

Abstract
Emerging evidence suggests that 40 Hz auditory stimulation may benefit cognition. Nested within a randomized crossover trial, this qualitative study evaluates the acceptability and experience of three auditory interventions—self-selected music, 40 Hz sound, and a novel combination, termed 40 Hz music—in individuals with Mild Cognitive Impairment (MCI), Semi-structured interviews were conducted with individuals with MCI post-intervention exposure. Findings indicated a preference for self-selected music due to its memory-boosting and emotional benefits, while responses to 40 Hz sound were mixed, with several participants reporting discomfort. The composite 40 Hz music intervention showed promise, striking a balance by enhancing user experience and mitigating the 40 Hz sound’s negative aspects. Engagement was influenced by personal music interests, listening routines, and support networks. This study highlights the potential of integrating 40 Hz sound with personalized music to offer a more acceptable 40 Hz auditory intervention for cognition in older adults with MCI.
Keywords: Mild cognitive impairment, dementia, gamma waves, 40 Hz, music therapy, cognitive health
Background
With the growing population of older adults, cognitive impairment and dementia have become prominent public health concerns worldwide1,2. Mild cognitive impairment (MCI) affects around 20% of individuals aged 65 years or older3,4 and represents a level of cognitive decline that exceeds generally expected age-related changes. It is often considered a transitional or prodromal phase between normal cognitive aging and dementia. Approximately 18.4% of those older adults with MCI develop dementia in one year and about one-third develop Alzheimer’s disease (AD)-related dementia within five years3,5–8. This risk highlights the critical importance of targeted interventions and prevention strategies at the MCI stage to mitigate the progressions toward dementia.
Neural oscillatory activity in the gamma range (~25–100 Hz) is thought to reflect bursts of spiking activity that are essential for memory and cognitive processes9,10. These oscillatory patterns are manifestations of electrical activity in the brain, originating from neuronal (nerve cell) activity, with their frequencies (measured in Hz) being directly quantifiable. Alterations in gamma neural activity have been noted in transgenic mouse models and humans in early or presymptomatic stages of AD10–14. These aberrations are linked to accelerated AD progression, marked by an increase in amyloid-β plaques, a precursor to AD10,11. Gamma frequency auditory stimulation, particularly at 40 Hz, is emerging as a non-pharmacological avenue for enhancing cognitive function in individuals with MCI and AD. Notably, 40 Hz stimulation achieves better gamma entrainment than stimulations at other frequencies, such as 8 Hz or 80 Hz9,15,16. In transgenic mice, 40 Hz auditory stimulation for seven days led to a nearly 50% reduction in amyloid-β plaque and tau accumulation within the hippocampus15–17. Preliminary findings in human AD models reinforce these mice model studies, suggesting that gamma entrainment at 40 Hz may mitigate memory impairments18–21, especially in individuals with MCI or AD22–24.
Various 40 Hz entrainment methods have been tested, including audio-visual stimulation with sound and light flickering. However, long-term visual stimulation may be risky, especially for those with conditions like photosensitive epilepsy, limiting its safety21,25. Recent studies support the effectiveness of stand-alone 40 Hz sound stimulation26. However, enhancing the appeal and enjoyment of interventions is a crucial factor in securing active participant engagement and achieving sustained long-term clinical benefits20,22,27,28. Although there are promising cognitive benefits from 40 Hz auditory stimulations, a notable challenge is that 40 Hz sound may be perceived as perturbing or displeasing27,28,43. Currently, research on older adults’ experience with 40 Hz auditory intervention is lacking, and questions remain about the feasibility and sustainability of this as a cognitive-enhancing treatment for older adults.
Music listening has emerged as another promising non-pharmacological auditory intervention for cognitive aging. As a multimodal stimulus, music can elicit visual, auditory, and motor responses29, such as visual reminiscences, spontaneous physical movements, and persistent mental replay of music. Music interventions have also demonstrated improved executive function, episodic memory, and overall cognitive function among those with MCI and dementia, with added benefits for verbal fluency in dementia30,31. In particular, personalized self-selected music has amplified the effects of existing music interventions by engaging meaningful autobiographical memories among persons with AD and has led to improved physical, cognitive, and socio-emotional outcomes32–35.
To enhance the participants’ engagement and their listening experiences, we have developed a modified 40 Hz intervention, 40 Hz music, combining self-selected music with 40 Hz sound stimulation. While existing research substantiates the potential of 40 Hz stimuli and self-selected music in isolation, there remain knowledge gaps in auditory acceptability, feasibility, and the potential of the two modalities together. In making this novel composite intervention, the goal was to enrich the overall auditory experience by including self-selected music while maintaining the audibility of the 40 Hz sound. In this study, we aim to understand participant acceptability and auditory experiences across three auditory modalities: self-selected music alone, 40 Hz sound alone, and 40 Hz music—providing insights for developing sustainable auditory interventions for long-term implementation among individuals with MCI.
Method
Study Design Overview
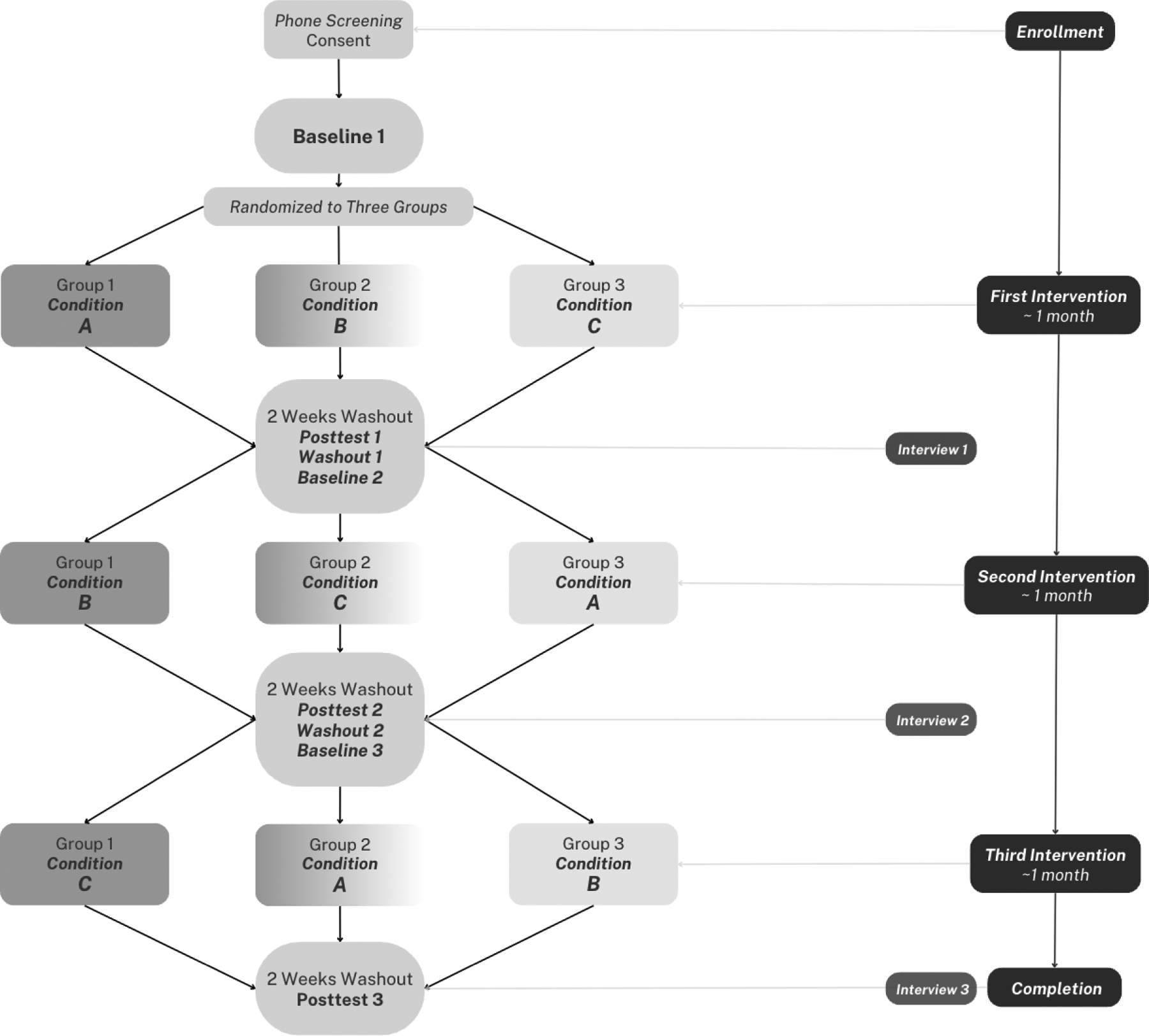
This qualitative study is nested in an ongoing prospective randomized controlled crossover trial that aims to evaluate the feasibility and preliminary acceptability of three distinct auditory interventions: (Condition A) Self-selected music alone; (Condition B) 40 Hz sound alone; and (Condition C) 40 Hz music, which combines 40 Hz sound with self-selected music. In the parent study, participants underwent all available conditions sequentially, with 2-week washout periods interposed between conditions in randomized assigned orders (Group 1, 2, 3). The protocol used in the parent study was approved by Johns Hopkins Medical Institutional Review Board, and participants were compensated $350 for completing the study.
