

Abstract
Objective:
The International Classification of Retinopathy of Prematurity (ICROP) is a consensus statement that creates a standard nomenclature for classification of retinopathy of prematurity (ROP). It was initially published in 1984, expanded in 1987, and revisited in 2005. This paper presents a third revision (ICROP3), which is now required because of challenges such as: (1) concerns about subjectivity in critical elements of disease classification, (2) innovations in ophthalmic imaging, (3) novel pharmacologic therapies (e.g. anti-vascular endothelial growth factor agents) with unique regression and reactivation features post-treatment compared to ablative therapies, and (4) recognition that patterns of ROP in some regions of the world do not neatly fit into the current classification system.
Design:
Review of evidence-based literature, along with expert consensus opinion.
Subjects, Participants, and/or Controls:
International ROP expert committee assembled in March 2019 (17 countries represented; 14 pediatric ophthalmologists, 20 retinal specialists; 12 females, 22 males).
Methods:
The committee was initially broken into three subcommittees (acute phase, regression/reactivation, imaging), each of which used iterative videoconferences and an online message board to identify key challenges and approaches. Subsequently, the entire committee used iterative videoconferences, two in-person multi-day meetings, and an online message board to develop consensus on classification.
Results:
ICROP3 retains current definitions such as zone (location of disease), stage (appearance of disease at the avascular-vascular junction), and circumferential extent of disease. Major updates in ICROP3 include refined classification metrics (e.g. “posterior zone II”, “notch” to describe incursion of disease into a more posterior zone, sub-categorization of stage 5, recognition that there is a continuous spectrum of vascular abnormality from normal to plus disease). They also include definition of aggressive ROP (A-ROP) to replace aggressive-posterior ROP because of increasing recognition that aggressive disease may occur in larger preterm infants and beyond the posterior retina, particularly in regions of the world with limited resources. ROP regression and reactivation are for the first time described in detail, with additional description of long-term sequelae.
Conclusions:
These principles may improve the quality and standardization of ROP care worldwide, and may provide a foundation to improve research and clinical care in the future.
Keywords: retinopathy of prematurity, prematurity, retina, pediatric ophthalmology, neonatology
INTRODUCTION
In 1953, Reese et al. published a classification of retrolental fibroplasia.1 By 1984, the International Classification of Retinopathy of Prematurity (ICROP) was developed by 23 ophthalmologists from 11 countries.2 This classification of acute ROP facilitated the first multicenter clinical treatment study (Cryotherapy for ROP [CRYO-ROP]), demonstrating that ROP could be successfully treated,3 thereby establishing the need for screening worldwide to identify a major cause of preventable childhood blindness.
In 1987, ICROP was expanded to include retinal detachment,4 and in 2005 was revisited to incorporate advances during the intervening years.5 Now, a third edition (ICROP3) is required for several reasons. First, certain components of ICROP are subjective and open to interpretation. Second, innovations in ophthalmic imaging have occurred. Third, introduction of anti-vascular endothelial growth factor (anti-VEGF) therapy has presented new challenges associated with recognition of clinical features characteristic of post-treatment regression and reactivation.6,7 Finally, the pattern of ROP in regions of the world with limited resources is not adequately described by the current classification system. Key features and changes in ICROP3, which are intended to address these challenges, are summarized in the Table. Each eye should be classified using examination parameters defined in this paper: zone, plus disease, stage, and extent. If aggressive ROP (A-ROP) is present, it should be noted.
Table. Summary of key components of International Classification of Retinopathy of Prematurity, 3rd edition (ICROP3) classification.
Each eye should be classified based on zone, plus disease, stage, and extent. If aggressive ROP (A-ROP) is present, it should be noted.
|
1. Zone a. Definition of 3 retinal zones centered on the optic disc. The location of the most posterior retinal vascularization or ROP lesion denotes the zone for the eye. b. Definition of a “posterior zone II" region that begins at the margin between zone I and zone II and extends into zone II for 2 disc diameters.* c. The term “notch" is used to describe an incursion by the ROP lesion of 1–2 clock hours into a more posterior zone. The ROP zone for such eyes should be noted by the most posterior zone of retinal vascularization with the qualifier “notch" (e.g. “zone I secondary to notch").* |
| 2. Plus and Pre-Plus disease: Plus disease is defined by the appearance of dilation and tortuosity of retinal vessels, and pre-plus disease is defined by abnormal vascular dilation and/or tortuosity insufficient for plus disease. Recognition that retinal vascular changes in ROP represent a continuous spectrum from normal to pre-plus to plus disease, with sample images demonstrating this range.* These changes should be assessed by vessels within zone I, rather than from only vessels within the field of narrow-angle photographs and rather than from the number of quadrants of abnormality.* |
| 3. Stage of acute disease (stages 1–3): defined by appearance of a structure at vascular-avascular juncture as stage 1 (demarcation line), stage 2 (ridge), and stage 3 (extraretinal neovascular proliferation or flat neovascularization). If more than one ROP stage is present in the same eye, the eye is classified by the most severe stage. |
| 4. Aggressive ROP (A-ROP): the term aggressive-posterior ROP (AP-ROP) was previously used to describe a severe, rapidly-progressive form of ROP located in posterior zone I or zone II. Because of increasing recognition that this may occur beyond the posterior retina and in larger preterm infants, particularly in regions of the world with limited resources, the Committee recommends the new term A-ROP.* |
|
5. Retinal detachment (Stages 4–5) a. Stages of retinal detachment are defined as stage 4 (partial: 4A with fovea attached, 4B with fovea detached) and stage 5 (total). b. Definition of stage 5 sub-categories: Stage 5A, in which the optic disc is visible by ophthalmoscopy (suggesting open-funnel detachment); Stage 5B, in which the optic disc is not visible due to retrolental fibrovascular tissue or closed-funnel detachment; and Stage 5C, in which stage 5B is accompanied by anterior segment changes (e.g. marked anterior chamber shallowing, irido-corneo-lenticular adhesions, corneal opacification), suggesting closed-funnel configuration.* |
| 6. Extent of disease: defined as 12 sectors in using clock hour designations. |
| 7. Regression: definition of ROP regression and its sequelae, whether spontaneous or following laser or anti-vascular endothelial growth factor (anti-VEGF) treatment. Regression can be complete or incomplete. Location and extent of persistent avascular retina (PAR) should be documented.* |
| 8. Reactivation: definition and description of nomenclature representing ROP reactivation following treatment, which may include new ROP lesions and vascular changes. When reactivation of ROP stages occurs, the modifier “reactivated" (e.g. “reactivated stage 2") is recommended* |
| 9. Long-term sequelae: emphasized beyond previous versions of ICROP, including sequelae such as late retinal detachments, PAR, macular anomalies, retinal vascular changes, and glaucoma. |
Key changes compared to previous ICROP publications.
LOCATION OF VASCULARIZATION: ZONE
Inner retinal vascularization commences around the 13th week of gestation, proceeding centrifugally from the peripapillary region to the peripheral retina, which is fully vascularized by approximately term.8 The location of retinal vascularization provides an indication of infant maturity and risk of developing ROP. The developing vasculature is lobular and closer to the optic disc nasally than temporally,9 but as a practical matter the state of vascularization (“zone”) is recorded as circles with the optic disc at the center.
There are 3 concentric retinal zones centered on the disc and extending to the ora serrata (Figure 1). The location of the most posterior retinal vascularization or ROP lesion denotes the zone for the eye. The most posterior region, zone I, is defined by a circle with radius twice the estimated distance from the optic disc center to the foveal center. Zone II is a ring-shaped region extending nasally from the outer limit of zone I to the nasal ora serrata and with the similar distance temporally, superiorly, and inferiorly. The Committee defines a region of 2-disc diameters peripheral to the zone I border as “posterior zone II” to indicate potentially more worrisome disease than ROP in more peripheral zone II (Table).
Figure 1. Schema of right eye (RE) and left eye (LE) showing zone borders and clock hour sectors used to describe the location of vascularization and extent of retinopathy.
