

Dear Editor,
Supine, left head rotation (LeHeR) manoeuvres have been reported to improve glottic view during direct laryngoscopy using Macintosh laryngoscope.[1]
A 35-year-old male (weight 70 kg, body mass index 25.71 kg/m2, American Society of Anesthesiologists physical status II) with a history of hemi-mandibulectomy 1 year back was posted for segmental maxillectomy with reconstruction. He had a 4 cm mouth opening with restricted tongue protrusion, normal neck extension and 6 cm thyromental distance with an El-Ganzouri score of 2. General anaesthesia with C-MAC video laryngoscope-assisted nasotracheal intubation was planned. The right nostril was decongested with two drops of oxymetazoline and lubricated with a dollop of 2% lidocaine jelly. The patient was premedicated with intravenous glycopyrrolate 0.2 mg, fentanyl 120 μg and midazolam 1 mg. Anaesthesia was induced with intravenous 120 mg propofol and, after ensuring mask ventilation, the patient received suxamethonium 100 mg. Indirect laryngoscopy with C-MAC (Karl Storz SE and Co.KG, Tuttlingen, Germany) D blade revealed only epiglottis, with a percentage of glottic opening (POGO) score 0 [Figure 1a]. The glottic view remained unchanged despite increasing the lifting force on the videoscope blade or external neck manipulations. The laryngoscope blade was removed, and the LeHeR manoeuvre was performed by turning the patient’s head 45° to the left side. Repeat laryngoscopy showed a POGO score of 50% [Figure 1b]. A 7.0-mm, cuffed, nasal Ring–Adair–Elwyn tube was introduced through the right nostril and advanced to the oropharynx. The trachea was intubated with the head kept in the same position following a slight medial rotation of the tube. Regular end-tidal carbon dioxide waveforms and chest auscultation confirmed correct tracheal placement. Oxygen saturation in the pulse oximeter remained 99%–100% during intubation.
Figure 1:
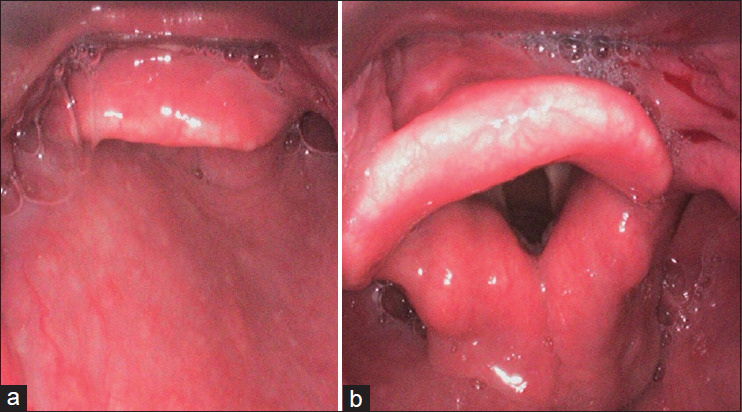
Glottic view (a) supine position, (b) after LeHeR manoeuvre. LeHeR = left head rotation
The LeHeR manoeuvre has proven successful after more than a single attempt at tracheal intubation. It usually improves the laryngoscopic view of Cormack–Lehane grades from 3 and 4 to 1 and 2, respectively.[1] It is postulated that during the LeHeR manoeuvre, the airway space increases and improves glottis visualisation mainly due to gravitational force. In addition, neck rotation increases the muscle tension and lifts the glottis. Ultrasonographic assessment during LeHeR showed that the cricoid cartilage compresses the oesophagus and moves anteriorly, improving the glottis view.
Magnetic resonance imaging studies have shown that in the supine position, the soft palate compromised the anterior portion of the retropalatal airway and there was a downward movement of the upper airway.[2] However, in patients in a supine position with head rotation, the cross-sectional area of the upper airway increases in the upper and lower retroglossal regions, moving the airway upwards. These results suggest that the beneficial effects of head rotation could be due to a marked increase in the upper airway diameter with an increase in the cross-sectional area in the retroglossal region.[2,3] LeHeR position can be shown to improve the oropharyngeal curve by shortening it, as explained by the two-curve theory by Greenland.[4] However, a recent study concluded that LeHeR did not improve laryngeal view during direct laryngoscopy.[5] However, its usefulness during video laryngoscopy is still unexplored and more robust evidence is needed to prove its usefulness in difficult intubations.
We conclude that during difficult video laryngoscopy, a simple technique like the LeHeR manoeuvre could be attempted, possibly improving the glottic view and leading to successful intubation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient consented to his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Yezid NH, Poh K, Md Noor J, Arshad A. LeHeR, a simple novel approach for difficult airway in non-trauma patients. BMJ Case Rep. 2019;12:e230201. doi: 10.1136/bcr-2019-230201. doi: 10.1136/bcr-2019-230201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ono T, Otsuka R, Kuroda T, Honda E, Sasaki T. Effects of head and body position on two- and three-dimensional configurations of the upper airway. J Dent Res. 2000;79:1879–84. doi: 10.1177/00220345000790111101. [DOI] [PubMed] [Google Scholar]
- 3.Itagaki T, Oto J, Burns SM, Jiang Y, Kacmarek RM, Mountjoy JR. The effect of head rotation on the efficiency of face mask ventilation in anaesthetized apnoeic adults: A randomised, crossover study. Euro J Anaesthesiol. 2017;34:432–40. doi: 10.1097/EJA.0000000000000582. [DOI] [PubMed] [Google Scholar]
- 4.Greenland K. The ramped position and its relationship to the 2-curve theory. Anesth Analg. 2011;113:1524–5. doi: 10.1213/ANE.0b013e318234a372. [DOI] [PubMed] [Google Scholar]
- 5.Chan DP, Jularbal Iii GCRM, Mapili IJR. Left head rotation as an alternative to difficult tracheal intubation: Randomized open label clinical trial. Interact J Med Res. 2023;12:e42500. doi: 10.2196/42500. doi: 10.2196/42500. [DOI] [PMC free article] [PubMed] [Google Scholar]