

Abstract
Background.
Although physical activity is widely recommended for reducing cardiovascular and all-cause mortality risks, females consistently lag behind males in exercise engagement.
Objectives.
To evaluate whether physical activity derived health benefits may differ by sex.
Methods.
In a prospective study of 412,413 U.S. adults (55% female, age 44±17 years) who provided survey data on leisure-time physical activity, we examined sex-specific multivariable-adjusted associations of physical activity measures (frequency, duration, intensity, type) with all-cause and cardiovascular mortality from 1997 through 2019.
Results.
During 4,911,178 person-years of follow up, there were 39,935 all-cause deaths including 11,670 cardiovascular deaths. Regular leisure-time physical activity compared to inactivity was associated with 24% (HR 0.76 [95% CI 0.73–0.80]) and 15% (0.85 [0.82–0.89]) lower risk of all-cause mortality in females and males, respectively (Wald F=12.0, sex interaction P<0.001). Males reached their maximal survival benefit of HR 0.81 from 300 min/week of moderate-to-vigorous physical activity, while females achieved similar benefit at 140 min/week and then continued to reach a maximum survival benefit of HR 0.76 also at ~300 min/week. Sex-specific findings were similar for cardiovascular death (Wald F=20.1, sex interaction P<0.001) and consistent across all measures of aerobic activity as well as muscle strengthening activity (Wald F=6.7, sex interaction P=0.009).
Conclusions.
Females compared to males derived greater gains in all-cause and cardiovascular mortality risk reduction from equivalent doses of leisure-time physical activity. These findings could enhance efforts to close the ‘gender-gap’ by motivating especially females to engage in any regular leisure-time physical activity.
Keywords: physical activity, mortality, sex differences
CONDENSED ABSTRACT
Females consistently lag behind males in physical activity engagement. We studied 412,413 U.S. adults and found that with ~300 min/week of moderate-to-vigorous leisure-time physical activity, the maximal mortality risk reduction achieved for males was 18% and for females 24%. Sex-specific findings were similar for cardiovascular death and consistent across all levels and measures of aerobic activity as well as muscle strengthening activity. The finding that females may derive especially pronounced survival benefits from equivalent doses of exercise could enhance efforts to close the ‘gender-gap’ by motivating especially females to engage in regular leisure-time physical activity.
INTRODUCTION
Although greater amounts of physical activity (PA) are associated with well-known reductions in cardiovascular and all-cause mortality, less than a quarter of all Americans meet the minimum guidelines for PA1 as recommended by the Centers for Disease Control and Prevention (CDC),2 and the American Heart Association/American College of Cardiology.3 Both sets of guidelines recommend a minimum 150 minutes per week of moderate PA or 75 minutes per week of vigorous PA, in addition to at least two days of muscle strengthening activities per week. While these recommendations are the same for males and females,2 it has been long known that females persistently lag behind males in physical activity engagement – manifesting a ‘gender gap’ that begins early in life and continues throughout adulthood.4,5 The extent to which this gap in levels of physical activity engagement may translate into differences in outcomes has been unclear. There are long-established and well-recognized sex differences in the physiologic response to PA, in thresholds of exercise tolerance, and in overall exercise capacity.6,7 In turn, it is possible that the degree of health benefit derived from physical activity could differ between sexes based on frequency, duration, intensity, type of exercise. Understanding any such differences could inform efforts to close the ‘gender gap’ and optimize PA related outcomes for all.
METHODS
All data and materials are publicly available from the CDC National Center for Health Statistics and are accessible online.8 The National Center for Health Statistics Disclosure Review Board approves the National Health Interview Survey (NHIS) study.9 Data analyses for this study were additionally approved by the Cedars-Sinai Medical Center institutional review board.
Study Sample
The CDC and the National Center for Health Statistics has conducted the NHIS with data collected from all 50 states and the District of Columbia (Supplemental Methods).10,11 We pooled data of a total of 646,279 adult participants of NHIS from years 1997 to 2017 and linked their records to the National Death Index records through December 31, 2019. We excluded participants with pre-existing diagnoses of coronary heart disease, myocardial infarction, stroke, emphysema, chronic bronchitis, or cancer (n=120,200), limitations in activities of daily living (n=6,332), missing data on physical activity (n=23,975), or missing data on follow-up status or key covariates (n=63,651). We further excluded individuals with outcomes occurring within the first 2 years of follow-up (n=19,708) to minimize the potential of reverse causation bias. The remaining 412,413 participants comprised our study sample.
Physical Activity, Clinical, and Outcomes Data
At each survey, a consistent set of standardized questions were used to ascertain frequency, duration, and type of regular physical activity engagement (Supplementary Methods).12,13 The frequency of the activity (times/week) was multiplied by the duration of the activity to provide the minutes per week of aerobic PA. To account for intensity, total weighted moderate-to-vigorous intensity aerobic physical activity (MVPA) was obtained by summing the duration of moderate intensity plus vigorous intensity multiplied by two.14,15 Data were also collected on sociodemographic characteristics, medical comorbidities, and self-rated health status (Supplemental Methods). All participants were under surveillance for all-cause and cardiovascular death.16
Statistical Analyses
For the primary outcomes analyses, we examined the association of PA measures with mortality using Cox proportional hazard regression models that accounted for the complex multistage sampling design of the survey (i.e. using weight, primary sampling units, and strata)17 and adjusted for covariates including age, race/ethnicity, body mass index, smoking status, hypertension, diabetes mellitus, alcohol consumption, education, income-to-poverty ratio, marriage status, access to medical care, self-reported health status, and chronic disease conditions. Before entering the model, unweighted PA measures were expanded using restricted cubic spline given potential nonlinear relationships. Sex differences in the associations between PA measures and mortality were assessed using likelihood ratio tests between models with and without parameters representing the interaction between sex and the cubic spline variables representing PA. The level of PA measure at which the maximal benefit was achieved for males was considered as the comparator referent. We secondarily assessed level of aerobic PA engagement based on frequency, duration per session, and intensity, where intensity was calculated as the proportion of vigorous PA out of total MVPA. Specifically, participants were categorized as physically inactive (<150 minutes per week [min/week] of MVPA) or physically active (≥150 min/week of MVPA), per the 2018 PA guideline.2 Physically active participants were then categorized by frequency, duration per session, and intensity of aerobic PA, and inactive participants were considered the referent for all analyses. Similarly, participants were also categorized by muscle strengthening activity as physically inactive (<2 sessions per week) or physically active (≥2 sessions per week). We then repeated multivariable-adjusted Cox models, as described above, to examine sex-specific associations for these categorized PA measures. We used the adjusted Wald test to evaluate the sex interaction by including the multiplicative terms of PA and sex.
