

Abstract
Background and Aims
Knee support, frequently made from sponge, is used to reduce injury. Sponge has less elasticity and durability compared with natural rubber. To our knowledge, there was no study that demonstrated the effectiveness of natural rubber and sponge in prevention of injury in children with bleeding disorders. The study aimed to demonstrate the effectiveness and satisfaction of natural rubber knee support compared with sponge knee support among children with bleeding disorders.
Methods
The study consisted of three phases: (I) measuring reduced compression force, (II) producing size‐appropriate knee support prototypes, and (III) conducting a randomized crossover trial, including 8 weeks wearing natural rubber knee support and sponge knee support with a 4‐week wash‐out period. The number of knee bleeds and user satisfaction were recorded.
Results
A better compression force reduction in natural rubber (60%) than sponge (12%) was demonstrated. Knee support comprised a body part, made from natural‐stretchable cotton and a protection part, made from either natural rubber or sponge. They were produced in four sizes: S, M, L, and XL and appropriately applied to 42 patients (21 hemophilia, 21 platelet disorders) with a mean (SD) age of 7.0 (2.9) years. The results from randomization showed no significant difference in the number of knee bleeds between the two knee support groups (10 vs. 7, p = 0.37). In terms of satisfaction score, the natural rubber knee supports were more durable (45.2% vs. 23.8%, p = 0.04) and easier to use (28.5% vs. 14.3%, p = 0.03). In addition, a higher percentage of parents chose natural rubber knee support when compared with sponge knee supports (71.0% vs. 29.0%, p = 0.006).
Conclusion
Natural rubber knee support showed comparable effectiveness in the prevention of knee bleeding but was superior to sponge knee support in compression force reduction and satisfaction.
Keywords: bleeding disorder, hemophilia, knee protection, natural rubber
1. INTRODUCTION
Joint bleeding can cause significant morbidity among patients with bleeding disorders and have a negative impact on quality of life due to limited range of motion and chronic pain caused by chronic arthropathy and irreversible joint damage secondary to repeated bleeding. Bleeding in joints results in hemosiderin deposition, inflammation, and synovial hypertrophy. 1 , 2 , 3 , 4 Knee joints are particularly affected 5 , 6 either from trauma or non‐trauma injuries 7 ; for example, in patients with hemophilia, von Willebrand disease, platelet disorders, and other coagulation defects.
Among people with hemophilia, hemarthrosis is a hallmark of presentation with various reports of median annualized joint bleeding rates (AJBR) depending on the prophylaxis protocols. The standard dose prophylaxis protocol for hemophilia A at 25−40 unit/kg alternating daily with standard half‐life (SHL) of factor VIII concentration, the median AJBRs for children (0−11 years) and adolescents (12−18 years) were reported at 2.0 (IQR, 0.0−7.0) and 1.0 (IQR, 0.0−3.0), respectively. 8 On the other hand, in countries with limited resource, low dose prophylaxis of hemophilia A at 10−15 U/kg twice weekly demonstrated the median AJBR in people with severe hemophilia A of 3.0 (IQR, 1.0−4.5), which was higher than the standard dose prophylaxis protocol, but lower than that without prophylaxis of 4 (IQR, 0−8). 9 In Thailand, the median AJBR among patients with severe hemophilia A receiving low dose SHL factor prophylaxis was reported at 18 (IQR, 6−24). 10 Other than the prophylaxis protocol, external factors contributing to hemarthrosis include patients' activities, disease severities, and the presence of target joints. 9 Therefore, campaigns to prevent and enhance joint health remain an essential measure.
Regular physical activities have been proven to increase bone health, strengthen muscles, improve coordination, enhance physical functioning, maintain healthy body weight, and promote positive self‐esteem 11 ; however, those activities can cause injury and result in joint bleeding. Knee supports are effective in preventing knee injuries, therefore, wearing knee support is recommended while doing outdoor activities to reduce bleeding risk. Currently, commercially available anticollision cushions are fabricated from sponge and polyester fiber. 12 , 13
Natural rubber is a polymer characterized as sustainable soft material. 14 The advantages of national rubber include tear resistance, high resilience, and elasticity. 15 At present, it is used in many medical products, such as cardiac pacemaker leads, mammary prostheses, artificial skin, catheters, blood pressure cuff coils, tubes, and seal rubber. 16 To our knowledge, there has been no report on knee supports with cushions made from natural rubber and their effectiveness in protecting knee joint and preventing its injurry. Therefore, this study aimed to compare between two types of knee supports, fabricated with cushions made from natural rubber and sponge, their transmitted impact force reduction and effectiveness in reducing any bleedings, and patients' satisfaction.
