

Abstract
Background.
Personal exposure to fine particulate matter (PM2.5) from household air pollution is well-documented in sub-Saharan Africa, but spatiotemporal patterns of exposure are poorly characterized.
Objective.
We used paired GPS and personal PM2.5 data to evaluate changes in exposure across location-time environments (e.g., household and community, during cooking and non-cooking hours), building density and proximity to roadways.
Methods.
Our study included 259 sessions of geolocated, gravimetrically-calibrated one-minute personal PM2.5 measurements from participants in the GRAPHS Child Lung Function Study. The household vicinity was defined using a 50-meter buffer around participants’ homes. Community boundaries were developed using a spatial clustering algorithm applied to an open-source dataset of building footprints in Africa. For each GPS location, we estimated building density (500m buffer) and proximity to roadways (100m buffer). We estimated changes in PM2.5 exposure by location (household, community), time of day (morning/evening cooking hours, night), building density, and proximity to roadways using linear mixed effect models.
Results.
Relative to nighttime household exposure, PM2.5 exposure during evening cooking hours was 2.84 (95%CI=2.70–2.98) and 1.80 (95%CI=1.54–2.10) times higher in the household and community, respectively. Exposures were elevated in areas with the highest versus lowest quartile of building density (FactorQ1vsQ4=1.60, 95%CI=1.42–1.80). The effect of building density was strongest during evening cooking hours, and influenced levels in both the household and community (31% and 65% relative increase from Q1 to Q4, respectively). Being proximal to a trunk, tertiary or track roadway increased exposure by a factor of 1.16 (95%CI=1.07–1.25), 1.68 (95%CI=1.45–1.95) and 1.27 (95%CI=1.06–1.53), respectively.
Significance.
Our findings suggest that community-wide solid fuel use for household cooking contributes to personal PM2.5 exposure. Building density may exacerbate community exposures when multiple households are cooking simultaneously. Proximity to large roadways (trunk) and unpaved roadways (tertiary, track) increase PM2.5 exposure.
Keywords: Geospatial Analyses, Particulate Matter, Personal Exposure, Child Exposure/Health, Vulnerable Populations, Sustainable Development
INTRODUCTION
The combustion of solid fuels for domestic cooking is the primary source of household air pollution in low-and-middle income countries (LMICs). Sub-Saharan Africa continues to suffer the highest rate of age-adjusted disease due to household air pollution1. Among environmental risk factors, household air pollution is the second largest contributor to the global burden of disease, while ambient air pollution is the top contributor2. In regions like Africa where over 80% of the population relies on solid fuels, household air pollution may contribute significantly to ambient air pollution3.
Few studies have evaluated the relationship between levels of air pollution in the household and the community in LMICs. A modeling analysis conducted in Ghana as part of the Climate Pollutant Action Plan reported an estimated 64% of anthropogenic emissions of fine particulate matter (PM2.5; ≤2.5 μg/m3 aerodynamic diameter) were attributed to residential emissions3. A monitoring campaign in Nepal found PM2.5 levels were 37% higher in rural sites during times of cooking relative to a background site4. A study in rural China reported ambient levels of black carbon in villages were moderately correlated with levels in the household (r=0.49)5.
There is also a limited understanding of the influence of geographic features, e.g., building density and roadways, on air pollution in rural LMIC communities. A study in Bangladesh demonstrated that a household’s use of solid fuels for cooking increased PM2.5 and carbon monoxide levels outdoors, as well as in other neighboring homes that used cleaner fuels (i.e., gas, electric)6. Outdoor levels of air pollution may be elevated in areas with a high density of households that use solid fuels, especially during typical hours of cooking. Roadways, a well-recognized source of air pollution in urban, developed settings7–9, are gaining recognition as an important contributor to exposure in rural settings, in tandem with solid fuel use10–14. In rural China, a PM2.5 source apportionment analysis reported that outdoor sources, including vehicles, may contribute 10–20% of household exposures14. In rural Ghana, a greater proportion of PM2.5 was attributed to black carbon in personal samples relative to stationary samples in the kitchen, highlighting the need to further investigate roadways as an important exposure source13.
