

Abstract
To assess current evidence of effectiveness of sequential lines of biologic and targeted small molecule drugs for psoriasis beyond first line. A systematic search of the literature (Medline, Embase and bibliographic) was undertaken in October and December 2022 to find all studies assessing effectiveness of biologics and targeted small molecules when used beyond first‐line in adults with psoriasis (PROSPERO CRD42022365298). Data extraction and a bias assessment (Risk Of Bias In Non‐randomized Studies—of Interventions/Cochrane RoB2) were undertaken for all included studies. A random effects proportional meta‐analysis was undertaken for PASI75/90/100 at 12–16 weeks for each line of treatment (1st to 4th). Of 2666 abstracts identified, a full text review was undertaken of 177 studies; 20 manuscripts met eligibility criteria. Twenty studies were included in the analysis: 19 observational studies and one sub analysis of a RCT; n = 6495 (average age 49.7 years, female 35.1%). Eleven studies assessed second line biologic, nine assessed third + line. A meta‐analysis of PASI75 at 12–16 weeks found pooled effect percentage achieving PASI75 of 61%, 56%, 79% and 61% in 1st, 2nd, 3rd and 4th line biologics respectively. Meta‐analyses of PASI90/100 also found no evidence of diminished effectiveness with sequential lines (PASI90 46.1%, 39.9%, 55.8% and 33.7% and PASI100 36.7%, 30.3%, 46.7% and 30.4% in 1st to 4th line respectively). Available evidence for effectiveness of biologics beyond first line in psoriasis is predominantly observational, at high risk of bias and of low quality. There is very limited data for effectiveness beyond second line. Evidence indicates that biologics can be effective to fourth‐line.
We assessed and synthesised the currently available data on response to biologic and targeted small molecule treatments in psoriasis, when used beyond first line. There is very little available data beyond second line, and data is of low quality and at high risk of bias. Available evidence qualitatively indicates a similar clinical response (relative PASI) to first and second line treatment, with chance of a good response up to fourth line treatment on a case‐by‐case basis. Meta‐analysis of PASI75/90/100 at 12–16 weeks found no diminishment of response from 1st to 4th line, but has to be interpreted with caution in view of the low data quality. Further prospective studies are required.

What's already known about this topic?
Increasingly people with psoriasis are being treated with multiple sequential lines of biologic and targeted small molecule drugs.
Drug survival has been shown to reduce with 2nd and beyond lines of biologic in psoriasis.
First line biologic treatment in psoriasis has been shown to be efficacious in clinical trials, but clinical response to lines beyond first line is unclear.
What does this study add?
The current available evidence shows that clinical response (as recorded by relative PASI) to first‐ and second‐line treatment is similar, and a good response can be achieved up to fourth‐line biologic treatment.
There is very little data currently available on response to third‐ and fourth‐ine biologics, with no data for 5th+ line.
A meta‐analysis of PASI75/90/100 at 12–16 weeks found a maintenance of response from 1st to 4th line biologic treatment.
1. INTRODUCTION
Psoriasis affects 60 million people worldwide, 1 with prevalence varying according to country, from 0.14% in East Asia to 1.99% in Australasia. 2 Up to 30% of those with skin psoriasis develop psoriatic arthritis (PsA), a heterogenous inflammatory musculoskeletal condition. 3 Psoriatic disease leads to significant morbidity, a reduction in work productivity and an overall decline in quality of life. 4 , 5 , 6
Over the past 2 decades, rapid advances have been made in the understanding and treatment of these conditions; multiple novel drugs have been approved, which have significantly advanced the treatment outcomes of people with psoriasis. 7 In the United Kingdom, there are currently 13 biologic and targeted small molecule drugs approved for use in psoriasis, within the classes anti‐TNFα (TNFi), anti‐interleukin‐17 (IL‐17i), anti‐interleukin‐12/23 p40 subunit (IL‐12/23i), anti‐interleukin‐23 p19 subunit (IL‐23i) and PDE‐4 inhibitors (PDE4i).
Despite the efficacy of these biologics in clinical trials, with real‐world use a significant percentage of patients stop treatment, and switch to another biologic, due to factors including inefficacy and adverse effects. 8 Due to the chronicity of psoriasis, increasingly patients have multiple lines of treatment over time. Registry data has shown that drug survival reduces with increasing lines of therapy. 9 Whilst drug survival is an important measure of real‐world use, it does not directly correspond to efficacy and can be limited by availability of a medication, patient and physician behavioural factors and adverse effects. 10
Randomised controlled trials, although best placed to determine efficacy of a novel biologic drug when used first line, often provide limited data on response to later lines of biologic treatment. Eligibility criteria in some cases limit the number and class of previous biologics, and the proportion of participants exposed to >1 prior biologic to avoid enriching the cohort with participants who may be difficult to treat. 11 In those trials that include biologic‐experienced populations, sub‐analyses assessing response stratified by number of previous lines of biologic are limited.
There is some observational data indicating advanced lines of biologic, beyond first‐line, are effective, suggesting that benefit can be obtained by appropriate treatment switching. However, in both psoriasis and PsA, the clinical response may be lower in later lines than with first line treatment. 12 , 13 Understanding how patients respond to later lines of treatment improves treatment decisions for people with psoriatic disease. The development of evidence of effectiveness beyond third line would also help inform healthcare systems that currently ration the permitted number of lines of biologic per patient.
