

Abstract
Background:
Virologic suppression has been defined using a HIV viral load of less than 1000 copies/ml. Low-level viremia (51–999 copies/ml) is associated with an increased risk of virologic failure and HIV drug resistance.
Methods:
Retrospective data from persons with HIV (PWH) who initiated ART between January 2016 and September 2022 in Nigeria were analyzed for virologic suppression at cut-off values less than 1000 copies/ml.
Results:
In 2022, virologic suppression at less than 1000 copies/ml was 95.7%. Using cut-off values of less than 400, less than 200 and less than 50 copies/ml, virologic suppression was 94.2%, 92.5%, and 87%, respectively.
Discussion:
Monitoring virologic suppression using lower cut-off values, alongside differentiated management of low-level viremia, may help Nigeria achieve HIV epidemic control targets.
Keywords: HIV-1, viral load, virologic suppression
Introduction
Effective HIV antiretroviral therapy (ART) decreases patient morbidity and mortality [1], and prevents sexual transmission when viral load is less than 200 copies/ml [2,3]. Expanding ART coverage and viral load monitoring are key components of the UNAIDS global strategy to achieve HIV epidemic control by 2030 [4]. Nigeria has a generalized HIV epidemic, with an estimated 1.9 million persons with HIV (PWH) in 2021 and 90% ART coverage, with over 1.73 million PWH on ART (https://www.unaids.org/en/regionscountries/countries/nigeria). By the end of September 2022, US President’s Emergency Plan for AIDS Relief (PEPFAR) supported 89.1% of all sites providing ART (n = 1,928) and 96.4% of the 1.96 million PWH on ART nationally (MOH program data). UNAIDS 95–95–95 Fast-Track targets require as part of the third 95 target that 86% of PWH achieve virologic suppression. The WHO has defined virologic suppression as less than 1000 HIV RNA copies/ml [5]. However, patients with low-level viremia (51–999 copies/mL) are at increased risk of virologic nonsuppression (≥1000 copies/ml) and failure (≥two consecutive virological nonsuppression results) [6], and HIV drug resistance [7–9], threatening Nigeria’s progress to reach HIV epidemic control by 2030.
Methods
We used retrospective longitudinal data of PWH who initiated and received at least 24 weeks of ART between January 2016 and September 2022 through support from PEPFAR in Nigeria to assess the status of virologic suppression at less than 1000 copies/ml compared with virologic suppression at lower cut-off values of less than 400 copies/ml, less than 200 copies/ml, and less than 50 copies/ml. We estimated the proportion of PWH on ARTwith virologic suppression using the latest viral load result per calendar year.
We analyzed differences in virologic suppression estimates across the cut-off values by sex and age. PWH who received PEPFAR-supported ART from 17 Nigerian states and who had at least one viral load result after at least 24 weeks on ART were included. When patients had more than one viral load in the year, we used the last viral load result per year. Key available demographic, clinical, and program-related variables were extracted from the Nigerian National Data Repository, a centralized data warehouse of regularly reported data from facility electronic medical record systems.
Ethical statement
The study received ethical approval from the Nigeria National Health Research Ethics Committee (NHREC/01/01/2007–13/11/2020). This project was reviewed in accordance with the US Centers for Disease Control and Prevention (CDC) human research protection procedures and was determined to be nonresearch.
Results
Data from 753 142 patients were abstracted, of whom 668 138 (88.7%) were included in the virologic suppression analysis (see Supplementary Table 1, http://links.lww.com/QAD/C940).
In 2022, virologic suppression rates at a cut-off of less than 1000 copies/ml were 95.7% compared with 72.3% in 2016. Similarly, virologic suppression rates at a cut-off of less than 50, less than 200, and less than 400 copies/ml were 87%, 92.5%, and 94.2%, respectively, in 2022 compared with 46.7%, 61.3%, and 67.1%, respectively, in 2016 (Fig. 1).
Fig. 1.