In secondary analyses, we repeated analyses for females and males stratified by age grouped by decade or two decades. To account for the previously reported tendency of women to under-report PA duration compared to men,18 we conducted secondary analyses that incorporated sex-specific PA duration weights applied to both women (i.e., multiplied by 1.2) and men (i.e., multiplied by 0.8) (Supplementary Methods). We also repeated analyses assessing for any sex differences in outcomes associated with aerobic and muscle strengthening activity combined. To contextualize observed PA associations with mortality, we examined associations of PA with prevalent major risk factors (i.e., hypertension, diabetes) and measures of self-reported health (Supplemental Methods). In exploratory analyses, to assess whether sex-specific associations may have changed over time, we also repeated the primary analyses while considering PA data collected during year 2007 (instead of year 1997) as the ‘baseline’ assessment in relation to outcomes surveillance data collected through 2017. All analyses were performed using R v4.2.1 and STATA v16. A two-tailed P value <0.05 was considered significant.
RESULTS
Of the 412,413 participants in our study, 54.7% were female, 14.4% identified as Black, and 18.4% identified as Hispanic. The baseline mean age was 43.9±16.6 years with characteristics shown in Table 1. Frequency and distribution of characteristics by sex were similar for participants included in our analyses when compared to those who were excluded (Table S1). Over a total 4,911,178 person-years of follow up, there occurred 39,935 all-cause deaths (8.1 per 1000 person-years) including 11,670 cardiovascular deaths (2.4 per 1000 person-years).
Table 1.
Characteristics of the Study Participants
| Variable | Frequency and Proportion, No. (%)* | ||
|---|---|---|---|
| Females | Males | P value | |
| Total no. | 225689 | 186724 | - |
| Age, year | <0.001 | ||
| 18–44 | 122559 (56.1) | 106129 (59.0) | |
| 45–64 | 67989 (31.2) | 60290 (32.2) | |
| 65–85 | 35141 (12.5) | 20305 (8.6) | |
| Race and ethnicity | <0.001 | ||
| Hispanic | 41974 (13.7) | 34099 (14.8) | |
| Non-Hispanic Black | 35806 (12.6) | 23725 (11.0) | |
| Non-Hispanic White | 135435 (67.9) | 117985 (68.6) | |
| Other# | 12474 (5.6) | 10915 (5.4) | |
| Education level | 0.089 | ||
| < High School degree | 39731 (14.9) | 32710 (16.1) | |
| High School degree | 53978 (24.3) | 44833 (24.6) | |
| >High School degree | 131221 (60.4) | 108470 (58.8) | |
| Body mass index | <0.001 | ||
| <25 kg/m2 | 106095 (48.7) | 60120 (32.0) | |
| 25–29 kg/m2 | 66069 (28.5) | 83499 (44.2) | |
| ≥30 kg/m2 | 53525 (22.7) | 43105 (23.7) | |
| Hypertension | 51741 (20.9) | 40741 (20.8) | <0.001 |
| Diabetes | 12545 (4.9) | 10365 (5.1) | 0.92 |
| Smoking status | <0.001 | ||
| Never | 148904 (66.1) | 100307 (55.1) | |
| Former | 37290 (16.6) | 42121 (21.9) | |
| Current | 39326 (17.1) | 44130 (22.8) | |
| Alcohol use, days/week | <0.001 | ||
| 0 | 169389 (74.0) | 102651 (55.7) | |
| 1 | 25796 (11.8) | 32075 (17.0) | |
| ≥2 | 30504 (14.1) | 51998 (27.1) | |
| Chronic conditions, No. | <0.001 | ||
| 0 | 151369 (68.7) | 129007 (69.7) | |
| 1 | 59425 (25.3) | 46717 (24.7) | |
| ≥2 | 14895 (5.9) | 11000 (5.4) | |
| Self-rated health | <0.001 | ||
| Excellent | 70560 (33.2) | 64287 (36.1) | |
| Very good | 77895 (34.8) | 65037 (34.8) | |
| Good | 58034 (24.5) | 44102 (22.8) | |
| Fair/Poor | 16395 (6.3) | 11361 (5.3) | |
| Access to Medical Care† | 198110 (88.3) | 143277 (78.0) | <0.001 |
| Marriage status | <0.001 | ||
| Never married | 49859 (20.1) | 50983 (25.0) | |
| Married/living with partner | 115146 (61.8) | 104940 (64.7) | |
| Widowed/divorced/separated | 60237 (17.8) | 30485 (10.1) | |
| Unknown | 447 (0.1) | 316 (0.1) | |
| Income-to-poverty Ratio‡ | <0.001 | ||
| <1 | 33977 (11.1) | 20311 (8.7) | |
| 1–1.99 | 39120 (15.1) | 28061 (13.6) | |
| ≥2 | 122754 (60.7) | 116877 (66.0) | |
| Other§ | 29838 (12.9) | 21475 (11.6) | |
Abbreviations: BMI, body mass index; DM, diabetes mellitus.
Analyses of percent values were conducted using the adjustment of weights, primary sampling units, and strata. Variable categories may not sum to 100% because of truncation and unspecified category (i.e. refused, not ascertained, or don’t know).
This category included American Indian or Alaska Native; Native Hawaiian or other Pacific Islander; Asian; Hispanic or Latino; mixed races; refused to respond; or race unknown.
Place of usual source of medical care included clinic or health center, doctor’s office, hospital emergency room, hospital outpatient department and some other places.
Income-to-poverty Ratio was calculated by dividing top-coded total combined imputed family income by the U.S. Census Bureau’s poverty thresholds.
This category included unknown and undefinable conditions.
Sex Differences in Aerobic Physical Activity Associations with All-Cause Mortality
The baseline characteristics of physically active participants are shown in Table S2. Overall, 32.5% of females and 43.1% of males regularly engaged in aerobic PA, and all major measures of PA were significantly higher in males (Table 2, P for all <0.001). In particular, regular engagement for females and males was 10.3% and 15.2% for MPA (≥150 min/week) and was 28.3% and 38.9% for VPA (≥75 min/week), respectively. For women, regular PA compared to inactivity was associated with a 24% lower risk of all-cause mortality (HR 0.76 [95% CI 0.73, 0.80]). For men, regular PA compared to inactivity was associated with a reduction in all-cause mortality by 15% (0.85 [0.82, 0.89]), and this magnitude of benefit was significantly less than that seen for women (Table 3, Wald test, F=12.0, Pinteraction <0.001).
Table 2.