In this review we set out to appraise the current available evidence for effectiveness of biologics and targeted small molecules when used beyond first‐line in psoriasis.
2. METHODS
2.1. Protocol
A prospective protocol was registered with PROSPERO (CRD42022365298); this literature review is reported in line with PRISMA (Preferred Reporting Items for Systematic reviews and Meta‐Analyses) guidelines. The literature review was planned to assess response in all psoriatic disease, however for feasibility and comprehensibility, the analysis and reports have been separated into psoriasis and PsA (Gollins et al, under review), with this report focusing on studies assessing psoriasis only. Studies were included of adult patients (≥18 years) with psoriasis who had been treated with second and later line biologics and targeted small molecules, where the line of treatment is clearly established within the study and primary response was reported. We excluded studies of conventional systemic treatments.
2.2. Search strategy
The literature search was carried out on 10 October 2022 in Medline and 21 October 2022 in Embase. The search was repeated on 19 December 2022 prior to full analysis of included texts. Conference abstracts were included. The search included terms for psoriasis, PsA, biologic and targeted small molecule drugs, and lines of therapy (Appendix S1). There was no date limit. A supplementary manual search of bibliographies of cited articles was undertaken. Observational studies and randomised controlled trials were included if in the English language, or with an English language translation available. Papers reporting only drug persistence and not effectiveness for different lines of treatment were excluded. Randomised controlled trials and observational studies that assessed only first line biologics and targeted small molecules were excluded.
2.3. Selection of studies
All titles and abstracts from the searches were screened by two independent reviewers (CG, RV). Following this, full text review of selected papers was completed by one reader (CG). A further reader (RV) assessed all included full texts independently to confirm appropriateness. Any discrepancies, if not resolved, were resolved by a third senior reader (WT) at all levels of screening. CG completed data extraction, RV independently reviewed data extraction.
2.4. Data collection process and bias and quality assessment
Management of citations was undertaken with Refworks™ and Microsoft™ Excel software. A pre‐determined table was followed to extract data from included papers. Extracted data included country, year and type of study, average age and sex of study participants, sample size, intervention, class of intervention and prior biologics and targeted small molecules (before intervention drug). Time of follow up was limited to a maximum of 12 months, as the aim of the review was to assess primary or initial clinical response. Up to three time points per study were collected for feasibility, with the earliest being the closest to first follow up (typically 12–16 weeks) and the latest the closest time point to 12 months, if applicable. Rate of drop out was included where available. No assumptions were made regarding missing data.
The outcome assessed was Psoriasis Area and Severity Index (PASI), in particular 75%, 90% and 100% relative improvement outcomes (PASI75/90/100 respectively). Absolute PASI improvement was included where provided.
The methodological quality of the studies was assessed using the Cochrane Risk Of Bias In Non‐randomized Studies—of Interventions (ROBINS‐I) tool for all observational studies, 14 and the Cochrane Risk of Bias tool 2 for all randomised controlled trials. 15 Risk of bias assessments were not undertaken for abstracts due to lack of evidence available to complete a meaningful assessment. The quality of evidence was assessed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) criteria for all studies included in the PASI75 meta‐analysis. There was a high level of crossover with studies included in the PASI90/100 meta‐analyses and so these studies were chosen to be representative of studies included in the statistical analyses.
2.5. Analysis
Studies were separated into manuscripts (Table S1) and abstracts (Table S2) for analysis. Manuscripts were narratively summarised, and statistically analysed as described. Abstracts were narratively summarised separately and were not included in the meta‐analysis, due to the limited available information prohibiting bias and quality assessment.
For manuscripts, a meta‐analysis was completed for the proportion of patients achieving PASI75, PASI90 and PASI100 at 12–16 weeks in each separate line of biologic treatment, for studies in which this was reported. These outcome measures were chosen as the most frequently reported within the included studies.
A proportional meta‐analysis using a random effects model was undertaken in MedCalc ™ for each group (1st, 2nd, 3rd/3rd + and 4th/4th + line biologic), with data included from all studies in which these outcomes were available. Abstracts were excluded from meta‐analysis. A random effects model was chosen due to the heterogeneity between studies, as indicated by the moderate to high I2 statistic found with each group of studies (Appendix S2).
A funnel plot was not undertaken to assess for reporting bias, as this test was primarily developed for comparative data, and is not recommended for use with proportional data. 16
3. RESULTS
3.1. Study selection
The search yielded 2666 unique papers and abstracts after duplicates had been removed (Figure 1) of which 162 were selected for full text screening. Fifteen additional papers were selected via bibliographic reference screening. Twenty manuscripts and one abstract assessing psoriasis were included.
FIGURE 1.