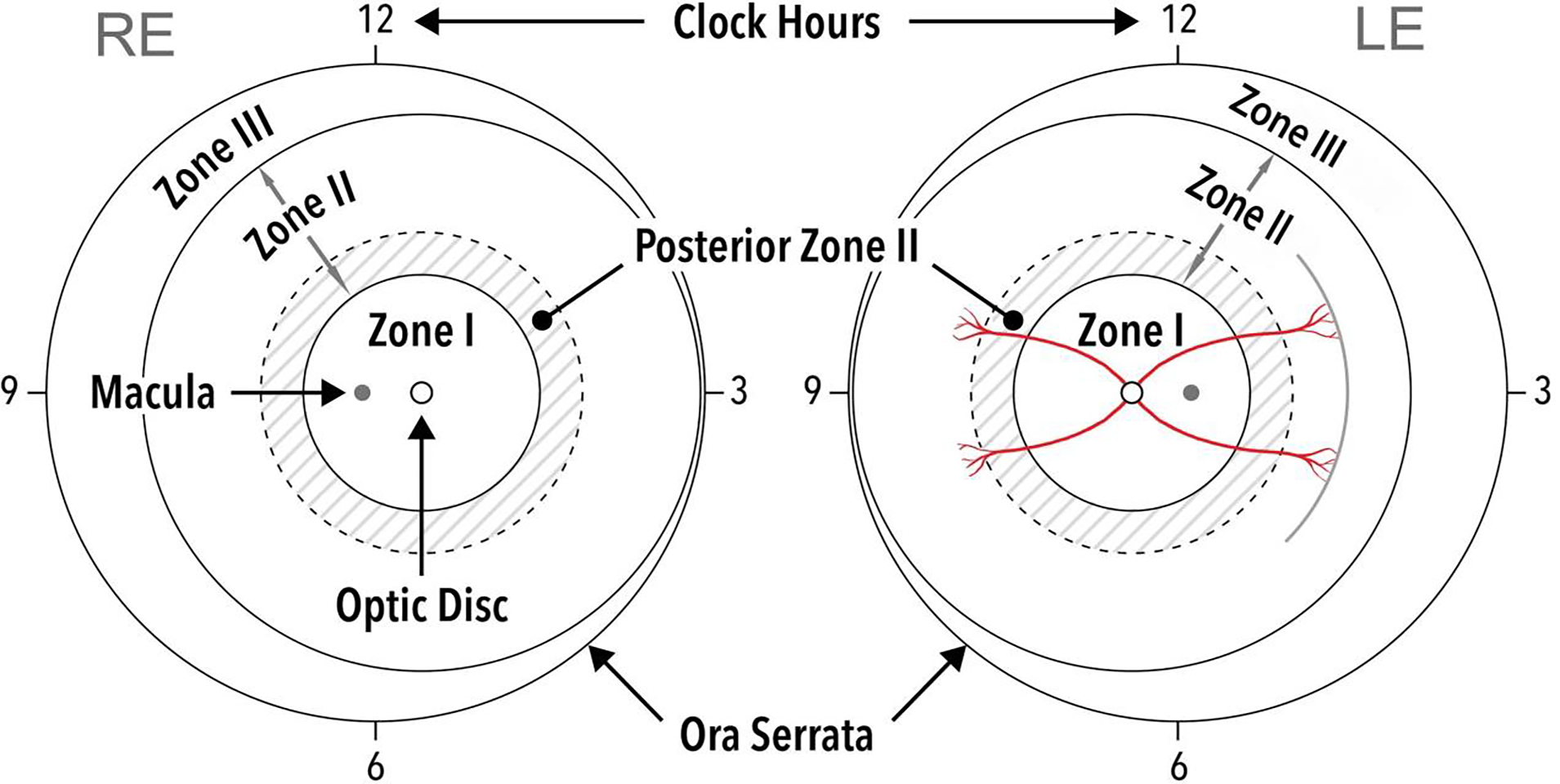
Solid circles represent borders of zones I-III, and dotted circles represent borders of posterior zone II (two disc diameters beyond zone I). A hypothetical example of examination findings is shown in the left eye, representing approximately three clock hours of stage 1 disease in zone II (note single line on drawing to document presence of stage 1 disease).
The Committee introduces the term “notch” to describe an incursion by the ROP lesion of 1–2 clock hours along the horizontal meridian into a more posterior zone than the remainder of the retinopathy. When present, this should be recorded by the most posterior zone of retinal vascularization with the qualifier “secondary to notch” (Table). For example, ROP in zone II in most places but with a temporal notch extending into zone I should be noted as “zone I secondary to notch”, thereby distinguishing it from an eye in which most disease was present in zone I.
Zone III is the residual crescent of peripheral retina that extends beyond zone II. To determine that ROP is in zone III, the ophthalmologist must ascertain that the nasal vessels are vascularized to the ora serrata, and that there is no ROP in the 2 nasal-most clock hours (Figure 1, nasally).
Practically, the temporal extent of zone I may be estimated using a 28-diopter lens. For example, by placing the nasal edge of the optic disc at one edge of the view, the limit of zone I is approximately at the temporal edge of the view. With retinal photography, the fovea may not be clearly identifiable in premature infants before 39 weeks PMA,10–12 so the foveal location may be approximated as the center of the macula.
PLUS AND PRE-PLUS DISEASE
Severe ROP is associated with dilation and tortuosity of the posterior retinal vessels, termed “plus disease” in 1982.13 A narrow-angle representative retinal photograph for plus disease was selected in ICROP 1984.2 A different photograph was selected for the CRYO-ROP Study and subsequent clinical trials to represent the minimum severity of vascular dilation and tortuosity necessary for plus disease.3,14 In ICROP 2005, “pre-plus disease” was defined to represent retinal vascular dilation and tortuosity that is abnormal but insufficient for plus disease.5 Of note, the original ICROP description of plus disease in 1984 included features of vascular engorgement of the iris, poor pupillary dilation, and peripheral retinal vascular engorgement with vitreous haze,2 which are now recognized as signs of advanced disease but not necessary for plus disease diagnosis.
The Committee recommends that the plus disease spectrum be determined from vessels within zone I, rather than from only vessels within the field of narrow-angle photographs and rather than from the number of quadrants of abnormality (Table).4,5,15,16 Representative examples of pre-plus (Figure 2A–C) and plus disease (Figure 2D–F) demonstrate this approximate field of view. The terms “pre-plus” and “plus” should continue to be used,17 but the Committee emphasizes that these terms represent a continuous spectrum of retinal vascular changes (Table). Figure 3 demonstrates gradings of this spectrum by members of this Committee. While gradings along this spectrum of plus and pre-plus disease may vary among observers,18–20 there is better agreement at the normal and severe ends.21 Importantly, in clinical practice, assessment of disease severity may consider other factors, including clinical and demographic risk factors, examination modality (e.g., digital retinal imaging vs. indirect ophthalmoscopy, lens power), zone of pathology, and rate of progression.22
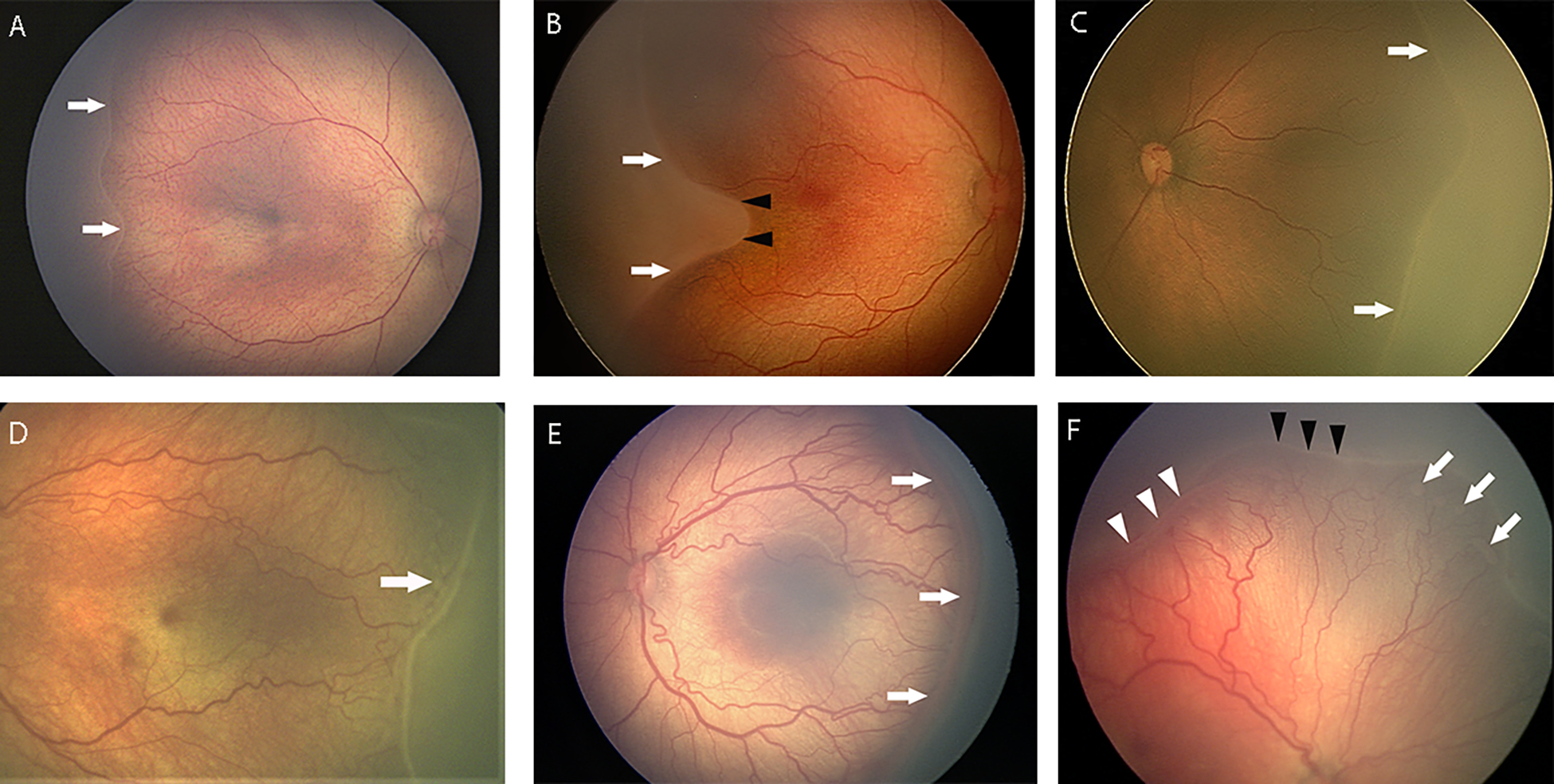
Figure 2. Wide-angle fundus photographs demonstrating examples of plus disease and pre-plus disease. Note varying levels of vascular abnormality, which are assessed in the central retina within the region of zone I.

(A) Mild pre-plus disease, with more arterial tortuosity and venous dilation than normal. (B) Pre-plus disease, with notable arterial tortuosity but minimal venous dilation. (C) Pre-plus disease, with moderate arterial tortuosity and venous dilation, but considered by majority of committee members to be insufficient for plus disease. (D) Plus disease with notable venous dilation and arterial tortuosity. Note that plus disease is out of proportion to visible peripheral findings, suggestive of flat neovascularization (stage 3, white arrows). (E) Severe plus disease, with dilation and tortuosity of both arteries and veins. (F) Severe plus disease. Note presence of ill-defined posterior flat stage 3 (arrows), which combined with severe plus disease is typical of aggressive ROP (A-ROP).
Figure 3. Continuous spectrum of vascular severity in ROP from normal to plus disease.