Community sources – including neighbors’ cooking – may partially explain why some improved cookstove trials have found less-than-expected reductions in personal PM2.5 exposure. In the Ghana Randomized Air Pollution and Health Study (GRAPHS), modest reductions in 48-hour PM2.5 exposure were observed among pregnant women who used an LPG cookstove (−35%; 95% confidence interval= −26, −38%) relative to those who used traditional cookstoves fueled by wood or charcoal15, 16. Despite using an LPG cookstove, 67% of these women experienced exposure levels that exceeded WHO interim guidelines (35μg/m3). These findings emphasize the need to identify sources beyond the household and evaluate patterns of exposure throughout the day. This has important implications for energy policy. If neighbors’ emissions contribute meaningfully to an individual’s exposure, then household-level clean energy interventions that only reach a portion of households in a community (as often is the case with commercial distribution that disproportionately reach richer households17) may underdeliver on health benefits.
Our study leveraged GPS-tracked personal PM2.5 measurements collected from mothers and children living in rural Ghana who are participants of the Child Lung Function Study, a cohort extension of GRAPHS. We aimed to compare exposure levels across location-time environments (e.g., household and community, during cooking and non-cooking hours), as well as by surrounding building density and proximity to roadways. Several previous studies from this cohort have demonstrated maternal exposure to PM2.5 is associated with higher blood pressure and impaired infant lung function and growth trajectories18–21. This study is the first to assess how personal exposure varies across location, time and sources outside of the household. Our findings will help to identify environmental conditions that increase air pollution exposure, which could lead to improved characterization of personal exposures in epidemiologic analyses22. This study also has implications in informing the design of policies aimed at reducing the burden of disease due to household and ambient air pollution.
METHODS
Study population
The Child Lung Function Study cohort includes non-smoking women and their children originally enrolled in GRAPHS, described elsewhere23. Briefly, a total of 1,414 pregnant women were recruited from 35 community clusters (2013–2016) in the now Bono East Region of Ghana. Following the randomized trial in which cleaner cookstoves were provided and used by participants for a duration of approximately two years24, mother-child dyads have continued to participate in several follow-up sessions that have collected personal measurements of air pollutants15, 25 and health outcomes including maternal blood pressure19, 20, child growth trajectories21 and lung function18, 26.
Our analysis includes GPS-tracked, one-minute personal measurements of PM2.5 collected from mothers and children, obtained during 48-hour logging sessions. These measurements were collected as part of a follow-up period conducted between August 2018 and July 2019, when the children in the cohort were approximately four years old. At the time of data collection, women had resumed using their traditional cookstoves. The protocol for this study was approved by the Kintampo Health Research Center Institutional Ethics Committee, Columbia University Medical Center and Mount Sinai. Women in the study provided written informed consent for the participation of themselves and their children. Analyses were conducted in R version 4.1.2. We interpreted the results using statistical measures, including a p-value threshold of <0.05 to discern statistical significance, and 95% confidence intervals to capture the range of potential values. For brevity, p-values less than 0.001 were abbreviated as ‘p-value<0.001’.
Personal exposure data
Participants wore an RTI MicroPEM V3.2 monitor (Research Triangle Park, NC) in a comfortable sling with the air inlet placed near the breathing zone. The monitor is equipped with a nephelometer for real-time PM2.5 readings, a Teflon filter for PM2.5 collection, and sensors for continuous recording of relative humidity and temperature. A built-in correction factor for relative humidity was applied to continuous nephelometer readings27. The methods and quality control procedures for obtaining one-minute PM2.5 estimates used in this study have been previously described15, 25. Briefly, this included the attachment of a HEPA filter to the device for at least five minutes before and after each monitoring session to assess for drifts in the readings. This facilitated a zero-drift correction applied to continuous readings. Monitoring sessions were deemed invalid if HEPA values exceeded 20μg/m3, or if the readings exhibited step-wise patterns or improbable plateaus. Gravimetric PM2.5 concentrations were obtained from the filters deployed in the field, and underwent field blank correction, involving the subtraction of a median field blank mass of 5μg, prior to concentration estimation. Gravimetric corrections were carried out by multiplying each reading by the ratio of the gravimetric PM2.5 concentration divided by the average of nephelometer PM2.5 readings for the total deployment time.
A randomly selected subset of participants consented to additionally wearing a Suunto Ambit 3 GPX tracker (Amer Sports Corporation, Vantaa, Finland) placed within the sling. The tracker recorded coordinate pairs (latitude/longitude at a precision of 6 decimal degrees) and corresponding timestamps when movement was detected. Therefore, GPS records were more frequent throughout the day (median/average=every 2/19 mins) relative to the night (median/average= every 26/95 mins), when participants were less active and removed the device before sleeping. Coordinates from the tracker were joined to PM2.5 measurements by matching timestamps. Since there was not a GPS record for each minute, we assumed participants remained in the same area until the next GPS record. We implemented this assumption by assigning the last observed coordinate pair to subsequent one-minute PM2.5 measurements until the next coordinate pair. The first coordinate pair linked to a PM2.5 measurement was carried upward and assigned to any preceding PM2.5 measurements at the beginning of the session.