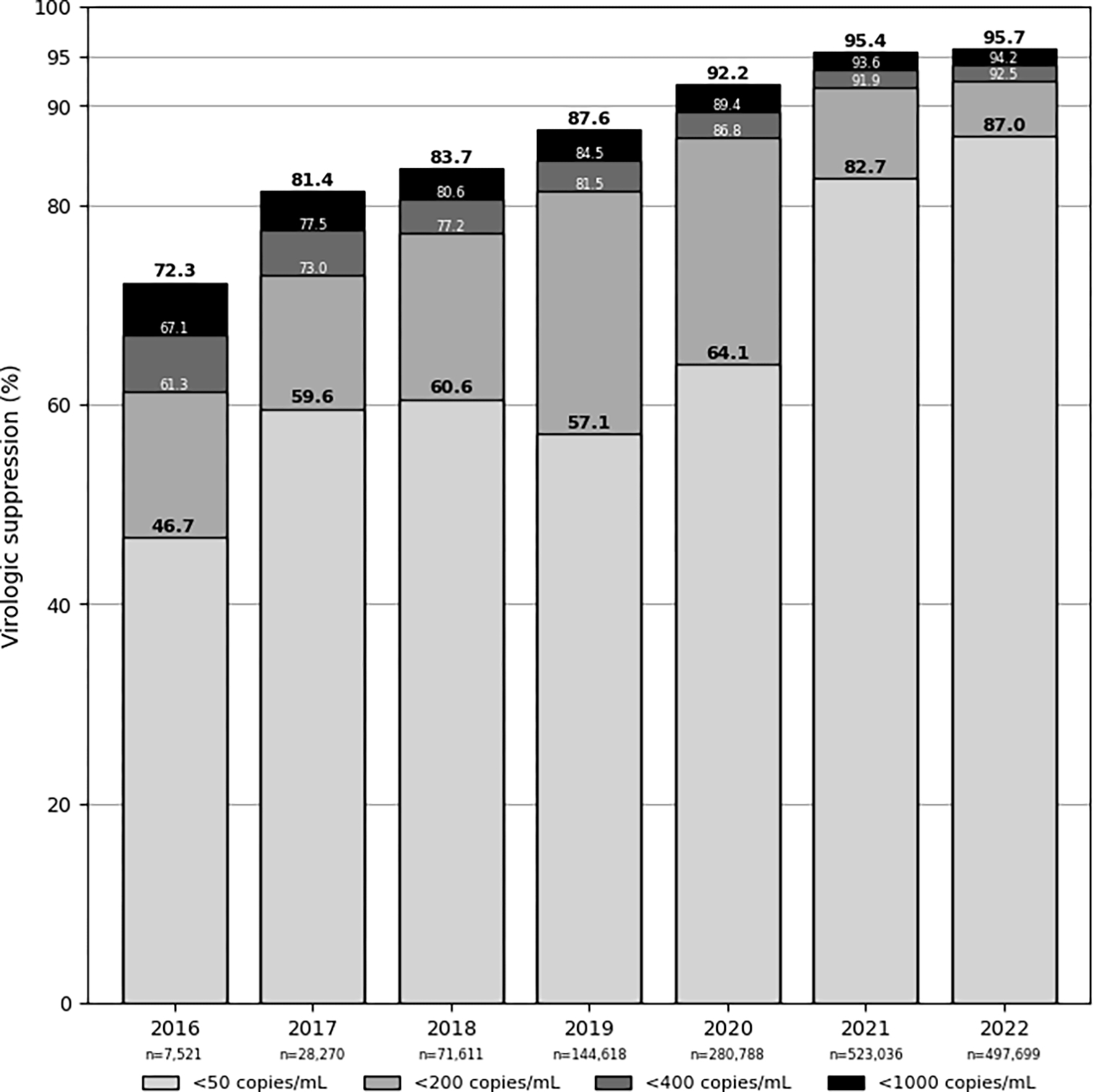
Virologic suppression prevalence estimates in relation to the third 95 of the 95–95–95 UNAIDS Fast-Track Targets by different viral load cut-off values.
Virologic suppression rates at all cut-off values improved over time by sex (Fig. 2a) and age (Fig. 2b). In 2022, virologic suppression at less than 50 copies/ml was observed in 86.5% and 87.8% of female and male individuals, respectively, and 74.2% and 87.5% in those less than 15 years and at least 15 years of age, respectively.
Fig. 2.