Participants
We recruited community-dwelling older adults living in Baltimore, Maryland, through community events at senior-living apartments, libraries, community centers, churches, and social media platforms. The inclusion criteria of the study include individuals aged 50 and above, community-dwelling, English-speaking, MCI status (Montreal Cognitive Assessment [MoCA scores: 18 to 25] and the Functional Activity Questionnaire [FAQ scores < 6]). People with one or more diagnoses of schizophrenia, Parkinson’s disease, severe hearing impairment, or acute medical conditions were ineligible to participate in the present study.
Study Procedure
During the consent process, we incorporated additional steps to ensure participants fully understood and provided informed consent. This included adding targeted questions in specific sections of the consent form which helped confirm their comprehension at each stage of the consent process. The enrolled participants were randomized into one of three treatment sequences as follows: A-B-C (Group 1), B-C-A (Group 2), and C-A-B (Group 3). During each treatment, the participants were asked to listen to the assigned condition for one hour daily, five days a week, over four weeks. Individual interviews about their experience with each condition were conducted with participants who consented to voice recording. To minimize potential carryover effects, these qualitative post-test data were collected after each treatment phase following a two-week washout period before the subsequent treatment condition phase. Following the final treatment phase, the interviews included questions comparing all three of the conditions. This data was collected anonymously as the parent study is longitudinal in nature. Figure 1 provides an overview of the study timeline and depicts each participant’s possible sequence of condition group assignments (A, B, C) from the baseline to the posttest assessments. Study team members provided follow-up calls, text reminders, and at-home support for participants (if needed) through each of these steps.
Figure 1:
Parent Study Design
Interventions
After completing baseline data collection, participants were guided through at-home listening practices. The study team helped create a comfortable audio station at each participant’s home, supplying a Samsung Galaxy 8.7’ Tab A7 Lite with a grey magnetic tablet book cover or a Sony Walkman MP3 Player if the participant’s home did not have a stable Wi-Fi connection (refer to Figure 2). During this setup, the volume was adjusted in person to ensure both safety and comfort, a step repeated for each new auditory condition. The team members were trained to adequately instruct participants and configure devices across two home visits for the initial condition and one home visit for the subsequent two conditions. This procedure included establishing a Wi-Fi connection (if available), introducing the tablet/MP3 device, guiding participants through the auditory app (for tablet users), setting up the headphone volume, providing troubleshooting guidance, and setting up the text message surveys on the participants’ phones. Some questions asked during text message surveys included whether participants listened to audio the day prior, duration, time of listening, and any potential discomfort. A note with the study team’s contact information was attached to the device for easy access in case of any issues with the device.
Figure 2:

Music/Sound Listening Devices for Participants
Participants received guidance to dedicate an hour to listening—preferably at least 3 hours prior to bedtime—with a recommendation to concentrate exclusively on the audio during this time. If other activities were necessary, they were advised to choose tasks that were not mentally strenuous, such as walking or simple household chores. To support adherence to this routine, daily reminders and surveys were dispatched through text messages, and a member of the research team made weekly follow-up calls to reinforce commitment to the protocol. Listening time was also tracked through the auditory app used on the Samsung tablet, and in a listening diary for those using MP3.
Condition A – Self-Selected Music
A personalized music playlist of approximately 30 to 60 songs was assembled, drawing from each participant’s preferred music. During baseline data collection, participants completed the “Assessment of Personal Music Preference” questionnaire and selected their favorite songs from an existing music library. Additional songs were added intermittently according to participant preferences.
Condition B – 40 Hz Sound
The 40Hz soundtrack consisted of a 1 ms sound clip with a 17000 Hz base frequency, 7000 Hz modulation depth, and −10.3 dB amplitude. It was followed by a 25 ms silent interval with a 0.1 Hz base frequency, and both modulation and amplitude values set to zero. This 25 ms unit was repeated 40 times per second. The 40 Hz sound is often likened to a buzzing noise, reminiscent of TV static, or the chirping sounds of cicadas.
Condition C – 40 Hz Music
Custom 40 Hz music playlists comprising approximately 30–60 tracks were created for each participant. The unaltered musical soundtrack was analyzed for spectral frequency and spectral pitch. Subsequently, the 40Hz soundtrack was integrated with the musical track. To ensure a balanced listening experience, the volume of the 40 Hz soundtrack was adjusted to match the volume envelope of the music’s decibel level. This volume match-up aimed to render the 40 Hz sound audible throughout the musical piece, enhancing the overall 40 Hz music stimulation experience.
Participant Interviews
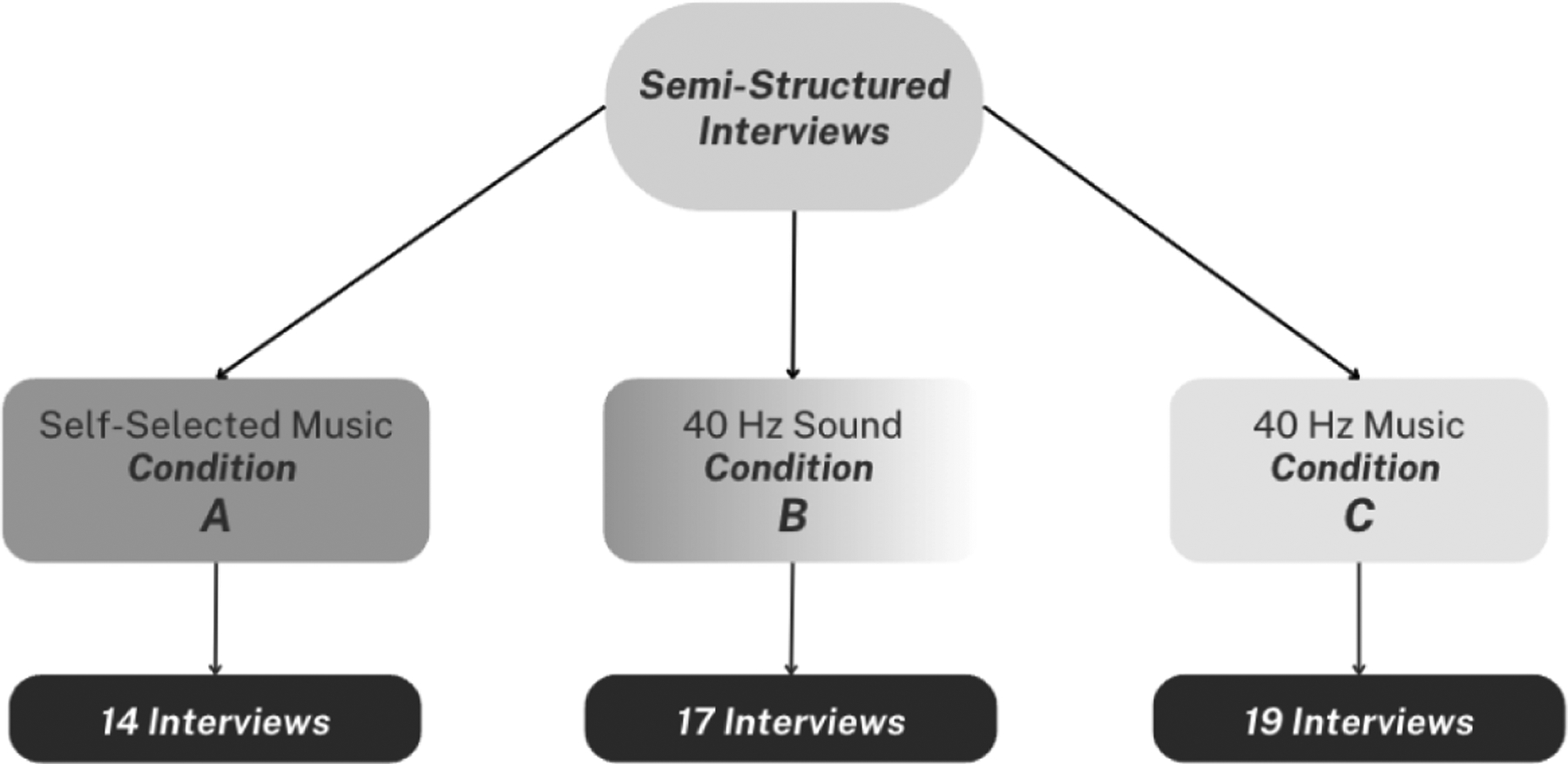
We conducted semi-structured interviews with 25 participants across the three condition groups. Interviewers were primarily study team members with whom the participants had previously interacted with during written consent and in-person baseline assessments. All study members received thorough study related interview training during orientation and dedicated team training sessions before conducting any participant interviews. Additionally, the first three supervised practice interviews with participants were conducted for further interviewer training and development. To ensure the quality and effectiveness of the interviews, random fidelity checks were performed with recordings and transcripts throughout the intervention, focusing on the quality of questions, effective probing, and the comfort of both participants and interviewers. The project’s study coordinator and qualitative data analysts were tasked with managing the quality checks. Their findings and updates were regularly reported at weekly team meetings to maintain open and consistent communication. If necessary, it could translate to a more thorough training day after consulting with knowledge experts. Figure 3 illustrates the distribution of participant interviews from each intervention: 14 transcripts for Condition A (self-selected music), 17 for Condition B (40 Hz sound), and 19 for Condition C (40 Hz music). Of these 50 transcripts, 9 participants underwent all three conditions, 7 underwent two conditions, and 9 underwent one condition. Interviews focused on the most recent condition, except for the last interview, where purposive questions were asked about all three conditions. However, participants often compared perceptions of the different conditions they had experienced if they were in their second or third condition at the time of the interview. Before the interviews, participants were informed of the study’s overarching objectives during screening and written consent procedures. Interviews were typically conducted in participants’ homes or at the Johns Hopkins School of Nursing. For those with transportation constraints, the study offered Lyft services to ensure participants’ access to the campus.