Physical Activity Type and Duration in NHIS Participants
| Variable | Frequency and Proportion, No. (%)* | ||
|---|---|---|---|
| Females | Males | P value | |
| MVPA, min/week | |||
| Mean value | 206 | 353 | <0.001 |
| <150 | 155978 (67.3) | 107065 (56.4) | <0.001 |
| 150–299 | 20423 (9.6) | 18731 (10.3) | |
| ≥300 | 49288 (22.9) | 60928 (33.1) | |
| MPA, min/week | |||
| Mean value | 53 | 84 | <0.001 |
| <150 | 203584 (89.6) | 158610 (84.7) | <0.001 |
| 150–299 | 12785 (6.0) | 14115 (7.6) | |
| ≥300 | 9320 (4.3) | 13999 (7.5) | |
| VPA, min/week | |||
| Mean value | 76 | 135 | <0.001 |
| <75 | 164914 (71.5) | 115272 (60.9) | <0.001 |
| 75–149 | 23305 (10.9) | 21944 (12.1) | |
| ≥150 | 37470 (17.4) | 49508 (26.8) | |
| Intensity (VPA/MVPA), % # | |||
| Mean value | 29.3 | 38.7 | <0.001 |
| <25 | 644 (0.3) | 974 (0.5) | <0.001 |
| 25–49 | 3356 (1.5) | 3900 (2.1) | |
| 50–74 | 27296 (12.9) | 28031 (15.3) | |
| 75–100 | 38415 (17.8) | 46754 (25.5) | |
| Muscle strengthening PA, sessions/week | |||
| Mean value | 0.85 | 1.25 | <0.001 |
| 0 | 182984 (79.9) | 135443 (72.0) | <0.001 |
| 2–3 | 26574 (12.5) | 27932 (15.3) | |
| 4–5 | 7982 (3.8) | 12075 (6.5) | |
| ≥6 | 8149 (3.6) | 11274 (6.0) | |
Abbreviations: MVPA, moderate-to-vigorous intensity physical activity; MPA, moderate intensity physical activity; VPA, vigorous intensity physical activity.
Analyses of percent values and mean values account for the complex multistage sample design of the survey using weights, primary sampling units, and strata. Variable categories may not sum to 100% because of truncation.
Only physically active participants (i.e. MVPA>0 min/week) were shown.
Table 3.
Association of Physical Activity with All-Cause Mortality by Sex
| All-cause Deaths | Females | Males | P Interaction | ||
|---|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | ||
| Aerobic Physical activity | |||||
| Inactive | Referent | - | Referent | - | |
| Active* | 0.76 (0.73, 0.80) | <0.001 | 0.85 (0.82, 0.89) | <0.001 | <0.001 |
| Frequency, sessions/week | |||||
| Inactive | Referent | - | Referent | - | |
| 1–5 | 0.71 (0.65, 0.76) | <0.001 | 0.84 (0.78, 0.89) | <0.001 | <0.001 |
| 6–9 | 0.74 (0.70, 0.79) | <0.001 | 0.83 (0.78, 0.88) | <0.001 | |
| ≥10 | 0.80 (0.76, 0.85) | <0.001 | 0.85 (0.80, 0.90) | <0.001 | |
| Duration of session, min | |||||
| Inactive | Referent | - | Referent | - | |
| <15 | 0.80 (0.75, 0.86) | <0.001 | 0.84 (0.79, 0.89) | <0.001 | 0.063 |
| 15–29 | 0.84 (0.77, 0.91) | <0.001 | 0.91 (0.84, 0.98) | 0.025 | |
| 30–59 | 0.73 (0.69, 0.78) | <0.001 | 0.78 (0.74, 0.83) | <0.001 | |
| ≥60 | 0.78 (0.73, 0.83) | <0.001 | 0.79 (0.74, 0.85) | <0.001 | |
| Intensity (VPA/MVPA), % | |||||
| Inactive | Referent | - | Referent | - | |
| <25 | 0.65 (0.51, 0.81) | <0.001 | 0.78 (0.64, 0.96) | 0.020 | 0.007 |
| 25–49 | 0.70 (0.62, 0.79) | <0.001 | 0.81 (0.73, 0.90) | <0.001 | |
| 50–74 | 0.75 (0.71, 0.80) | <0.001 | 0.83 (0.78, 0.88) | <0.001 | |
| 75–100 | 0.78 (0.75, 0.82) | <0.001 | 0.82 (0.78, 0.86) | <0.001 | |
| Muscle Strengthening Activity | |||||
| Inactive | Referent | - | Referent | - | |
| Active* | 0.81 (0.76, 0.85) | <0.001 | 0.89 (0.85, 0.94) | <0.001 | 0.005 |
| Frequency, sessions/week | |||||
| Inactive | Referent | - | Referent | - | |
| 2–3 | 0.74 (0.69, 0.80) | <0.001 | 0.86 (0.81, 0.92) | <0.001 | <0.001 |
| 4–5 | 0.80 (0.73, 0.88) | <0.001 | 0.89 (0.81, 0.97) | 0.014 | |
| ≥6 | 0.91 (0.85, 0.98) | 0.008 | 0.96 (0.90, 1.03) | 0.27 | |
Abbreviations: MVPA, moderate-to-vigorous intensity physical activity; MPA, moderate intensity physical activity; VPA, vigorous intensity physical activity; HR, hazard ratio; CI, confidence interval. All models accounted for the multi-staged survey sample design and were adjusted for total MVPA, muscle strengthening PA (i.e., frequency) and covariates that included age, race/ethnicity, body mass index, smoking status, hypertension, diabetes mellitus, alcohol consumption, education, income-to-poverty ratio, marriage status, access to medical care, self-rated health, and chronic disease conditions.
Physically active adults were then stratified by frequency, duration, and intensity of physical activity.
In dose-dependent analyses for the entire cohort, the benefit of PA on all-cause mortality peaked at ~300 min/week of MVPA and then plateaued (Figure S1). The greatest mortality benefit in males was achieved at 300 min/week of MVPA with an 18% lower hazard in all-cause mortality. Women derived a similar magnitude of benefit at 140 minutes/week of MVPA, and continued to benefit with increasing minutes/week of MVPA until the greatest benefit of 24% lower hazard (0.76 [0.72, 0.80]) was achieved at ~300 min/week (Figure 1). When examining the relationship specifically for VPA and all-cause mortality, the sex difference was significant: the greatest benefit was seen in males who engaged in 110 min/week of VPA, with a 19% lower hazard in all-cause mortality (0.81 [0.77, 0.85]); by comparison, females derived the same benefit from only 57 min/week of VPA (Likelihood ratio test, χ2=12.8, P=0.004). Although the benefit of VPA reached a plateau beyond 110 min/week in males, further benefit was derived from more min/week of VPA in females (Figure S2). For females, the 110 min/week of VPA was associated with 24% lower hazard for all-cause mortality (0.76 [0.72, 0.80]) and while the absolute maximum benefit for females was reached at 120 min/week, the corresponding risk reduction was similar at 24% lower hazard (0.76 [0.72, 0.79]). Similarly, for MPA, females appeared to derive a greater mortality benefit per unit time spent engaging in this level of PA: for males the maximal benefit was seen at 90 min/week of MPA with a 20% reduction in all-cause mortality (0.80 [0.75, 0.84]), and for females the same magnitude of benefit was seen at 50 min/week of MPA (0.79 [0.75, 0.84], Figure S2) although the interaction term for this sex difference did not reach statistical significance (Likelihood ratio test, χ2=3.85, P=0.27). For females, 90 min/week of MPA was associated with 24% lower hazard for all-cause mortality (0.76 [0.71, 0.80]) and while the maximum benefit for females was reached at 97 min/week of MPA, the corresponding risk reduction was similar at 24% lower hazard (0.76 [0.71, 0.80]).