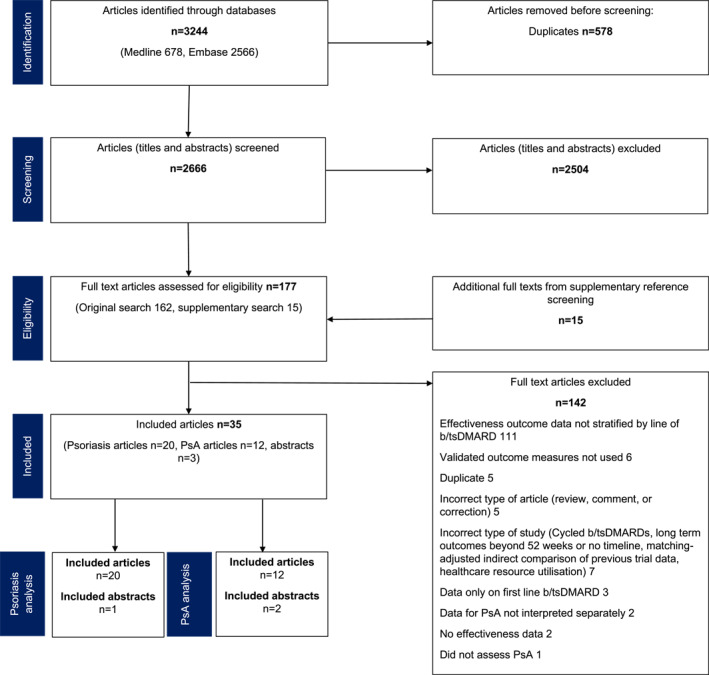
Study selection flow diagram for systematic review.
Studies were excluded if lines of biologic were aggregated, for example, comparing ‘biologic‐naïve’ to ‘biologic experienced’ patients. 17 , 18 Several identified studies assessed response after an intra‐ or inter‐class switch of biologic, however were excluded from analysis if the prior number of lines of therapy were not clearly defined. 19 , 20 Both types of study described preclude analysis of effectiveness of specific lines of biologic and so were not appropriate for the current review. No contact with authors was required for clarification.
3.2. Study characteristics
Twenty studies meeting inclusion criteria were included (Table S1), published between 2007 and 2021, with data accrual from 2002 to 2019. Fifteen were based in Europe, 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 two in Canada, 36 , 37 two in both Europe and North America 38 , 39 and one in Japan. 40 As expected, the majority were observational studies (19/20) of which 11 were retrospective, and eight prospective. One sub‐analysis of a randomised controlled trial was included. There was a high rate of heterogeneity in study design and outcomes.
The percentage of patients achieving a given outcome for PASI75/90/100 and Physician Global Assessment are reported in Table S1. Mean PASI is displayed as an actual value, and mean PASI reduction as a percentage reduction from baseline.
3.3. Patient characteristics
Included studies contained reported data from 6495 patients (Figure 2), with sample sizes varying considerably from 16 to 3038 patients' data per study. On average 35.1% were female (range 14%–54%) and mean age was 49.7 years (range 42–59).
FIGURE 2.

The number of patients reported in the included literature by line of biologic or targeted small molecule drug.
3.4. Effectiveness of second‐line biologics in psoriasis
Eleven studies assessed the use of second‐line biologics and targeted small molecule drug, with or without a comparison to first‐line. 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 37 , 38 , 40 Of the six studies that directly compared first‐to second‐line biologics or targeted small molecule drugs, four found comparable PASI outcomes in first‐ and second‐line. 26 , 27 , 31 , 38 The LIBERATE study 38 was the only randomised controlled trial included, assessing apremilast versus placebo in biologic naïve patients, however also included an active comparator of etanercept. Patients within the active comparator line were switched to second‐line apremilast at 16 weeks, continuing to 52 weeks. PASI75 was similar in apremilast at week 52 in first‐line (53%) to week 36 in second‐line (57%), indicating similar PASI75 response for first‐ and second‐line biologic, however the study was not designed for first‐versus second‐line comparison.
In contrast, two studies found a higher PASI response in first‐line compared to second‐line, 30 , 40 with one study 40 reaching significance (p < 0.05). This study compared first‐ and second‐line biologics in a single centre group of patients (n = 326). A higher rate of PASI75 was found in first‐than second‐line at 14–16 weeks (59.1% vs. 43.7%), but mean PASI was significantly lower in second‐line (2.9) than first‐line (4.3). This discrepancy, with a greater PASI75 response in first‐line, but a higher mean PASI at 14–16 weeks, was due to the lower baseline PASI at the start of second‐line treatment.
The further five studies assessed second‐line treatment only, with no lines of comparison 24 , 25 , 28 , 29 , 37 : results shown in Table S1.
3.5. Effectiveness of third‐line + biologics in psoriasis
Nine studies assessed third‐ and later line biologic or targeted small molecules. 21 , 22 , 23 , 32 , 33 , 34 , 35 , 36 , 39 Four of the studies found a reduction in effectiveness in third‐ or fourth‐line, compared to first‐ or second‐line. 23 , 33 , 36 , 39 This included the largest study in this group, 39 PSO‐BIO‐REAL (n = 846), which was a multi‐national prospective study of biologic‐naive and ‐experienced patients over 12 months, to assess for complete skin clearance. Generally, the rate of PASI100 decreased with increased numbers of prior biologics: 25% at week 26 for first‐line compared to 14% for fourth‐line.
A diminishing response with successive lines of biologic was not however found in all included studies, with some finding varying differences in outcomes at different time points. A multicentre study 21 retrospectively assessed the use of risankizumab in 77 patients, finding the odds of achieving PASI75 were significantly lower in patients on 3rd+ line of biologic compared to first‐ and second‐line, at week 16 (p 0.018) however there was no difference between lines in achieving PASI75 at week 40. The real‐world use of secukinumab in two centres was retrospectively assessed, 22 with mean PASI reported as lower at week 12 with third‐line treatment (3.8) than first‐(5.3) and second‐line (4.6), but higher by week 40 (3.7 vs. 1.3 and 2.4).
