

Abstract
The coronavirus 2019 (COVID-19) pandemic resulted in serious limitations for healthcare systems, and this study aimed to investigate the impact of COVID-19 surges on in-patient care capacities in Iran employing the Adaptt tool. Using a cross-sectional study design, our study was carried out in the year 2022 using 1-year epidemiologic (polymerase chain reaction-positive COVID-19 cases) and hospital capacity (beds and human resource) data from the official declaration of the pandemic in Iran in February 2020. We populated several scenarios, and in each scenario, a proportion of hospital capacity is assumed to be allocated to the COVID-19 patients. In most of the scenarios, no significant shortage was found in terms of bed and human resources. However, considering the need for treatment of non- COVID-19 cases, in one of the scenarios, it can be observed that during the peak period, the number of required and available specialists is exactly equal, which was a challenge during surge periods and resulted in extra hours of working and workforce burnout in hospitals. The shortage of intensive care unit beds and doctors specializing in internal medicine, infectious diseases, and anesthesiology also requires more attention for planning during the peak days of COVID-19.
Keywords: COVID-19, forecasting, hospitalization, pandemics, policymaking, scenario analysis
Introduction
The coronavirus 2019 (COVID-19) pandemic caused an unprecedented strain on healthcare systems around the world.[1] It was a challenge for national, regional, and global preparedness and response capacities and demonstrated the limitations of many health systems at the time of the pandemic.[2] These challenges demonstrated that scenario analysis and having an estimated burden of care in a pandemic can improve preparedness and response.
Generally, one in five of COVID-19 cases requires hospitalization and up to 16% of all hospitalized patients need ICU admission.[3,4] However, the hospital’s in-patient care capacity is limited and exceeding healthcare capacity can lead to reduced quality of care and increased mortality.[5,6]
This has raised serious concerns about the potential impact on health systems in low- and middle-income countries (LMICs) where some healthcare approaches were about to collapse in response to the COVID-19 pandemic.[7] Iran had one of the highest death rates from COVID-19 among Middle Eastern countries and was dealing with a couple of COVID-19 surges.[8,9]
Many of the healthcare systems with different levels of development employed innovative measures to increase the in-patient capacity by adding extra temporary beds or delaying the selective surgeries and care to provide COVID-19 care. However, managing the pandemic depends on predicting the next surges and there is an urgent need for tools to model the capacity of health systems.[10,11]
Intending to improve preparedness and national response plans, the World Health Organization (WHO) has designed several surge planning tools.[12,13] The one which is employed in this study is the Adaptt tool, developed by the WHO Regional Office for Europe, and was used to predict intensive care unit (ICU) and human resources capacity in Gulf Cooperation Council (GCC) countries as well.[14,15,16]
Therefore, this study aims to investigate the in-patient care at COVID-19 surges in Iran by using the Adaptt tool and real-world data to compare the estimation of shortages with measures employed by the healthcare system and discuss the lessons learned for future preparedness. These quantitative estimates based on the retrospective data can help healthcare authorities to use scenario analysis to promote hospital preparedness for an appropriate response to future public health emergencies.
Materials and Methods
Using a cross-sectional study design, our study was carried out using 1-year data from the official declaration of the pandemic in Iran in February 2020. We employed the Adaptt tool to evaluate the capacities of the hospitals covered by the Iran University of Medical Sciences (IUMS) in Tehran province. This study was approved by the Research Ethics Committee of the Iran University of Medical Sciences (ethical code: IR.IUMS.REC.1400.696).
Tool
The Adaptt Surge Planning Support Tool is an Excel-based graphical tool that simulates various parameters and accordingly allows policy-makers and senior planners to focus on surge planning information.[12]
Data collection
The required data to input the model in the Adaptt tool were categorized into two parts:
Epidemiologic data: Daily confirmed COVID-19 cases and a cumulative number of COVID-19 cases since the beginning of the outbreak obtained from the IUMS deputy of health. It should be noted that these data were for those patients whose polymerase chain reation (PCR) tests were found positive and include those patients who were clinically diagnosed based on the computed tomography (CT) scan.