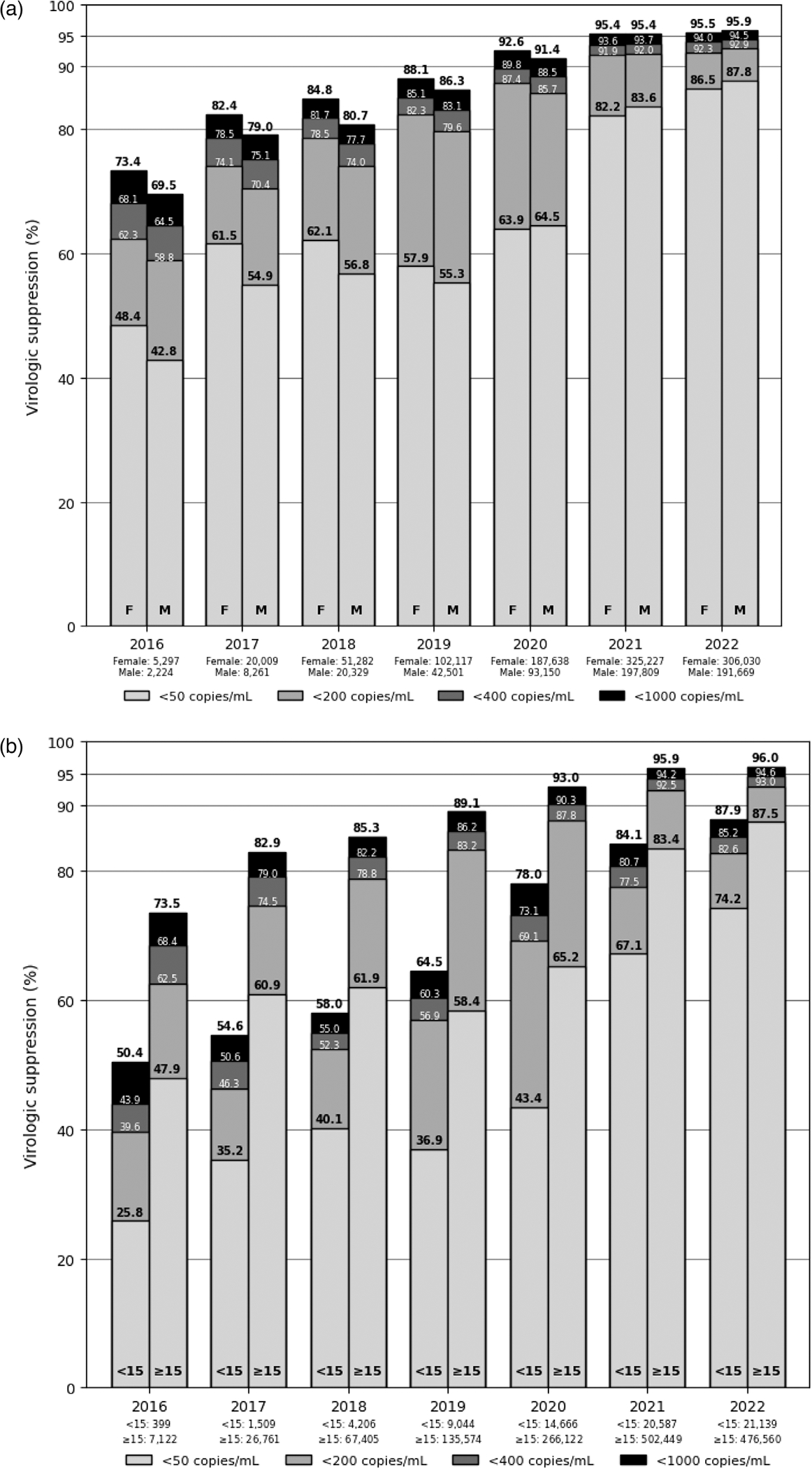
Virologic suppression prevalence and distribution by calendar year using different viral load cut-off values among persons with HIV on antiretroviral therapy by sex (a) and age (b), 2016–2022.
Discussion
Given the increased risk of virologic nonsuppression, virologic failure, HIV drug resistance, immune activation, inflammation, noncommunicable diseases, and serious non-AIDS events [10] associated with low-level viremia, monitoring virologic suppression at lower viral load cut-off values is important for understanding progress towards HIV epidemic control. As of 2022, the Nigeria program has not only achieved the third 95 of 95–95–95 at the less than 1000 copies/ml cut off value but has also achieved rates of virologic suppression at even lower cut off values of less than 50 copies/ml in 87% of PWH on ART with potential implications toward reduced morbidity, mortality, and transmission. Differences in virologic suppression rates by sex have lessened over time; however, children less than 15 years still lag behind with lower virologic suppression rates at all cut off values. For example, in 2022, 84.4% of PWH less than 15 years and 91.1% of PWH at least 15 years with viral load less than 1000 copies/ml also had viral load less than 50 copies/ml. This proportion of PWH at the lowest viral load cut off has increased over time; however, consistently remains lower for less than 15 years. This highlights the utility of reviewing data for action to identify ways to narrow the differences observed to ensure durable virologic suppression equity is achieved among all populations.