Figure 3:
Completed Participant Interviews
The average interview duration was approximately 10 minutes, ranging from 4 to 40 minutes. Overall, semi-structured interview guides for Posttests 1 and 2 were shorter, and those for Posttests 3 were more comprehensive to account for the participant having finished all three interventions. Most interviews were situated between 15–20 minutes, with a few outliers including that of our minimum and maximum interview times. Broad interview categories and sample questions are illustrated in Figure 4, ranging from the routine of listening, sound or music impressions, comfort, to more recruitment and retention-based questions. Trained interviewers from the study team employed more probing inquiries within each category.
Figure 4:

Interview Categories and Sample Questions Asked
Analysis
Following HIPAA regulations, the audio-recorded interviews were transcribed verbatim and subsequently de-identified by a third-party transcription service. These transcripts were then verified against original recordings for accuracy. The de-identified transcripts were then imported into MAXQDA for coding and thematic analysis.
We employed an abductive qualitative methodology, which neither relies solely on empirical data nor starts with preconceived hypotheses36. It involves an equitable and simultaneous consideration of both empirical data and theorizing of the most plausible explanation. Its primary goal is to identify the most rational and practical explanation for observed phenomena. Our process started with transcript familiarization, where the primary coders (CW and ML) identified recurring patterns and potential code categories. While a structured and a priori coding approach was employed to explore factors related to intervention acceptability, we remained receptive to unforeseen code patterns and relationships as long as they were theorized based off existing data. An open coding approach was used to capture approximately 53 derived preliminary coding categories. The primary coders shared these initial code results with the team to be refined and specified through team reviews. After subsequent team reviews, these codes were then consolidated into ten primary and 44 secondary categories to facilitate ease of coding.
Following the finalization of the codebook, coding comparisons were conducted between the two primary coders to ensure coder reliability, with other team members involved in data collection to act as third coders when needed. Following multiple iterations of manual code cross-checking within the same transcripts, once consensus was achieved among the primary coders and an acceptable level of reliability was established, subsequent coding was carried out independently. Periodic quality checks were implemented to uphold fidelity throughout the process.
Results
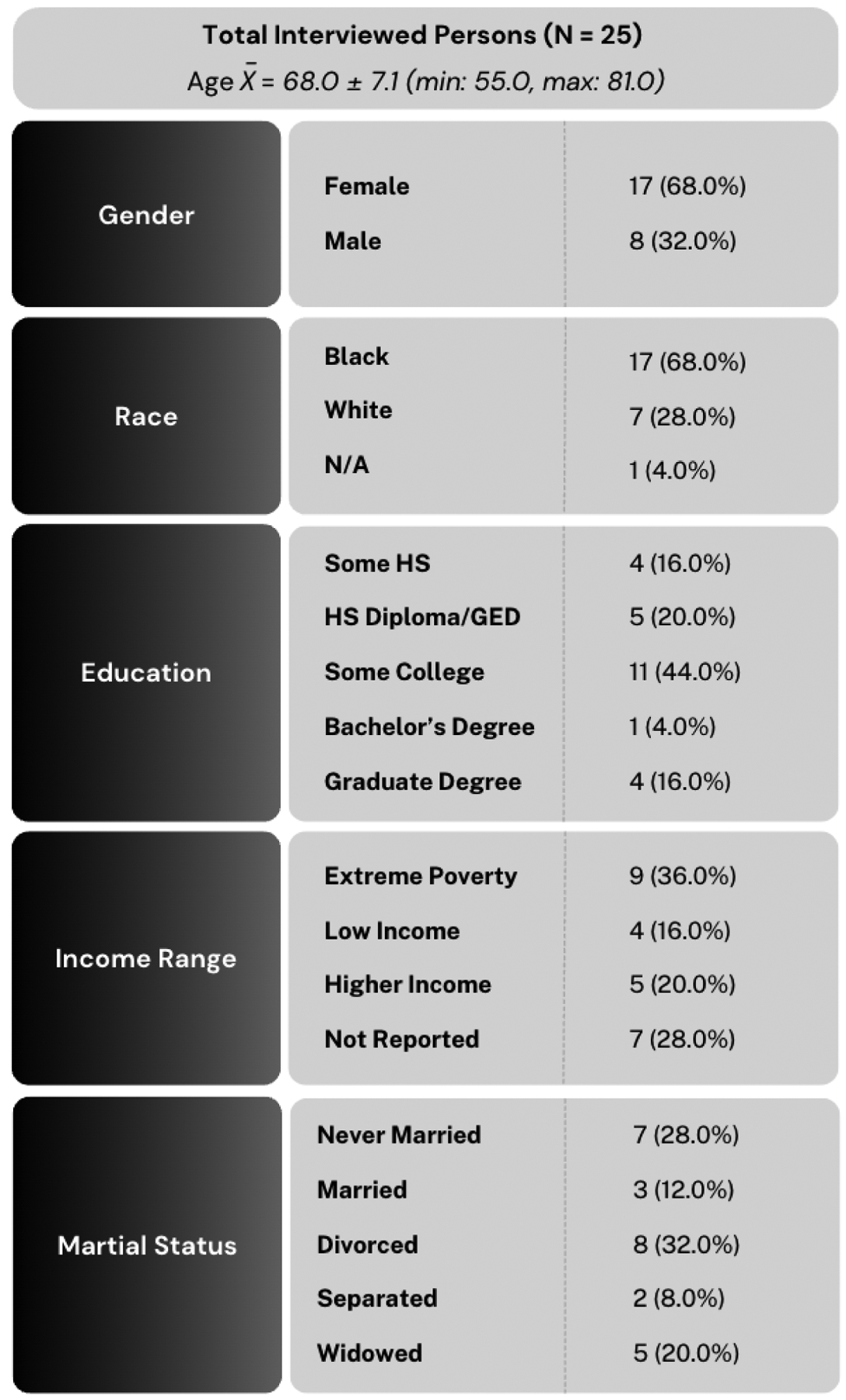
We interviewed 25 participants in total, with an average age of 68 years. The majority of participants were women (68%), identified as Black/African American (68%), and nearly half reported some college education (refer to Figure 5). Additionally, 50% (n = 9) of the 18 participants who reported participant incomes were below the Maryland extreme poverty threshold. Data on intervention adherence were not yet available at the time of writing.