2. MATERIALS AND METHODS
2.1. Study design
The study employed a prospective design, conducted at the Faculty of Medicine Ramathibodi Hospital, a tertiary care hospital in Thailand, from April 2021 to September 2022; and approved by the Hospital's Committee on Human Rights Related to Research Involving Human Subjects (COA. MURA2021/292) and the trial registration number was NCT06039904. Written informed consents were obtained from individual patients and their legal guardians. The study was divided into three phases: measurement of transmitted impact force, fabrication of knee supports, and randomized cross‐over trial of natural rubber and sponge knee supports.
2.1.1. Phase I
Transmitted impact forces were measured using an impact tester (Model DC Power Supply GW Instek GPS‐30300 and Multi‐Meter Fluke DT‐9208a). Three types of knee support samples, size 30 × 30 × 1 cm (W × L × H): with no barrier, with natural rubber cushion, and with sponge cushion were prepared for experiment. The experiment was performed using the same force in the ballistic pendulum test (1 kg momentum ball with a radius of 50 cm). The test was repeated three times, and the average results were recorded as force (Newton) and time (s) after the sphere hit the receptive sensor. Natural rubber used in this study was made from natural rubber and polymer (Patent ID 74814).
2.1.2. Phase II
Knee supports were designed and fabricated in various sizes. Three measurements, knee circumferences, patella sizes, and knee heights, were taken from 20 Thai children aged between 9 months and 10 years and having body weights within the 50th to 75th percentile. The knee support comprised two parts, the support body and the protective cushion. The width of the support body was derived from half of the knee circumference, and the length was taken from 80% of the knee height, measured from knee to medial malleolus. From those measurements, final knee supports were categorized into four sizes, S, M, L, and XL according to widths and lengths, as follows: size S, 8 × 17 cm; size M, 10 × 19 cm; size L, 12 × 24 cm; and size XL, 14 × 28 cm. The support body was made of stretchable natural cotton fabrics, which were comfortable, breathable, washable, less irritant, and flexible. 17 Similarly, the protective cushion was classified into four sizes: S, M, L, and XL with diameters (based on the patellar diameters) of 5, 6, 7, and 8 cm, respectively. Cushions were made from either natural rubber or sponge and inserted at the front of the support body (to cover the patellar). As a result, natural rubber and sponge knee supports were fabricated, and they both had similar external appearance (Figure 1).
Figure 1.

Knee supports designed and used in the study: (A) body of knee support made with elastic natural cotton fabrics; (B) cushion center made from natural rubber; (C) cushion center made from sponge material; and (D) final knee supports, with cushion B (left) or C (right) inserted into the center of the body (A) to cover the patella and tibial tuberosity.
2.1.3. Phase III
A randomized, single‐blinded to patients and parents, cross‐over trial using natural rubber and sponge knee supports was conducted among patients with bleeding disorders. The patients were divided into two groups, A and B, by computer‐generated randomization sequence using a box of 10. A total of 44 patients were enrolled with 21 in Group A and the other 23 in Group B. Later, two patients in Group A were excluded due to loss of follow‐ups. Therefore, the final number of patients in the study was 42 with 19 in Group A and 23 in Group B. Group A was first assigned to Treatment I of natural rubber knee support followed by Treatment II of sponge knee support, while Group B was first assigned to Treatment II followed by Treatment I (Figure 2). Patients were advised to use the supports during physical activities; for example, walking and crawling among toddlers and playing sports among school‐aged children. Each treatment covered a period of 8 weeks, with 4 weeks of wash‐out period of cross‐over from the first treatment to the second. Survey data on demographics, number of bleeds, types of bleeding (extraarticular or intraarticular), and user's satisfaction were collected. User's compliance and bleeding data, including severity and activity when injury occurred, were collected weekly using freeware application, online electronic form, or direct telephone contact. Satisfaction survey was conducted following the Client Satisfaction with Device module of Orthotics and Prosthetic User' Survey (CSD‐OPUS) 18 with Thai translation. The survey consisted of nine aspects: fitting well, weight, comfort, ease to use, attractiveness, durability, irritation, pain, and overall satisfaction. Patients aged >7 years and all parents were included in the survey, sent to them in electronic format, twice; that was, at the end of the two treatments. Scores were graded in absolutely agree, agree, disagree, and absolutely disagree. At the end of the second treatment, parents of both groups were asked to choose either the knee support of Treatment I or Treatment II as a preference.