Figure 1. Sex-Specific Association of Moderate-to-Vigorous Aerobic Physical Activity with All-Cause Mortality.
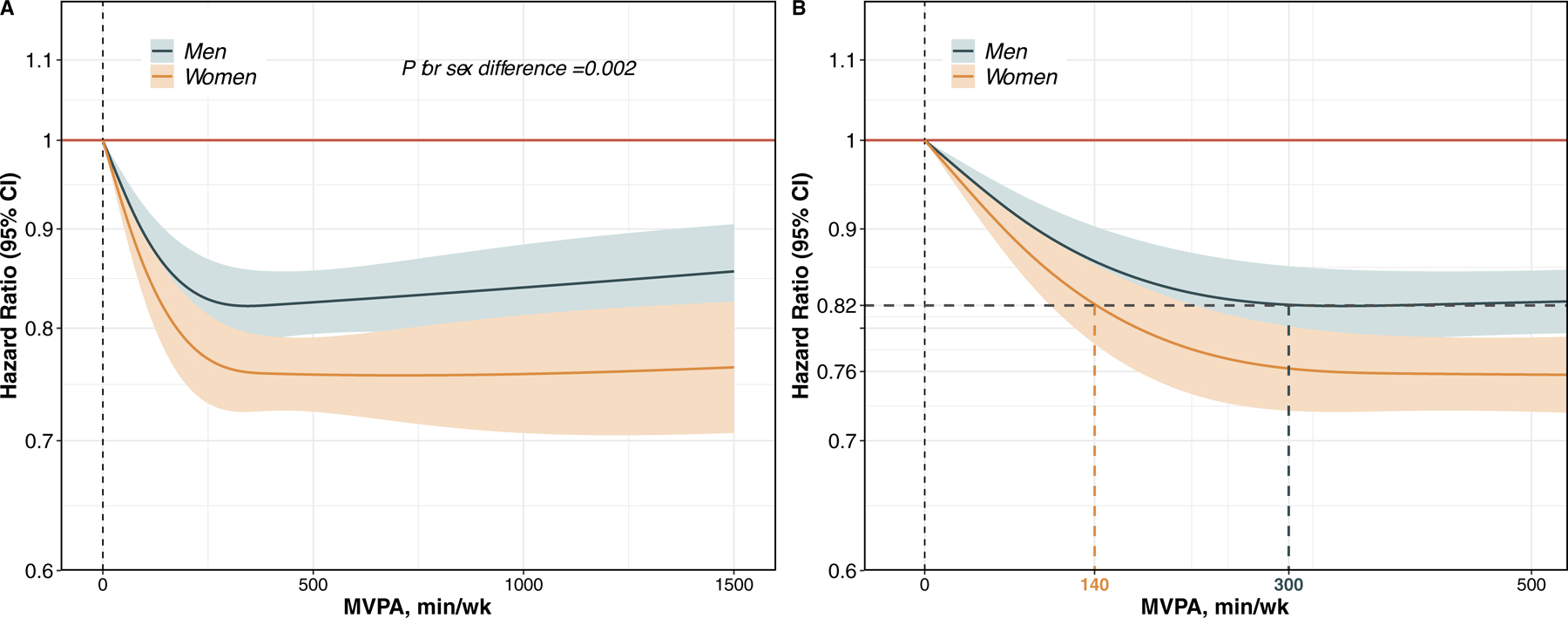
The multivariable-adjusted association of moderate-to-vigorous intensity aerobic physical activity (MVPA) duration with all-cause mortality is shown by sex overall (Panel A) and with focused comparison on the maximal survival benefit achieved for females compared to males (Panel B).
Sex Differences in Muscle Strengthening Activity Associations with All-Cause Mortality
Males compared to females were more likely to engage in muscle strengthening PA and with greater frequency (Table 2). Overall, 19.9 % of females and 27.8 % of males reported engaging in any regular muscle strengthening PA, with fewer sessions for females (average 0.85 sessions/week) than males (average 1.25 sessions/week). For males who performed regular muscle strengthening PA compared to inactivity, mortality risk was reduced by 11% (0.89 [0.85, 0.94]; for females, the mortality risk reduction was 19% (0.81 [0.76, 0.85]) and this sex difference was significant (Table 3, Wald test, F=7.9, P=0.005 for interaction). In dose-dependent analyses, males derived the greatest mortality benefit from engaging in 3 sessions/week of muscle strengthening PA with a 14% lower hazard in all-cause mortality; females derived equivalent or greater benefit by engaging in only a single muscle strengthening PA per week (Figure 2). For females compared to males engaging in 3 sessions/week of muscle strengthening PA, there was ~2-fold greater relative reduction in all-cause mortality.
Figure 2. Sex-Specific Association of Muscle Strengthening Physical Activity with All-Cause Mortality.
