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Friedman J, Godvin M, Shover CL, Gone JP, Hansen H, Schriger DL. Trends in drug overdose deaths among US adolescents, January 2010 to June 2021. JAMA 2022;327: 1398–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tanz LJ, Dinwiddie AT, Mattson CL, O’Donnell J, Davis NL. Drug overdose deaths among persons aged 10–19 Years — United States, July 2019–December 2021. MMWR Morb Mortal Wkly Rep 2022;71: 1576–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Palamar JJ, Ciccarone D, Rutherford C, Keyes KM, Carr TH, Cottler LB. Trends in seizures of powders and pills containing illicit fentanyl in the United States, 2018 through 2021. Drug Alcohol Depend 2022; 234:109398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.King C, Beetham T, Smith N, et al. Treatments used among adolescent residential addiction treatment facilities in the US, 2022. JAMA 2023;329:1983–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.