Of the initial 595 GPX tracker sessions, 439 were linked to validated MicroPEM data15. We restricted to sessions in which the start time of both devices were within 2 hours (to account for set-up time) and with a total logging time of 12 or more hours after linkage (n=283). An additional 24 sessions were excluded after visual inspection of GPS trajectories revealed locations to be outside of study communities, often explained by the return of the devices to the research center in Kintampo after failed deployment, or study participants who were temporarily residing away from their home. Our final dataset included 259 sessions among 145 mothers and 114 children of GPS-tracked, one-minute PM2.5 measurements for a total of approximately 695k minutes.
Household boundaries
We estimated participants’ home coordinates using GPS data during the nighttime (21 to 4 the next day), assuming participants would be home during this time. We evaluated GPS coordinates after linkage to continuous one-minute PM2.5 data; therefore, infrequent coordinates, likely recorded when the wearer removed the GPS tracker at home before bed, served to approximate participants’ location for most of the night. We categorized nighttime coordinates into clusters with a 5m radius, and found similar results with a 10m radius28. The centroid of the densest cluster was used to estimate the participant’s home longitude and latitude. Among those who had available survey data that included field-logged GPS coordinates for participants’ homes, the median distance between estimated and field-logged home coordinates was 23 meters (IQR=14–139m).
Our next step was to define a boundary around the home coordinates to account for imprecision in coordinates (e.g., satellite interference from the walls of a home) as well as activities of daily life, such as cooking, which typically occur outside but in the vicinity of the home structure15. First, we computed the average distance between unique coordinates recorded at nighttime and the estimated home centroid of each participant. The IQR of average distances ranged from 16 to 24 meters. Second, we evaluated patterns of average PM2.5 exposure when moving away from the home during cooking hours (Figure S1). When the household boundary was smallest (25–30m), the distribution of community exposures was higher compared to larger household buffer sizes (40–100m). This suggested that when the buffer size around the home was too small, household cooking exposures were misclassified as community exposures. Such patterns of potential misclassification diminished at buffer sizes >40m. Informed by this distribution, we defined household boundaries using a 50m radius around the home. As depicted in Figure 1, exposures occurring within a 50m buffer around the home are classified as ‘household exposures’.
Figure 1.
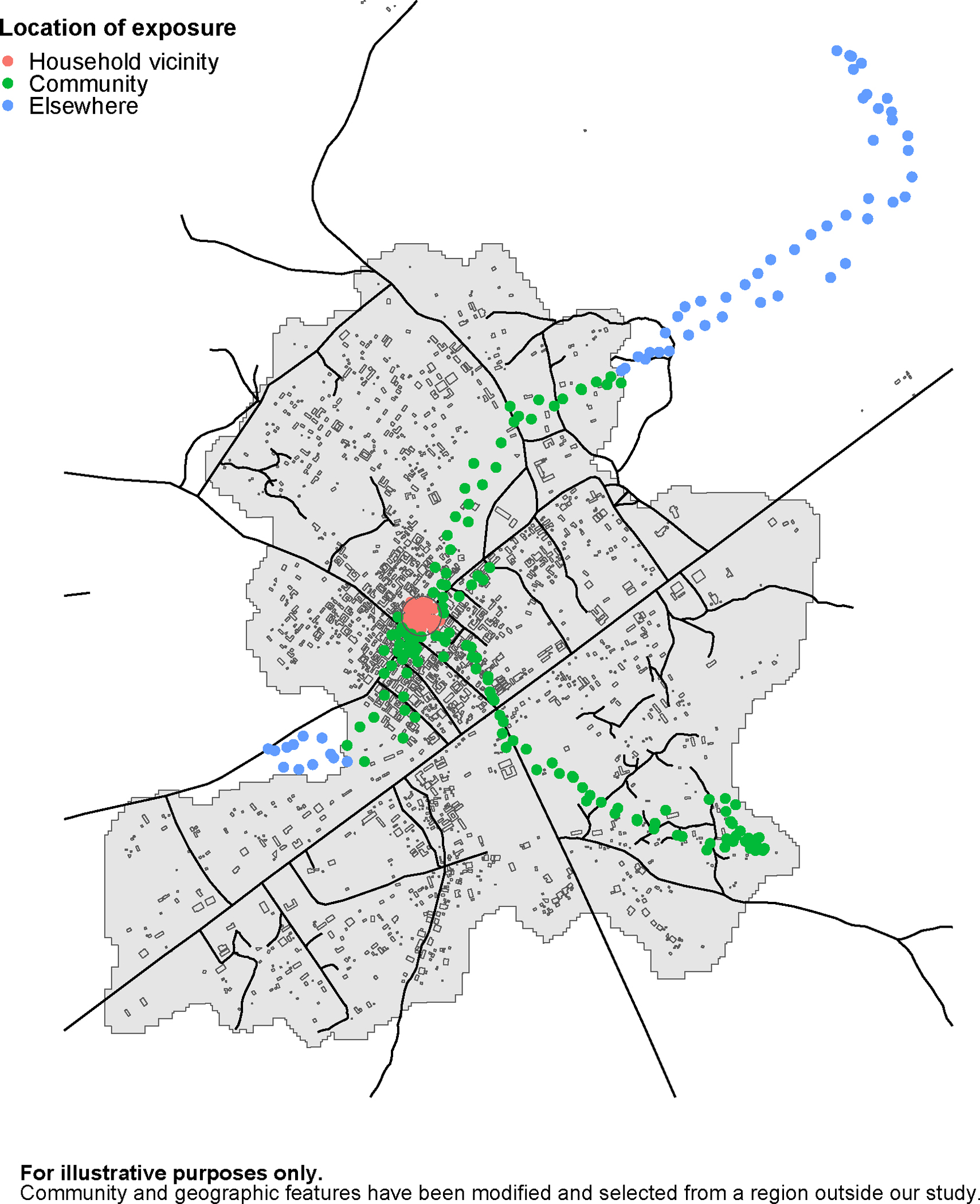
Example of a GPS trajectory throughout a session. GPS points are color-coded as being within the vicinity of the household (50m buffer), community boundaries or elsewhere. Outlines of arbitrary shapes represent buildings in the area and lines represent roadways.