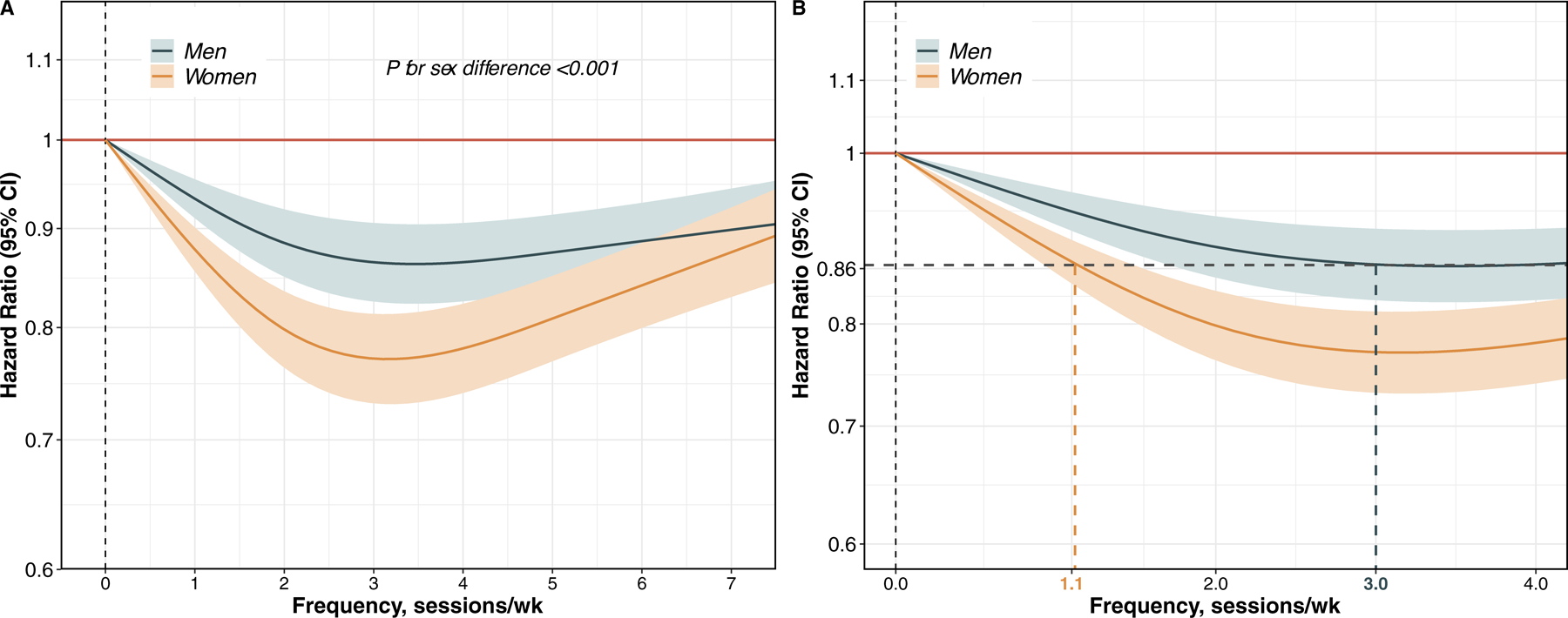
The multivariable-adjusted association of muscle strengthening frequency with all-cause mortality is shown by sex overall (Panel A) and with focused comparison on the maximal survival benefit achieved for females compared to males (Panel B).
Sex Differences in Physical Activity Associations with Cardiovascular Mortality
For cardiovascular mortality, engaging in regular aerobic PA compared to inactivity was associated with a risk reduction of 14% (0.86 [0.80, 0.93) for men and 36% (0.64 [0.58, 0.71]) for females; this sex difference was significant (Wald test, F=18.8, P<0.001 for interaction, Table S3). Similarly, engaging in regular muscle strengthening activities compared to inactivity was associated with a cardiovascular risk reduction of 11% (0.89 [0.80, 0.98] in men and 30% (0.70 [0.62, 0.78]) in females, and this 3-fold relative sex difference was also significant (Wald test, F=9.9, P=0.001 for interaction, Table S3).
Secondary Analyses
Across measures of aerobic PA frequency, duration per session, and intensity, the relative magnitude of survival benefit was consistently higher in females than in males for all-cause and cardiovascular mortality (Table 3 and Table S3). Due to slightly variations in the questions related to physical activity in the NHIS 1997 survey, compared to the surveys from subsequent years, we conducted sensitivity analyses excluding participant data from year 1997 and findings remained consistent (Table S4). In analyses that age-stratified results by decade and then by two decades (Tables S5 and S6), the magnitude of PA related mortality risk reduction was consistently greater in females than males particularly for middle aged individuals (i.e. age 40–59 years, P<0.05 for interaction); within the age <40 or ≥60 year strata, the magnitude of sex difference was attenuated (P>0.05 for interaction, Tables S5 and S6). In secondary analyses accounting for potential under-reporting of PA in women compared to men, results were consistent with those of primary analyses (Table S7 and Figure S3). When considering regular engagement in both aerobic physical activity and muscle-strengthening activity combined, in an additive manner, we observed slightly greater risk reduction in women (0.72 [0.67, 0.87]) and men (0.76 [0.71, 0.87]) for all-cause mortality although this difference was not statistically significant (Table S8). In analyses of PA and self-reported health status, we found that both aerobic PA and muscle strengthening PA were associated with lower odds of self-rated poorer health, indicating a positive relationship with perceived quality of life; these associations also did not significantly differ by sex (Table S9). In cross-sectional analyses of PA and risk factors, we found that PA engagement was associated with lower odds of prevalent diabetes in both sexes, to varying degrees (Table S10). Interestingly, PA engagement was associated with lower odds of prevalent hypertension in females but higher odds in males; notwithstanding the limitations of cross-sectional analyses, this finding may represent reverse causality (i.e. men with a diagnosis of hypertension may be more motivated to exercise).
Exploratory Analyses
To examine the extent to which sex-specific associations may have changed over time, we repeated analyses of PA measures and all-cause mortality while considering year 2007 as the ‘baseline’ year of PA data collection (instead of year 1997) with ~10 years of outcomes surveillance through year 2017 (instead of ~20 years’ surveillance). Results of these analyses were similar in directionality of sex difference to those of the primary analyses for both overall aerobic PA and muscle strengthening activity measures, although the magnitude of differences was attenuated in the setting of fewer events accrued per category over the shorter follow-up period (Table S11).
DISCUSSION
In a population-scale nationally representative cohort of US adults, we observed evidence of substantial sex-differences in the relations of self-reported leisure time PA with survival benefit. While both sexes achieved a peak survival benefit at 300 min of weekly aerobic MVPA, females derived a 24% mortality reduction that was substantially greater than for than males who derived a 18% mortality reduction from the same degree of regular exercise; similarly, for any given dose of PA leading up to 300 min per week, females derived proportionately greater benefits than men. These findings were evident for both all-cause and cardiovascular-specific mortality. Importantly, the greater magnitude of PA-related survival benefit in females than males was consistently found across varied measures and types of PA including frequency, duration per session, and intensity of aerobic PA as well as frequency of muscle strengthening activities. Our results from this large representative population study not only highlight a sex differential response in health benefits from PA but suggest that females stand to especially gain in reduction of cardiovascular and all-cause mortality risk (Central Illustration). Such findings could be used to further motivate engagement in physical activity among larger segments of the female population and particularly in those individuals for whom time represents a barrier to exercise.
Central Illustration. Sex Differences in Physical Activity Associated Mortality Risk Reduction.