Figure 2.
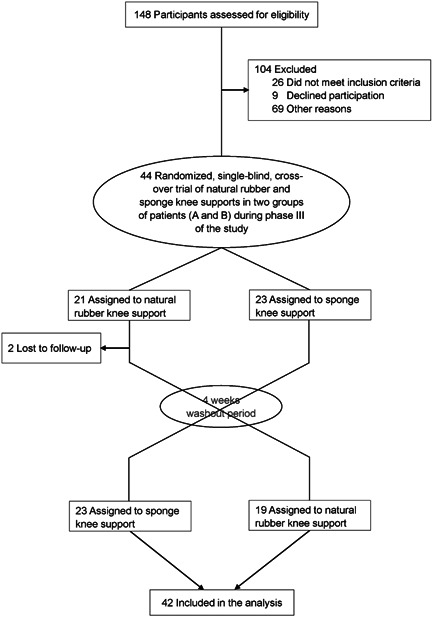
Flow diagram of randomized, single‐blind, cross‐over trial of natural rubber and sponge knee supports in two groups of patients (A and B) during phase III of the study.
2.2. Patients
The inclusion criteria were bleeding disorder patients, aged 9 months to 12 years old, with written consents The enrolled patients had no coexisting diseases affecting their activities, or bleeding episodes 2 weeks before the study. Children or parents who were not able to continue the study until the end were excluded.
2.3. Statistical analysis
The sample size was calculated based on available data of the median ABR among bleeding disorder patients; for example, hemophilia patients, 19 and the rate reduction of knee injuries after using knee support. 20 An 80% power was used to detect a significant difference (p = 0.05); hence, a minimal total of 40 patients were required for the study. Analyses of baseline characteristics were described by mean ± SD. The comparative analysis of McNemar's test was used for categorical data, and the paired t‐test for continuous data. Multilevel mixed‐effects Poisson regression was used to evaluate the differences between Treatments I and II. A p value < 0.05 was considered significant. Statistical analyses were performed using Stata Software by StataCorp LLC, Version 16.
3. RESULTS
3.1. Phases I and II
The transmitted impact forces acting on the sensor through three types of knee support samples with no barrier, with natural rubber cushion, and with sponge cushion were 400, 160, and 350 N, respectively. The results contributed to transmitted impact force reductions in natural rubber and sponge knee supports, compared with that without barrier or protection, of 60% and 12.5%, respectively (eFigure S1).
3.2. Phase III
Forty‐four patients with bleeding disorder were enrolled. Two patients were loss to follow. A total of 42 patients were analyzed. Thirty‐four (80.9%) patients were male, and half of the patients were hemophilia, with other inherited bleeding disorders found in the other half. In the platelet disorder group (15 patients), 93% presented thrombocytopenia with a median (range) platelet count of 51,700 (41,350−62,050)/mm3. Thirteen (31%) patients were in the toddler age group (0−5 years), and 69% of the patients were in the school age group (>5 years) (Table 1).
Table 1.