Figure 5:
Demographic Results from Total Interviewed Persons (N = 25)
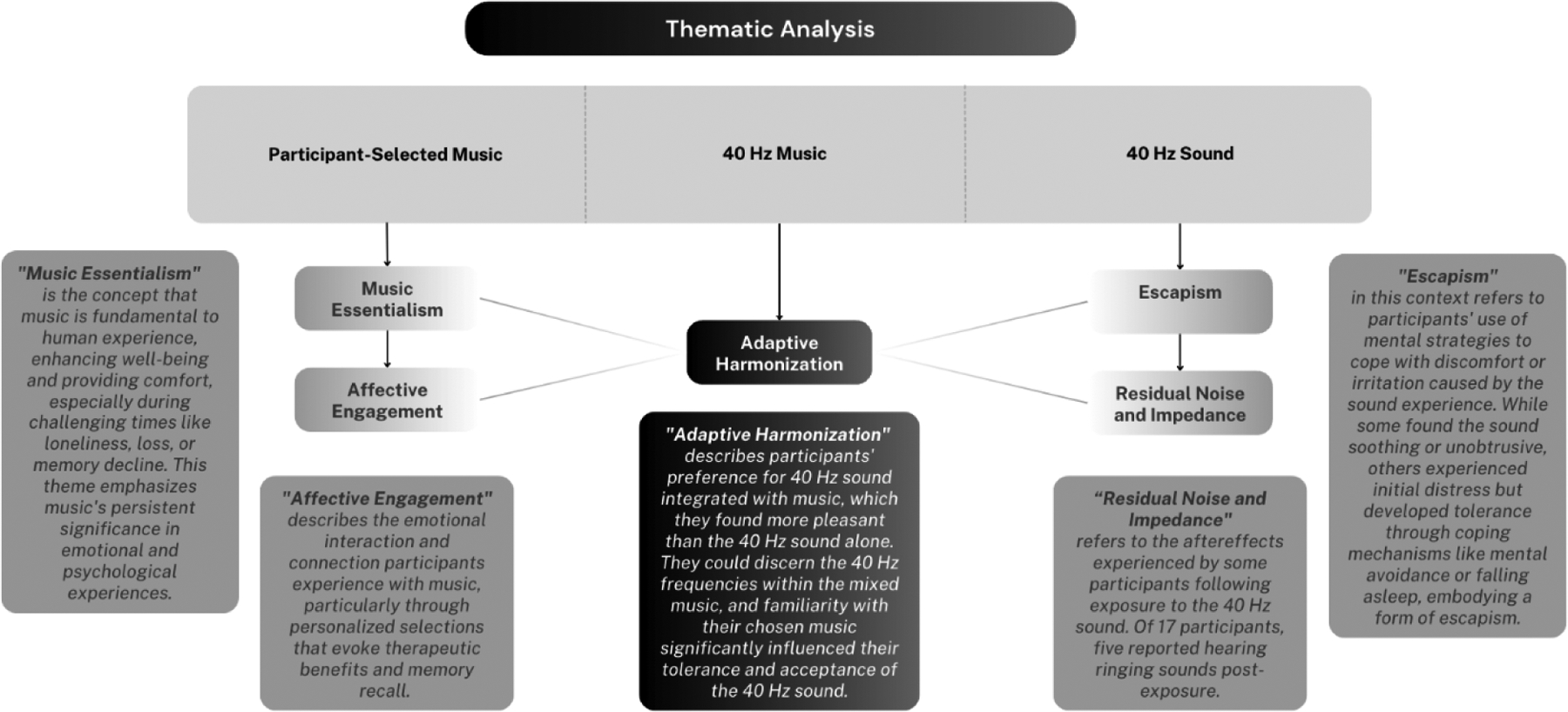
Our analysis highlighted varying levels of acceptability across the three intervention groups. Employing a crossover research design, participants experienced one to three conditions based on their progress through the project. This approach allowed the nine participants who had completed all three conditions to serve as their own control, reducing variability between those subjects when comparing between conditions. We distilled our observations from 50 transcripts into five primary themes: music essentialism, affective engagement, escapism, residual noise and impedance, and adaptive harmonization. These themes are categorized under the respective intervention headings of self-selected music, 40 Hz sound, and 40 Hz music. Additionally, we introduced a feasibility category to capture insights for future auditory interventions.
Self-Selected Music
Music Essentialism
Participants demonstrated a strong connection to music, anchored by a core belief in its essential function for maintaining memory and fostering emotional health. The customization of chosen tracks seemed to aid in recollections. Many participants opted for songs from their youth, which they said triggered vivid memories of distinct times, locations, and events in their lives. Additionally, some highlighted the crucial role music played in inspiring, energizing, and being an integral part of life.
Yeah, it makes me feel good. It makes me feel great. It makes me… Well, I’m not supposed to think because I think about certain songs and makes me think about what I was doing at that time in my life […] I mean, you can’t help it - I mean, because every song is associated with something within your life. Music is the key to life. It unites everyone.
(Female, 66 years old, second condition)
The self-selected music functioned as a therapeutic tool, uplifting their mood while also stirring participants’ memory and sense of self. Participants’ narratives underscored the power of self-selected music in providing emotional solace, support during grief, relief from stress, and a connection to significant memories from their lives. There was also a degree of helpfulness in which music listening had assisted with recovering or remembering past experiences.
I was lonely at one time. The music takes that away. I miss my wife. The music helped me remember the days we were together. How much fun we had. Sometimes I have tears because I’m missing her. It’s not a bad thing to cry. It’s good sometimes. So, it’s uh, music is a very instrumental part of your life. Because if you listen, It’s around you all the time.
(Male, 70 years old, second condition)
One participant reflected on music’s enduring impact, stating that the last remnants of a person’s memory and essence often reside in music, songs, and singing. That participant recalled that their spouse, despite late-stage Alzheimer’s disease, could sing songs from her past during the final week of her life.
I’ll be the first one to tell you, my wife could still sing a week or two before she passed away but she didn’t know who I was or what was going on. But she hears a song come on, she’d sit there and sing it. And music is one of the last things a person with dementia or Alzheimer’s loses … trust me. That’s coming with first-hand experience […] And my wife could … she could sing songs if they come across the radio and even when we went to church, she was right along with the tune.
(Male, 70 years old, first condition)
Affective Engagement
Pre-existing music habits significantly boosted participant engagement, particularly noticeable in those with established routines for listening to music. Some participants pointed out that the required one-hour daily listening session disrupted their usual music-listening practices or was insufficient.
I mean, you know, um. Just the music, because we only did it for an hour - it could be a little longer, you know, because you know […] Yeah, I enjoy it.
(Female, 67 years old, third condition)
The ability to personalize their song choices played a crucial role in engaging participants emotionally. This personalization resulted in a broad spectrum of emotional responses, ranging from joy to calmness, influenced by the song’s genre or tempo.
I could take the music along when I walk, which helps me you know, and helps keep me relaxed because I walks when I get upset, to calm myself right to deal with whatever the world throws at me at the time I find hard to take. Music is really calming. It’s better than medicine. It’s the best medicine to tell you the truth […] It just depends on how I feel. It’s not - I don’t look for specific thing just to listen to music. If I feel music, I feel it.
(Male, 70 years old, second condition)
Additionally, this customization allowed participants to experience familiar songs in new ways, bringing a sense of novelty and excitement to their listening sessions. Overall, the enjoyment derived from music, the resurgence of memories, and the ease of engaging in the activity—all contributed significantly to enhancing participants’ belief in the potential for improved memory retention.
It brought back a lot of memories. Yes. Which is a good thing. I think it’s a good thing because it helps me. It helps me to realize that all is not totally lost when it comes to my memory.
(Female, 71 years old, third condition)
As the intervention continued, some participants raised concerns about the possibility of the listening experience becoming monotonous, particularly if their song choices were limited. Many expressed a desire to prolong their favorite songs, introduce more variety by adding different genres, songs in other languages, or songs from various eras to maintain engagement and enjoyment.
Good, fine. I have noticed that it’s getting repetitive. I’m starting to learn the words a little better. But I think I might need more songs because I’m getting kind of bored. And I’ll find that I’m flipping through them sometimes.
(Female, 60 years old, first condition)
40 Hz Sound
Escapism
Challenges arose during the 40 Hz sound intervention, with a division in participant responses. Nine of the 17 participants reported adverse reactions such as irritation, discomfort, and a sense of distress, highlighting the challenges of engaging with the 40 Hz sound, particularly for extended periods beyond the study duration. The remaining eight participants had no issue with the sound and described it as either background noise or as soothing and relaxing.