Furthermore, two studies found a reduction in effectiveness (PASI75/90/100) beyond first‐line, but no difference between subsequent lines 32 , 35 and Papoutsaki et al 34 found a higher PASI90 at 24 weeks in fourth‐than third‐line adalimumab (100% vs. 63%) in a small open label single‐centre study. Notably, the frequency of adalimumab used was higher than currently licenced for psoriasis (40 mg weekly) which may explain the high effectiveness compared to other studies.
3.6. Comparison of studies
A meta‐analysis of the proportion of participants achieving PASI75 at 12–16 weeks, in the studies that recorded this outcome (16/20), found that effectiveness did not appear to reduce with successive lines of biologic (Figure 3). The pooled effect percentage of patients achieving PASI75 with 1st, 2nd, 3rd and 4th line biologics was 61%, 56%, 79% and 61% respectively. A meta‐analysis of PASI90 at 12–16 weeks in studies that included this outcome (10/20) found a pooled effect percentage achieving PASI90 of 46.1%, 39.9%, 55.8% and 33.7% in 1st to 4th line respectively (Figure 4). A meta‐analysis of PASI100 at 12–16 weeks (7 studies) found a pooled effect percentage achieving PASI100 of 36.7%, 30.3%, 46.7% and 30.4% in 1st to 4th line biologics respectively (Figure 5).
FIGURE 3.
(a) Meta‐analysis of PASI75 at 12–16 weeks for 1st and 2nd line. (b) Meta‐analysis of PASI75 at 12–16 weeks for 3rd and 4th line.


FIGURE 4.

Meta‐analysis of PASI90 at 12–16 weeks for 1st to 4th line.
FIGURE 5.

Meta‐analysis of PASI100 at 12–16 weeks for 1st–4th line.
3.7. Abstracts
Only one abstract of a small retrospective European study of 34 patients met inclusion criteria 41 ; results displayed in Table S2. This study assessed PASI90 response to second‐line adalimumab or ustekinumab after etanercept. A numerically but not statistically higher response was found in second line ustekinumab (PASI90 68.4%) compared to adalimumab (PASI90 46.6%) at 12 weeks.
3.8. Bias and quality assessment
Risk of bias was assessed for all included studies (Tables 1 and 2), with the overall risk of bias considered ‘serious’ or ‘of some concern’ for all studies. ROBINS‐I assesses bias by comparing an observational study to a ‘target randomised controlled trial’, or the ideal RCT that could answer the research question, whether or not this would be feasible in the real world. It is therefore inevitable that most observational studies will score seriously for bias, due to inherent limitations in study design when compared to an RCT, for example, selection bias. The GRADE criteria confirmed that the available evidence is of very low quality (Table 3). It is therefore important to interpret the meta‐analysis results with caution. However, these studies currently provide the best evidence available for understanding effectiveness of advanced lines of treatment in psoriasis.
TABLE 1.
Assessment of bias for included observational studies utilising the ROBINS‐I assessment tool.
| Study | Bias due to confounding | Bias in selection of participants | Bias in classification of interventions | Bias due to deviations from intended intervention | Bias due to missing data | Bias in measurement of outcomes | Bias in selection of reported result | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|
| Borroni 2021 | Serious | Serious | Low | No information | Moderate | Serious | Serious | Serious |
| Carpentieri 2020 | Serious | Serious | Low | No information | No information | Serious | Serious | Serious |
| Cozzani 2020 | Serious | Serious | Serious | No information | No information | Serious | Serious | Serious |
| Deza 2018 | Serious | Serious | Moderate | No information | Serious | Serious | Serious | Serious |
| Esposito 2019 | Serious | Serious | Moderate | Serious | No information | Serious | Serious | Serious |
| Galluzzo 2018 | Serious | Serious | Low | No information | Serious | Serious | Serious | Serious |
| Ganzetti 2018 | Serious | Serious | Moderate | No information | No information | Serious | Serious | Serious |
| Honda 2017 | Serious | Serious | Serious | No information | No information | Serious | Serious | Serious |
| Ozkur 2021 | Serious | Serious | No information | Serious | No information | Serious | Serious | Serious |
| Papoutsaki 2007 | Serious | Serious | Low | No information | No information | Serious | Serious | Serious |
| Piaserico 2014 | Serious | Serious | Moderate | No information | Low | Serious | Serious | Serious |
| Pitarch 2008 | Serious | Serious | Moderate | Serious | Moderate | Serious | Serious | Serious |
| Qiang 2016 | Serious | Serious | Serious | No information | No information | Serious | Serious | Serious |
| Ruiz Salas 2012 | Serious | Serious | Low | Moderate | Low | Serious | Serious | Serious |
| Sator 2015 | Serious | Serious | Moderate | Serious | Serious | Serious | Low | Serious |
| Seneschal 2020 | Serious | Serious | Serious | No information | No information | Serious | Serious | Serious |
| Talamonti 2018 | Moderate | Serious | Moderate | No information | Moderate | Serious | Serious | Serious |
| van Lumig 2010 | Serious | Serious | Serious | Moderate | Serious | Serious | Serious | Serious |
| Vender 2011 | Serious | Serious | Low | No information | No information | Serious | Low | Serious |
TABLE 2.
Assessment of bias for included sub‐analyses of randomised controlled trials utilising the Cochrane Risk of Bias 2 tool.
| Study | Bias arising from randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of outcome | Bias in selection of reported result | Overall risk of bias |
|---|---|---|---|---|---|---|
| Reich 2017 | Low | Low | Some concerns | Low | Some concerns | Some concerns |
TABLE 3.