Characteristics of the enrolled patients with bleeding disorders.
| Parameter | N (%) |
|---|---|
| Total patients | 42 |
| Age (mean ± SD) | 7.1 ± 2.9 |
| Sex (n, %) | |
| ‐ Male | 34 (80.9%) |
| ‐ Female | 8 (19.1%) |
| Diagnosis (n, %) | |
| ‐ Hemophilia | 21 (50%) |
| Hemophilia A | 16 (76.2%) |
| Mild | 1 |
| Moderate | 1 |
| Severe | 14 |
| Hemophilia B | 5 (23.8%) |
| Moderate | 1 |
| Severe | 4 |
| ‐ Platelet disorder | 15 (35.7%) |
| ● Thrombocytopenia | 14 (93.3%) |
| Chronic immune thrombocytopenia | 10 |
| MYH9‐related disorder | 2 |
| Hypoplastic myelodysplastic syndrome | 1 |
| Severe aplastic anemia | 1 |
| ● Platelet dysfunction | 1 (6.7%) |
| Glanzmann thrombasthenia | 1 |
| ‐ Von Willebrand disease | 6 (14.3%) |
| Type 1 | 2 |
| Type 2A | 4 |
| Prophylaxis in hemophiliaa | 17 (85%) |
| Hemophilia patients with target joint | 2 (9.5%) |
| Knee | 1 |
| Ankle | 1 |
| Number of patients experienced knee support | 11 (26.2%) |
Abbreviation: SHL, standard half‐life.
Low‐dose prophylaxis of 10−15 IU/kg, 2 days/week of SHL factor VIII concentration in severe hemophilia A and 40−50 IU/kg of SHL factor IX concentration weekly in severe hemophilia B.
Among the 21 hemophilia patients, 10 with a diagnosis of severe hemophilia A, received a low dose prophylaxis protocol of 10−15 IU/kg, 2 days/week of SHL factor VIII concentration. Four patients with severe hemophilia B received 40−50 IU/kg of SHL factor IX concentration weekly. One patient with moderate hemophilia A received 10 U/kg, 2 days/week of SHL factor VIII concentration. One patient with moderate hemophilia B received 10 U/Kg weekly SHL factor IX concentration. Only one patient with severe hemophilia A and inhibitor received a low dose emicizumab standard regimen of 4 weekly doses of 3 mg/kg, followed by 4 weekly maintenance doses of 1−1.5 mg/kg, which was equivalent to factor VIII activity 3%. 21 Only 12 (29.3%) patients had used knee supports before enrollment (Table 1).
The total number of days patients using natural rubber knee support (natural rubber group) and sponge knee support knee support (sponge group) were 716 days or 2.1 ± 1.6 days weekly and 837 days or 2.5 ± 1.7 days weekly, respectively; and were not significantly differ between the two groups (p = 0.37). Number of bleeding events while wearing knee supports in the natural rubber group and the sponge group were 10, equal to the ABR of 0.04 and 7, equal to the ABR of 0.03, respectively. Knee hemarthrosis event was diagnosed once in each group and occurred only in two severe hemophilia A patients (both patients were admitted to the hospital to receive factor treatment). One hemarthrosis event was found related to trauma. Fifteen events were small ecchymoses around the knee, occurring among eight patients without hospitalization. After stratified knee bleeding events by type (joint bleeding and small ecchymosis), diseases (hemophilia and other bleeding disorders), history of knee supports used before the enrollment, prophylaxis use and trauma‐ and non‐trauma related injuries, no statistically significant differences were noted in those compared factors with bleeding occurrence. Number of knee bleeding events occurred while wearing knee supports, 17 in 463 weeks, was significantly fewer than those without knee supports of 15 events of 209 weeks; RR 0.45, 95% confidence interval 0.21−0.97, p = 0.04 (Table 2). Moreover, monthly knee bleeding events before enrollment to the study were higher than during the study period, which were 1.34 and 0.16 monthly extra‐articular bleeding events, respectively.
Table 2.