No [emphasized], I don’t think it’s reasonable to listen to that sound for an hour out of the day, because it’s annoying for a person that just starting. What, uh, then you figure out a way to deal with it? And that’s what you do. You just deal with it […] It is not reasonable, no. Only if you have to listen to it.
(Male, 75 years old, first condition)
I guess something not as harsh. This seemed harsh to me. I guess I would relate it to almost a torture that they used on prisoners in war. They would put a sound in a room. They’re isolated in a room and just put a sound to the room.
(Male, 70 years old, first condition)
As the intervention progressed and in subsequent post-test interviews, 3 of the 9 participants who were initially averse to the sound reported that it became a bit more tolerable. They developed strategies to mentally block out the sound, combined listening sessions with other activities, or used the sound as a pre-sleep relaxation tool. Over time, continued engagement led to increased feelings of calmness and the establishment of a routine. However, this often resulted in deviations from the intervention, such as falling asleep during sessions, watching TV, avoidance of listening, or adopting other listening strategies that diverted attention away from the 40 Hz sound, potentially diminishing the intervention’s effectiveness. This phenomenon of seeking distractions to mediate a discomfortable listening experience, inspired the theme of Escapism.
Ah yes sleeping, helps me to relax, so I’m able to go to sleep.
(Female, 69 years old, second condition)
You had to program yourself to try to relax and not let it get the best of you, because it would drive you crazy if-- well, it’ll raise your anxiety-- I’m not gonna say “drive you crazy”-- if you allow it to, so I had to reprogram my mind like “This is just a test. This supposed to relax me under a circumstance that’s-- I have to do this.” So other than that I felt like it was an experiment […] I would get a slight headache when I listened to it back-to-back, so I noticed if I skip a day or two I wouldn’t feel like I’m tense and like I’m getting a headache, and that’s the side effects that I got from it.
(Female, 66 years old, third condition)
Residual Noise and Impedance
Five of 17 participants noted ringing sounds post-exposure to the 40 Hz sound intervention. The lingering noise continued, with durations ranging from 5 to 20 minutes for two participants. Two others experienced intermittent sounds later the same day, and one participant reported the sound lasting over an hour. This led to feelings of irritation and discomfort, negatively impacting their motivation to participate. Furthermore, dedicating time for uninterrupted sound listening became a challenge as the task lost its appeal for these participants.
Dislikes was like I said in the beginning that humming sound after I finish for about an hour. Zinging sound.
(Male, 75 years old, first condition)
On various times during the day, and the only thing that irritated me was that when I stopped listening, I could still hear it […] for 15 to 20 minutes.
(Female, 68 years old, second condition)
After we finished? It made my ears buzz for at least about 5–6 more minutes
(Male, 56 years old, first condition)
40 Hz Music
Adaptive Harmonization
Participants reported a better auditory experience while engaged in the mixed-music interventions compared to their exposures to the 40 Hz sound in isolation. They described how the coexistence of both 40 Hz sounds and music within these interventions produced a more tolerable auditory environment that more effectively balanced the perceived advantages and disadvantages of the music and 40 Hz sound interventions.
Compared to the static [40 Hz], [the 40 Hz mixed music was] much better, by all means.
(Male, 70 years old, second condition)
Last session I like the most… with the music and the light noise [40 Hz mixed music]
(Female, 77 years old, third condition).
Participants were able to identify the presence of 40 Hz sound frequencies within the mixed music intervention.
The thing that caught me off guard and you know like how sometimes you, I mean, you’d be hearing the humming, and you’d be expecting that a humming bother you or something? It don’t bother me because the volume of the humming, is that a perfect tone, perfect level of volume, when you can enjoy the music and still hear that that harmony, but it don’t mean nothing because the music overwhelms the humming. So, I like that.
(Female, 55 years old, first condition)
I actually enjoyed the selections that I made. And because it was such a variety of selections for me. So, I enjoyed it because it would always surprise me - I would hear a song and I was like, oh, I liked that song. Or oh, I remember that song. So, I actually really enjoyed the variety of my selections. And I absolutely never felt like the background noise was a distraction at all, because I enjoy hearing the songs.
(Female, 66 years old, first condition)
I could hear it if I concentrated on the buzzing. But it was I was more listening to the music. So, I was like singing and dancing to the music around the house…. I could definitely hear the buzzing, but it didn’t give me any issues.
(Female, 60 years old, third condition)
The humming sound didn’t bother me.
(Male, 59 years old, first condition)
It (40 Hz sounds) was there, but it didn’t bother me.
(Male, 70 years old, first condition)
Some participants were put off by the 40 Hz background sound, while others learned to accommodate it. The familiarity with the chosen music played a crucial role in participants’ tolerance of the 40 Hz sound.
Oh, the sound? The sound, I don’t think I liked that one too much. Yeah, I kind of just sit there and close my eyes [inaudible 1:10]. Try to take it and put it out of my head.
(Male, 66 years old, third condition)
But now when I was listening to the noise with the music now that wasn’t as good as listening to just the music because you hear this sound in the background of the music.
(Female, 65 years old, second condition)
If it’s a song that I know I could get through it with the buzzing sound because I’m singing along, right, “Oh I really know this one,” so that buzzing doesn’t bother me because I know that song and that buzzing is not a part of the song, so I can get through it, it don’t bother me. But if really don’t know the song and if I focus on the buzzing it gives you a headache or it makes your anxiety like, “Please stop the buzzing.” And you want to take it off, but you know you can’t because I’m doing the study so I don’t take it off. Yeah, other than that you have to really focus. If I sing along out loud it doesn’t bother me, but if I’m quiet and just listen to the song it gets a little overwhelming…But most of the ones that was put on I enjoyed it along with the humming, I enjoyed it because I was familiar with all the artists.
(Female, 66 years old, first condition)
Feasibility
Psychosocial Motivation and Self-Efficacy
Participants shared various psychosocial factors that influenced their engagement with the auditory interventions. For the self-selected music, a prior interest in song listening (i.e., leisure listening, past song enjoyment, worship songs) played a role in their acceptance and enjoyment of the intervention.
I enjoyed sitting there and that hour went by really quick. […] I like music, yeah, I’m a music person. Music gets me moving I want to say. When I get in the shower, I have to have the music on, it gets me moving, it gets me up out of the bed, it gets me moving, get my heart racing. You hear these sounds and you just-- it makes me feel good about myself, to tell the truth.
(Female, 65 years old, third condition)
Listen to the music motivates you, calms you, it innovates you to do things you know.
(Male, 70 years old, second condition)
Oh, I love it. I love it. I pick different songs. I like basically I like the old school music. Sometimes it’s gospel. Sometimes, you know, I’ll try something different.
(Female, 67 years old, second condition)
In contrast, for the 40 Hz sound, concerns about cognitive aging and memory loss motivated participants to persist with the prescribed sound or the intervention. The participants below described their motivations to persist within the intervention, during 40 Hz sound or 40 Hz music interviews.
Because my memory is getting bad, and I’m not that old, and I was getting concerned, and I feel as though research is a very important part of science for us to find cures for things and solutions to problems. So, I am very happy to participate when I can.
(Female, 60 years old, third condition)
Overall, unrelated to this, my memory, I think is actually getting worse considering my age, it’s getting worse compared to how young I consider myself to be.
(Female, 66 years old, first condition)
As far as memory, man, I - my recall is getting lousy, but I’m working on it. So, you know, I, I’m hoping the music helps.
(Female, 77 years old, second condition)
Spontaneity and Autonomy
Across all listening formats, participants varied in the timing and location in which they engaged in the intervention. Participants had flexibility in deciding when (e.g., time – morning to night), where (e.g., home – bedroom, kitchen, living room), and what they could listen to in their self-selected music playlists. These options allowed for personalization. For instance, morning listeners tended to describe boosts of energy and productivity, while late-night listeners described moods of relaxation and sleep. Music genre played an important role that allowed participants to tailor their experience, opting for upbeat and faster-paced tracks in the morning, and slower, calming songs for evenings.
I love music, so if it’s upbeat I don’t know I’m kind of, I would say give you more energy like you want to do more. And then the other type of music, the classical music kind of mellows you out kind of like relaxing you.
(Female, 66 years old, third condition)
At night after- after nine o’clock [when the participant would listen to the auditory intervention]? […] Ah, I was very- I’m very relaxed. I’m finished with everything, with my routine.