Assessment of quality of eligible studies in PASI75 meta‐analysis, separated by line of biologic or targeted small molecule using GRADE criteria.
| Quality assessment of included studies in meta‐analysis of PASI75 | Effect | Quality | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of studies | Design of studies | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Number of patients included | Absolute (PASI75%) | Relative (95% CI) | |
| First line | ||||||||||
| 11 | 11 NRSI | Serious a | Some inconsistency b | Direct | No serious imprecision | None | 4208 | 61.0 | 47.0–74.2 | Very low |
| 1 RCT sub‐analysis | ⊕ΟΟΟ | |||||||||
| Second line | ||||||||||
| 14 | 14 NRSI | Serious a | Some inconsistency b | Direct | No serious imprecision | None | 745 | 56.1 | 41.9–69.9 | Very low |
| ⊕ΟΟΟ | ||||||||||
| Third/third + line | ||||||||||
| 5 | 5 NRSI | Serious a | Some inconsistency c | Direct | Some imprecision d | None | 85 | 79.0 | 65.3–90.0 | Very low |
| ⊕ΟΟΟ | ||||||||||
| Fourth/fourth + line | ||||||||||
| 3 | 3 NRSI | Serious a | Some inconsistency c | Direct | Some imprecision d | None | 73 | 61.0 | 43.4–77.3 | Very low |
| ⊕ΟΟΟ | ||||||||||
Abbreviations: CI, confidence intervals; NRSI, non‐randomised studies on interventions; PASI, psoriasis area severity index; RCT, randomised controlled trials.
Details of risk of bias of all studies present in Table 3.
Significant statistical heterogeneity and wide variation in effect estimates across studies.
Moderate statistical heterogeneity.
small sample size.
4. DISCUSSION
The overall aim of this systematic review was to evaluate the evidence of primary response of lines of biologics and targeted small molecules in psoriasis, beyond first line.
In qualitative assessment of eligible studies, PASI response to first‐ and second‐line biologics is often similar, but there is a variation in response to third‐line and beyond (Appendix S3). A meta‐analysis of PASI75/90/100 did not find a reduction in response to sequential lines of biologic/targeted small molecule beyond first line for all three outcome measures. In fact, pooled response to third line exceeded response to second line in all assessed outcome measures. However there was significant heterogeneity found within the studies, as well as very low numbers of included cases in the analysis of 3rd and 4th lines. It is possible that there was publication bias in the studies reporting later lines of therapy, leading to higher than expected responses to 3rd and 4th lines. The low sample sizes, heterogeneity and low quality of the studies limit the applicability of the meta‐analysis results.
The review only included studies assessing second and later lines of treatment, and therefore the assessment of response to first line is taken entirely from eligible studies that had a first line comparator. It is likely that if studies assessing first line alone had been included, within this line, bias would be lower and quality higher as a first line biologics would have been assessed in the context of randomised controlled trials.
There is overall very little data available at third‐line and beyond, with only 412 patients contributing to results at third‐ and fourth‐line, and no current evidence in the literature for response to biologics or targeted small molecules at 5th+ lines. Lower numbers of patients assessed in later lines reduced the power of eligible observational studies, often precluding statistical testing to assess for differences in outcome compared to first‐ and second‐line.
Relative PASI (PASI75/90/100) is conventionally accepted as the primary outcome measure for efficacy of psoriasis drugs. However it has been suggested that absolute PASI, for example, PASI < 3 or ≤ 2, is an additional relevant disease end point. 40 , 42 , 43 Relative PASI may be less appropriate to assess later lines of treatment, as baseline PASI at the start of successive lines of biologic tends to decrease, potentially leading to more difficulty in achieving relative PASI scores. 40 , 43 This could have played a role in the included studies due to the lack of wash out periods in most. This would lead to disease activity improvement from one line of treatment being carried over to the baseline of the next drug, particularly in cases where the drug was stopped due to factors other than efficacy, for example, adverse effects.
The review is limited to 12 months follow up, to focus on primary response, hence long‐term effectiveness is not assessed.
5. CONCLUSION
The current evidence available for effectiveness of advanced lines of biologic and targeted small molecule therapy for the treatment of psoriasis is primarily observational, at high risk of bias and of very low quality. Qualitatively, response in psoriasis to first‐ and second‐line biologics appears similar, with a reduction in response from third‐line suggested by individual studies but not confirmed by meta‐analysis. Meta‐analysis of PASI75/90/100 did not find a diminishment in effectiveness with sequential lines of treatment, but needs to be interpreted with caution. There is good evidence of a potential benefit to patients in later lines of treatment on a case‐by‐case basis. Further prospective studies are required to build an understanding of response to third‐line and beyond biologics in psoriasis.
AUTHOR CONTRIBUTIONS
Charlotte E. Gollins: Conceptualization (equal); data curation (lead); formal analysis (lead); methodology (equal); project administration (lead); writing – original draft (lead); writing – review & editing (lead). Rosie Vincent: Data curation (equal); formal analysis (equal); methodology (equal); writing – review & editing (equal). Caoimhe Fahy: Conceptualization (equal); methodology (equal); supervision (equal); writing – review & editing (equal). Neil McHugh: Conceptualization (equal); formal analysis (equal); methodology (equal); supervision (equal); visualization (equal); writing – review & editing (equal). William Tillett: Conceptualization (equal); methodology (equal); supervision (lead); visualization (equal); writing – review & editing (equal).