Number of knee bleeding events between natural rubber and sponge knee‐supports.
| Parameter | Natural rubber knee support | Sponge knee support | p Value |
|---|---|---|---|
| Total days of knee‐support used | 716 | 837 | 0.26 |
| Days of knee‐support used per week per patient (mean ± SD) | 2.1 ± 1.6 | 2.5 ± 1.7 | 0.26 |
| Numbers of knee bleedings during protection | 10 | 7 | 0.37 |
| ‐ Joint bleeds | 1 | 1 | 1.00 |
| ‐ Ecchymoses | 9 | 6 | 0.49 |
| In hemophilia | |||
| Total knee bleeds | 7 | 4 | 0.29 |
| ‐ Intraarticular bleeds | 1 | 1 | 1.00 |
| ‐ Ecchymoses | 6 | 3 | 0.29 |
| In platelet disorder and VWD | |||
| Total knee bleeds | 3 | 3 | 1.00 |
| ‐ Intraarticular bleeds | 0 | 0 | ‐ |
| ‐ Ecchymoses | 3 | 3 | 1.00 |
| Bleedings associated with traumaa | 9 | 6 | 0.84 |
| Bleedings not associated with trauma | 1 | 1 | 1 |
Abbreviation: VWD, von Willebrand disease.
Fall on the floor (65%), hit against hard objects (35%).
4. ADVERSE EVENTS AND SATISFACTION OUTCOMES
Satisfaction scores of parents and patients on nine aspects from the survey were analyzed (Table 3). In the natural rubber group, the durability aspect reported by parents was significantly better (p = 0.04), while the ease to use aspect was significantly better reported by patients (p = 0.03). The other satisfaction aspects were similar between the two groups. Parents were blinded to choose only one material of choice, 30 (71.4%) parents selected natural rubber, while 12 (28.6%) parents selected sponge (p = 0.006). One patient reported mild itchiness without rash, but this did not disturb his activities while wearing knee supports. The patient continued wearing knee supports until the study finished. The symptoms resolved after removing the knee‐supports.
Table 3.
Satisfaction survey on patients and parents.
| Aspect of evaluation | Parent satisfaction | Patient satisfaction | ||||
|---|---|---|---|---|---|---|
| Natural rubber knee support | Sponge knee support | p Value | Natural rubber knee support | Sponge knee support | p Value | |
| Fit well | 0.24 | 0.12 | ||||
| Absolutely disagree | 0 | 0 | 0 | 0 | ||
| Disagree | 3 | 7 | 1 | 4 | ||
| Agree | 28 | 23 | 12 | 14 | ||
| Absolutely agree | 11 | 12 | 14 | 9 | ||
| Weight | 0.92 | 0.32 | ||||
| Absolutely disagree | 0 | 0 | 0 | 0 | ||
| Disagree | 2 | 2 | 1 | 3 | ||
| Agree | 29 | 28 | 15 | 17 | ||
| Absolutely agree | 11 | 12 | 11 | 7 | ||
| Comfort | 0.57 | 0.08 | ||||
| Absolutely disagree | 1 | 0 | 0 | 1 | ||
| Disagree | 6 | 8 | 6 | 3 | ||
| Agree | 25 | 26 | 12 | 19 | ||
| Absolutely agree | 10 | 8 | 9 | 4 | ||
| Ease to use | 0.08 | 0.03 | ||||
| Absolutely disagree | 0 | 0 | 0 | 1 | ||
| Disagree | 0 | 5 | 2 | 4 | ||
| Agree | 35 | 19 | 13 | 16 | ||
| Absolutely agree | 7 | 18 | 12 | 6 | ||
| Attractiveness | 0.11 | 0.18 | ||||
| Absolutely disagree | 0 | 0 | 0 | 0 | ||
| Disagree | 3 | 7 | 4 | 3 | ||
| Agree | 21 | 22 | 11 | 18 | ||
| Absolutely agree | 18 | 13 | 12 | 6 | ||
| Durability | 0.04 | 0.10 | ||||
| Absolutely disagree | 0 | 0 | 0 | 0 | ||
| Disagree | 4 | 5 | 3 | 1 | ||
| Agree | 19 | 27 | 11 | 17 | ||
| Absolutely agree | 19 | 10 | 13 | 9 | ||
| No irritation | 0.06 | 0.25 | ||||
| Absolutely disagree | 0 | 0 | 0 | 0 | ||
| Disagree | 0 | 5 | 1 | 2 | ||
| Agree | 26 | 20 | 13 | 15 | ||
| Absolutely agree | 16 | 17 | 13 | 10 | ||
| No pain | 0.37 | 0.26 | ||||
| Absolutely disagree | 1 | 0 | 0 | 0 | ||
| Disagree | 5 | 4 | 2 | 2 | ||
| Agree | 17 | 18 | 11 | 15 | ||
| Absolutely agree | 19 | 20 | 14 | 10 | ||
| Overall | 0.55 | 0.61 | ||||
| Absolutely disagree | 0 | 0 | 0 | 1 | ||
| Disagree | 8 | 10 | 6 | 7 | ||
| Agree | 19 | 20 | 11 | 8 | ||
| Absolutely agree | 15 | 12 | 10 | 11 | ||
5. DISCUSSION
Knee supports are quite effective in reducing forces experienced by the knee joint 12 and reducing athletic knee injury. 20 The force that could have a significant injury to the knee joint was reported to be around 600−2300 N. 22 Therefore, the force reduction using knee‐supports could benefit in preventing knee joints from serious injury. To our knowledge, the present study was the first to demonstrate the residual impact force of knee support when protected with natural rubber compared with sponge material. The residual impact was reduced by 60% which was the highest reduction when compared with sponge and results reported by another study. 12 The reduction of residual impact force was due to the characteristics of natural rubber; that is, viscosity and elasticity.
