

Abstract
Among the various anatomical landmarks during neck dissection, digastric muscle is one of the most important. It is well known that all important blood vessels in neck lies deep to digastric. Thus, it acts as a safety landmark during neck dissection. In this article we describe a variation in vascular anatomy with relation to posterior belly of digastric that has not been reported so far during live surgery. Surgeon performing neck dissection should have a detailed knowledge of anatomy and infrequent anatomical variation. The knowledge of current anatomical variation will avoid torrential bleed during neck dissection and preserve the artery for vascular related procedures.
Keywords: Carotid arteries, Carotid artery injury, Neck muscle, Neck dissections
Brief Communication
Neck dissection is one of the common procedures done by surgeons over the last two centuries. It poses various challenges more so when anatomical variation happens. Digastric muscle marks the boundary of submandibular triangle of neck and it has two bellies. Among them, the posterior belly is an important anatomical landmark during neck surgeries especially during neck dissections. It is considered as a safety muscle, as all the great vessels on neck lie deep to it thus help to avoid potential major surgical complications. It is well known that common facial vein may be the only major vascular structure that needs to be tackled during dissection around this region [1]. We report an anomalous major artery encountered in this region.
A 40 year old man was diagnosed to have carcinoma right lateral border of tongue cT2N0M0. He underwent wide local excision of the lesion and selective neck dissection (Level 1–4). During neck dissection we noticed an anomalous course of external carotid artery (ECA) which was crossing over, lateral to the posterior belly of digastric muscle and then entering the parotid gland (Fig. 1). Facial artery was noted running medial to digastric muscles.
Fig. 1.
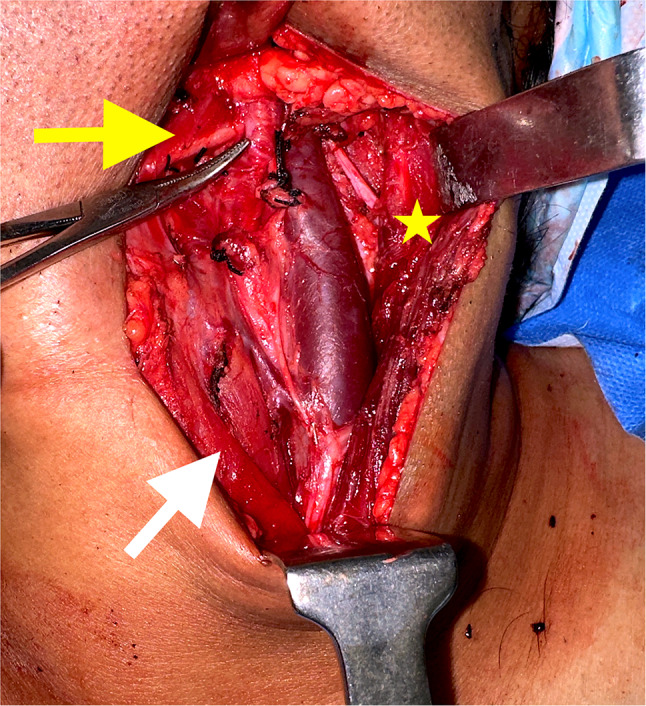
Photo showing lateral relation of ECA (pointed by haemostat) with posterior belly of digastric muscle (Yellow arrow). White arrow points omohyoid muscle, “Star” points sternocleidomastoid muscle close to spinal accessory nerve
This anomaly is rare and has been reported only in cadaveric studies, by Kawai K on 1086 head sides. The study noted that 95.76% of cases had ECA deep to the posterior belly of digastric muscle and the stylohyoid muscle, and between the muscle in 3.87% of cases. ECA lateral to digastric muscle was found only in 0.37% of the cases. Among the four anomalous course reported, with ECA running lateral to digastric, three had facial artery arising and running medial to digastric as in our case, the one had a lateral course [2].
The carotid arteries typically follow a relatively predictable course in the neck. Abnormalities in branching pattern of ECA has been well recognised. However, abnormalities in variations in the course of the carotid arteries, needs to be kept in mind, from surgical point of view. To the best of our knowledge, this is the first report of an ECA positioned lateral to the digastric muscle encountered during neck dissection in a live patient. Preoperative imaging studies, such as magnetic resonance imaging and contrast enhanced computed tomography, may help identify the anatomical relationships of carotid artery with digastric muscle.
It is worth noting that, though this variation in the course of the ECA can present challenge, it can be easily managed during operative procedure if one is aware of the variation. Hence awareness of these variations, regardless of the surgeon’s level of experience, is crucial to avoid injury of vessel and related sequelae.
Abbreviation
- ECA
External carotid artery
Author Contributions
Concept and design-JR; Acquisition of data-JR, PV; Drafting the article-JR, PV; Final approval-JR.
Funding
Nil.
Declarations
Conflict of interest
None.
Ethical Approval
Not obtained due to nature of study.
Informed Consent
Obtained from patient.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Wistermayer P, Anderson KG. (2023) Radical neck dissection. [Updated 2023 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls publishing. Available from: www.ncbi.nlm.nih.gov/books/NBK563186/ [PubMed]
- 2.Kawai K. Anomalous course of the external carotid artery. Anat Sci Int. 2016;91:334–340. doi: 10.1007/s12565-015-0304-z. [DOI] [PubMed] [Google Scholar]