Community boundaries
Administrative boundaries for communities in the Bono East Region of Ghana are not publicly available (and appear not to exist in any form). Therefore, we developed a geospatial dataset of community boundaries that encompass participants’ homes. We used the “Open Buildings” public dataset of building footprints for the continent of Africa that was developed by the Google AI team in Ghana and released in August 202129, 30. Briefly, the dataset was created using a machine learning method, U-net, that classified 50-centimeter pixels of satellite imagery as ‘building’ or ‘non-building’ along with a confidence level for the classification decision. The dataset includes spatial polygons that outline the footprints of each building, as well as the building centroid and the corresponding confidence level.
We developed community boundaries using buildings that had a confidence level of 70% or greater, which represented about 77% of buildings in our study region. This decision aimed to minimize false positives (such as mistaking other geographic features for buildings) and was guided by both the developers’ recommendations30 and our observations when overlaying polygons onto Google Maps satellite imagery. Communities were distinguished as groups of buildings belonging to the same cluster, identified with the spatial algorithm, DBSCAN (Density-Based Spatial Clustering of Applications with Noise)31–33. The DBSCAN method provides flexibility, permitting the formation of clusters, or ‘communities’ in the context of our study, of various shapes and sizes. It also does not require prior knowledge about the number of communities in the dataset, and can disregard sparse buildings seemingly not belonging to any community (e.g., outlying or industrial buildings). The algorithm requires two parameters: epsilon (the maximum distance between a given building and its neighbors within the same community) and the minimum number of neighboring buildings required to constitute a community. Reasonable epsilon values were determined using k-nearest neighbor graphs (k-NNG), which order the smallest distance between each building in our dataset and a specified number of neighboring buildings (k). Epsilon values were identified at the ‘elbow’ of the k-NNG, where distances beyond the ‘elbow’ suggest buildings are too far apart to reasonably belong to the same community (Figure S2). These values were inputted into the clustering algorithm and further refined based on visual assessment of resulting clusters. Once community clusters were created, spatial polygons were drawn around each cluster to form community boundaries (Figure S3), allowing for concavity34 and including a 50m buffer35. Otherwise, boundaries would intersect the centroid of bordering buildings within the cluster. Participants were assigned to the community whose boundaries encompassed their home location. Exposures that occurred within each participant’s community but outside their household boundaries were classified as ‘community exposures’ (Figure 1). An anonymized R workflow is accessible in the GitHub repository: https://github.com/dmedgyesi/GeospatialGhana.