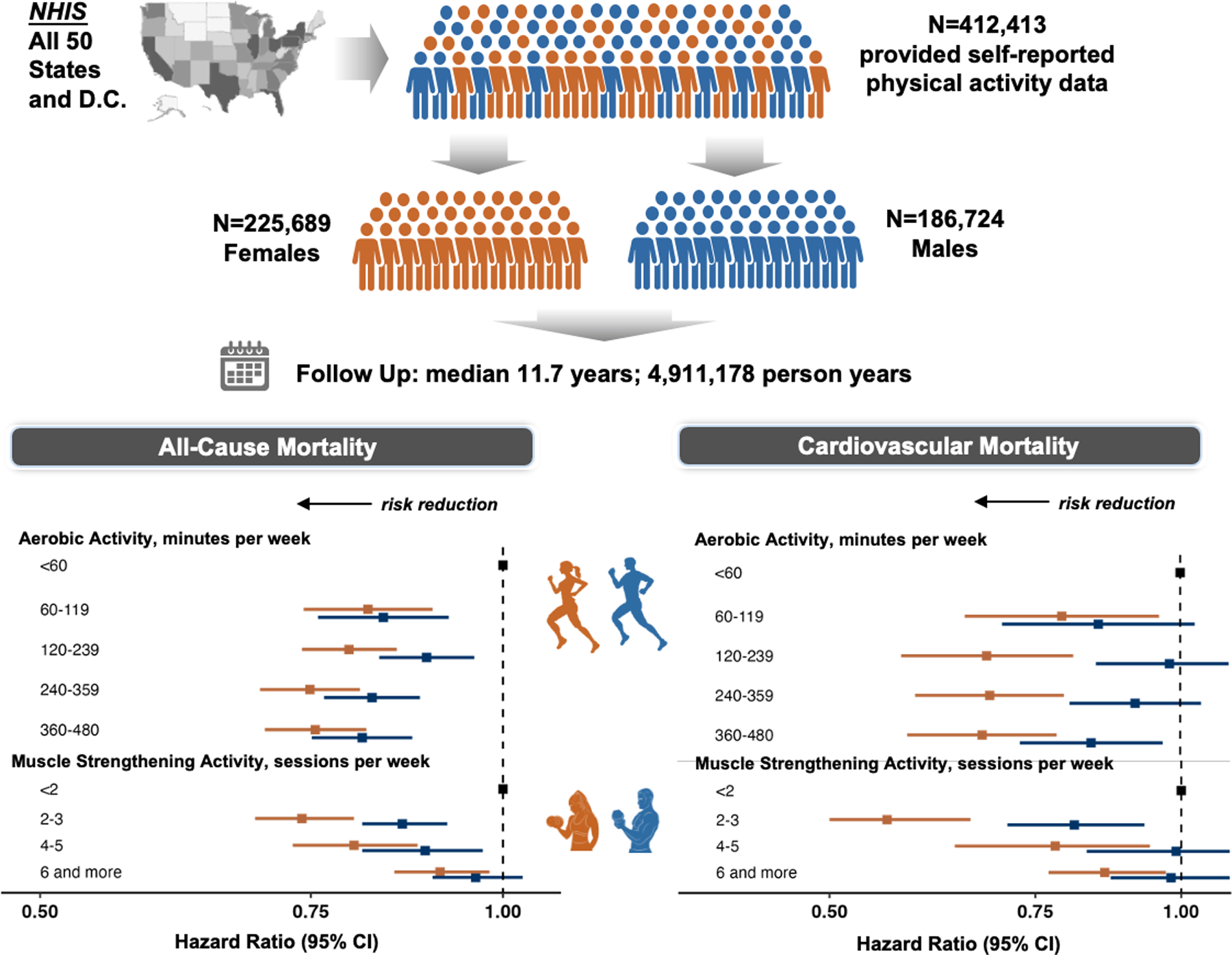
We studied 412,413 U.S. adults and found that females compared to males derived greater gains in all-cause and cardiovascular mortality risk reduction from equivalent doses of leisure-time physical activity.
Prior data on sex differences in PA associated outcomes are limited. In a Taiwanese cohort study of 199,265 males and 216,910 females, designed to identify the minimum amount of exercise needed to reduce all-cause mortality, both sexes derived a similar 14% risk reduction in association with as little as 15 minutes of moderate intensity activity per day or 90 minutes per week.19 Consistent with these findings, our results also showed that all-cause mortality benefit was comparable between sexes at similarly lower doses of exercise. Extending from these findings, we further found that sex differences emerged at higher doses of exercise. With respect to cardiovascular outcomes, a meta-analysis of 33 studies showed that relative risk for coronary heart disease was two-fold lower for females compared with males at similar levels of PA, with a significant sex interaction.20 Our study adds to these findings by demonstrating similar sex differences in PA associated risk for not only incident disease but also cardiovascular mortality.
There are several potential explanations for our findings. It has long been known that males have measurably greater exercise capacity than females across all ages.6,7,21 This may be in part due to attributes including on average proportionately larger hearts, wider lung airways, greater lung diffusion capacity, and larger muscle fibers in males compared to females.22–24 In particular, men have ~38% more lean body mass compared to women,23 and so a relatively lower absolute limit to exercise-induced vasodilatory capacity imposed by substantially lower lean mass and muscle mass in women may be proportionately more efficiently improved by strengthened muscle from PA and especially from muscle strengthening PA of the same dose.25 Indeed, this phenomenon could underlie the marked sex differences in mortality risk reduction seen from equivalent frequencies of muscle strengthening activity. In fact, physiology studies have demonstrated that females exhibit greater vascular conductance and blood flow during exercise, with females having a higher density of capillaries per unit of skeletal muscle when compared with males.26 Accordingly, although females have generally lower muscle strength at baseline, when both males and females undergo strength training, females experience greater relative improvements in strength, which is a stronger predictor of mortality than muscle mass.27,28 Furthermore, sexual dimorphism at the level of muscle fiber type and muscle fiber metabolic, contractile, and dynamic function may also contribute to sex differential responses to the same dose of PA.29 For example, males having a greater proportion of Type II glycolytic muscle fibers whereas females have a greater proportion of Type I oxidative fibers.30,31 These differences could contribute to not only the known greater female sensitivity to disuse atrophy32 but also, conversely, the greater female sensitivity to PA observed in our study. We did note an age-interaction such that the female benefit appeared to be attenuated in older compared to younger age; further research may discern whether this finding is related to the menopausal transition with or without hormone replacement therapy taken by some women. Notably, in age-stratified analyses, sex differences were most pronounced for middle-aged adults (i.e. ages 40 to 59 years) and this finding aligns with the wealth of prior evidence indicating that relative differences in cardiovascular risk factor burden in middle age are highly impactful on not just later but overall life-long risks for adverse outcomes.33
Notwithstanding the need to validate our results in separate studies and using complementary measures of PA exposure and response, our findings have several implications. The longstanding conventional assumption has been that males and females across all age groups should engage in the same amount of regular PA to gain the same benefit.5 This assumption has motivated public health attention on the frequently observed “PA gap” between females and males,5 wherein females are from childhood onward consistently found to be approximately 6–10% less physically active than their male counterparts.34,35 Our findings suggest that attention to the “PA gap” may benefit from a greater emphasis on equalizing levels of engagement rather than equalizing specific dose exposures. Large studies of European children have shown that males consistently perform better on tests of muscular strength, power, and endurance, as well as speed-agility and exercise capacity, while females perform better on flexibility measures.36 In adults, at least one study has shown that the predicted exercise capacity assessed from a Bruce protocol treadmill stress test should be adjusted lower for women than for men, in relation to all-cause as well as cardiovascular death.7 In the context of prior studies, our findings indicate that females stand to gain proportionately more than males in reduction of cardiovascular and all-cause mortality risk for a given dose of regular exercise. While existing PA guidelines currently offer sex-agnostic recommendations,2,3 sex-specific considerations could enhance individual risk assessments and tailored exercise prescriptions in the effort to increase engagement in PA especially for females.