Natural rubber consists of polymers of isoprene, an organic compound. Rubber trees grow in Southeast Asia including Thailand. The elasticity of natural rubber is demonstrated by the disorganized cluster of inconsistently altering wrinkled chain structure. 23 Because of its elasticity, natural rubber has been used in several medical products including the knee support in this study.
People with hemophilia have a risk of hemarthrosis especially while doing high‐risk activities. Preventing injury to the joints and educating patients and family members are suggested. In the present study, 50% of enrolled children were hemophilia patients. Other bleedings disorders, such as the skin, soft tissues, and hemarthrosis with a similar ABR to patients with hemophilia, also posed a risk of bleeding symptoms. Those bleeding symptoms were included as an outcome measurement. The history of bleeding was recorded before and during the study. Knee joint bleeding events decreased from 1 to 0.2 times monthly before and during the study, respectively. In the present study, only 30% of patients used knee supports before the enrollment to the study. Therefore, protecting the knee joint was able to reduce bleedings. Although the better force reduction of natural rubber compared with sponge was demonstrated, there was no difference in ABR. This result might be explained by mild injuries (fall on the floor and hit against hard objects), reported by the parents and restricted outdoor activities during the COVID‐19 pandemic; therefore, no serious injuries were reported. In addition, educating patients with bleeding disorders to avoid high risk bleeding activities have been suggested. However, both natural rubber and sponge materials exhibited similar rates of bleedings. The satisfaction survey results demonstrated the preference for natural rubber knee supports. In the durability aspect, natural rubber knee supports revealed a significantly better satisfaction score than the sponge knee supports which might be due to the characteristics of natural rubber. 15 One natural rubber property is good tack which makes it easy to set into product shapes 17 ; hence, contributing to placing the knee support into shape and providing another significant satisfaction aspect, namely, ease to use. Other aspects of patient satisfaction, such as fitting well and attractiveness, did not significantly differ between the two groups; but they played certain positive roles in the overall satisfaction. Although natural rubber weight was 80 g per pair of knee supports and sponge weight was only 5 g per pair, no difference was noted in the satisfaction weight category between the two groups.
The body part of knee supports used in this study was made from stretchable natural cotton fabrics instead of neoprene, which is used in one of the commercially available knee supports for adults. The use of neoprene in knee support is for joint stabilization. Our knee support was designed for protection of the knee joint and reduce injury to common injury areas. The stretchable natural cotton support body was comfortable for everyday use; and with its good ventilation property, it was suitable for the weather in tropical countries due to less irritation and more flexibility. 24 Those features may have improved patient compliance. Moreover, because of those qualities, the patients and the guardians were satisfied. Only one patient reported mild itchiness without any rash, which resolved without medication. The price of one pair of natural rubber knee supports (USD7.15) was two to three times higher than sponge knee support (USD2.43−6.08). From a questionnaire, patients using commercial sponge knee support purchased two to three pairs yearly. Therefore, with a longer lifetime of the natural rubber knee support, the total yearly cost might not be differed.