Surrounding building density
The Open Buildings dataset was also used to estimate the building density surrounding each GPS coordinate. We chose to estimate building density within a 500m buffer of each location, a distance that has been previously used to obtain land use attributes around air monitoring sites and demonstrated to be predictive of air pollutant levels36–38.
The following two variables were created for each location: 1) the number of buildings within the buffer and 2) the building density, which was calculated as the sum of the area of all buildings within the buffer (m2) divided by the total area of the buffer (196,350 m2). Two variations of these variables were created: 1) including buildings with a confidence level of at least 70% and 2) further restricting to buildings with at least 80% confidence. The number of buildings and building density at both confidence levels were correlated (Spearman’s rho=0.97–0.98). Variables were categorized into tertiles and quartiles to evaluate exposure in areas with low- to high- building density.
Proximity to roadways
We obtained road data for our study region from OpenStreetMap (OSM), an open-source database of geographic features worldwide39. Despite the potential for crowd-sourced data like OSM to have less complete information in rural and developing regions40, 41, our linkage found a diverse range of road types in our study communities (n=35). Trunk roads were present in 46% of communities, secondary roads in 26%, tertiary roads in 11%, unclassified roads in 80%, residential roads in 43%, service roads in 14%, track roads in 26%, and footway roads in 6% (Table S1). As detailed in Table S1, it should be noted that ‘unclassified’ refers to minor roads classified lower than tertiary, not roads of unknown type.
We assessed proximity to roadways within a 100m radius of each GPS coordinate, a buffer size relevant to first-order decay of air pollutants from major roadways7, and shown to be associated with risk of several health outcomes (e.g., premature mortality, asthma) for those living near roadways at this distance9, 42. For each road type, we computed the segment length (meters) within a 100m radius of each location. The effect of nearby roadways on PM2.5 exposure was first assessed using a binary variable indicating whether any piece of road was within 100m. We created additional variables that further categorized locations near roadways as below or at or above the median segment length.
Statistical analyses
We described the distribution of logging time for mothers and children, as well as the percentage of total logging time by location (household vicinity, community boundaries or elsewhere) and wearing compliance during daylight hours (after 4 GMT and before 21 GMT). Wearing compliance was estimated using data from an embedded accelerometer in the MicroPEM device that indicates whether the device was worn at a given time (yes/no).
The distribution of average PM2.5 exposure per participant is reported overall and by participant type and whether the session occurred during the Harmattan season (December-March), a dry period with high winds that increase dust levels15. We also evaluated the distribution of PM2.5 exposure per participant averaged across categories of the following variables: time of day (morning cook hours: 5–9 GMT, evening cook hours: 16–20 GMT, nighttime: 21–4 GMT the next day, and other daytime hours), location, surrounding building density, nearby roadways and wearing compliance. Time of day and location were combined to evaluate exposure by location-time environment (e.g., community during cooking hours).
Our data follows a hierarchical structure, consisting of multiple non-independent PM2.5 measurements for each participant, many of whom reside in the same community. To account for such dependencies, we employed linear mixed effects models that incorporated nested random effects: community and participant ID. We estimated the change in log-transformed PM2.5 exposures by our fixed variables of interest including time of day, location, surrounding building density and nearby roadways. Models were adjusted for additional fixed variables including whether the session occurred in the Harmattan season, participant type and wearing compliance. Estimates are expressed as a factor, calculated as the exponent of the beta coefficient [eβ], along with corresponding 95% confidence intervals (95%CI). Additionally, we computed the conditional R2 for each model, which reflects the variance explained by both fixed and random effects.
Our primary models were designed to answer the three main research questions: 1) Does exposure differ by location and time of day?, 2) Does exposure in the household and community vary by time of day?, and 3) Is exposure also influenced by surrounding building density and nearby roadways? (Figure S4). Our first model estimated the change in exposure by time of day and location, included as separate variables. Our second model then combined these variables to evaluate exposure by location-time environment (e.g., in community during cooking periods). Building density was added to the third model, adjusting for location-time environment. Finally, all binary variables of nearby road types were added to the fourth model, adjusting for both location-time environment and building density. For road types that were associated with PM2.5 exposure, we further explored effects when split at the median segment length. In secondary analyses, we jointly modeled location-time environment and quartiles of building density, hypothesizing that the effect of building density may be greater during cooking hours. Given the strong influence of the Harmattan season on ambient dust levels, we also conducted stratified analyses, separately modeling sessions occurring in the non-Harmattan (n=193) and Harmattan season (n=66).