All 34 members of this committee graded 30 images as normal, pre-plus, or plus. Experts’ opinions varied as to the level of disease severity that constitutes pre-plus and plus disease. (A) Six representative images are displayed, where color scale on top reflects the average grading of committee members (from green = normal to red = plus), and demonstrates that vascular severity presents on a continuum. (B) Nine representative segmented images are displayed, where color scale represents mean vascular severity grading by committee members for each image (from green = normal to red = plus), and demonstrates that vascular severity presents on a continuum.
STAGE OF ACUTE DISEASE (STAGES 1–3)
In the developing premature infant, the retina is incompletely vascularized (Figure 4). When there is no ROP lesion, the Committee suggests using the term “incomplete vascularization” accompanied by the zone of vascularization (e.g. “incomplete vascularization into zone II”), rather than using terms such as “no ROP” or “immature retina”. When acute ROP vascular features develop at the junction of vascularized and avascular retina, “stages” are used to describe the appearance. If more than one ROP stage is present in the same eye, the eye is classified by the most severe stage.
Figure 4. Wide-angle fundus photograph demonstrating incomplete vascularization into zone II in the right eye of a premature infant at risk for retinopathy of prematurity.

Note progressive tapering and termination of retinal vascular arcades (white arrows).
Stage 1: Demarcation line
The demarcation line is a thin structure at the vascular-avascular juncture (Figure 5A–B, Figure 6A), which is relatively flat and white, lies within the plane of the retina, and may be associated with abnormal branching of vessels posterior to the line. Dilatation and tortuosity of peripheral retinal vessels at the vascular-avascular juncture alone are insufficient for diagnosis of stage 1.
Figure 5. Wide-angle fundus photographs demonstrating examples of acute retinopathy of prematurity (ROP) stages 1–3.
(A) Stage 1 demarcation line at border between vascular and avascular retina (white arrows). (B) Stage 1 demarcation line (white arrows) and associated notch (black arrowheads) between vascular arcades which would be considered zone I secondary to notch. Note pre-plus disease with mild retinal vascular tortuosity and dilation. (C) Stage 2 ridge, which is raised (white arrows) and thicker than stage 1. (D) Stage 2 ridge. Note “popcorn” lesions posterior to ridge (arrows) and pre-plus disease with mild vascular tortuosity and dilation. (E) Stage 3 disease with extraretinal neovascularization (white arrows). Note plus disease with vascular tortuosity and dilation. (F) Eye with both stage 2 (black arrowheads) and stage 3 (white arrowheads), and associated “popcorn” (white arrows). Note plus disease with vascular tortuosity and dilation.
Figure 6. Optical coherence tomography (OCT) images demonstrating examples of retinopathy of prematurity stages 1–3.
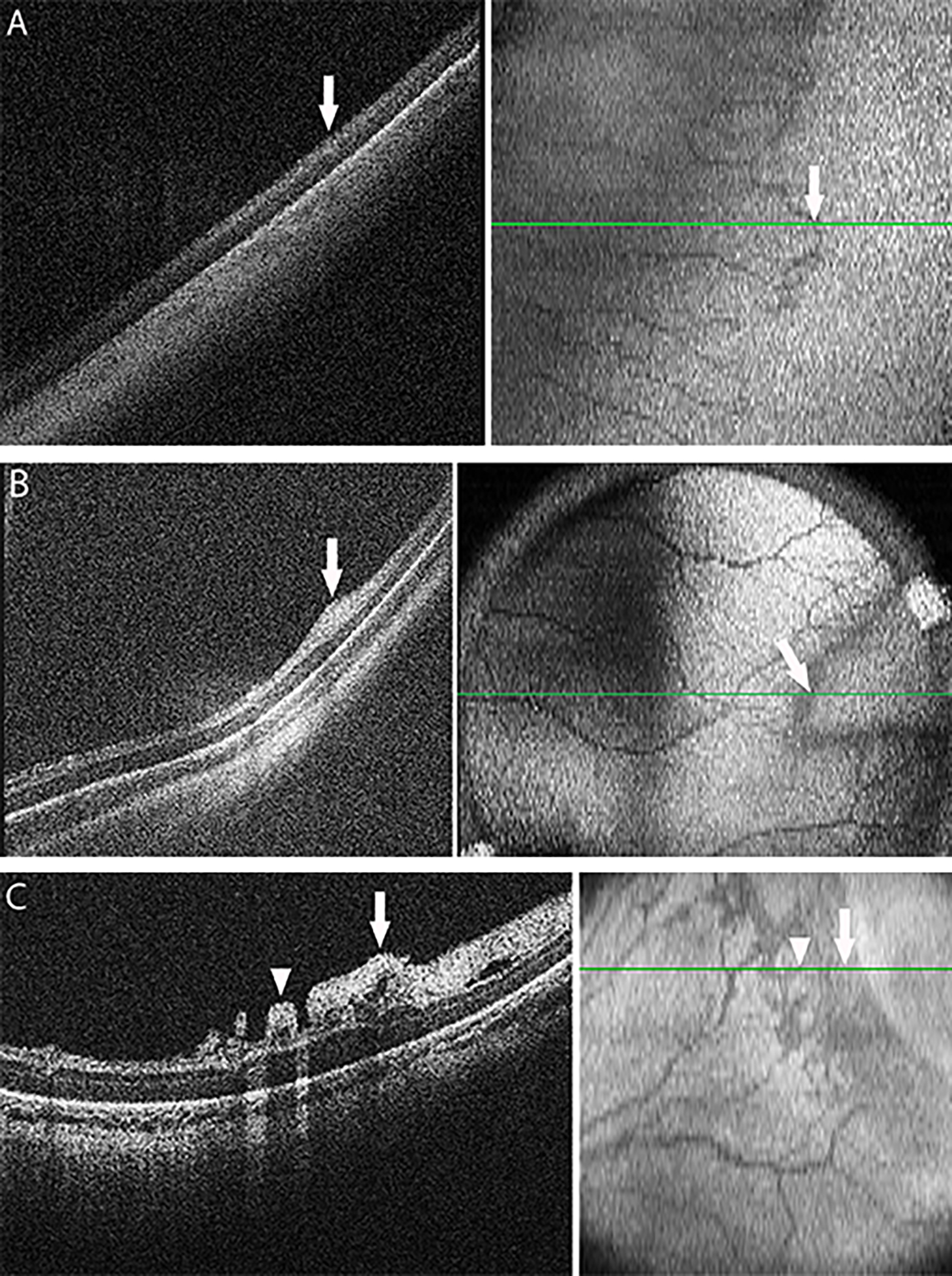
OCT cross-sectional B-scans (left side) are extracted from the raster scans that make up the OCT volume, at the location of the green-line (right side). The en face OCT images (right side) are summed from the OCT volume, and blood in retinal vessels casts a shadow across the underlying retina and choroid. (A) Stage 1 demarcation line (white arrows) on cross-sectional B-scan OCT image (left side) align with the retinal vascular-avascular junction (right side, note the vascular retina is to the left in all images). (B) Stage 2 ridge (white arrows) on cross-sectional B-scan OCT image (left side) at a site of focal thickening and bulge of inner retinal layers, aligns with the en face (right side) wider dark border of the vascular-avascular junction. (C) Stage 3 extraretinal neovascular proliferation at (white arrows) and posterior to (arrowheads) the vascular-avascular junction on cross-sectional B-scan OCT image (left side) and on en face view (right side). Note that blood in the extraretinal vessels also casts a shadow across the underlying retina and choroid.
Stage 2: Ridge
The hallmark of stage 2 ROP is a ridge with width and height that evolves from the demarcation line (Figure 5C–D, Figure 5F, Figure 6B). The ridge may vary in height and may be from white to pink in color. Small isolated tufts of neovascular tissue lying on the surface of the retina, commonly called “popcorn”, can be seen posterior to the ridge (Figure 5D, Figure 5F), but do not constitute stage 3.23,24
Stage 3: Extraretinal Neovascular Proliferation
In stage 3 ROP, extraretinal neovascular proliferation extends from the ridge into the vitreous (Figure 5E–F, Figure 6C) and is continuous with the posterior aspect of the ridge, causing a ragged appearance as proliferation becomes more extensive. “Flat”-appearing extraretinal neovascularization can occur in eyes with zone I or posterior zone II disease, in the absence of an obvious ridge or demarcation line, and is also considered stage 3. There may be varying degrees of extraretinal neovascular tissue associated with stage 3 (Figure 5E–F, Figure 6C).
AGGRESSIVE ROP (A-ROP)
Aggressive-posterior ROP (AP-ROP) was added to ICROP in 2005 to describe a severe, rapidly-progressive form of ROP located in zone I or posterior zone II.5 Previously known as “rush disease”, it may have been the florid acute ROP seen in the 1940s.1 AP-ROP as originally described typically affected the smallest premature infants.5,25 However, aggressive ROP is increasingly recognized to also occur in larger preterm infants and beyond the posterior retina, particularly in regions of the world with limited resources.26 Therefore, because the key diagnostic features of this phenotype are the tempo of disease and the appearance of vascular abnormalities, but not the location of disease, the Committee recommends use of the new term Aggressive ROP (A-ROP) to replace AP-ROP (Table).
The hallmark of A-ROP is rapid development of pathologic neovascularization and severe plus disease without progression being observed through the typical stages of ROP. In early A-ROP, the retina may exhibit capillary abnormalities posterior to the original border of vascularized retina, such as arterio-venous shunting resembling dilated vascular loops surrounding areas of vascular injury (Figure 7A). In some cases, this can be extreme with apparent loss of almost the entire vascularized retina (Figure 7). Eyes that develop A-ROP with more posterior disease may have thin vessels within zone I early in the disease course. Eyes with A-ROP often develop a form of stage 3 which may appear as deceptively featureless networks of “flat” neovascularization (Figure 7B–C), which can be difficult to visualize using a 28-diopter lens on ophthalmoscopy, but the use of greater magnification (e.g. 20-diopter lens) or fluorescein angiography may be helpful. Of note, extraretinal neovascularization as seen in classic stage 3 can also be seen in eyes with A-ROP (Figure 7C).27
Figure 7. Aggressive retinopathy of prematurity (A-ROP).