Hospital capacity data: Including the number of general and ICU beds in each hospital and data on the number of COVID-19 patients hospitalized in both general and ICU wards. We also obtained the human resource (HR) data for different types of staff including nurses, general practitioners, and specialists in each hospital.
Modeling
The model needs to be populated by choosing the epidemiologic model tab first. The epidemiologic model should be chosen from two options: the widely used SIR (Susceptible, Infected, and Recovered) model[17] or another customized model. We selected the SIR model based on the input variables.[18]
Further parts of the tool were completed by the following parameters: COVID-19 daily update, hospital activity and practices (in/out), installed capacity, HRs, HR capacity (to COVID-19 in-patients), and HR occupational risk.
Data analysis
We examined different scenarios to understand how the surge in the cases and resource allocation to COVID-19 patients would affect the hospital’s capacities. These scenarios were defined by changing the available hospital capacities (both beds and HRs) to respond to the surges. Therefore, we assumed a range of best-case scenarios (when the majority of beds and HRs were allocated to COVID-19 patients) to worse-case scenarios (when there were minimum resources available to these patients).
Results
Scenarios for prediction of required hospital beds
First scenario
In the first scenario, we assumed that 100% of university hospital beds are allocated to COVID-19 patients; as can be seen in Figure 1, there will be no shortage in the system. Since it is not possible to allocate all beds to COVID-19 patients, we examined other scenarios as well.
Figure 1.
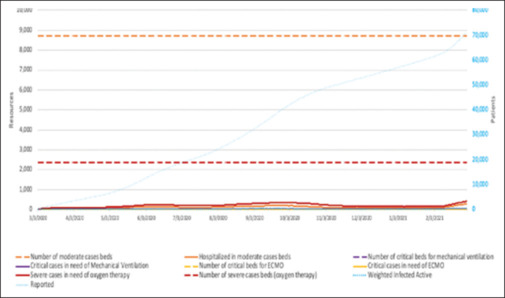
Prediction of required hospital beds with 100% capacity of hospital beds for COVID-19 patients
Second scenario
In the second scenario, we assumed 30% of the capacity of the hospital beds is allocated to COVID-19 patients. In this scenario, we still do not have any shortage in the healthcare system as the beds available for oxygen therapy could cover up to 20,000 cases and the peak does not reach this point in this scenario.
Scenarios for prediction of the required HRs
First scenario
In this scenario, we assumed that 100% of our HRs in the hospitals are allocated to COVID-19 patients and the results showed no shortage.
Second scenario
As mentioned earlier, allocating all available HRs to the treatment of COVID-19 patients is far from the reality that happened in the healthcare system. So, in a more realistic scenario, we assumed that 70% of the HR capacity is allocated to treat COVID-19 patients. In this case, no shortage was observed in HRs including GP, specialists, and nurses.
Third scenario
In the final scenario, to get as close as possible to the existing realities, we considered the HRs available for the treatment of COVID-19 patients are 50% of the total hospital capacity. Figure 2 below reports the shortage divided up into different specialties.
Figure 2.
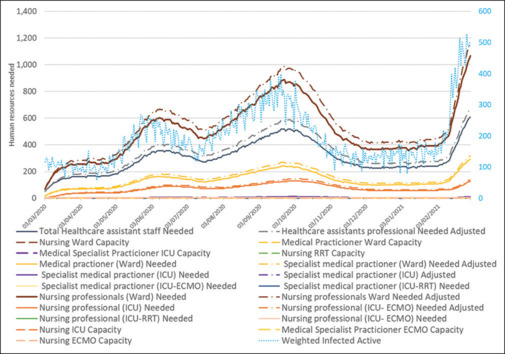
Prediction of the required HRs with 50% capacity
Discussion
The Adaptt tool may assist the program managers and health authorities to manage in-patient capacities by predicting the number of beds and HRs required for providing care for different categories (mild, moderate, severe, or critical) of COVID-19 patients.[5,19]
The recommendations for upgrading the capacity of the hospitals to meet the requirement of acute and intensive care broadly target four domains, namely, staff, premises, supplies, and finally the framework. From the staff point of view, the Adaptt tool estimates the requirement of the health specialists and social workers depending on their competence level to meet the daily health needs of the diagnosed patients.[20,21]
In our initial scenario and assuming 100% allocation of the available HRs to COVID-19 in-patient care, there is no shortage of nurses in this scenario. The maximum number of nurses is 3400, and at the peak of the disease, the need for nursing staff reaches about 1200 people, which is less than the number of available staff.