(Female, 66 years old, first condition)
Music genre played an important role which allowed participants to tailor their experience, opting for upbeat and faster-paced tracks in the morning, and slower, calming songs for evenings. Participants chose a diverse range of music spanning various genres, including pop, blues, metal, hip hop, jazz, country, soul, gospel, among others. While this autonomy and spontaneity offered a personalized experience, it also introduced the risk of procrastination and delays, potentially hindering the development of a consistent listening habit. This could impact adherence and overall acclimation to the intervention. Particularly within the 40 Hz sound groups, participants who found the prescribed sound unpleasant tended to progressively postpone their listening sessions to later in the day.
If I didn’t remember to 11 o’clock at night to listen to it. I had to hurry up and do it before it changed to the next day.
(Female, 77 years old, third condition)
Social Support
Participants leaned on family and friends for support and motivation throughout the intervention process. These individuals played a vital role in assessing the benefits of the interventions, assisting with memory-related tasks, and monitoring any deviations from usual memory patterns.
I just know that I’m still forgetting as much as before… maybe even more than before. According to my friends I’m repeating things which, they’re used to, and we joke about it.
(Female, 71 years old, second condition)
My friend who’s a nurse, she’s like, “You really need to see somebody about your memory,” and I don’t know if it’s a memory issue, or if it’s a concentration issue, or a focus issue.
(Female, 60 years old, third condition)
You know, but how it affects me cognitively, I’ll do anything to improve my cognition. So, you know, whatever it does, or doesn’t do, you know, I have groups of friends, and we’re always talking about this. You know, how to improve this, one does Sudoku, you know, this one does in it, whatever it is.
(Female, 77 years old, second condition)
Troubleshooting
Family and friends often acted as the primary source of technical support, encouraging participation in the intervention, and aiding in the resolution of minor technical issues.
All of the songs that I listened to were songs that were probably when I was younger. So, I thought oh, yeah, I was- I was in junior high school. Oh, I was 20. And those things like that. Made me think of people that knew back then, where I was back then. So much so that my daughter’s now she’s playing the station for me – say mommy like that old music.
(Female, 68 years old, first condition)
It was challenging [in reference to the first time using the tablet to select music], because I didn’t want to do it, because I’m not used to doing it. I usually ask my son or my daughter or a grandson to do it for me like that.
(Female, 66 years old, third condition)
Study team involvement in minor to larger technical problems and check-ins were important in facilitating these interventions in people with MCI, while also providing a degree of social contact or interaction for more isolated participants. In early feedback, participants emphasized the importance of portability for the tablet-listening experience. Many described wanting to do small tasks around the house, or walk outdoors. However, the cord from the headphones and bulkiness of the tablet often got in the way. As we progressed through the intervention, study team members made individual solutions for participants such as carrying straps for the tablet and wireless headphones if needed.
The device was okay, it’s just kind of like bulky. If it was smaller […] Where if I could carry it around with me around the house like doing the laundry and the dishes and all that, I could be doing other things while listening to the music, yeah.
(Female, 66 years old, third condition)
Well, the only dislike and I heard that you’re all working on this won’t affect me. The only dislike is, I would be in my kitchen. And I’ll being doing it, and the cord from the headphones would always get stuck on one of the kitchen knobs, or if I did other things that caught on things, so you know. I don’t know if they want you to be stationary while listening to it.
(Female, 77 years old, second condition)
No. This is better [referring to cord solution], because I could hang it around my neck and walk around. Yeah, this is better for me, because if I have a tablet I’m just gonna be sitting here, and this I can walk and eat my breakfast, empty the trash, wash the dishes, do good stuff that doesn’t require brain power.
(Female, 60 years old, second condition)
An offline tablet app was discussed among the study team to provide ease of sound-music listening and tracking, especially for homes without broadband connection or when taken outside. Even among our small sample of interviews, there were differing levels of familiarity with technology resulting in diverse technological needs. Having a variety of supports in place—such as text messages, home visit device setups, device tutorials, and calls—played a critical role in participant comfort and ease of intervention adherence.
Because so far. I mean, like you communicate with me well, you check on me. It makes sure if I have any problems, you can correct it. You sent me texts. So, I mean, like, you keep the communication line open. So, if there was a problem, I wouldn’t be panicking. Like, what do I do? How do I have to wait and things like that? So I mean, like, I don’t know, I guess my personal opinion be so far you doing okay.
(Female, 55 years old, first condition)
I think they were very nice. It’s sort of like, you know, especially being new in my neighborhood. I don’t, I’m not the type to visit my neighbors. And because I’m working. When I say working I mean I’m doing my artwork, or packing or unpacking or whatever, I don’t visit other people. But you know, when you, when you guys came, I could still do it. I could move and talk at the same time. You know, which I tend to do. And it was just good having somebody coming to visit me, you know? I don’t go out much. You know, other than the two nights that I still work a week, two nights a week.
(Female, 71 years old, third condition)
Discussion
We studied the acceptance and listening experience of three auditory interventions in individuals with MCI, including self-selected music, 40 Hz sound, and a combination of the two—40 Hz music. The findings revealed varied experience and acceptance, with self-selected music acting as a memory preserver and emotional support, 40 Hz sound producing more adverse reactions, and 40 Hz music offering a more harmonized and bridged experience between the two modalities. The findings suggest that integrating self-selected music with 40 Hz sound enhanced the overall listening experience, when compared to 40Hz alone.
These findings have important implications for the development and implementation of auditory interventions in individuals with MCI. Self-selected music was more favored among the participants. The deeply personal and emotional connection participants felt towards their selected songs underscored its therapeutic importance for emotional challenges and memory preservation37–42. The unique ability of music to tap into poignant life memories aligns with previous research on the positive impact of music on cognitive and emotional well-being in individuals with MCI34,35. This strong emotional engagement resonated with the participants, reinforcing the importance of personalization and emotional resonance in designing effective auditory interventions for this population.
In contrast, approximately half of the participants expressed negative responses to the 40 Hz sound, citing discomfort, irritation, and even torment. Some participants reported varied durations of lingering sounds after one-hour of 40 Hz sound exposure. This aversion could be attributed to individual sensitivity to sound or an inherent dislike of the specific 40 Hz frequency, which has been found in other studies27,28,43. Also, some of the participants who initially disliked the sound found ways to adapt and even derive relaxation from it. It highlights that, despite their initial resistance, some participants may adapt, albeit sometimes at the expense of certain intervention deviations, such as falling asleep, tuning out the sound entirely, or engaging in tasks that divert their focus. Future studies may consider a shorter duration of daily exposure and closely monitor potential side effects of 40 Hz sound exposure.
The introduction of 40 Hz music, combining the 40 Hz sound with self-selected music, provided a unique insight into the interplay between music and the 40 Hz sound. Improving the balance between the 40 Hz sound and music was crucial, as early feedback indicated issues with volume levels. By refining our volume envelope technique, we found that it was also crucial to ensure that the 40 Hz sound was audible but well integrated with the music. Overall, participants reported a more positive auditory experience when exposed to mixed-music interventions compared to 40 Hz sound alone. However, some participants found the 40 Hz sound in the background to still be perturbing. Individual preferences and familiarity with the music played a crucial role in shaping the overall experience, which may shape future research directions.
Distinct motivators were evident across the three conditions. It became apparent that pre-existing enjoyment of music played a pervasive role in influencing the acceptance and enjoyment of self-selected music. In contrast, concerns related to cognitive aging and memory loss emerged as the primary drivers for adherence to the intervention during the 40 Hz sound condition. Flexibility in timing and location allowed personalized experiences, bolstering acceptability but also presenting a risk of procrastination. Participants also benefited from robust support from friends, family, and our team, serving as accountability partners, motivating adherence, and addressing technical issues, thus ensuring comfort and adherence beyond academic confines. Notably, the longitudinal nature of the study spanning a period of 5 months, presented a few challenges. The daily nature of listening, coupled with more substantial study requirements, occasionally led to some variations of intervention application. For example, in terms of listening strategies, there were some ambiguities regarding recommended activities during the intervention, which led to activity choices not in line with the study protocol, potentially affecting participant engagement and impacting the experience and cognitive effects of 40 Hz. However, striking the right balance between relevance and internal validity remains crucial for the future stages of this research. This equilibrium is essential to ensure that participant preferences, flexibility, and the study’s long-term applicability are maintained, all while upholding the required methodological rigor and effectiveness44,45. Evaluating this balance will draw, in part, from the insights provided by participants in this qualitative study and subsequently through quantitative research examining both intended and unintended effects.