CONFLICT OF INTEREST STATEMENT
WRT has received research funding, speaker fees or honoraria from Abbvie, Amgen, Eli‐Lilly, GSK, Janssen, MSD, Novartis, Ono‐Pharma, Pfizer and UCB. CF has received honararia (speaker fees) from Pfizer and Eli Lilly. NJM has received a grant for unrelated work from UCB, honoraria (speaker fee) from Janssen and participated in data monitoring and safety in the NIHR HTA Astute trial. RV has received payment to her institution (speaker fees) from Leo Pharma and funding from Dermal to attend an educational event. CG has no conflicts of interest to declare.
ETHICS STATEMENT
Not applicable.
Supporting information
Supporting Information S1
Supporting Information S2
Supporting Information S3
Table S1
Table S2
ACKNOWLEDGEMENTS
We would like to thank Jason Ovens, Head of Library and knowledge services, Royal United Hospitals Trust, for his valuable help and guidance in undertaking the literature search. We would also like to thank Anita McGrogan for her crucial advice regarding statistics and meta‐analysis. This article received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
Gollins CE, Vincent R, Fahy C, McHugh N, Tillett W. Effectiveness of sequential lines of biologic and targeted small molecule drugs in psoriasis: a systematic review and meta‐analysis. Skin Health Dis. 2024;4(2):e350. 10.1002/ski2.350
DATA AVAILABILITY STATEMENT
No new data were generated or analysed in support of this research.
REFERENCES
- 1. World Health Organization . Global report on psoriasis. [Internet]. 2016. [cited 2023 Apr 1]. Available from: https://www.who.int/publications/i/item/9789241565189
- 2. Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ (Online). 2020;369:m1590. 10.1136/bmj.m1590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic arthritis. N Engl J Med 2017;376(10):957–970. 10.1056/nejmra1505557 [DOI] [PubMed] [Google Scholar]
- 4. Gelfand JM, Feldman SR, Stern RS, Thomas J, Rolstad T, Margolis DJ. Determinants of quality of life in patients with psoriasis: a study from the US population. J Am Acad Dermatol. 2004;51(5):704–708. 10.1016/j.jaad.2004.04.014 [DOI] [PubMed] [Google Scholar]
- 5. Taylor WJ. Impact of psoriatic arthritis on the patient: through the lens of the WHO International Classification of Functioning, Health, and Disability. Curr Rheumatol Rep. 2012;14(4):369–374. 10.1007/s11926-012-0263-5 [DOI] [PubMed] [Google Scholar]
- 6. Horn EJ, Fox KM, Patel V, Chiou CF, Dann F, Lebwohl M. Association of patient‐reported psoriasis severity with income and employment. J Am Acad Dermatol. 2007;57(6):963–971. 10.1016/j.jaad.2007.07.023 [DOI] [PubMed] [Google Scholar]
- 7. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. The Lancet (British edition). 2021;397(10281):1301–1315. 10.1016/s0140-6736(20)32549-6 [DOI] [PubMed] [Google Scholar]
- 8. Yiu ZZN, Mason KJ, Hampton PJ, Reynolds N, Smith C, Lunt M, et al. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: a prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2020;183(2):294–302. 10.1111/bjd.18981 [DOI] [PubMed] [Google Scholar]
- 9. Yiu ZZN, Becher G, Kirby B, Laws P, Reynolds NJ, Smith CH, et al. Drug survival associated with effectiveness and safety of treatment with guselkumab, ixekizumab, secukinumab, ustekinumab, and adalimumab in patients with psoriasis. JAMA Dermatol. 2022;158(10):1131–1141. 10.1001/jamadermatol.2022.2909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. van den Reek JMPA, Kievit W, Gniadecki R, Goeman JJ, Zweegers J, van de Kerkhof PC, et al. Drug survival studies in dermatology: principles, purposes, and pitfalls. J Invest Dermatol. 2015;135(7):1–5. 10.1038/jid.2015.171 [DOI] [PubMed] [Google Scholar]
- 11. Perrotta FM, Scriffignano S, Ciccia F, Lubrano E. Clinical characteristics of potential “difficult‐to‐treat” patients with psoriatic arthritis: a retrospective analysis of a longitudinal cohort. Rheumatol Ther. 2022;9(4):1193–1201. 10.1007/s40744-022-00461-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Reddy SM, Crean S, Martin AL, Burns MD, Palmer JB. Real‐world effectiveness of anti‐TNF switching in psoriatic arthritis: a systematic review of the literature. Clin Rheumatol. 2016;35(12):2955–2966. 10.1007/s10067-016-3425-4 [DOI] [PubMed] [Google Scholar]
- 13. Merola JF, Lockshin B, Mody EA. Switching biologics in the treatment of psoriatic arthritis. Semin Arthritis Rheum. 2017;47(1):29–37. 10.1016/j.semarthrit.2017.02.001 [DOI] [PubMed] [Google Scholar]