We evaluated our models for residual temporal autocorrelation using ACF plots and Durbin Watson Tests (DWT). To reduce temporal autocorrelation in our models due to high correlation between one-minute PM2.5 measurements (model series a), we also present results for 30-minute averaged data (model series b). In this approach, measurements were discarded if participants were observed in more than one location during a 30-minute window. While this resulted in data being lost for short-trips into the community, this approach has the advantage of removing brief observations on the household-boundary, likely reducing location misclassification. In addition to aggregating data to 30-minutes, we integrated a first-order autocorrelation structure within participant (model series c), which fully accounted for the dependence of lagged PM2.5 measurements (based on non-significant DWT). We evaluated for spatial autocorrelation using Moran’s I test. Before modeling, there was evidence of dependence in PM2.5 measurements at a small distance of approximately 200 meters (Moran’s I=0.20, p-value<0.001). We found limited evidence of spatial dependence in model series a-b residuals (Moran’s I=0.02–0.03) and no significant evidence of dependence in model series c residuals (Moran’s I=0.002), suggesting location and geographic covariates in our models accounted for spatial dependence.
RESULTS
Total logging time was similar for children and mother participants (median=48 hours); Table 1. The majority of participant logging time was spent within household boundaries (IQR=73–96% of total logging time). Most of the remaining time spent outside the household was within the community boundaries (IQR=2–13%). Time spent outside household and community boundaries varied by participant, where 25% of participants never left the community during the exposure monitoring period and another 25% of participants spent >10% of their time elsewhere. On average, children spent 4% more of their logging time in the community compared to mothers. Mothers spent about 6% more time outside both household and community boundaries than children, likely farming. On average, devices were worn by participants for 54% of daytime logging hours; distributions of wearing compliance for children and mothers were similar.
Table 1.
Distribution of total logging time (hours) for sessions with geolocated one-minute PM2.5 measurements, and the percentage of total logging time (%) by location and wearing compliance for children and mother participants in the Child Lung Function Study
| N sessions | Mean | Median | Perc. 25th | Perc. 75th | |
|---|---|---|---|---|---|
| Total logging time (hours) | |||||
| All participants | 259 | 45 | 48 | 46 | 49 |
| Children participants | 114 | 43 | 48 | 40 | 49 |
| Mother participants | 145 | 46 | 48 | 47 | 49 |
| Percentage of total logging time by location (%) | |||||
| All participants | |||||
| Household vicinity | 259 | 84 | 87 | 73 | 96 |
| Community boundaries | 259 | 10 | 6 | 2 | 13 |
| Outside both boundaries (elsewhere) | 259 | 7 | 1 | 0 | 11 |
| Children participants | |||||
| Household vicinity | 114 | 85 | 89 | 75 | 96 |
| Community boundaries | 114 | 12 | 7 | 3 | 17 |
| Outside both boundaries (elsewhere) | 114 | 3 | 0 | 0 | 2 |
| Mother participants | |||||
| Household vicinity | 145 | 83 | 83 | 72 | 96 |
| Community boundaries | 145 | 8 | 5 | 2 | 12 |
| Outside both boundaries (elsewhere) | 145 | 9 | 3 | 0 | 17 |
| Percentage wearing compliance (%) 1 | |||||
| All participants | 254 | 54 | 56 | 38 | 71 |
| Children participants | 109 | 54 | 58 | 40 | 71 |
| Mother participants | 145 | 53 | 54 | 37 | 71 |
Accelerometer data from the MicroPEM device was not available for 5 participants. During daytime hours after 4 GMT to before 21 GMT
Average participant PM2.5 exposures ranged from a median of 78μg/m3 and IQR of 49–114μg/m3 (Table 2). Average participant exposures were greater if conducted during the Harmattan season (median=105μg/m3) versus the non-Harmattan season (median=72μg/m3). Exposures during the day were higher when participants were wearing their device (median=110μg/m3) versus non-wearing periods (median=58μg/m3). Average exposures by time of day were lowest during the night (median=31μg/m3) and elevated during morning and evening cooking hours (median=83 and 123μg/m3, respectively). Patterns of elevated exposures during times of cooking were observed both in the household vicinity and community. In the community, median exposure was about 20μg/m3 higher during evening cook hours relative to non-cooking daytime hours. In the household, the median difference in exposure during morning (5–9 GMT) and evening (16–20 GMT) cook hours was about 10 and 40μg/m3 greater for mothers compared to children (Table S2).