And although initial instructions were clearly understood, participants with MCI may have forgotten some of the study requirements as time progressed through the intervention. There were instances of confusion regarding the compensation amounts, as well as feedback that the entire intervention, including post-tests and baselines, was excessively time-consuming relative to the compensation provided. This could potentially impact their perception and willingness to complete the full study, particularly if they found it to be overly time-consuming46. Another limitation of the study lies in the ongoing nature of our parent study. While this qualitative study was intended to be nested in a prospective randomized controlled crossover trial, not all participants in the parent study had undergone all three conditions at the time of this qualitative analysis. With this in mind, it may have potentially introduced some degree of bias and variability.
Despite these limitations, to our knowledge, our study is the first to investigate how participants respond to 40 Hz auditory interventions. Furthermore, by focusing on a sample with mainly low-income individuals, our research highlights the accessibility and affordability of such auditory interventions. With 68% of the sample being Black, it is essential to consider race-based factors in existing and future studies. The high prevalence of Alzheimer’s disease among Black Americans, who are twice as likely to develop dementia and commonly have personal connections to those affected, highlights the need for focused dementia care in these communities5. The cultural importance of music in Black culture may also influence the effectiveness of interventions integrating music therapy49,50. For instance, among some of the Black participants, their religion (e.g., gospel music/choir) or upbringing surrounding music in childhood and young adulthood (e.g., radio music in car) potentially played a critical role in their existing listening adherence. Considering these sociodemographic impacts will be critical in the tailoring of future programs, particularly given the lack of racial diversity in clinical trials and program interventions47, 48. These findings, among others identified in the study, will help to ensure that dementia care strategies are more practical and culturally appropriate to higher risk Black populations.
The quantitative phase of the parent study, which aims to evaluate the preliminary efficacy of the three auditory interventions, is currently underway. The insights gained from this qualitative exploration, along with the results from the ongoing quantitative research, will collectively contribute to the development of future 40 Hz auditory interventions for individuals with MCI.
Conclusion
Given the diverse reactions to the three auditory interventions, factors such as a strong emotional connection to music, the personalization of the experience, and established listening habits significantly influenced the acceptability and engagement with the 40 Hz music intervention. These elements of acceptability and listening enjoyment are crucial considerations that have been absent in prior 40 Hz interventions. Although both transgenic mouse models and initial short-term human trials have shown some efficacy, these interventions will not be as impactful if they are not feasible or acceptable for long-term use among individuals with MCI and AD. Clinical trials often fail to capture the subjective preferences of participants, which are critical for the real-world success of any intervention. The first-hand insights into acceptability obtained from this study are crucial for ensuring that these interventions are not only effective but also practically applicable within a diverse community.
Figure 6:
Thematic Analysis Findings
Highlights.
Targeted interventions in people with mild cognitive impairment are crucial to preventing progression towards dementia or Alzheimer’s disease.
40 Hz auditory stimulation may be a promising treatment modality cognition in people with early stage of Alzheimer’s disease.
Merging 40 Hz sound with self-selected music may improve usability and practical enjoyment among older adults with mild cognitive impairment.
Acknowledgements
As the team leading this study, we recognize the importance of reflexivity and positionality in our research process. Our primary coders, CW and ML, as early-career researchers, bring a unique and evolving perspective to this work. Their youth and position at the onset of their research careers provide fresh insights. Nonetheless, we acknowledge the generational divide between ourselves and our older adult subjects. Through ongoing self-reflection, learning, and consultation with study participants, we aim to address our implicit biases, ensuring our research reflects the diverse realities of aging with cultural humility. This approach, grounded in the ethos of diversity and inclusion, guides our interactions within the academic and research community, shaping our contributions to this field of geriatric nursing.
Funding
This work was supported by the National Institute on Aging (Grant R21 AG078917), the Johns Hopkins Center for Equity in Aging Pilot Fund, and the Johns Hopkins School of Nursing Discovery and Innovation Award.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- 1.Vespa J The U.S. Joins Other Countries With Large Aging Populations.; 2018. Accessed May 2, 2023. https://www.census.gov/library/stories/2018/03/graying-america.html
- 2.Padeiro M, Santana P, Grant M. Chapter 1 - Global aging and health determinants in a changing world. In: Oliveira PJ, Malva JO, eds. Aging. Academic Press; 2023:3–30. doi: 10.1016/B978-0-12-823761-8.00021-5 [DOI] [Google Scholar]
- 3.Kim JG, Kim H, Hwang J, et al. Differentiating amnestic from non-amnestic mild cognitive impairment subtypes using graph theoretical measures of electroencephalography. Sci Rep. 2022;12(1):6219. doi: 10.1038/s41598-022-10322-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: Mild cognitive impairment. eurology. 2018;90(3):126–135. doi: 10.1212/WNL.0000000000004826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alzheimer’s Association. 2023 Alzheimer’s disease facts and figures. Alzheimers Dement. 2023;19(4):1598–1695. doi: 10.1002/alz.13016 [DOI] [PubMed] [Google Scholar]
- 6.Shimada H, Doi T, Lee S, Makizako H. Reversible predictors of reversion from mild cognitive impairment to normal cognition: a 4-year longitudinal study. Alzheimer’s Research & Therapy. 2019;11(1):24. doi: 10.1186/s13195-019-0480-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davis M, O Connell T, Johnson S, et al. Estimating Alzheimer’s Disease Progression Rates from Normal Cognition Through Mild Cognitive Impairment and Stages of Dementia. Curr Alzheimer Res. 2018;15(8):777–788. doi: 10.2174/156720501566618011909242710.2174/1567205015666180119092427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thaipisuttikul P, Jaikla K, Satthong S, Wisajun P. Rate of conversion from mild cognitive impairment to dementia in a Thai hospital-based population: A retrospective cohort. Alzheimer’s & Dementia: Translational Research & Clinical Interventions. 2022;8(1):e12272. doi: 10.1002/trc2.12272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Traikapi A, Konstantinou N. Gamma Oscillations in Alzheimer’s Disease and Their Potential Therapeutic Role. Front Syst Neurosci. 2021;15:782399. doi: 10.3389/fnsys.2021.782399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mably AJ, Colgin LL. Gamma oscillations in cognitive disorders. Curr Opin Neurobiol. 2018;52:182–187. doi: 10.1016/j.conb.2018.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Goutagny R, Gu N, Cavanagh C, et al. Alterations in hippocampal network oscillations and theta-gamma coupling arise before Aβ overproduction in a mouse model of Alzheimer’s disease. Eur J Neurosci. 2013;37(12):1896–1902. doi: 10.1111/ejn.12233 [DOI] [PubMed] [Google Scholar]
- 12.Guillon J, Attal Y, Colliot O, et al. Loss of brain inter-frequency hubs in Alzheimer’s disease. Sci Rep. 2017;7(1):10879. doi: 10.1038/s41598-017-07846-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Koenig T, Prichep L, Dierks T, et al. Decreased EEG synchronization in Alzheimer’s disease and mild cognitive impairment. Neurobiol Aging. 2005;26(2):165–171. doi: 10.1016/j.neurobiolaging.2004.03.008 [DOI] [PubMed] [Google Scholar]
- 14.Mehak SF, Shivakumar AB, Kumari S, Muralidharan B, Gangadharan G. Theta and gamma oscillatory dynamics in mouse models of Alzheimer’s disease: A path to prospective therapeutic intervention. Neuroscience & Biobehavioral Reviews. 2022;136:104628. doi: 10.1016/j.neubiorev.2022.104628 [DOI] [PubMed] [Google Scholar]