(A) A-ROP with severe vasoconstriction, capillary nonperfusion, non-physiologic dilated vascular loops and arterio-venous shunts, and plus disease in zone I. (B) A-ROP with border between vascular and avascular retina in zone I, dilated vascular loops (white arrows), diffuse flat extraretinal neovascularization most prominent superotemporally, and severe plus disease. Note absence of a typical stage 3 lesion. (C) A-ROP in zone I with severe plus disease, flat extraretinal neovascularization with fibrosis and early contraction superiorly (white arrowheads), and intraretinal and vitreous hemorrhage superotemporally. (D) and (E) are two examples of wide-angle fundus photographs (left sides) demonstrating A-ROP with ill-defined junction between vascular and avascular retina in zone I (white arrows), and severe plus disease. Fluorescein angiography (right sides) demonstrate significant vaso-obliteration with capillary nonperfusion. Note that there are no typical ROP lesion appearances and that there are vaso-attenuated areas posterior to the ridge.
RETINAL DETACHMENT (STAGES 4–5)
Acute disease and its regression are not always clearly demarcated. This is particularly apparent in retinal detachment, where both may be occurring.
Stage 4: Partial Retinal Detachment
Stage 4 describes partial retinal detachment, which either spares (stage 4A, Figure 8A–B) or involves the fovea (stage 4B, Figure 8C–E). Clinical features suggesting retinal detachment include loss of fine detail of choroidal vasculature or of granular pigment epithelium, and/or a “ground glass” appearance relative to adjacent attached retina. Macular ectopia and straightening of arcade vessels are signs of peripheral traction. Subtle foveal involvement may be most effectively discerned using optical coherence tomography (OCT) imaging (Figure 9). Stage 4 ROP may be exudative or tractional, occur in treated or untreated eyes, and vary in appearance depending on the tractional vectors and presence of exudation.28,29
Figure 8. Wide-angle fundus photographs demonstrating examples of retinopathy of prematurity stage 4.

(A) Stage 4A in temporal retina. Traction on extraretinal neovascularization leads to retinal elevation (white dots), which may be recognized during ophthalmoscopy by subtle change in brightness and loss of visible retinal pigment epithelium granularity and choriocapillaris detail. Note that approximate foveal center (asterisk) is not elevated, and that the extraretinal neovascularization (white arrows) may be significantly more peripheral than posterior extent of the detachment. (B) Stage 4A with 360-degree tractional retinal detachment in area of the peripheral ridge. (C) Stage 4B detachment involving the macula. Note straightening of the arcuate vessels and dragged optic disc appearance. (D) Stage 4B detachment with associated subretinal hemorrhage and lipid exudation into the macula. (E) Volcano shaped stage 4B. In eyes with posterior ROP, contraction of pathologic neovascularization can result in detachment of vascularized retina into a volcano-shaped configuration.
Figure 9. Optical coherence tomography (OCT) images demonstrating examples of stage 4 disease.
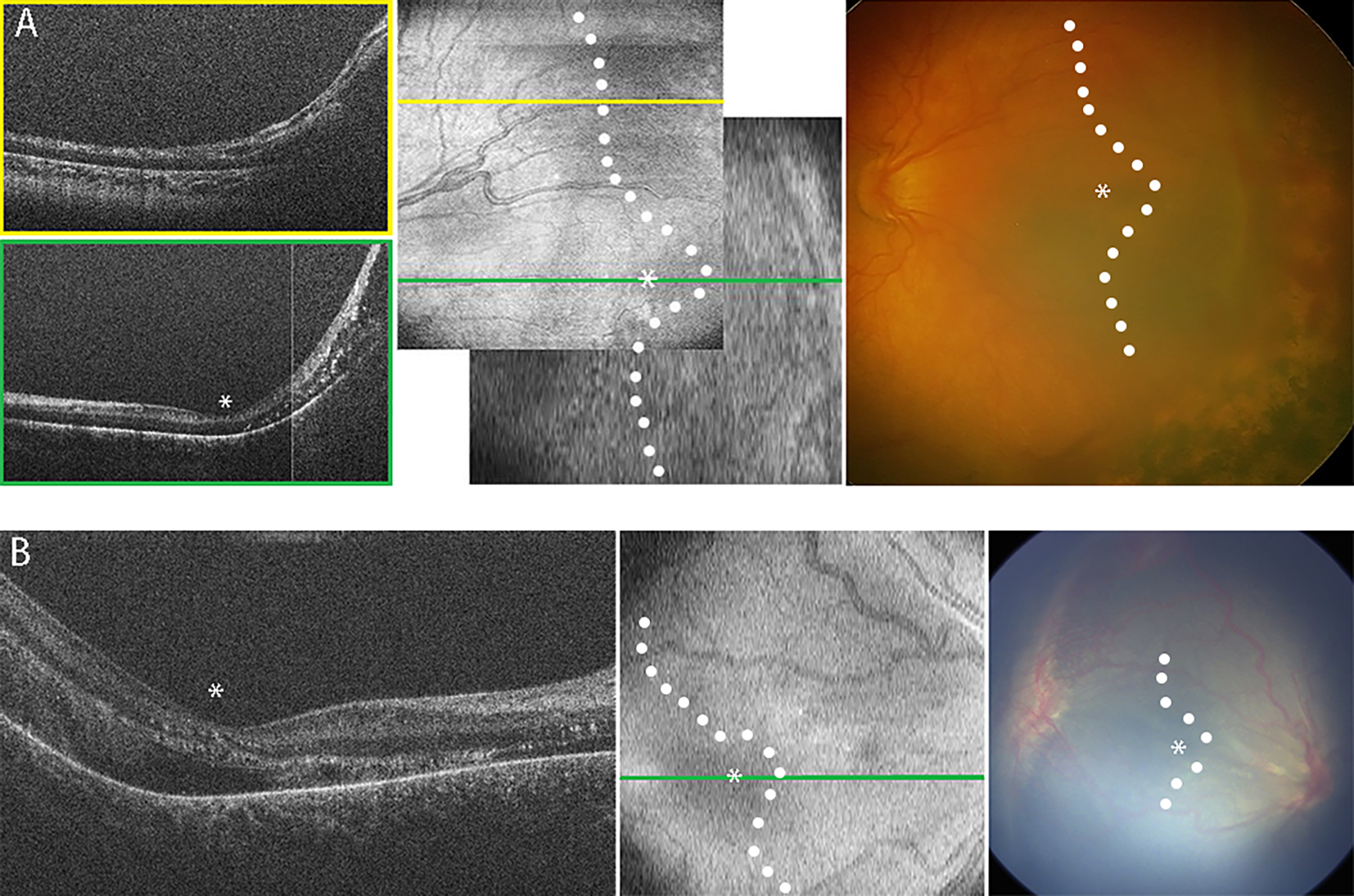
OCT cross-sectional B-scans (left side) are extracted from the raster of scans that make up the OCT volumes, viewed as summed en face (middle) with corresponding color photographs (right side). Note that in the color photographs, it is difficult to discern the extent of retinal detachment, especially foveal involvement. In en face OCT and color photos, the location of the fovea (asterisk) and margin of detachment (white dots) are determined from OCT B-scans. Blood in retinal vessels casts a shadow across the underlying retina and choroid in the en face views. (A) Stage 4A retinal detachment. On the en face OCT image (middle), yellow line demonstrates location of B-scan superior to the foveal center (upper left side, yellow box), green line demonstrates location of B-scan through the foveal center (bottom left side, green box). Note the attached retina on B-scan at the foveal center (asterisk), along with intraretinal exudates (hyperreflective dots), peripheral retinal detachment, and retinoschisis. (B) Stage 4B retinal detachment. Note detachment of retina at the foveal center (asterisks), which was very difficult to appreciate on ophthalmoscopic examination.
Exudative stage 4 detachments occur most commonly within days following laser treatment. They are typically convex in appearance, sometimes localized, and self-limited. Tractional detachments are associated with progressive fibrovascular organization and vitreous haze, and may be associated with lipid and/or subretinal hemorrhage (Figure 8D). Distinction by clinical examination between retinoschisis and detachment can be difficult. Eyes with A-ROP can develop a unique posterior “volcano” tractional detachment28 generally involving the fovea, in which the peripheral retina remains attached (Figure 8E). While the clinical appearance is reminiscent of a stage 5 funnel shaped detachment, these are more correctly considered stage 4B since the treated peripheral retina remains attached and the detachment is therefore not total.
Stage 5: Total retinal detachment
Total retinal detachment is designated as stage 5 (Figure 10). When fibrosis precludes visualization of the posterior pole, the extent of detachment can be examined by B-scan ultrasonography. The Committee recommends that total detachment be subcategorized into three configurations:30–32 stage 5A, in which the optic disc is visible by ophthalmoscopy (Figure 10A, suggesting open-funnel detachment); stage 5B, in which the optic disc is not visible secondary to retrolental fibrovascular tissue or closed-funnel detachment (Figure 10B–C); and stage 5C, in which findings of stage 5B are accompanied by anterior segment abnormalities (e.g., anterior lens displacement, marked anterior chamber shallowing, irido-capsular adhesions, and/or capsule-endothelial adhesion with central corneal opacification) (Figure 10D, suggesting a closed-funnel configuration).4,33
Figure 10. Images demonstrating examples of stage 5 retinopathy of prematurity.