The current study encountered several limitations. First, the duration of this study of 8 weeks for each type of knee support was rather too short to observe more bleeding events. The intra‐articular AJBR was 0.06 and 0.004 times monthly among patients with hemophilia and platelet disorders, respectively, and the extra‐articular knee bleeding rate was around 1.3 times monthly. Second, the lower‐than expected bleeding rates also affected the calculated sample‐size because the sample size in this study was determined from the reported data by the World Bleeding Disorders Registry 2018 of ABR six times/year. 19 Third, the variety of patient activities and time duration could not be accurately measured in each patient; therefore, it was difficult to compare them between the two materials. Fourth, although the external appearance of the two types of knee supports were similar, they were different in weight and consistency. Therefore, patients and parents might observe the contrast between them.
6. CONCLUSION
The present study demonstrated that natural rubber knee supports could be an alternative option for joint protection among patients with bleeding disorders. They were as effective as the commercial sponge knee supports, but with higher satisfaction among patients and their parents.
AUTHOR CONTRIBUTIONS
Supicha Maneekhiew: Data curation; formal analysis; funding acquisition; investigation; methodology; project administration; visualization; writing—original draft. Nalinee Kovitwanawong: Project administration; resources; supervision; visualization; writing—review and editing. Sakrawee Raweekul: Investigation; resources; supervision; validation; writing—review and editing. Chusak Kijkunasathian: Supervision; visualization; writing—review and editing. Monratta Panuwannakorn: Supervision; visualization; writing—review and editing. Parsiri Uampornvanich: Resources; visualization; writing—review and editing. Ampaiwan Chuansumrit: Resources; supervision; visualization; writing—review and editing. Pakawan Wongwerawattanakoon: Resources; visualization; writing—review and editing. Nongnuch Sirachainan: Conceptualization; data curation; formal analysis; methodology; resources; supervision; visualization; writing—review and editing. All authors have read and approved the final version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
TRANSPARENCY STATEMENT
The lead author Nongnuch Sirachainan affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Supporting information.
{kind=link}
Supporting information.
ACKNOWLEDGMENTS
The authors would like to thank Associate Professor Sasivimol Rattanasiri for the statistical analysis. Nongnuch Sirachainan is a recipient of the Career Development Award of the Faculty of Medicine Ramathibodi Hospital. The study was supported by a grant (RF_64086) from the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand as part of the study design and data collection.
Maneekhiew S, Kovitwanawong N, Raweekul S, et al. Comparison between natural rubber knee support and sponge knee support on the protection of knee joint: a crossover randomized controlled study among patients with bleeding disorders. Health Sci Rep. 2024;7:e2003. 10.1002/hsr2.2003
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request. All authors had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
REFERENCES
- 1. Fish JD, Lipton JM, Lanzkowsky P. Lanzkowsky's Manual of Pediatric Hematology and Oncology. 7th ed. Academic Press; 2021:299‐309. [Google Scholar]
- 2. Gooding R, Thachil J, Alamelu J, Motwani J, Chowdary P. Asymptomatic joint bleeding and joint health in hemophilia: a review of variables, methods, and biomarkers. J Blood Med. 2021;12:209‐220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. O'Hara J, Walsh S, Camp C, et al. The impact of severe haemophilia and the presence of target joints on health‐related quality‐of‐life. Health Qual Life Outcomes. 2018;16(1):84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Wilkins RA, Stephensen D, Siddle H, et al. Twelve‐month prevalence of haemarthrosis and joint disease using the haemophilia joint health score: evaluation of the UK National Haemophilia Database and Haemtrack patient reported data: an observational study. BMJ Open. 2022;12(1):e052358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kraus T, Švehlík M, Singer G, Schalamon J, Zwick E, Linhart W. The epidemiology of knee injuries in children and adolescents. Arch Orthop Trauma Surg. 2012;132(6):773‐779. [DOI] [PubMed] [Google Scholar]
