

Abstract
The inflammatory process involving the maxillary sinus is often exacerbated by a functional obstruction due to laterally displaced uncinate process which obstructs the infundibulum and the natural ostium. Physiologically the drainage pathway may be adequate but during periods of inflammation resulting in nasal oedema, the ostium/infundibulum interface is inadequate, preventing adequate ventilation and drainage of the maxillary sinus. Incomplete removal of the uncinate process without including the natural ostium may result in failure and recurrence. This method of Middle meatal antrostomy that does not include the natural ostium of the maxillary sinus, leads to the missed ostium sequence and continued sinus disease. Here a case of missed maxillary sinus syndrome and its management is presented. A 28-year-old man with complaints of post nasal drip and Left facial pain for 4 months. 3 years prior the patient underwent functional endoscopic sinus surgery (FESS), following surgery patient had recurrent episode of sinusitis. Diagnostic nasal endoscopy revealed presence of mucopurulent discharge in left middle meatus, CT scan Paranasal sinus was suggestive of opacity in left maxillary sinuses and in left middle meatus with wide maxillary antrostomy. Revision FESS surgery was performed, where two ostia were present was converted into single wide middle meatal antrostomy using a back bitting forceps and microdebrider to avoid maxillary sinus mucus recirculation phenomenon. On follow up 1 year later, patient had no symptoms of repeated sinusitis. Missed maxillary sinus ostium syndrome has to be recognized and timely addressed by joining the natural and surgically created ostia as single wide middle meatal antrostomy window.
Supplementary Information
The online version contains supplementary material available at 10.1007/s12070-023-04385-x.
Keywords: Maxillary sinus, Ostium, Syndrome, FESS
Background
The inflammatory process involving the maxillary sinus is often exacerbated by a functional obstruction due to laterally displaced uncinate process which obstructs the infundibulum and the natural ostium. Physiologically the drainage pathway may be adequate but during periods of inflammation resulting in nasal oedema, the ostium/infundibulum interface is inadequate, preventing adequate ventilation and drainage of the maxillary sinus. Incomplete removal of the uncinate process without including the natural ostium may result in failure and recurrence. This method of Middle meatal antrostomy that does not include the natural ostium of the maxillary sinus, leads to the missed ostium sequence and continued sinus disease.
Here a case of missed maxillary sinus syndrome and its management is presented.
Case Presentation
A 28-year-old man with complaints of post nasal drip and Left facial pain for 4 months. There was previous history of repeated sinusitis. 3 years prior, patient underwent functional endoscopic sinus surgery and left middle meatal antrostomy was done. Diagnostic Nasal endoscopy revealed presence of mucopurulent discharge in the left middle meatus. Computerized tomography of the paranasal sinuses was suggestive of opacity in left maxillary sinuses and in the left middle meatus (Fig. 1), wide patent left maxillary antrostomy. The patient was treated with antibiotic and oral steroids for 2 weeks prior to surgery. The patient underwent revision functional endoscopic sinus surgery under local anaesthesia with intravenous sedation.
Fig. 1.
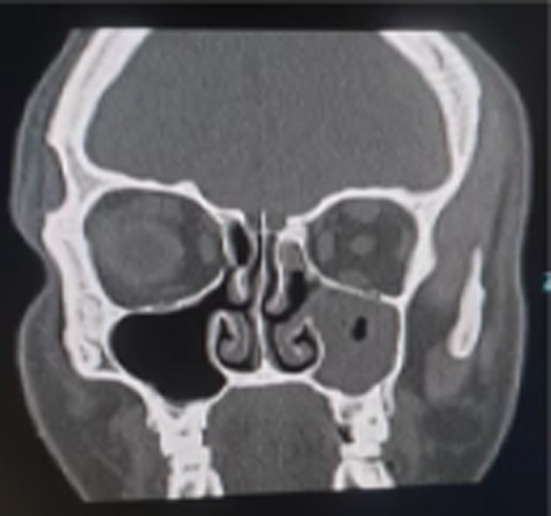
CT Scan of paranasal Sinuses showing Left maxillary Sinusitis
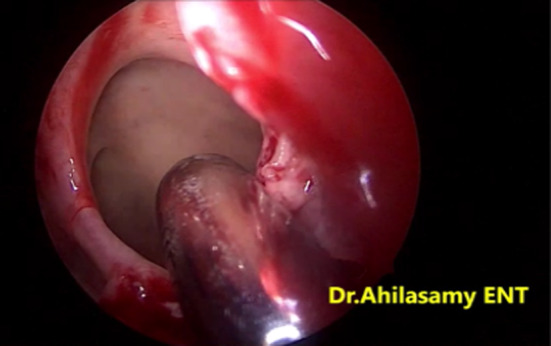
Intraoperative findings was suggestive of a healed previously performed middle meatal antrostomy (MMA) in the posterior part of the left middle meatus (Fig. 2), there were no polypoidal changes seen as suggested as per CT scan of Paranasal sinuses. A distinct, oblique oval-shape maxillary sinus ostium was located anterior to the previously created antrostomy site. This finding represents a case of a "missed maxillary sinus ostium."(Video-1). This was not expected before. The antero-inferior uncinate remnants of the previous surgery was removed.
Fig. 2.