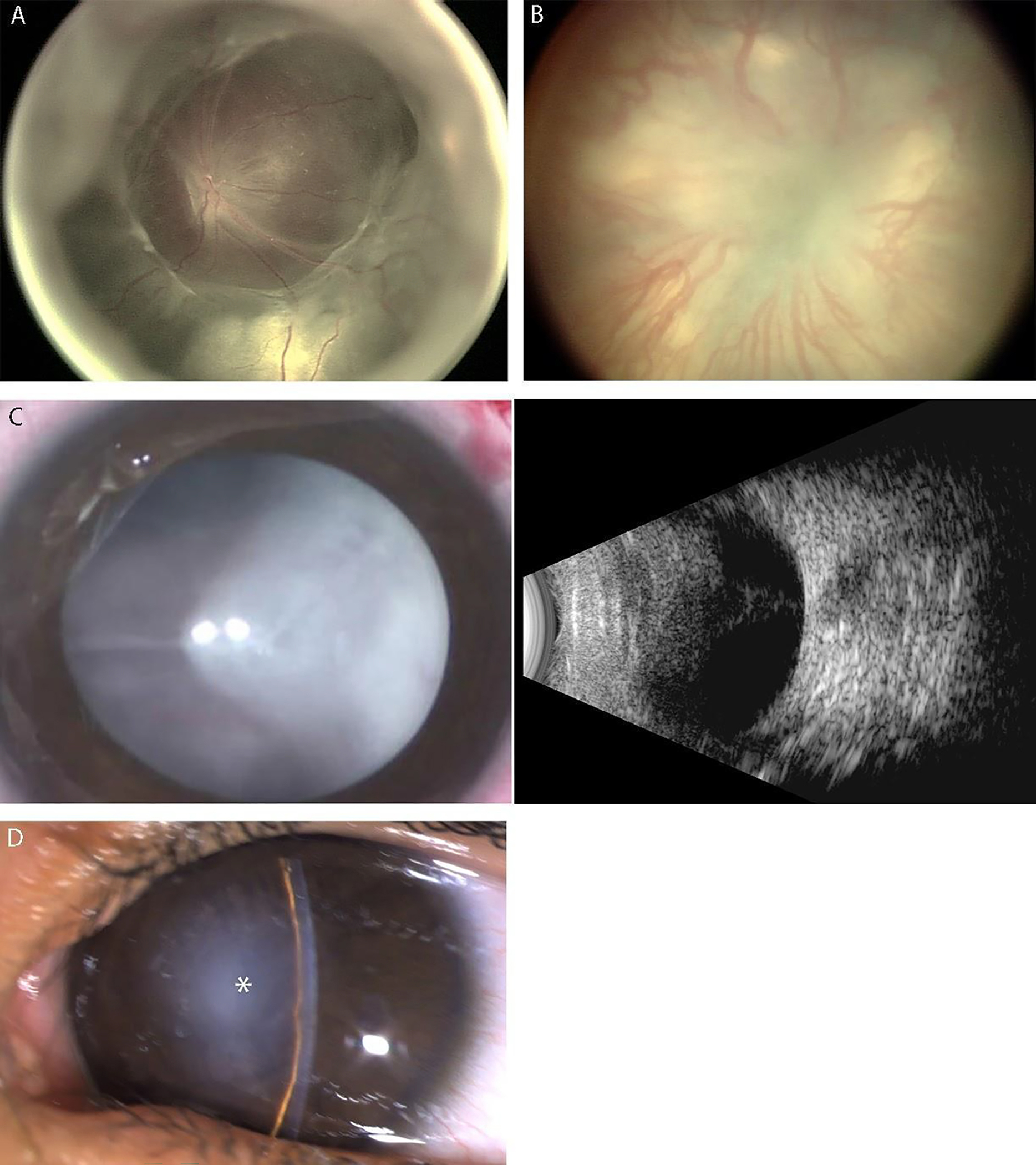
(A) Wide-angle fundus photograph showing stage 5A, characterized by a total retinal detachment with visible optic disc. Note open-funnel configuration. (B) Wide-angle fundus photograph showing Stage 5B, with no view of optic disc because of fibrovascular tissue. (C) External photograph of the normal anterior segment in stage 5B (left side), with no view of optic disc or retina secondary to retrolental fibrovascular tissue. B-scan ultrasonography (right side) reveals total retinal detachment with a posteriorly closed funnel configuration. (D) External photograph showing anterior segment characteristic of Stage 5C with anterior lens displacement, marked anterior chamber shallowing, central irido-capsule-endothelial adhesion, and central corneal opacification (asterisk) that prevent view of closed-funnel retinal detachment.
EXTENT
Extent of disease is classified using 30-degree sectors with boundaries along clock-hour positions (Figure 1).
REGRESSION, REACTIVATION, AND LONG-TERM SEQUELAE
To date, ROP classification has focused on acute disease, with less attention to regression.4,5,33 The introduction of anti-VEGF agents has presented new challenges. The clinical features and time course of regression following anti-VEGF treatment of ROP may differ compared to laser-treated eyes. When describing later phases of ROP, the Committee recommends use of two terms (Table): (1) “Regression,” which refers to disease involution and resolution, and (2) “Reactivation,” which refers to recurrence of acute phase features. Regression may be complete or incomplete, including persistence of retinal abnormalities. Regression and reactivation should not be regarded as either the reverse or the repetition of acute ROP.
Regression
Patterns of acute phase regression in ROP differ between spontaneous regression and those occurring following treatment. The Committee highlights features of regression related to vasculature as well as peripheral ROP findings (Figure 11).
Figure 11. Wide-angle fundus photographs demonstrating examples of ROP regression.
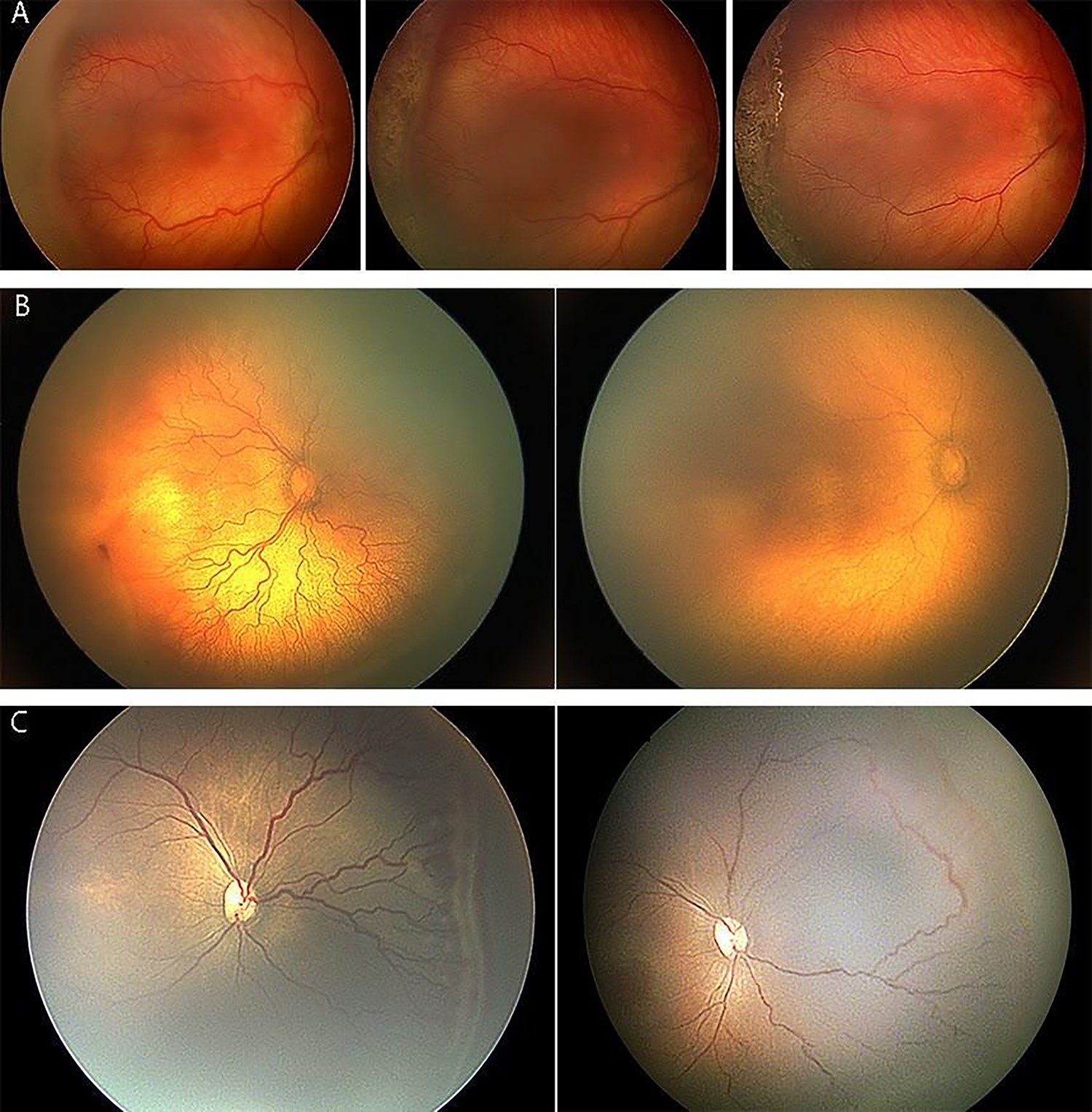
(A) Regression after laser treatment. Image on left is pre-treatment, showing stage 3 with plus disease. Image in middle is 1 week post-treatment, showing that stage 3 is thinner and whiter. Image on right is 1 month post-treatment, showing disease regression. (B) Regression of plus disease after anti-VEGF injection for aggressive ROP (A-ROP). Image on left is pre-treatment, showing plus disease and flat neovascularization (stage 3). Image on right is 2 weeks post-treatment, showing improvement in plus disease with no visible ROP lesion. (C) Regression after anti-VEGF injection. Image on left is pre-treatment. Image on right is 4 weeks post-treatment, showing absence of stage 3 and improvement in plus disease, with vascularization into peripheral avascular retina. Note the circumferential anastomosis in the area of original stage 3, along with reactivated stage 1 more anteriorly.