Table 2.
Distribution of personal exposures to PM2.5 (μg/m3) among children and mothers in the Child Lung Function Study. For each participant, exposure was averaged for the duration of their session and reported overall, by participant type (child or mother) and by Harmattan season (December-March). Participant exposures were also averaged across categories of wearing compliance, time of day, location, surrounding building density and nearby roadways.
| PM2.5 exposure (μg/m3) | |||||
|---|---|---|---|---|---|
|
| |||||
| N participants | Mean | Median | Perc. 25th | Perc. 75th | |
|
| |||||
| PARTICIPANT EXPOSURES AVERAGED FOR DURATION OF SESSION | |||||
|
| |||||
| Overall | 259 | 100 | 78 | 49 | 114 |
| Children | 114 | 102 | 77 | 47 | 95 |
| Mothers | 145 | 99 | 81 | 54 | 119 |
| Harmattan season | |||||
| No | 193 | 94 | 72 | 43 | 95 |
| Yes | 66 | 117 | 105 | 84 | 137 |
|
| |||||
| PARTICIPANT EXPOSURES AVERAGED ACROSS CATEGORIES | |||||
|
| |||||
| Wearing compliance 1 | |||||
| No | 254 | 85 | 58 | 32 | 94 |
| Yes | 254 | 146 | 110 | 71 | 170 |
| Time of day | |||||
| Nighttime (21–4 GMT next day) | 259 | 46 | 31 | 18 | 59 |
| Morning cook hrs (5–9 GMT) | 258 | 125 | 83 | 41 | 155 |
| Evening cook hrs (16–20 GMT) | 259 | 198 | 123 | 82 | 202 |
| Other (non-cooking) daytime hours | 259 | 86 | 64 | 40 | 98 |
| Participant location | |||||
| Household vicinity | 259 | 98 | 78 | 48 | 113 |
| Community boundaries | 254 | 128 | 66 | 34 | 112 |
| Outside both boundaries (elsewhere) | 147 | 61 | 39 | 18 | 81 |
| Location-time environment | |||||
| Household, morning cook hrs | 257 | 113 | 81 | 41 | 156 |
| Household, evening cook hrs | 258 | 208 | 132 | 89 | 203 |
| Household, other daytime hrs | 259 | 88 | 61 | 36 | 102 |
| Household, nighttime | 259 | 46 | 32 | 18 | 59 |
| Community, morning cook hrs | 217 | 147 | 48 | 25 | 137 |
| Community, evening cook hrs | 196 | 170 | 70 | 38 | 128 |
| Community, other daytime hrs | 231 | 97 | 51 | 25 | 93 |
| Another place/time | 168 | 56 | 36 | 16 | 76 |
| Surrounding building density (500m) | |||||
| Quartiles | |||||
| Q1[0.000,0.011) | 157 | 85 | 57 | 30 | 95 |
| Q2[0.011,0.018) | 160 | 87 | 53 | 19 | 117 |
| Q3[0.018,0.032) | 162 | 104 | 62 | 31 | 102 |
| Q4[0.032,0.155] | 109 | 148 | 70 | 31 | 106 |
| Proximal to roadways (100m) | |||||
| Any segment length nearby, by road type | |||||
| Trunk | 149 | 154 | 82 | 38 | 134 |
| Primary | 2 | 54 | 54 | 50 | 59 |
| Secondary | 82 | 123 | 68 | 29 | 125 |
| Tertiary | 50 | 136 | 45 | 26 | 94 |
| Unclassified | 155 | 166 | 57 | 30 | 91 |
| Residential | 111 | 86 | 71 | 35 | 105 |
| Service | 34 | 67 | 25 | 8 | 73 |
| Track | 38 | 130 | 67 | 18 | 133 |
| Footway | 15 | 45 | 32 | 5 | 64 |
Accelerometer data from the MicroPEM device was not available for 5 participants. During daytime hours after 4 to before 21
Participant average exposures were generally greater in areas with higher versus lower building density/number of buildings. We observed the greatest differences across quartiles of building density with 80%+ confidence (medians Q1=57, Q2=53, Q3=62 and Q4=70μg/m3), and therefore we present this variable in our main findings (Table 2) and list other variations of surrounding buildings in supplementary information (Table S3). The distribution of average exposures in areas with the highest (Q4) versus lowest (Q1) building density, stratified by time of day, reveal differences are most pronounced during times of cooking (Figure 2).