- 14.Chapter 25 Sterne JAC, Hernán MA, McAleenan A, Reeves BC, Higgins JPT. Assessing risk of bias in a non‐randomized study. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane handbook for systematic reviews of interventions version 6.3 (updated february 2022). Cochrane; 2022. www.training.cochrane.org/handbook [Google Scholar]
- 15.Chapter 8 Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane handbook for systematic reviews of interventions version 6.3 (updated february 2022). Cochrane; 2022. www.training.cochrane.org/handbook [Google Scholar]
- 16. Barker TH, Migliavaca CB, Stein C, Colpani V, Falavigna M, Aromataris E, et al. Conducting proportional meta‐analysis in different types of systematic reviews: a guide for synthesisers of evidence. BMC Med Res Methodol. 2021;21(1):1–189. 10.1186/s12874-021-01381-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Orbai AM, Husni ME, Gladman DD, Leung YY, Siebert S, Tillett W, et al. Secukinumab efficacy on psoriatic arthritis GRAPPA‐OMERACT core domains in patients with or without prior tumor necrosis factor inhibitor use: pooled analysis of four phase 3 studies. Rheumatol Ther. 2021;8(3):1223–1240. 10.1007/s40744-021-00337-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ozcelik S, Kilic FA, Basara R. Retrospective analysis of patients with psoriasis receiving biological therapy: real‐life data. Dermatol Ther. 2020;33(6):e14336. 10.1111/dth.14336 [DOI] [PubMed] [Google Scholar]
- 19. Sotiriou E, Bakirtzi K, Papadimitriou I, Tsentemeidou A, Kougkas N, Panagopoulou A, et al. Real‐life intraclass switch among IL‐17 inhibitors in psoriasis: results from a single‐centre, 24‐week, retrospective study. J Eur Acad Dermatol Venereol. 2022;36(11):e952–e953. 10.1111/jdv.18381 [DOI] [PubMed] [Google Scholar]
- 20. Berenguer‐Ruiz S, Rivera R, Herranz P, De la Cueva P, Hospital M, Ruiz‐Genao D, et al. Ustekinumab to guselkumab transitions: a series of 54 patients emulating the navigate trial in real life. Dermatol Ther. 2022;35(10):e15757. 10.1111/dth.15757 [DOI] [PubMed] [Google Scholar]
- 21. Borroni RG, Malagoli P, Gargiulo L, Valenti M, Pavia G, Facheris P, et al. Real‐life effectiveness and safety of risankizumab in moderate‐to‐severe plaque psoriasis: a 40‐week multicentric retrospective study. Acta Derm Venereol. 2021;101(11):a00605. 10.2340/actadv.v101.283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Carpentieri A, Mascia P, Fornaro M, Beylot‐Barry M, Taieb A, Foti C, et al. Effectiveness and safety of secukinumab in patients with moderate‐severe psoriasis: a multicenter real‐life study. Dermatol Ther. 2020;33(6):e14044. 10.1111/dth.14044 [DOI] [PubMed] [Google Scholar]
- 23. Cozzani E, Wei Y, Burlando M, Signori A, Parodi A. Serial biologic therapies in psoriasis patients: a 12‐year, single‐center, retrospective observational study. J Am Acad Dermatol. 2020;82(1):37–44. 10.1016/j.jaad.2019.05.064 [DOI] [PubMed] [Google Scholar]
- 24. Esposito M, Prignano F, Rongioletti F, Hansel K, Bianchi L, Pescitelli L, et al. Efficacy and safety of adalimumab after failure of other anti‐TNF alpha agents for plaque‐type psoriasis: clinician behavior in real life clinical practice. J Dermatol Treat. 2019;30(5):441–445. 10.1080/09546634.2018.1529382 [DOI] [PubMed] [Google Scholar]
- 25. Ganzetti G, Campanati A, Bettacchi A, Brandozzi G, Brisigotti V, Bugatti L, et al. Switching from a biological therapy to another biologic agent in psoriatic patients: the experience of PsOMarche group. G Ital Dermatol Venereol. 2018;153(1):5–10. 10.23736/s0392-0488.16.05463-8 [DOI] [PubMed] [Google Scholar]
- 26. Ozkur E, Kivanc Altunay I, Oguz Topal I, Aytekin S, Topaloğlu Demir F, Özkök Akbulut T, et al. Switching biologics in the treatment of psoriasis: a multicenter experience. Dermatology. 2021;237(1):22–30. 10.1159/000504839 [DOI] [PubMed] [Google Scholar]
- 27. Piaserico S, Cazzaniga S, Chimenti S, Giannetti A, Maccarone M, Picardo M, et al. Efficacy of switching between tumor necrosis factor‐alfa inhibitors in psoriasis: results from the Italian Psocare Registry. J Am Acad Dermatol. 2014;70(2):257–262. 10.1016/j.jaad.2013.10.019 [DOI] [PubMed] [Google Scholar]
- 28. Pitarch G, SanchezCarazo JL, Mahiques L, Oliver V. Efficacy of etanercept in psoriatic patients previously treated with infliximab. Dermatology. 2008;216(4):312–316. 10.1159/000113943 [DOI] [PubMed] [Google Scholar]
- 29. Sator P, Richter L, Saxinger W, Vasiljevic M, Stingl G. Adalimumab in the treatment of moderate‐to‐severe chronic plaque psoriasis in patients switching from other biologics. J Eur Acad Dermatol Venereol. 2015;29(9):1742–1749. 10.1111/jdv.12981 [DOI] [PubMed] [Google Scholar]