Previous Middle meatal antrostomy (Arrow)
The two ostia were then made into single wide middle meatal antrostomy using a back bitting forceps (Fig. 3) and microdebrider (Fig. 4) to avoid maxillary sinus mucus recirculation phenomenon. No postoperative nasal packing was done. Saline nasal douching started from 2nd postoperative day, continued for 2 weeks. On follow up 1 year later, patient had no symptoms of repeated sinusitis. Diagnostic nasal endoscopy was suggestive of wide patent left maxillary middle meatal antrostomy site (MMA) well healed and epithelialize. (Fig. 5).
Fig. 3.

Remnant uncinate is removed using backbiting forceps
Fig. 4.
Septum in between the two ostia is removed using microdebrider
Fig. 5.

Wide single middle meatal antrostomy
Maxillary sinus ventilation and mucocillary drainage (from anterior, posterior, medial, lateral wall & roof) of the secretion follow a stellate pattern, starting from the floor of the maxillary sinus eventually draining in to the osteomeatal complex. Along with anterior ethmoids, frontal sinuses the mucocillary secretions pass towards the nasopharynx.
Maxillary sinus recirculation phenomenon occurs when the natural ostia of maxillary sinus is not communicated with the surgically created middle meatal antrostomy, patient presents with symptoms of chronic rhinosinusitis (persistent nasal obstruction and post nasal drip). Diagnostic nasal endoscopy with a 0° endoscope is useful to identify the pathology of the mucus originating from natural maxillary ostia site and flowing back in the surgically middle meatal antrostomy site predisposing to recirculation phenomenon.
In the traditional anterior to posterior approach by Messerklinger’s technique, the anterior-inferior uncinate remnant may hide the natural maxillary sinus ostium as it is obliquely placed, this finding can be missed leading to “missed ostium syndrome”. [1–3]
Discussion
Retrograde uncinectomy approach is a safe method to identifying the natural maxillary sinus ostium while performing middle meatal antrostomy (MMA).When patients complain of recurrent sinusitis symptoms following Functional endoscopic sinus surgery (FESS), recirculation phenomenon in the maxillary sinus may have to be considered as a causative factor for persistent nasal and sinus symptoms.
Setliff RC et al., Christmas DA et al. have described missed maxillary sinus ostium in their case study and clinical practice [4–6], which has to be recognized and timely addressed by joining the natural and surgically created ostia as single wide middle meatal antrostomy window.
Conclusion
Missed maxillary sinus ostium syndrome has to be recognized and timely addressed by joining the natural and surgically created ostia as single wide middle meatal antrostomy window.
Supplementary Information
Below is the link to the electronic supplementary material.
Author Contributions
AN Performed surgery, prepared the manuscript and patient preoperative and postoperative management and follow up. Major Contributor in writing he manuscript. RDK Review and editing the manuscript. SS Legends to Figures. SK patient postoperative follow up and helpline. AR Proof reading of the manuscript. All authors have read and agreed to the contents.
Data Availability
This is a case report and all the data pertaining to the case report have been included in this published article.
Declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical Approval
This is a case report, and case reports are exempted from the Institute ethics committee, RRMCH, Bangalore. This article was prepared in accordance with the Declaration of Helsinki. Written informed consent was obtained prior to publication of the case report from the patient.
Consent for Publication
Written informed consent for publication of the patient’s clinical details and clinical images was obtained from the patient.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Yanagisawa E. Atlas of rhinoscopy: endoscopic sinonasal anatomy and pathology. San Diego: Singular Thomson Learning; 2000. [Google Scholar]
- 2.Parsons DS, Stivers FE, Talbot AR. The missed ostium sequence and the surgical approach to revision functional endoscopic sinus surgery. Otolaryngol Clin North Am. 1996;29(1):169–183. doi: 10.1016/S0030-6665(20)30424-2. [DOI] [PubMed] [Google Scholar]
- 3.Owen RG, Kuhn FA. The maxillary sinus ostium: demystifying middle meatal antrostomy. Am J Rhinol. 1995;9:313–320. doi: 10.2500/105065895781808757. [DOI] [Google Scholar]
- 4.Setliff RC., III The hummer: a remedy for apprehension in functional endoscopic sinus surgery. Otolaryngol Clin North Am. 1996;29:95–104. doi: 10.1016/S0030-6665(20)30418-7. [DOI] [PubMed] [Google Scholar]
- 5.Christmas DA, Yanagisawa E, Joe JK. Transnasal endoscopic identification of the natural ostium of the maxillary sinus: a retrograde approach. Ear Nose Throat J. 1998;77:454–455. doi: 10.1177/014556139807700605. [DOI] [PubMed] [Google Scholar]
- 6.Christmas DA, Mirante JP, Yanagisawa E. The missed maxillary sinus ostium syndrome. Ear Nose Throat J. 2003;82(8):546–548. doi: 10.1177/014556130308200803. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
This is a case report and all the data pertaining to the case report have been included in this published article.