Study Limitations
Several limitations of our study merit consideration. First, all PA data collected were self-reported, albeit using a standardized questionnaire that remained stable over time.12,13 Numerous PA studies have examined the validity of similarly standardized questionnaire data and found generally acceptable reliability and moderate validity.37 Objective measures of PA, using devices such as accelerometers or wearables, are increasingly feasible but still incur substantial costs and so the availability of such data linked to outcomes across diverse populations remains limited.38 Fortunately, a degree of external validity for the PA data collected in the current analysis is also provided by separate studies that used accelerometry and observed the magnitude and significance of mortality associations to be consistent with our results.39 Although our analyses considered the potential effects of sex differences in self-reported PA level, additional studies are needed to further investigate how variable recall bias may influence the extent to which benefits from PA can differ by sex. While the primary focus of this analysis was on leisure-time PA, unmeasured variation in household or other activities that can vary by sex could yet have contributed to outcome differences. When estimating muscle strengthening activities, the only information collected was the frequency and not the duration of such activity; nonetheless, this type of reporting is consistent with the 2018 U.S. guidelines on PA that simply recommend performing muscle strengthening activities at least twice weekly without mention of duration.2 Additionally, the NHIS collects aerobic PA data based on exercise occurring for at least 10 minutes and benefits can be derived from periods of PA shorter than 10 minutes. Similarly, the NHIS data on muscle strengthening activities were limited to questions on lifting weights or doing calisthenics. Given the observational design of the study, causal relationships cannot be presumed and results should be interpreted with caution. To mitigate the effects of potential confounding, we excluded participants who were censored within the first 2 years of follow-up for initial analysis. However, unmeasured confounders could yet have influenced results including differential reporting by males and females, unassessed health status factors, and variations in PA engagement over time. Although our sampling methods aimed to reduce the likelihood of reverse causation, we cannot entirely rule out its possible influence in the analyses. While our exploratory analyses suggest that sex-specific outcomes likely persisted throughout the two decades of outcomes surveillance studied, trends in PA engagement continue to evolve and will warrant future additional studies.12
CONCLUSION
In summary, we found evidence of significant sex differences in association of self-reported leisure-time PA with all-cause and cardiovascular death in a large nationally representative cohort of U.S. adults followed for over 4 million person-years. Overall, females compared to males derived greater gains in all-cause and cardiovascular mortality risk reduction from equivalent doses of leisure-time physical activity. These findings could motivate efforts to close the ‘gender-gap’ by encouraging especially females to engage in any regular leisure-time physical activity. Our findings extend from a continually growing body of concordant evidence from physiology and clinical studies on sexual dimorphism in exercise capacity and associated outcomes. Taken together, the results from the current study combined with those of prior investigations suggest that PA related risk assessments and recommendations could benefit from sex-specific considerations; in turn, sex-specific guidance could serve to motivate increased PA engagement particularly among females who stand to gain substantial health benefits. Recognizing the limitations of a one-size-fits-all approach, increasing attention to sex differences in PA related risks and benefits could augment precision medicine efforts to improve health outcomes for all.
Supplementary Material
CLINICAL PERSPECTIVES.
Competency in Patient Care and Medical Knowledge:
Physiological responses to various types and intensity of physical activity differ between men and women, as does the associated health benefit. While women tend to engage in less physical activity, the survival benefit gained from exercise is greater for women than for men.
Translational Outlook:
Awareness of this gender gap and motivating women to engage regularly in leisure-time physical activity could increase their longevity.
Funding/Support.
This work was supported in part by NIH grants K23HL153888, K23AG058752, R21HL156132, R01HL142983, R01HL151828, R01HL131532, R01HL143227, R01AG072475, U54AG062319, and U54AG065141, and the Erika J Glazer Family Foundation, National Key R&D Program of China (2022YFC2502800), National Natural Science Foundation of China (82103908), Shandong Provincial Natural Science Foundation (ZR2021QH014), Shuimu Scholar Program of Tsinghua University, and National Postdoctoral Innovative Talent Support Program (BX20230189).
Role of the Funder/Sponsor.
The funding sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Abbreviations
- PA
Physical Activity
- CDC
Centers for Disease Control and Prevention
- AHA
American Heart Association
- ACC
American College of Cardiology
- NHIS
National Health Interview Survey
- MVPA
Moderate-to-vigorous intensity aerobic physical activity
- MPA
Moderate-intensity physical activity
- VPA
Vigorous-intensity physical activity
Footnotes
Ethical approval. The National Center for Health Statistics Disclosure Review Board approves the NHIS. Data analyses for this study were additionally approved by the Cedars-Sinai Medical Center institutional review board.
Conflicts of Interest: None.
REFERENCES
- 1.Elgaddal N, Kramarow EA, Reuben C. Physical activity among adults aged 18 and over: United States, 2020. NCHS Data Brief, no 443. 2022. doi: 10.15620/cdc:120213. Published August/30/2022. Accessed 03/11/2023. [DOI] [PubMed] [Google Scholar]
- 2.Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for Americans. JAMA. 2018;320(19):2020–2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e563–e595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Guthold R, Willumsen J, Bull FC. What is driving gender inequalities in physical activity among adolescents? J Sport Health Sci. 2022;11(4):424–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.The Lancet Public H Time to tackle the physical activity gender gap. Lancet Public Health. 2019;4(8):e360. [DOI] [PubMed] [Google Scholar]
- 6.Al-Mallah MH, Juraschek SP, Whelton S, et al. Sex Differences in Cardiorespiratory Fitness and All-Cause Mortality: The Henry Ford ExercIse Testing (FIT) Project. Mayo Clin Proc. 2016;91(6):755–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gulati M, Black HR, Shaw LJ, et al. The prognostic value of a nomogram for exercise capacity in women. N Engl J Med. 2005;353(5):468–475. [DOI] [PubMed] [Google Scholar]
- 8. https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm.