- 30. Talamonti M, Galluzzo M, Bernardini N, Caldarola G, Persechino S, Cantoresi F, et al. Psoriasis Area and Severity Index response in moderate‐severe psoriatic patients switched to adalimumab: results from the OPPSA study. J Eur Acad Dermatol Venereol. 2018;32(10):1737–1744. 10.1111/jdv.15077 [DOI] [PubMed] [Google Scholar]
- 31. Van Lumig PPM, Lecluse LLA, Driessen RJB, Spuls P, Boezeman J, Van De Kerkhof P, et al. Switching from etanercept to adalimumab is effective and safe: results in 30 patients with psoriasis with primary failure, secondary failure or intolerance to etanercept. Br J Dermatol. 2010;163(4):838–846. 10.1111/j.1365-2133.2010.09950.x [DOI] [PubMed] [Google Scholar]
- 32. Deza G, Notario J, Lopez‐Ferrer A, Vilarrasa E, Ferran M, del Alcazar E, et al. Initial results of ixekizumab efficacy and safety in real‐world plaque psoriasis patients: a multicentre retrospective study. J Eur Acad Dermatol Venereol. 2019;33(3):553–559. 10.1111/jdv.15288 [DOI] [PubMed] [Google Scholar]
- 33. Galluzzo M, Talamonti M, De Simone C, D’Adamio S, Moretta G, Tambone S, et al. Secukinumab in moderate‐to‐severe plaque psoriasis: a multi‐center, retrospective, real‐life study up to 52 weeks observation. Expert Opin Biol Ther. 2018;18(7):727–735. 10.1080/14712598.2018.1481503 [DOI] [PubMed] [Google Scholar]
- 34. Papoutsaki M, Chimenti M, Costanzo A, Talamonti M, Zangrilli A, Giunta A, et al. Adalimumab for severe psoriasis and psoriatic arthritis: an open‐label study in 30 patients previously treated with other biologics. J Am Acad Dermatol. 2007;57(2):269–275. 10.1016/j.jaad.2006.12.003 [DOI] [PubMed] [Google Scholar]
- 35. Ruiz Salas V, Puig L, Alomar A. Ustekinumab in clinical practice: response depends on dose and previous treatment. J Eur Acad Dermatol Venereol. 2012;26(4):508–513. 10.1111/j.1468-3083.2011.04325.x [DOI] [PubMed] [Google Scholar]
- 36. Qiang JK, Shahbaz A, Kim W, Marinas J, Greaves S, Yeung J. Effectiveness of sequential use of biologics in the treatment of moderate to severe psoriasis in real world Canadian academic clinical practice: a cohort study. J Am Acad Dermatol. 2016;74(1):176–177. 10.1016/j.jaad.2015.08.030 [DOI] [PubMed] [Google Scholar]
- 37. Vender R. An open‐label, prospective cohort pilot study to evaluate the efficacy and safety of etanercept in the treatment of moderate to severe plaque psoriasis in patients who have not had an adequate response to adalimumab. J Drug Dermatol. 2011;10(4):396–402. [PubMed] [Google Scholar]
- 38. Reich K, Gooderham M, Green L, Bewley A, Zhang Z, Khanskaya I, et al. The efficacy and safety of apremilast, etanercept and placebo in patients with moderate‐to‐severe plaque psoriasis: 52‐week results from a phase IIIb, randomized, placebo‐controlled trial (LIBERATE). J Eur Acad Dermatol Venereol. 2017;31(3):507–517. 10.1111/jdv.14015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Seneschal J, Lacour J, Bewley A, Faurby M, Paul C, Pellacani G, et al. A multinational, prospective, observational study to estimate complete skin clearance in patients with moderate‐to‐severe plaque PSOriasis treated with BIOlogics in a REAL world setting (PSO‐BIO‐REAL). J Eur Acad Dermatol Venereol. 2020;34(11):2566–2573. 10.1111/jdv.16568 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Honda H, Umezawa Y, Kikuchi S, Yanaba K, Fukuchi O, Ito T, et al. Switching of biologics in psoriasis: reasons and results. J Dermatol. 2017;44(9):1015–1019. 10.1111/1346-8138.13860 [DOI] [PubMed] [Google Scholar]
- 41. Garcia Gil S, Gutierrez Nicolas F, Nazco Casariego GJ, Bustinduy MG, Martín‐Neda FG, Ramos JR, et al. Ustekinumab and adalimumab for psoriasis patients who are no‐responders to etanercept: a comparative effectiveness study. Eur J Hosp Pharm. 2018;25((Suppl 1)):A110. 10.1136/ejhpharm-2018-eahpconf.237 [DOI] [Google Scholar]
- 42. Zweegers J, Roosenboom B, PCMvd K, van den Reek J, Otero M, Atalay S, et al. Frequency and predictors of a high clinical response in patients with psoriasis on biological therapy in daily practice: results from the prospective, multicenter BioCAPTURE cohort. Br J Dermatol. 2017;176(3):786–793. 10.1111/bjd.14888 [DOI] [PubMed] [Google Scholar]
- 43. Mahil SK, Wilson N, Dand N, Reynolds N, Griffiths C, Emsley R, et al. Psoriasis treat to target: defining outcomes in psoriasis using data from a real‐world, population‐based cohort study. Br J Dermatol. 2020;182(5):1158–1166. 10.1111/bjd.18333 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information S1
Supporting Information S2
Supporting Information S3
Table S1
Table S2
Data Availability Statement
No new data were generated or analysed in support of this research.