The first visible signs of regression are typically vascular and tend to occur more rapidly following anti-VEGF therapy (as early as 1–3 days)34 than following laser photocoagulation (around 7–14 days) or during spontaneous regression.33,35,36 These signs include decreased plus disease, where components of vascular dilation and tortuosity may become uncoupled (e.g., after anti-VEGF injection, reduced vessel dilatation can occur before reduced tortuosity, which may or may not occur); and vascularization into peripheral avascular retina, which can occur spontaneously or after anti-VEGF treatment. Other clinical signs of regression include involution of tunica vasculosa lentis, better pupillary dilation, greater media clarity, and resolution of intra-retinal hemorrhages.
Regression of the ROP lesion is characterized by thinning and whitening of neovascular tissue. Following spontaneous or treatment-induced regression, vascularization into the peripheral avascular retina can be complete or incomplete with what is termed “persistent avascular retina” (PAR) (Figure 12). PAR may occur in either the peripheral or posterior retina. Compared to peripheral PAR following spontaneous regression, PAR following treatment with anti-VEGF agents appears to occur with greater frequency and to involve a larger retinal area.37 PAR should be described by its location (e.g., posterior zone II) and extent (e.g., nasal).
Figure 12. Examples of persistent avascular retina (PAR) and long-term sequelae of ROP.

(A) Combined tractional and exudative detachment in an 18 year-old with a history of untreated ROP whose fellow eye was phthisical from ROP. (B) Ultra-widefield fluorescein angiogram (UWFFA) demonstrating PAR (asterisks) in a 7 year-old child with a history of spontaneously regressed ROP. Note the abnormal vascular configuration, particularly inferotemporally (circle). (C) UWFFA from a 7 year-old with spontaneously regressed ROP but with PAR and leakage in incompletely regressed stage 3 inferotemporally (asterisks). (D) Ultra-widefield fundus image (left side) displays an incompletely regressed ridge (white arrowheads) with PAR (asterisks) in a 15 year-old child with a history of extreme prematurity and no prior ROP treatment. Two years later (right side), the patient presented with a macula-involving rhegmatogenous detachment. The fellow eye had a similar appearance and disease course. (E) Optical coherence tomography angiography (OCTA) image of an incompletely developed foveal contour (left) and poorly-defined foveal avascular zone (right) in a 7 year-old with history of type 1 ROP treated with laser.
Reactivation
Reactivation is seen more frequently after anti-VEGF treatment than following spontaneous regression, and rarely if ever occurs after complete laser photocoagulation. Reactivation may occur after incomplete or complete regression of the original ROP lesion. Although the maximum time interval until reactivation after anti-VEGF injection is unknown, current evidence suggests it occurs most commonly between 37–60 weeks postmenstrual age (PMA). However, this may be affected by choice and dosage of anti-VEGF agent and may occur significantly later especially if re-injections are performed.38,39
Signs of reactivation range from development of a new self-limiting demarcation line to reactivated stage 3 with plus disease. The Committee highlights features of disease reactivation related to vasculature and ROP lesions (Figure 13) and notes that reactivation may not progress through the normal sequence of stages of acute phase disease.
Figure 13. Examples of ROP reactivation.

(A) Image at 38 weeks post-menstrual age (PMA) after intravitreal anti-vascular endothelial growth factor (anti-VEGF) injection at 32 weeks PMA with vascularization into peripheral avascular retina. Demarcation line (arrow) at the leading edge is reactivated stage 1. (B) Image of left eye at 100 weeks PMA after treatment with intravitreal anti-VEGF injection at 38 weeks PMA. There was vascularization into the peripheral avascular retina. There are often notable vascular abnormalities at the site of the original ridge, and in some cases residual fibrosis (asterisk), which is not indicative of reactivation unless accompanied by increasing vascular activity. (C) Image of vascularization into peripheral avascular retina with reactivated stage 1 disease (arrow) at 68 weeks PMA, after treatment with intravitreal anti-VEGF injection at 37 weeks PMA. Note multiple circumferential vascular loops at the site of the original ridge (asterisk). (D) Reactivation in a right eye at 67 weeks PMA, which had undergone intravitreal anti-VEGF injection at 33 weeks and again at 52 weeks PMA. There is reactivated stage 3 (asterisk) posterior to the leading edge of vascularization (arrow). (E) Left eye with reactivated stage 3 at the leading edge (arrow) at 50 weeks PMA, after intravitreal anti-VEGF injection at 36 weeks PMA. Vascularization into peripheral avascular retina has occurred between the original ridge (asterisks) and anterior reactivation. (F) Fluorescein angiogram at 45 weeks PMA of a left eye that had intravitreal anti-VEGF injection at 34 weeks PMA. There is leakage both at sites of leading edge reactivation (arrow), and at the original border (asterisk). (G) Right eye with zone I disease treated with intravitreal anti-VEGF injection at 34 weeks PMA (left side, arrow), and which appeared regressed on clinical exam at 38 weeks PMA (middle image, arrow). At 51 weeks PMA, the eye developed reactivated stage 3 at the same site (right side, arrow), without evidence of vascularization into peripheral avascular retina.
Vascular changes in ROP reactivation include recurrent vascular dilation and/or tortuosity, similar to acute phase “pre-plus” or “plus disease”. Extraretinal new vessels can occur and may be relatively delicate compared to those of acute ROP, making them difficult to visualize. Hemorrhages can occur around fronds of extraretinal vessels. Alternatively, extraretinal vessels may appear as a fibrovascular ridge, which may progress to fibrosis, contraction, and tractional detachment.28,29,40
Documentation of reactivation should specify presence and location(s) of new ROP features, noted by zone and stage using the modifier “reactivated”. For example, presence of a demarcation line during reactivation would be noted as “reactivated stage 1”. Reactivation typically occurs at the site of the original ridge and/or at the new leading edge of intraretinal vascular growth, but may also occur elsewhere within the vascularized retina. Signs of reactivation may be relatively subtle (Figure 13G). Reactivation with progression to stages 4 and 5 ROP is associated with vitreous condensation, haze, fibrotic contraction, and/or retinal breaks.4,5,28,29,33,40
Long-Term Sequelae
Patients with a history of premature birth, even without history of ROP, exhibit a spectrum of ocular abnormalities that may lead to permanent sequelae (Figure 12):4,33,41
Late tractional, rhegmatogenous, or rarely exudative retinal detachments (Figure 12D).42 Retinal detachment occurring in the absence of signs of ROP activity should not be designated as being due to reactivation, but rather as a sequela.43
Retinoschisis from chronic traction of involuted Stage 3 may progress without retinal detachment into the macula and threaten visual field and acuity.
PAR (Figure 12A–C). Avascular retina is prone to retinal thinning, holes, lattice-like changes, and may be associated with retinal detachments later in life.42–45
Macular anomalies including smaller foveal avascular zone,46–48 and blunting or absence of the foveal depression (Figure 12E). These may be related to the degree of acute phase ROP, and may be more apparent with fluorescein angiography or OCT imaging.24,37
Retinal vascular changes. These may include persistent tortuosity, straightening of the vascular arcades with macular dragging, and falciform retinal fold. Abnormal non-dichotomous retinal vessel branching, circumferential interconnecting vascular arcades, and telangiectatic vessels frequently occur. Vitreous hemorrhage may occur.
Glaucoma. Eyes with history of ROP can develop secondary angle closure glaucoma later in life.49,50
CONCLUSION
Understanding of disease pathophysiology and clinical management of ROP have evolved with advances in science, technology, and the art of medicine. Since the ICROP publication in 2005, some specific advances have involved neonatal care, anti-VEGF therapy, ophthalmic imaging, machine learning, and pediatric vitreoretinal surgery. This paper updates ROP classification in response to those advances by integrating review of evidence-based literature with expert consensus opinion. The Table summarizes how ICROP3 maintains many existing classification metrics, while refining and adding others such as revised classification metrics (e.g. “posterior zone II”, “notch”, sub-categorization of stage 5, recognition of continuous spectrum of vascular abnormality while maintaining the terms “pre-plus disease” and “plus disease”), definition of A-ROP to replace aggressive-posterior ROP, and definition of nomenclature representing ROP regression and reactivation. These principles will provide a foundation for improving research and clinical care in the future.
Still, ICROP3 simply marks a point in the journey toward improving ROP care and outcomes. We hope this will lead to increased understanding of acute phase ROP, its regression, and its reactivation. Areas in need of additional research include methods for quantifying vascular changes, the long-term risks of PAR, and the signs and timing of ROP reactivation. Further collaboration with other caregivers and investigators will improve the quality and standardization of ROP care worldwide.
Acknowledgments:
We acknowledge Lauren Kalinoski, MS, CMI (University of Illinois at Chicago) for assistance with artwork; Jimmy Chen, BA (Oregon Health & Science University) and Shwetha Mangalesh, MBBS (Duke University) for assistance with images; and Faruk Orge, MD (Case Western Reserve University), Sonal Farzavandi, FRCS (Edin) (Singapore National Eye Centre), and Derek Sprunger, MD (Indiana University School of Medicine) for support of this project through the International Pediatric Ophthalmology & Strabismus Council. None of these people were paid for their services.
Financial support:
This project was supported by a grant from the Knights Templar Eye Foundation; by departmental funding from the Illinois Eye and Ear Infirmary at the University of Illinois at Chicago (Chicago, IL); by grants R01EY19474, K12EY027720, P30EY001792, and P30EY10572 from the National Institutes of Health (Bethesda, MD); by R01EY015130 and R01EY017011 to MEH; NIH EY014800 and an Unrestricted Grant from Research to Prevent Blindness, Inc., New York, NY, to the Department of Ophthalmology & Visual Sciences, University of Utah; and by unrestricted departmental funding and a Career Development Award (JPC) from Research to Prevent Blindness (New York, NY). The sponsor or funding organization had no role in the design or conduct of this research.