The Nigerian Federal Ministry of Health adopted into their HIV treatment guidelines [11] the expanded ART ‘Treat All’ approach at the end of 2016 with concomitant expansion of viral load monitoring to monitor treatment effectiveness with the scale-up of viral load testing laboratories and sample collection, primarily using plasma sample type, which has the limit of detection of less than 50 copies/ml. Since the launch of an ART surge in 2019 to rapidly increase the number of PWH diagnosed and receiving ARTand improve ARTadherence and retention, tremendous gains in the number of PWH receiving ART and viral load monitoring have been observed [12]. Monitoring progress towards virologic suppression using the cut off value of less than 50 copies/ml for all populations (sex, age), and identifying and addressing root causes for these disparities may help Nigeria achieve and sustain successful HIV epidemic control by 2030.
Supplementary Material
Acknowledgements
We thank the Nigerian Federal Ministry of Health, the National AIDS and STD Control Programme, viral load laboratories, implementing partners, and patients. This publication has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC).
Role of the funding source:
no specific funding was received for the analysis. HIV program support was provided by the President’s Emergency Plan for AIDS Relief through the CDC.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Disclaimer: the findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies. Applicable federal law for ethical review include: 45C.F.R. part 46.102(l)(2), 21C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S. C. §552a; 44 U.S.C. §3501 et seq.
References
- 1.Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet 2006; 367:817–824. [DOI] [PubMed] [Google Scholar]
- 2.Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med 2016; 375:830–839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, et al. , PARTNER Study Group. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA 2016; 316:171–181. [DOI] [PubMed] [Google Scholar]
- 4.Joint United Nations Programme on HIV/AIDS (UNAIDS). Fast-track: ending the AIDS epidemic by 2030. UNAIDS; 2014. Available at: https://www.unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf [Google Scholar]
- 5.World Health Organization. Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. WHO; 2021. Available at: https://www.who.int/publications/i/item/9789240031593. [Accessed 1 March 2023] [PubMed] [Google Scholar]
- 6.Chun HM, Abutu A, Milligan K, Ehoche A, Shiraishi RW, Odafe S, et al. , Nigeria Low-Level Viremia Investigation Group. Low-level viraemia among people living with HIV in Nigeria: a retrospective longitudinal cohort study. Lancet Glob Health 2022; 10:e1815–e1824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Delaugerre C, Gallien S, Flandre P, Mathez D, Amarsy R, Ferret S, et al. Impact of low-level viremia on HIV-1 drug-resistance evolution among antiretroviral treated-patients. PLoS One 2012; 7:e36673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Swenson LC, Min JE, Woods CK, Cai E, Li JZ, Montaner JS, et al. HIV drug resistance detected during low-level viraemia is associated with subsequent virologic failure. AIDS 2014; 28:1125–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Li JZ, Gallien S, Do TD, Martin JN, Deeks S, Kuritzkes DR, Hatano H. Prevalence and significance of HIV-1 drug resistance mutations among patients on antiretroviral therapy with detectable low-level viremia. Antimicrob Agents Chemother 2012; 56:5998–6000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Crespo-Bermejo C, de Arellano ER, Lara-Aguilar V, Valle-Millares D, Gómez-Lus ML, Madrid R, et al. Persistent low-level viremia in persons living with HIV undertreatment: An unresolved status. Virulence 2021; 12:2919–2931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Federal Ministry of Health (FMOH). (2016). National guideline for HIV prevention, treatment, and care. Abuja, Nigeria: FMOH. Available at: https://www.prepwatch.org/wp-content/uploads/2017/08/nigeria_national_guidelines_2016.pdf. [Accessed 1 March 2023] [Google Scholar]
- 12.Dirlikov E, Jahun I, Odafe SF, Obinna O, Onyenuobi C, Ifunanya M, et al. , CDC Nigeria ART Surge Team. Rapid scale-up of an antiretroviral therapy program before and during the COVID-19 pandemic - nine states, Nigeria, March 31, 2019-September 30, 2020. MMWR Morb Mortal Wkly Rep 2021; 70:421–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.