In the scenario of 70% available HRs, which is a more realistic scenario and considers the HRs required for other patients, the nursing staff capacity is reduced to 2,400 nurses, which still indicates the adequacy of the HR during the surge period.
In the 70% scenario, considering the fact that the available specialists are also treating other patients and not all of them necessarily play a role in the treatment of COVID-19 patients, it can be observed that during the peak period, the number of required and available specialists is exactly equal, which was a challenge during surge periods and resulted in extra hours of working and workforce burnout in hospitals.
It should be noted that the main limitation of this study was the epidemiologic data, which only reflected the official positive test cases and not the CT scan or clinically diagnosed ones. Therefore, the daily and total cases reported are under-estimated. Although none of the scenarios above shows the shortage of beds or HRs, in real-world experience, there were severe shortages at some points which interrupted the usual care, leading to the cancelation of the surgeries while operation halls were equipped for temporary intensive care of the COVID-19 patients. Furthermore, during the first year of the pandemic, temporary in-patient beds were installed in non-hospital settings for COVID-19 patients who needed care.
As for nursing staff, there were also real-world shortages and the IUMS used temporary short-term contracts to employ nursing senior students and those who were not employed permanently by other hospitals for the period of the pandemic only.
By having an estimation of required resources at surges with monitoring the rapid upsurge within the number of cases, actions should be taken to make more capacities within or outside of the hospital, which can be reserved for the care of COVID-19 patients, without compromising the care for other patients.[21,22]
The general coordination between different departments of the hospital is important, and they should work in utmost collaboration with each other to respond to the challenge of meeting the demands of healthcare services at the time of the pandemic.[5,23]
Conclusion
The Adaptt tool is an applicable tool to predict shortages at the sudden upsurge of COVID-19 cases, and thereby, this analysis could be expanded to Tehran province and country level in order to improve our planning for preparedness and response to the COVID-19 surges in future. The shortage of ICU beds and doctors specializing in internal medicine, infectious diseases, and anesthesiology requires more attention for planning during the peak days of COVID-19.
Financial support and sponsorship
This study was supported by Iran University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
References
- 1.McCabe R, Schmit N, Christen P, D’Aeth JC, Løchen A, Rizmie D, et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020;18:329.. doi: 10.1186/s12916-020-01781-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Haldane V, De Foo C, Abdalla SM, Jung A-S, Tan M, Wu S, et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat Med. 2021;27:964–80. doi: 10.1038/s41591-021-01381-y. [DOI] [PubMed] [Google Scholar]
- 3.Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in lombardy, Italy: Early experience and forecast during an emergency response. JAMA. 2020;323:1545–6. doi: 10.1001/jama.2020.4031. [DOI] [PubMed] [Google Scholar]
- 4.Leclerc QJ, Fuller NM, Keogh RH, Diaz-Ordaz K, Sekula R, Semple MG, et al. Importance of patient bed pathways and length of stay differences in predicting COVID-19 hospital bed occupancy in England. BMC Health Serv Res. 2021;21:566.. doi: 10.1186/s12913-021-06509-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Li R, Rivers C, Tan Q, Murray MB, Toner E, Lipsitch M. Estimated demand for US Hospital inpatient and intensive care unit beds for patients with COVID-19 based on comparisons with Wuhan and Guangzhou, China. JAMA Network Open. 2020;3:e208297.. doi: 10.1001/jamanetworkopen.2020.8297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Castagna F, Xue X, Saeed O, Kataria R, Puius YA, Patel SR, et al. Hospital bed occupancy rate is an independent risk factor for COVID-19 inpatient mortality: A pandemic epicentre cohort study. BMJ Open. 2022;12:e058171.. doi: 10.1136/bmjopen-2021-058171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rees EM, Nightingale ES, Jafari Y, Waterlow NR, Clifford S, CA BP, et al. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020;18:270.. doi: 10.1186/s12916-020-01726-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pormasoumi H, Rostami D, Jamebozorgi K, Mirshekarpour H, Heshmatnia J. COVID-19 management in Iran and international sanctions. Eu J Transl Myol. 2022;32:10777.. doi: 10.4081/ejtm.2022.10777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rassouli M, Ashrafizadeh H, Shirinabadi Farahani A, Akbari ME. COVID-19 management in Iran as one of the most affected countries in the world: Advantages and weaknesses. Front Public Health. 2020;8:510.. doi: 10.3389/fpubh.2020.00510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sheikhbardsiri H, Raeisi AR, Nekoei-Moghadam M, Rezaei F. Surge capacity of hospitals in emergencies and disasters with a preparedness approach: A systematic review. Disaster Med Public Health Prep. 2017;11:612–20. doi: 10.1017/dmp.2016.178. [DOI] [PubMed] [Google Scholar]
- 11.Bekker R, uit het Broek M, Koole G. Modeling COVID-19 hospital admissions and occupancy in the Netherlands. Eur J Oper Res. 2023;304:207–18. doi: 10.1016/j.ejor.2021.12.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Caygill R, Peardon M, Waite C, Wright J. Comparing a longitudinal integrated clerkship with traditional hospital-based rotations in a rural setting. Med Teach. 2017;39:520–6. doi: 10.1080/0142159X.2017.1297893. [DOI] [PubMed] [Google Scholar]
- 13.Shrivastava SR, Shrivastava PS. Employing adaptt tool to respond to the rising COVID-19 caseload in the European region. Med Sci. 2020;9:524–5. [Google Scholar]
- 14.Richmond A. The chicken and the egg: Clinical reasoning and uncertainty tolerance. Med Educ. 2022;56:696–8. doi: 10.1111/medu.14814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McQuide PA, Finnegan A, Terry KM, Brown A, Toure CO, Tessougue J, et al. Applying WHO COVID-19 workforce estimate tools remotely in an African context: A case report from Mali and Kenya. Hum Resour Health. 2022;19(Suppl 1):111. doi: 10.1186/s12960-021-00653-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Al-Aamri AK, Al-Harrasi AA, AAl-Abdulsalam AK, Al-Maniri AA, Padmadas SS. Forecasting the SARS COVID-19 pandemic and critical care resources threshold in the Gulf Cooperation Council (GCC) countries: Population analysis of aggregate data. BMJ Open. 2021;11:e044102.. doi: 10.1136/bmjopen-2020-044102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cooper I, Mondal A, Antonopoulos CG. A SIR model assumption for the spread of COVID-19 in different communities. Chaos, solitons, and fractals. Chaos Solitons Fractals. 2020;139:110057.. doi: 10.1016/j.chaos.2020.110057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Weissman GE, Crane-Droesch A, Chivers C, Luong T, Hanish A, Levy MZ, et al. Locally informed simulation to predict hospital capacity needs during the COVID-19 Pandemic. Ann Intern Med. 2020;173:21–8. doi: 10.7326/M20-1260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Organization. WH Files from WHO Europe at World Health Organization - Adaptt Surge Planning Support Tool. 2020 Available from: https://euro.sharefile.com/share/view/scef08a92a9d43b68/fo62fb4f-ba90 -. [Google Scholar]
- 20.Arora VM, Chivu M, Schram A, Meltzer D. Implementing physical distancing in the hospital: A key strategy to prevent nosocomial transmission of COVID-19. J Hosp Med. 2020;15:290–1. doi: 10.12788/jhm.3434. [DOI] [PubMed] [Google Scholar]
- 21.Organization. WH COVID-19: Launch of new WHO tools to help hospitals manage the rapid arrival of patients. 2020 Available from: www.euro.who.int/fr/health-topics/health-emergencies/coronavirus?covid-19/news/news/2020/4/new-who-tools-launched-to-help-hospitals?manage-surge-in-covid-19-patients. [Last accessed on 2020 Apr 01]. [Google Scholar]
- 22.World Health Organization Novel Coronavirus (2019-nCoV): Strategic preparedness and response plan 2019 [Google Scholar]
- 23.World Health Organization . World Health Organization; Regional Office for Europe: 2020. Hospital readiness checklist for COVID-19 interim version February 24 2020. [Google Scholar]