Conflict of interest disclosures:
J. Peter Campbell receives research support from Genentech (South San Francisco, CA).
Antonio Capone Jr is an equity owner of Phoenix Technology Group, LLC, a founder and equity owner of Retinal Solutions, LLC and receives research support from AURA Biosciences (Cambridge, MA), Bayer (Leverkusen, Germany), Genentech (South San Francisco, CA), Ionis Pharmaceuticals (Carlsbad, CA), Novartis (Basel, Switzerland) and Regeneron Pharmaceuticals (Tarrytown, NY).
R. V. Paul Chan is on the Scientific Advisory Board for Phoenix Technology (Fremont, CA), a Consultant for Alcon (Ft. Worth, TX), and a Consultant for Novartis (Basel, Switzerland).
Michael F. Chiang was previously a Consultant for Novartis (Basel, Switzerland), an equity owner of InTeleretina (Honolulu, HI), and received research support from Genentech (South San Francisco, CA).
Alistair Fielder is a consultant for Novartis (Basel, Switzerland) and Bayer (Reading, United Kingdom)
Brian Fleck is a consultant for Novartis (Basel, Switzerland).
Mary Elizabeth Hartnett receives research support from the National Institutes of Health (R01EY017011, F01EY01730, EY014800), and is a consultant for Regeneron (Tarrytown, NY).
Domenico Lepore is a Consultant for Novartis (Basel, Switzerland) and Bayer (Leverkusen, Germany).
Şengül Özdek is a consultant for Novartis (Basel, Switzerland), Bayer (Leverkusen, Germany), and Allergan (Dublin, Ireland).
Andreas Stahl receives research support from Novartis (Basel, Switzerland), and is a Consultant for Novartis (Basel, Switzerland) and Bayer (Leverkusen, Germany).
Cynthia A. Toth receives research support from the National Institutes of Health (R01EY025009, U01EY028079, P30EY005722) and from a Research to Prevent Blindness Stein Award, royalties from Alcon (Fort Worth, TX), and is a founding and equity owner of Theia Imaging, LLC.
Wei-Chi Wu is a consultant for Novartis (Basel, Switzerland), Bayer (Leverkusen, Germany), and Allergan (Dublin, Ireland).
Conflict of interest:
Dr. Campbell is supported by research funding from the National Institutes of Health (R01EY19474, K12EY27720), the National Science Foundation (SCH-1622679), and Genentech (South San Francisco, CA). Dr. Capone is an equity owner of Phoenix Technology Group, LLC, a founder and equity owner of Retinal Solutions, LLC and receives research support from AURA Biosciences (Cambridge, MA), Bayer (Leverkusen, Germany), Genentech (South San Francisco, CA), Ionis Pharmaceuticals (Carlsbad, CA), Novartis (Basel, Switzerland) and Regeneron Pharmaceuticals (Tarrytown, NY). Dr. Fleck is a consultant for Novartis (Basel, Switzerland). Dr. Hartnett receives research support from the National Institutes of Health (R01EY017011, F01EY01730, EY014800), and is a consultant for Regeneron (Tarrytown, NY). Dr. Lepore is a Consultant for Novartis (Basel, Switzerland) and Bayer (Leverkusen, Germany). Dr. Özdek is a consultant for Novartis (Basel, Switzerland), Bayer (Leverkusen, Germany), and Allergan (Dublin, Ireland). Dr. Stahl receives research support from Novartis (Basel, Switzerland), and is a Consultant for Novartis (Basel, Switzerland) and Bayer (Leverkusen, Germany). Dr. Toth receives research support from the National Institutes of Health (R01EY025009, U01EY028079, P30EY005722) and from a Research to Prevent Blindness Stein Award, royalties from Alcon (Fort Worth, TX), and is a founding and equity owner of Theia Imaging, LLC. Dr. Wu is a consultant for Novartis (Basel, Switzerland), Bayer (Leverkusen, Germany), and Allergan (Dublin, Ireland).
On Behalf of the International Classification of Retinopathy of Prematurity Committee:
Writing Committee: Michael F. Chiang, Graham E. Quinn, Alistair R. Fielder, Susan R. Ostmo, R. V. Paul Chan
Committee Members:
Chair: Michael F. Chiang, MD (National Eye Institute, Bethesda, MD, USA)a
Vice Chair: Graham Quinn, MD, MSCE (Children’s Hospital of Philadelphia, Philadelphia, PA, USA)b
Audina Berrocal, MD (Bascom Palmer Eye Institute, Miami, FL, USA)
Gil Binenbaum, MD, MSCE (Children’s Hospital of Philadelphia,Philadelphia, PA, USA)
Michael Blair, MD (University of Chicago, Chicago, IL, USA)
J. Peter Campbell, MD, MPH (Oregon Health & Science University, Portland, OR, USA)
Antonio Capone, Jr., MD (Associated Retinal Consultants; Oakland University, Rochester, MI, USA)
R.V. Paul Chan, MD (University of Illinois at Chicago, Chicago, IL, USA) - Chair, International Pediatric Ophthalmology and Strabismus Council (IPOSC) ROP Committee
Yi Chen, MD (China-Japan Friendship Hospital, Beijing, China)
Shuan Dai, MD (Queensland Children’s Hospital, Brisbane, Australia)
Anna Ells, MD (Calgary Retina Consultants, Calgary, Alberta, Canada)
Alistair Fielder, FRCP (City, University of London, England)c
Brian Fleck, MD (University of Edinburgh, Edinburgh, Scotland)
William Good, MD (Smith-Kettlewell Eye Institute, San Francisco, CA, USA)
Mary Elizabeth Hartnett, MD (University of Utah, Salt Lake City, Utah, USA)
Gerd Holmstrom, MD (Uppsala University, Uppsala, Sweden)
Shunji Kusaka, MD, PhD (Kindai University, Osakasayama, Japan)
Andrés Kychenthal, MD (KYDOFT Foundation, Santiago, Chile)
Domenico Lepore, MD (A. Gemelli Foundation IRCSS, Catholic University of the Sacred Heart, Rome, Italy)
Birgit Lorenz, MD (Justus-Liebig-University Giessen, Germany and University Eye Department, Bonn, Germany)
Maria Ana Martinez-Castellanos, MD (APEC, Mexico City, Mexico)
Susan R. Ostmo, MS (Oregon Health & Science University, Portland, OR, USA)
Şengül Özdek, MD (Gazi University, Ankara, Turkey)
Dupe Ademola-Popoola, MD (University of Ilorin, Ilorin, Nigeria)
James Reynolds, MD (Ross Eye Institute, University at Buffalo, Buffalo, NY, USA)
Parag K. Shah, MD (Aravind Eye Hospital, Coimbatore, Tamil Nadu, India)
Michael Shapiro, MD (Retina Consultants, Des Plaines, IL, USA)
Andreas Stahl, MD (University Medicine Greifswald, Germany)
Cynthia Toth, MD (Duke University, Durham, NC, USA)
Anand Vinekar, MD, PhD (Narayana Nethralaya Eye Institute, Bangalore, Karnataka, India)
Linda Visser, MD (University of KwaZulu-Natal, Durban, South Africa)
David Wallace, MD, MPH (Indiana University School of Medicine, Indianapolis, IN, USA)
Wei-Chi Wu, MD, PhD (Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan)
Peiquan Zhao, MD (Xinhua Hospital and Shanghai Jiao Tong University School of Medicine, Shanghai, China)
Andrea Zin, MD, PhD (Fernandes Figueira Institute, FIOCRUZ, Rio de Janeiro, Brazil)
Footnotes
Lead of imaging subcommittee
Lead for acute phase subcommittee
Lead for regression/reactivation subcommittee
Meeting presentation: portions of this material were presented at the 2020 American Academy of Ophthalmology Annual Meeting (Retina and Pediatric Ophthalmology Subspecialty Days), and will be presented at the 2021 American Association for Pediatric Ophthalmology & Strabismus Annual Meeting.