- 15.Iaccarino HF, Singer AC, Martorell AJ, et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature. 2016;540(7632):230–235. doi: 10.1038/nature20587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Martorell AJ, Paulson AL, Suk HJ, et al. Multi-sensory Gamma Stimulation Ameliorates Alzheimer’s-Associated Pathology and Improves Cognition. Cell. 2019;177(2):256–271.e22. doi: 10.1016/j.cell.2019.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu C, Han T, Xu Z, et al. Modulating Gamma Oscillations Promotes Brain Connectivity to Improve Cognitive Impairment. Cereb Cortex. 2022;32(12):2644–2656. doi: 10.1093/cercor/bhab371 [DOI] [PubMed] [Google Scholar]
- 18.Clements-Cortes A, Ahonen H, Evans M, Freedman M, Bartel L. Short-Term Effects of Rhythmic Sensory Stimulation in Alzheimer’s Disease: An Exploratory Pilot Study. J Alzheimers Dis. 2016;52(2):651–660. doi: 10.3233/JAD-160081 [DOI] [PubMed] [Google Scholar]
- 19.Cimenser A, Hempel E, Travers T, et al. Sensory-Evoked 40-Hz Gamma Oscillation Improves Sleep and Daily Living Activities in Alzheimer’s Disease Patients. Front Syst Neurosci. 2021;15:746859. doi: 10.3389/fnsys.2021.746859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chan D, Suk HJ, Jackson BL, et al. Gamma frequency sensory stimulation in mild probable Alzheimer’s dementia patients: Results of feasibility and pilot studies. PLOS ONE. 2022;17(12):e0278412. doi: 10.1371/journal.pone.0278412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Manippa V, Palmisano A, Filardi M, et al. An update on the use of gamma (multi)sensory stimulation for Alzheimer’s disease treatment. Front Aging Neurosci. 2022;14:1095081. doi: 10.3389/fnagi.2022.1095081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.He Q, Colon-Motas KM, Pybus AF, et al. A feasibility trial of gamma sensory flicker for patients with prodromal Alzheimer’s disease. Alzheimers Dement (N Y). 2021;7(1):e12178. doi: 10.1002/trc2.12178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moretti DV, Frisoni GB, Fracassi C, et al. MCI patients’ EEGs show group differences between those who progress and those who do not progress to AD. Neurobiol Aging. 2011;32(4):563–571. doi: 10.1016/j.neurobiolaging.2009.04.003 [DOI] [PubMed] [Google Scholar]
- 24.Musaeus CS, Nielsen MS, Musaeus JS, Høgh P. Electroencephalographic Cross-Frequency Coupling as a Sign of Disease Progression in Patients With Mild Cognitive Impairment: A Pilot Study. Front Neurosci. 2020;14:790. doi: 10.3389/fnins.2020.00790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hermes D, Kasteleijn-Nolst Trenité DGA, Winawer J. Gamma oscillations and photosensitive epilepsy. Curr Biol. 2017;27(9):R336–R338. doi: 10.1016/j.cub.2017.03.076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Han C, Zhao X, Li M, et al. Enhancement of the neural response during 40 Hz auditory entrainment in closed-eye state in human prefrontal region. Cogn Neurodyn. 2023;17(2):399–410. doi: 10.1007/s11571-022-09834-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Olem D, Sharp KM, Johnson MO. Challenges with engaging participants in behavioral intervention research trials. OAJCT. 2009;1(Default):17–21. doi: 10.2147/OAJCT.S6841 [DOI] [Google Scholar]
- 28.Weinheimer EA, Chang A, Neubert SW, Wildes JE, Graham AK. Past, current, and future willingness to engage with treatment targets: Applying user-centered design to inform the design of a mobile behavioral intervention. Int J Eat Disord. 2020;53(4):611–617. doi: 10.1002/eat.23252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Greer T, Ma B, Sachs M, Habibi A, Narayanan S. A Multimodal View into Music’s Effect on Human Neural, Physiological, and Emotional Experience. In: Proceedings of the 27th ACM International Conference on Multimedia. ACM; 2019:167–175. doi: 10.1145/3343031.335086710.1145/3343031.3350867 [DOI] [Google Scholar]
- 30.Ito E, Nouchi R, Dinet J, Cheng CH, Husebø BS. The Effect of Music-Based Intervention on General Cognitive and Executive Functions, and Episodic Memory in People with Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials. Healthcare. 2022;10(8):1462. doi: 10.3390/healthcare10081462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lam HL, Li WTV, Laher I, Wong RY. Effects of Music Therapy on Patients with Dementia—A Systematic Review. Geriatrics (Basel). 2020;5(4):62. doi: 10.3390/geriatrics5040062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Baird A, Brancatisano O, Gelding R, Thompson WF. Music evoked autobiographical memories in people with behavioural variant frontotemporal dementia. Memory. 2020;28(3):323–336. doi: 10.1080/09658211.2020.171337910.1080/09658211.2020.1713379 [DOI] [PubMed] [Google Scholar]
- 33.Gassner L, Geretsegger M, Mayer-Ferbas J. Effectiveness of music therapy for autism spectrum disorder, dementia, depression, insomnia and schizophrenia: update of systematic reviews. Eur J Public Health. 2021;32(1):27–34. doi: 10.1093/eurpub/ckab042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Xue B, Meng X, Liu Q, Luo X. The effect of receptive music therapy on older adults with mild cognitive impairment and depression: a randomized controlled trial. Sci Rep. 2023;13(1):22159. doi: 10.1038/s41598-023-49162-610.1038/s41598-023-49162-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.El Haj M, Postal V, Allain P. Music Enhances Autobiographical Memory in Mild Alzheimer’s Disease. Educational Gerontology. 2012;38(1):30–41. doi: 10.1080/03601277.2010.515897 [DOI] [Google Scholar]
- 36.Thompson J A Guide to Abductive Thematic Analysis. The Qualitative Report. 2022;27(5):1410–1421. doi: 10.46743/2160-3715/2022.5340 [DOI] [Google Scholar]
- 37.Bleibel M, El Cheikh A, Sadier NS, Abou-Abbas L. The effect of music therapy on cognitive functions in patients with Alzheimer’s disease: a systematic review of randomized controlled trials. Alzheimer’s Research & Therapy. 2023;15(1):65. doi: 10.1186/s13195-023-01214-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Innes KE, Selfe TK, Khalsa DS, Kandati S. Effects of Meditation versus Music Listening on Perceived Stress, Mood, Sleep, and Quality of Life in Adults with Early Memory Loss: A Pilot Randomized Controlled Trial. J Alzheimers Dis. 2016;52(4):1277–1298. doi: 10.3233/JAD-151106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kaiser AP, Berntsen D. The cognitive characteristics of music-evoked autobiographical memories: Evidence from a systematic review of clinical investigations. WIREs Cognitive Science. 2023;14(3):No Pagination Specified-No Pagination Specified. doi: 10.1002/wcs.1627 [DOI] [PubMed] [Google Scholar]
- 40.Moreno-Morales C, Calero R, Moreno-Morales P, Pintado C. Music Therapy in the Treatment of Dementia: A Systematic Review and Meta-Analysis. Front Med (Lausanne). 2020;7:160. doi: 10.3389/fmed.2020.00160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Matziorinis AM, Koelsch S. The promise of music therapy for Alzheimer’s disease: A review. Ann N Y Acad Sci. 2022;1516(1):11–17. doi: 10.1111/nyas.14864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ting B, Chen DTL, Hsu WT, et al. Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Clin Med. 2023;12(17):5497. doi: 10.3390/jcm12175497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tichko P, Kim JC, Large E, Loui P. Integrating music-based interventions with Gamma-frequency stimulation: Implications for healthy ageing. Eur J Neurosci. 2022;55(11–12):3303–3323. doi: 10.1111/ejn.15059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Blazar D, Kraft MA. Balancing Rigor, Replication, and Relevance: A Case for Multiple-Cohort, Longitudinal Experiments. AERA Open. 2019;5(3):2332858419876252. doi: 10.1177/2332858419876252 [DOI] [Google Scholar]
- 45.Geng EH, Peiris D, Kruk ME. Implementation science: Relevance in the real world without sacrificing rigor. PLOS Medicine. 2017;14(4):e1002288. doi: 10.1371/journal.pmed.1002288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Pandya M, Desai C. Compensation in clinical research: The debate continues. Perspect Clin Res. 2013;4(1):70–74. doi: 10.4103/2229-3485.106394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Reardon S Alzheimer’s drug trials plagued by lack of racial diversity. Nature. 2023;620(7973):256–257. doi: 10.1038/d41586-023-02464-1 [DOI] [PubMed] [Google Scholar]
- 48.Babulal GM, Quiroz YT, Albensi BC, et al. Perspectives on Ethnic and Racial Disparities in Alzheimer’s Disease and Related Dementias: Update and Areas of Immediate Need. Alzheimers Dement. 2019;15(2):292–312. doi: 10.1016/j.jalz.2018.09.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Rosselli M, Uribe IV, Ahne E, Shihadeh L. Culture, Ethnicity, and Level of Education in Alzheimer’s Disease. Neurotherapeutics. 2022;19(1):26–54. doi: 10.1007/s13311-022-01193-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Rosselli M, Ardila A. The impact of culture and education on non-verbal neuropsychological measurements: a critical review. Brain Cogn. 2003;52(3):326–333. doi: 10.1016/s0278-2626(03)00170-2 [DOI] [PubMed] [Google Scholar]