- 9.National Center for Health Statistics. Health Care Surveys. . https://wwwcdcgov/nchs/ahcd/ahcd_confidentialityhtm.
- 10.CDC. About the National Health Interview Survey. US Centers for Disease Control and Prevention; https://www.cdc.gov/nchs/nhis/about_nhis.htm#sample_design. Published 2022. Accessed March 12, 2023. [Google Scholar]
- 11.Parsons VL, Moriarity C, Jonas K, Moore TF, Davis KE, Tompkins L. Design and estimation for the national health interview survey, 2006–2015. Vital Health Stat 2. 2014(165):1–53. [PubMed] [Google Scholar]
- 12.Whitfield GP, Hyde ET, Carlson SA. Participation in Leisure-Time Aerobic Physical Activity Among Adults, National Health Interview Survey, 1998–2018. J Phys Act Health. 2021;18(S1):S25–s36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hyde ET, Whitfield GP, Omura JD, Fulton JE, Carlson SA. Trends in Meeting the Physical Activity Guidelines: Muscle-Strengthening Alone and Combined With Aerobic Activity, United States, 1998–2018. J Phys Act Health. 2021;18(S1):S37–s44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dos Santos M, Ferrari G, Lee DH, et al. Association of the “Weekend Warrior” and Other Leisure-time Physical Activity Patterns With All-Cause and Cause-Specific Mortality: A Nationwide Cohort Study. JAMA Intern Med. 2022;182(8):840–848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wang Y, Nie J, Ferrari G, Rey-Lopez JP, Rezende LFM. Association of Physical Activity Intensity With Mortality: A National Cohort Study of 403 681 US Adults. JAMA Intern Med. 2021;181(2):203–211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Statistics. NCfH. The Linkage of National Center for Health Statistics Survey Data to the National Death Index — 2019 Linked Mortality File (LMF): Linkage Methodology and Analytic Considerations. Hyattsville, Maryland. 2022. [Google Scholar]
- 17.López-Bueno R, Ahmadi M, Stamatakis E, Yang L, Del Pozo Cruz B. Prospective Associations of Different Combinations of Aerobic and Muscle-Strengthening Activity With All-Cause, Cardiovascular, and Cancer Mortality. JAMA Intern Med. 2023;183(9):982–990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dyrstad SM, Hansen BH, Holme IM, Anderssen SA. Comparison of self-reported versus accelerometer-measured physical activity. Med Sci Sports Exerc. 2014;46(1):99–106. [DOI] [PubMed] [Google Scholar]
- 19.Wen CP, Wai JP, Tsai MK, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011;378(9798):1244–1253. [DOI] [PubMed] [Google Scholar]
- 20.Sattelmair J, Pertman J, Ding EL, Kohl HW 3rd, Haskell W, Lee IM. Dose response between physical activity and risk of coronary heart disease: a meta-analysis. Circulation. 2011;124(7):789–795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346(11):793–801. [DOI] [PubMed] [Google Scholar]
- 22.Dominelli PB, Molgat-Seon Y. Sex, gender and the pulmonary physiology of exercise. European Respiratory Review. 2022;31(163):210074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Janssen I, Heymsfield SB, Wang ZM, Ross R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J Appl Physiol (1985). 2000;89(1):81–88. [DOI] [PubMed] [Google Scholar]
- 24.Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39.e14. [DOI] [PubMed] [Google Scholar]
- 25.Diaz-Canestro C, Pentz B, Sehgal A, Yang R, Xu A, Montero D. Lean body mass and the cardiovascular system constitute a female-specific relationship. Sci Transl Med. 2022;14(667):eabo2641. [DOI] [PubMed] [Google Scholar]
- 26.Beltrame T, Villar R, Hughson RL. Sex differences in the oxygen delivery, extraction, and uptake during moderate-walking exercise transition. Appl Physiol Nutr Metab. 2017;42(9):994–1000. [DOI] [PubMed] [Google Scholar]
- 27.Roberts BM, Nuckols G, Krieger JW. Sex Differences in Resistance Training: A Systematic Review and Meta-Analysis. J Strength Cond Res. 2020;34(5):1448–1460. [DOI] [PubMed] [Google Scholar]
- 28.Newman AB, Kupelian V, Visser M, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci. 2006;61(1):72–77. [DOI] [PubMed] [Google Scholar]
- 29.Vanhatalo A, Black MI, DiMenna FJ, et al. The mechanistic bases of the power-time relationship: muscle metabolic responses and relationships to muscle fibre type. J Physiol. 2016;594(15):4407–4423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Staron RS, Hagerman FC, Hikida RS, et al. Fiber type composition of the vastus lateralis muscle of young men and women. J Histochem Cytochem. 2000;48(5):623–629. [DOI] [PubMed] [Google Scholar]
- 31.Miller AE, MacDougall JD, Tarnopolsky MA, Sale DG. Gender differences in strength and muscle fiber characteristics. Eur J Appl Physiol Occup Physiol. 1993;66(3):254–262. [DOI] [PubMed] [Google Scholar]
- 32.Wang Y, Pessin JE. Mechanisms for fiber-type specificity of skeletal muscle atrophy. Curr Opin Clin Nutr Metab Care. 2013;16(3):243–250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Berry JD, Dyer A, Cai X, et al. Lifetime Risks of Cardiovascular Disease. New England Journal of Medicine. 2012;366(4):321–329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. 2018;6(10):e1077–e1086. [DOI] [PubMed] [Google Scholar]
- 36.Tomkinson GR, Carver KD, Atkinson F, et al. European normative values for physical fitness in children and adolescents aged 9–17 years: results from 2 779 165 Eurofit performances representing 30 countries. Br J Sports Med. 2018;52(22):1445–14563. [DOI] [PubMed] [Google Scholar]
- 37.Helmerhorst HHJF, Brage S, Warren J, Besson H, Ekelund U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. International Journal of Behavioral Nutrition and Physical Activity. 2012;9(1):103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lee IM, Shiroma EJ. Using accelerometers to measure physical activity in large-scale epidemiological studies: issues and challenges. Br J Sports Med. 2014;48(3):197–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Feng H, Yang L, Liang YY, et al. Associations of timing of physical activity with all-cause and cause-specific mortality in a prospective cohort study. Nat Commun. 2023;14(1):930. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.