Contributions and Access to data:
Dr. Chiang had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis
REFERENCES
- 1.Reese AB, King MJ, Owens WC. Classification of retrolental fibroplasia. Am J Ophthalmol. 1953;36(10):1333–1335. [PubMed] [Google Scholar]
- 2.The Committee for the Classification of Retinopathy of Prematurity. An international classification of retinopathy of prematurity. Arch Ophthalmol. 1984;102(8):1130–1134. [DOI] [PubMed] [Google Scholar]
- 3.Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Arch Ophthalmol. 1988;106(4):471–479. [DOI] [PubMed] [Google Scholar]
- 4.ICROP Committee for classification of late stages of ROP: An international classification of retinopathy of prematurity: II The classification of retinal detachment. Arch Ophthalmol. 1987;105:906–912. [PubMed] [Google Scholar]
- 5.Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity Revisited. Arch Ophthal. 2005;123(7):991. [DOI] [PubMed] [Google Scholar]
- 6.Mintz-Hittner HA, Kennedy KA, Chuang AZ, BEAT-ROP Cooperative Group. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603–615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Stahl A, Lepore D, Fielder A, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019;394(10208):1551–1559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Provis JM. Development of the primate retinal vasculature. Prog Retin Eye Res. 2001;20(6):799–821. [DOI] [PubMed] [Google Scholar]
- 9.Gallagher K, Moseley MJ, Tandon A, Watson MP, Cocker KD, Fielder AR. Nasotemporal asymmetry of retinopathy of prematurity. Arch Ophthalmol. 2003;121(11):1563–1568. [DOI] [PubMed] [Google Scholar]
- 10.Isenberg SJ. Macular development in the premature infant. Am J Ophthalmol. 1986;101(1):74–80. [DOI] [PubMed] [Google Scholar]
- 11.De Silva DJ, Cocker KD, Lau G, Clay ST, Fielder AR, Moseley MJ. Optic disk size and optic disk-to-fovea distance in preterm and full-term infants. Invest Ophthalmol Vis Sci. 2006;47(11):4683–4686. [DOI] [PubMed] [Google Scholar]
- 12.Chiang MF, Thyparampil PJ, Rabinowitz D. Interexpert agreement in the identification of macular location in infants at risk for retinopathy of prematurity. Arch Ophthalmol. 2010;128(9):1153–1159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Quinn GE, Schaffer DB, Johnson L. A revised classification of retinopathy of prematurity. Am J Ophthalmol. 1982;94(6):744–749. [DOI] [PubMed] [Google Scholar]
- 14.Capone A Jr, Ells AL, Fielder AR, et al. Standard image of plus disease in retinopathy of prematurity. Arch Ophthalmol. 2006;124(11):1669–1670. [DOI] [PubMed] [Google Scholar]
- 15.Gelman SK, Gelman R, Callahan AB, et al. Plus disease in retinopathy of prematurity: quantitative analysis of standard published photograph. Arch Ophthalmol. 2010;128(9):1217–1220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kim SJ, Campbell JP, Kalpathy-Cramer J, et al. Accuracy and Reliability of Eye-Based vs Quadrant-Based Diagnosis of Plus Disease in Retinopathy of Prematurity. JAMA Ophthalmol. 2018;136(6):648–655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Early Treatment For Retinopathy Of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol. 2003;121(12):1684–1694. [DOI] [PubMed] [Google Scholar]
- 18.Chiang MF, Jiang L, Gelman R, Du YE, Flynn JT. Interexpert Agreement of Plus Disease Diagnosis in Retinopathy of Prematurity. Arch Ophthal. 2007;125(7):875–80. [DOI] [PubMed] [Google Scholar]
- 19.Wallace DK, Quinn GE, Freedman SF, Chiang MF. Agreement among pediatric ophthalmologists in diagnosing plus and pre-plus disease in retinopathy of prematurity. J AAPOS. 2008;12(4):352–356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fleck BW, Williams C, Juszczak E, et al. An international comparison of retinopathy of prematurity grading performance within the Benefits of Oxygen Saturation Targeting II trials. Eye. 2018;32(1):74–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Campbell JP, Kalpathy-Cramer J, Erdogmus D, et al. Plus Disease in Retinopathy of Prematurity: A Continuous Spectrum of Vascular Abnormality as a Basis of Diagnostic Variability. Ophthalmology. 2016;123(11):2338–2344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gschlieber A, Stifter E, Neumayer T, et al. Effect of patients’ clinical information on the diagnosis of and decision to treat retinopathy of prematurity. Retina. 2018;38(11):2253–2259. doi: 10.1097/iae.0000000000001864 [DOI] [PubMed] [Google Scholar]
- 23.Wallace DK, Kylstra JA, Greenman DB, Freedman SF. Significance of isolated neovascular tufts (“Popcorn”) in retinopathy of prematurity. J AAPOS. 1998;2(1):52–56. [DOI] [PubMed] [Google Scholar]
- 24.Lepore D, Molle F, Pagliara MM, et al. Atlas of fluorescein angiographic findings in eyes undergoing laser for retinopathy of prematurity. Ophthalmology. 2011;118(1):168–175. [DOI] [PubMed] [Google Scholar]
- 25.Flynn JT, Chan-Ling T. Retinopathy of Prematurity: Two Distinct Mechanisms That Underlie Zone 1 and Zone 2 Disease. Am J Ophthalmol. 2006;142(1):46–59.e2. [DOI] [PubMed] [Google Scholar]
- 26.Shah PK, Narendran V, Saravanan VR, et al. Fulminate retinopathy of prematurity - clinical characteristics and laser outcome. Indian J Ophthalmol. 2005;53(4):261–265. [DOI] [PubMed] [Google Scholar]
- 27.Sanghi G, Dogra MR, Dogra M, Katoch D, Gupta A. A hybrid form of retinopathy of prematurity. Br J Ophthalmol. 2012;96(4):519–522. [DOI] [PubMed] [Google Scholar]
- 28.Hartnett ME, McColm JR. Retinal features predictive of progressive stage 4 retinopathy of prematurity. Retina. 2004;24(2):237–241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kondo H, Arita N, Osato M, Hayashi H, Oshima K, Uchio E. Late recurrence of retinal detachment following successful vitreous surgery for stages 4B and 5 retinopathy of prematurity. Am J Ophthalmol. 2009;147(4):661–666.e1. [DOI] [PubMed] [Google Scholar]
- 30.Jabbour NM, Eller AE, Hirose T, Schepens CL, Liberfarb R. Stage 5 retinopathy of prematurity. Prognostic value of morphologic findings. Ophthalmology. 1987;94(12):1640–1646. [DOI] [PubMed] [Google Scholar]
- 31.Gadkari SS, Deshpande M, Kulkarni S. Minimally fibrotic stage 5 ROP: a clinical prognostic factor in eyes undergoing vitrectomy for stage 5 retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2016;254(7):1303–1309. [DOI] [PubMed] [Google Scholar]
- 32.Ozsaygili C, Ozdek S, Ozmen MC, Atalay HT, Yeter DY. Preoperative anatomical features associated with improved surgical outcomes for stage 5 ROP. Retina. Published online September 10, 2020. doi: 10.1097/IAE.0000000000002948 [DOI] [PubMed] [Google Scholar]
- 33.Coats DK, Miller AM, Hussein MAW, McCreery KMB, Holz E, Paysse EA. Involution of retinopathy of prematurity after laser treatment: factors associated with development of retinal detachment. Am J Ophthalmol. 2005;140(2):214–222. [DOI] [PubMed] [Google Scholar]
- 34.Stahl A, Krohne TU, Eter N, et al. Comparing Alternative Ranibizumab Dosages for Safety and Efficacy in Retinopathy of Prematurity: A Randomized Clinical Trial. JAMA Pediatr. 2018;172(3):278–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ling CS, Fleck BW, Wright E, Anderson C, Laing I. Diode laser treatment for retinopathy of prematurity: structural and functional outcome. Br J Ophthalmol. 1995;79(7):637–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kwon JY, Ghodasra DH, Karp KA, et al. Retinal vessel changes after laser treatment for retinopathy of prematurity. J AAPOS. 2012;16(4):350–353. [DOI] [PubMed] [Google Scholar]
- 37.Vural A, Ekinci DY, Onur IU, Hergünsel GO, Yiğit FU. Comparison of fluorescein angiographic findings in type 1 and type 2 retinopathy of prematurity with intravitreal bevacizumab monotherapy and spontaneous regression. Int Ophthalmol. 2019;39(10):2267–2274. [DOI] [PubMed] [Google Scholar]
- 38.Mintz-Hittner HA, Geloneck MM, Chuang AZ. Clinical Management of Recurrent Retinopathy of Prematurity after Intravitreal Bevacizumab Monotherapy. Ophthalmology. 2016;123(9):1845–1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Wallace DK, Dean TW, Hartnett ME, et al. A Dosing Study of Bevacizumab for Retinopathy of Prematurity: Late Recurrences and Additional Treatments. Ophthalmology. 2018;125(12):1961–1966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Yonekawa Y, Thomas BJ, Thanos A, et al. The cutting edge of retinopathy of prematurity care: Expanding the Boundaries of Diagnosis and Treatment. Retina. 2017;37(12):2208–2225. [DOI] [PubMed] [Google Scholar]
- 41.Bowl W, Lorenz B, Stieger K, Schweinfurth S, Holve K, Andrassi-Darida M. Fundus-Controlled Dark Adaptometry in Young Children Without and With Spontaneously Regressed Retinopathy of Prematurity. Transl Vis Sci Technol. 2019;8(3):62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Uner OE, Rao P, Hubbard GB 3rd. Reactivation of Retinopathy of Prematurity in Adults and Adolescents. Ophthalmol Retina. Published online February 11, 2020. doi: 10.1016/j.oret.2020.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hamad AE, Moinuddin O, Blair MP, et al. Late-Onset Retinal Findings and Complications in Untreated Retinopathy of Prematurity. Ophthalmol Retina. 2020;4(6):602–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Garcia Gonzalez JM, Snyder L, Blair M, Rohr A, Shapiro M, Greenwald M. Prophylactic peripheral laser and fluorescein angiography after bevacizumab for retinopathy of prematurity. Retina. 2018;38(4):764–772. [DOI] [PubMed] [Google Scholar]
- 45.Al-Taie R, Simkin SK, Douçet E, Dai S. Persistent Avascular Retina in Infants With a History of Type 2 Retinopathy of Prematurity: To Treat or Not to Treat? J Pediatr Ophthalmol Strabismus. 2019;56(4):222–228. [DOI] [PubMed] [Google Scholar]
- 46.Mintz-Hittner HA, Knight-Nanan DM, Satriano DR, Kretzer FL. A small foveal avascular zone may be an historic mark of prematurity. Ophthalmology. 1999;106(7):1409–1413. [DOI] [PubMed] [Google Scholar]
- 47.Takagi M, Maruko I, Yamaguchi A, Kakehashi M, Hasegawa T, Iida T. Foveal abnormalities determined by optical coherence tomography angiography in children with history of retinopathy of prematurity. Eye. 2019;33(12):1890–1896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yanni SE, Wang J, Chan M, et al. Foveal avascular zone and foveal pit formation after preterm birth. Br J Ophthalmol. 2012;96(7):961–966. [DOI] [PubMed] [Google Scholar]
- 49.Bremer DL, Rogers DL, Good WV, Tung B, Hardy RJ, Fellows R. Glaucoma in the Early Treatment for Retinopathy of Prematurity (ETROP) study. J AAPOS. 2012;16(5):449–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Robinson J, Cheung AY, Nudleman E, et al. Ocular Hypertension in Adults with a History of Prematurity. Ophthalmol Retina. 2018;2(6):629–635. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Dr. Chiang had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis