

Abstract
Benign laryngeal lesions like vocal nodules, vocal polyp, vocal fold cysts are mostly found in patients complaining of change in voice. S/Z ratio has become the most frequently used clinical tool to assess phonatory mechanics. This study shows the pre-treatment and post-treatment comparison of S/Z ratios in patients with benign laryngeal lesions. To evaluate the outcome of microlaryngeal surgery in patients with benign laryngeal lesions using S/Z ratio as an outcome parameter. During this study, 65 patients with complaints of change in voice, with clinical evidence of benign laryngeal lesions underwent microlaryngeal surgery. Improvement in symptoms were measured preoperatively and postoperatively using S/Z ratio. This ratio was calculated by asking the patient to to maximally sustain ‘S’ and ‘Z’, repeated thrice. S/Z ratio was calculated by dividing the maximum duration for which /S/ was sustained by the maximum duration for which /Z/ was sustained. A ratio of more than 1.4 suggested a vocal cord disorder. There was statistically significant difference observed in S/Z ratio values, from pre-treatment to 6 months post-treatment, with P value 0.001. Pre and post treatment assessment of patients with benign vocal fold lesions showed significant improvement in S/Z ratio postoperatively. It is the simplest and a reliable objective method of voice assessment and can also be used in assessing the outcome of the treatment.
Keywords: Microlaryngeal surgery, Benign laryngeal lesions, S/Z ratio, Phonatory mechanics
Introduction
The normal phonatory phenomenon requires proper structure, physiology, coordination, and efficiency of the larynx. A complication in any of these properties has adverse effects on phonation.
The term dysphonia is often used interchangeably with hoarseness. Hoarseness is a symptom of a change in voice quality reported by patients, whereas dysphonia indicates impairment of voice quality as recognized by a clinician [8].
The most widely accepted and predominant cause of hoarseness is benign lesions of vocal folds, which affect vibratory vocal fold function and result in significant dysphonia. The treatment for such lesions includes a combination of microlaryngeal surgery, voice therapy, low dose steroid therapy, and lifestyle modifications like quitting smoking and elimination of.
behaviour aggravating phonotrauma. Contributing factors like allergy, reflux, and psychological issues need to be addressed.
A detailed evaluation includes visualization of the larynx and voice assessment. Voice assessment is an important part of the examination for laryngeal pathology. Various methods of both subjective and objective analysis are used for voice analysis. The simplest of all objective methods are the maximum phonation time (MPT) and S/Z score.
S/Z score is the ratio of maximum sustained time for a speaker to make both /S/ and /Z/ sound. A normal speaker can usually maintain the sound for approximately the same amount of time for both /S/ and voiced /Z/ consonant, giving a ratio of approximately 1:1 [8]. Abnormalities that interfere with vocal fold vibration or which affect glottic closure reduce the /Z/ value but do not significantly affect the /S/ time, thus increasing the ratio. This simple test is used quite widely in clinical practice. The dysphonic subjects with laryngeal pathology usually have S/Z ratios above 1.4.
According to Boone [2], in a person with normal vocal cords S/Z ratio approximates to 1, as the normal vocal cords prolong the voiceless /S/ and voiced /Z/ phonemes for the same length of time. Eckel and Boone [1] hypothesized that it would be difficult to prolong the voiced /Z/ for the same duration as voiceless /S/ for patients with laryngeal pathology, due to a decrement in glottal efficiency and such patients with vocal cord pathology may have a ratio more than 1.0.
Hence, our study aims to evaluate the outcome of microlaryngeal surgery in patients with benign laryngeal lesions using S/Z ratio as an outcome parameter.
Methodology
Source of Data
Those patients of either sex, in age group 13–65 years, with benign laryngeal lesions undergoing Microlaryngeal surgery, were selected from teaching hospitals attached to JJM Medical College; Bapuji Hospital and Chigateri Government Hospital, Davangere.