- 6. Schnitzer PG. Prevention of unintentional childhood injuries. Am Fam Physician. 2006;74(11):1864‐1869. [PubMed] [Google Scholar]
- 7. Lombardi M, Cardenas AC. Hemarthrosis. StatPearls; 2020. [PubMed] [Google Scholar]
- 8. Scott MJ, Xiang H, Hart DP, et al. Treatment regimens and outcomes in severe and moderate haemophilia A in the UK: the THUNDER study. Haemophilia. 2019;25(2):205‐212. [DOI] [PubMed] [Google Scholar]
- 9. Wu R, Li X, Yao W, et al. Significant reduction in hemarthrosis in boys with severe hemophilia A: the China hemophilia individualized low‐dose secondary prophylaxis study. Res Practice Thrombosis Haemostasis. 2021;5(6):e12552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rakmanotham A, Moonla C, Sosothikul D. Clinical outcomes of low‐dose pharmacokinetic‐guided extended half‐life versus low‐dose standard half‐life factor VIII concentrate prophylaxis in haemophilia A patients. Haemophilia. 2023;29(1):156‐164. [DOI] [PubMed] [Google Scholar]
- 11. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(suppl 6):1‐158. [DOI] [PubMed] [Google Scholar]
- 12. Schwarze M, Hurschler C, Welke B. Force, impulse and energy during falling with and without knee protection: an in‐vitro study. Sci Rep. 2019;9(1):10336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Paluska SA, McKeag DB. Knee braces: current evidence and clinical recommendations for their use. Am Fam Physician. 2000;61(2):411‐418. [PubMed] [Google Scholar]
- 14. Ikeda Y, Phakkeeree T, Junkong P, et al. Reinforcing biofiller “Lignin” for high performance green natural rubber nanocomposites. RSC Adv. 2017;7:5222‐5231. [Google Scholar]
- 15. Tanasi P, Hernández Santana M, Carretero‐González J, Verdejo R, López‐Manchado MA. Thermo‐reversible crosslinked natural rubber: a Diels‐Alder route for reuse and self‐healing properties in elastomers. Polymer. 2019;175:15‐24. [Google Scholar]
- 16. Rahimi A, Mashak A. Review on rubbers in medicine: natural, silicone and polyurethane rubbers. Plastics, Rubber Composites. 2013;42:223‐230. [Google Scholar]
- 17. Prasopdee T, Smitthipong W. Effect of fillers on the recovery of rubber foam: from theory to applications. Polymers. 2020;12(11):2745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bettoni E, Ferriero G, Bakhsh H, Bravini E, Massazza G, Franchignoni F. A systematic review of questionnaires to assess patient satisfaction with limb orthoses. Prosthetics Orthotics Int. 2016;40(2):158‐169. [DOI] [PubMed] [Google Scholar]
- 19. World Federation of Hemophilia . WBDR 2018 data report. 2019. https://elearning.wfh.org/wp-content/uploads/2022/05/WBDR-2018-data-report-EN.pdf
- 20. Yang J, Marshall SW, Bowling JM, Runyan CW, Mueller FO, Lewis MA. Use of discretionary protective equipment and rate of lower extremity injury in high school athletes. Am J Epidemiol. 2005;161(6):511‐519. [DOI] [PubMed] [Google Scholar]
- 21. Chuansumrit A, Sirachainan N, Jaovisidha S, et al. Effectiveness of monthly low dose emicizumab prophylaxis without 4‐week loading doses among patients with haemophilia A with and without inhibitors: a case series report. Haemophilia. 2023;29(1):382‐385. [DOI] [PubMed] [Google Scholar]
- 22. Marieswaran M, Jain I, Garg B, Sharma V, Kalyanasundaram D. A review on biomechanics of anterior cruciate ligament and materials for reconstruction. Appl Bionics Biomech. 2018;2018:4657824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Brüning K. Natural Rubber. In: Encyclopedia of Polymeric Nanomaterials. Springer; 2015:1377‐1382. [Google Scholar]
- 24. Latif W, Basit A, Ali Z, Ahmad Baig S. The mechanical and comfort properties of cotton and regenerated fibers blended woven fabrics. Int J Clothing Sci Technol. 2018;30:112‐121. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Supporting information.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. All authors had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.