Study Design
Prospective, follow-up, comparative (pre & post treatment) study.
Study Duration
March 2021 to August 2022.
Sample Size
65 patients attending OPD with symptoms of change in voice and found to have clinical evidence of benign laryngeal lesions, who fulfilled all inclusion and exclusion criteria were selected.
Sampling Criteria
Inclusion Criteria
1. Patients with benign laryngeal lesions.
2. Either sex.
3. Patients between 13–65 years of age.
Exclusion Criteria
1. Patients with comorbid conditions (hepatic,cardiac,endocrine).
2. Patients with suspected malignancy.
3. Patient who were not willing to take part in the study.
Data Collection Method
Patients who presented to ENT OPD with symptoms of change in voice were subjected to routine ENT history taking and examination. They also underwent indirect laryngoscopy and from those patients found to have clinical evidence of benign laryngeal lesions, a written informed consent was taken from those who were willing to take part in the study. Patients with vocal polyps, vocal cord cysts, vocal nodules and vocal cord papilloma underwent.
microlaryngeal surgery. Aerodynamic analysis was done to evaluate glottic efficiency preoperatively and 6 months postoperatively using S/Z ratio.
S/Z ratio: Patient was asked to take a deep breath and then to sustain the sound ‘s’ for as long as possible, at a comfortable pitch and loudness on one exhalation, without straining. The time was recorded as first ‘S’. The procedure was repeated similarly for the sound ‘Z’. The procedure was repeated for a total of three attempts. S/Z ratio was calculated by dividing the maximum duration for which /S/ was sustained by the maximum duration for which /Z/ was sustained. A ratio of 1.4 was considered as abnormal or indicating a degree of vocal cord dysfunction (Tables 1, 2, 3 and 4).
Table 1.
Age distribution
| Age (years) | No. of Cases (N) | Percentage (%) |
|---|---|---|
| 11–20 | 09 | 13.8 |
| 21–30 | 15 | 23.1 |
| 31–40 | 17 | 26.2 |
| 41–50 | 16 | 24.6 |
| 51–60 | 06 | 9.2 |
| 61–70 | 02 | 3.1 |
| Total | 65 | 100.0 |
| Mean ± SD | 36.11 ± 13.36 | |
| Range | 13–68 | |
Table 2.
Gender distribution
| Sex | No. of Cases (N) | Percentage (%) |
|---|---|---|
| Female | 39 | 60.0 |
| Male | 26 | 40.0 |
| Total | 65 | 100.0 |
Inference: Most of the patients belonged to 31–40 years age group
Table 3.
Diagnosis
| Diagnosis | No. of Cases (N) | Percentage (%) |
|---|---|---|
| Bilateral vocal nodules | 25 | 38.5 |
| Left vocal fold cyst | 05 | 7.7 |
| Left vocal fold papilloma | 03 | 4.6 |
| Left vocal polyp | 11 | 16.9 |
| Right vocal fold cyst | 04 | 6.2 |
| Right vocal fold papilloma | 06 | 9.2 |
| Right vocal polyp | 11 | 16.9 |
| Total | 65 | 100.0 |
Inference: The most common presentation in this study was bilateral vocal fold nodules
Table 4.
S/Z ratio comparison from pre-treatment to 6 months post-treatment
| S/Z Ratio | (Mean ± SD) | Range | P Value |
|---|---|---|---|
| Pre-treatment | 1.58 ± 0.17 | 1.3–1.9 | 0.001 (S) |
| 6 months post-treatment | 1.06 ± 0.11 | 0.8–1.3 |
Inference: Statistically significant reduction is observed for S/Z ratio values from pre-treatment to 6 months post-treatment
Statistical Analysis
Statistical analyses were performed using IBM SPSS Version 22 for Windows. Categorical data was represented in the form of frequency and percentage. Association of variables was assessed with Chi Square test. Quantitative data will be represented as Mean & Sd. Comparison between pre and post treatment was done with paired t Test. P value of < 0.05 was considered statistically significant.
Results
26.2% were in age group of 31–40 years, 24.6% in 41–50 years, 23.1% in 21–30 years, 13.8% in 11–20 years, 9.2% in 51–60 years and 3.1% in 61–70 years age groups. Most of the patients belonged to 31–40 years age group.
60% of patients (39 cases) were females and 40% (26 cases) were males. Significant female preponderance was noted.
38.5% (25 cases) presented with bilateral vocal nodules, 16.9% (11 cases) with left vocal polyp, 16.9% (11 cases) with right vocal polyp, 9.2% (6 cases) with right vocal fold papilloma, 7.7% (5 cases) with left vocal fold cyst, 6.2% (4 cases) with right vocal fold cyst and 4.6% (3 cases) with left vocal fold papilloma. The most common presentation in this study was bilateral vocal fold nodules.
The mean S/Z ratio in patients with bilateral vocal nodules reduced significantly from 1.52(preoperatively) to 1.25(postoperatively), in left vocal fold cyst from 1.61 to 1.45, in left vocal fold papilloma from 1.53 to 1.25, in left vocal fold polyp from 1.47 to 1.25, in right vocal fold cyst from 1.31 to 1.27, in right vocal fold papilloma from 1.46 to 1.25 and in right vocal polyp from 1.44 to 1.25 (Fig. 1).
Fig. 1.
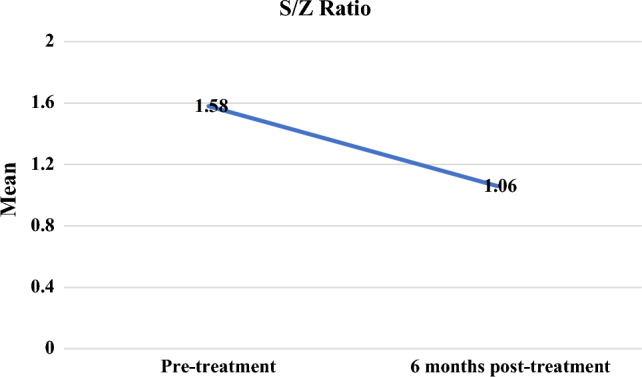
Pre and post treatment S/Z ratio
Statistically significant reduction was observed for S/Z ratio values from pre-treatment to 6 months post-treatment.
Discussion
Vocal fold benign lesions like vocal nodules, vocal fold polyps and vocal fold cysts are significant, because they alter the vocal fold vibratory function causing voice disorders. Microlaryngeal surgery is applied to those lesions, which are not responsive to voice therapy or medical therapy. Goals of treatment are complete excision of lesions and thereby restoring the better vocal cord functional levels. Pre operative and post operative assessment by s/z ratio will help to evaluate the quality of the treatment.
Dr.Sorenson [3] examined the S/Z ratio in 11 children with vocal cord pathologies. Results indicated the group with vocal cord pathologies had significantly lower maximally sustained /Z/ production and significantly higher overall s/z ratio (Mean S/Z ratio of 1.24). However, after treatment the mean s/z ratio of the subjects reduced to 1.06.
Dr.Rastatter and Dr.Hyman [4] examined the mean S/Z ratio in 16 subjects who were diagnosed with bilateral vocal fold nodules and was observed to be > 1.4. The subjects were enrolled for voice therapy for one month. Post-treatment the mean S/Z ratio in these subjects were observed to be 0.81.
Dr.Hufnagle [5] applied the s/z ratio in 123 dysphonic children with vocal nodules. Results showed mean s/z ratio of 1.2. The mean s/z ratio was examined post-treatment of these subjects and were observed to be 1.0.
Dr.Tait, Dr.Michel and Dr.Carpenter [6] observed the maximum phonation time (MPT) of the /s/ and /z/ phonemes of 15 children with vocal nodules. The mean s/z ratio was observed to be > 1.1. Post-treatment (voice rest), the s/z ratio was found to be < 1.
Dr.Larson, Dr.Mueller and Dr.Summers [7] examined the s/z ratio in 88 subjects with vocal cord pathologies and was observed to be 1.24. Post-treatment the s/z ratio of these subjects were observed to be < 1.
In this study, vocal fold nodules were the most common presentation. The vocal fold lesions prevent a complete glottic closure. Excision of the lesion resulted in complete glottic closure.
Complete glottic closure results in greater vocal fold contact because of a smooth edge, with generation of a greater subglottic pressure and better amplitude of cord vibration. The resulting equality of vocal fold mass and regular oscillation of each fold produces an improved voice. In our study, there is agreement with the above mentioned studies, in the usage of S/Z ratio as a reliable objective method for assessing the outcome of surgery in patients with benign laryngeal lesions.
Conclusion
Irrespective of age and gender, S/Z ratio is a simple and effective objective clinical test to diagnose benign laryngeal pathologies and provides interesting data about phonation dynamics. This ratio can be used as indicator for laryngeal valving and glottic efficiency. As the laryngeal pathology heals postoperatively, S/Z ratio is expected to normalize, indicating therapeutic progress hence making it an effective parameter to assess the outcome of microlaryngeal surgery in patients with benign laryngeal lesions.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by KBP, Dr. RAM, Dr. HAM, Dr. PJP The first draft of the manuscript was written by Dr. RAM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors have no relevant financial or nonfinancial interest to disclose.
Data Availability
The data used in this study was not used/published in any other publications.
Code Availability
The data was compiled and analyzed using IBM SPSS Version 22 for Windows.
Declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical Approval
The study was done after approval of the Institutional Ethics committee from JJM Medical College, Davangere, Karnataka, India in accordance with ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to Participate
Written informed consent was taken from all the patients.
Consent to Publication
All authors have reviewed the manuscript and approved the version to be published.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Eckel FC, Boone DR. The S/Z ratio as an indicator of laryngeal pathology. J Speech Hear Disord. 1981;46(2):147–149. doi: 10.1044/jshd.4602.147. [DOI] [PubMed] [Google Scholar]
- 2.Boone D (1997) The voice and voice therapy. Prentice-Hall, Englewood Cliffs
- 3.Sorenson DN, Parker PA. The voiced/voiceless phonation time in children with and without laryngeal pathology. Lang Speech Hear Sch. 1992;23:163–168. doi: 10.1044/0161-1461.2302.163. [DOI] [Google Scholar]
- 4.Rastatter MP, Hyman M. Maximum phoneme duration of /s/ and /z/ by children with vocal nodules. Lang Speech Hear Serv Sch. 1982;13:197–199. doi: 10.1044/0161-1461.1303.197. [DOI] [Google Scholar]
- 5.Hufnagle J, Hufnagle KK. s/z ratio in dysphonic children with and without vocal nodules. Lang Speech Hear Serv Sch. 1988;19:418–422. doi: 10.1044/0161-1461.1904.418. [DOI] [Google Scholar]
- 6.Tait NA, Michel JF, Carpenter MA. Maximum duration of sustained /s/ and /z/ in children. J Speech Hear Disord. 1980;45:239–246. doi: 10.1044/jshd.4502.239. [DOI] [PubMed] [Google Scholar]
- 7.Larson GW, Mueller PB, Summers PA. The effects of procedural variations on the s/z ratios of adults. J Commun Disord. 1991;24:135–140. doi: 10.1016/0021-9924(91)90017-D. [DOI] [PubMed] [Google Scholar]
- 8.Watkinson JC, Clarke RW. Scott-Brown’s otorhinolaryngology head and neck surgery. Boca Raton: CRC Press; 2018. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used in this study was not used/published in any other publications.
The data was compiled and analyzed using IBM SPSS Version 22 for Windows.