Figure 2.
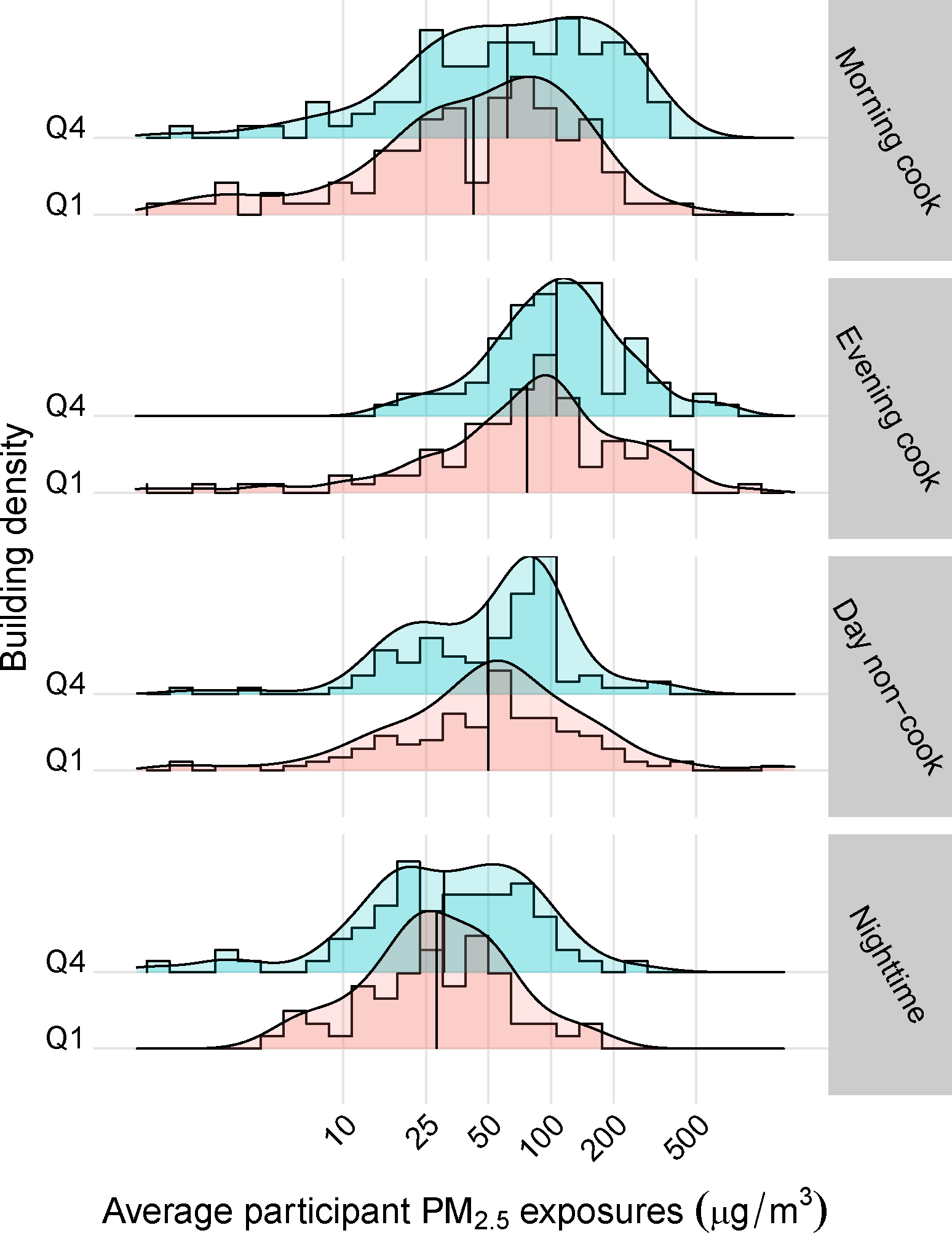
Distribution of average participant PM2.5 exposures (μg/m3) for the fourth versus first quartile (Q4 vs. Q1) of surrounding building density (80%+ confidence) by time of day. The intersecting black vertical line in each histogram represents the mean value.
We observed a large variation in the distribution of average exposures on/near roadways (Table 2), and no consistent patterns in exposure by roadway density (< or ≥ median segment length); Table S3. Only exposures occurring near trunk roadways were consistently greater at the mean (154μg/m3) and median (82μg/m3) relative to participant averages (mean=100μg/m3; median= 78μg/m3). Average exposure near trunk roadways was greater during the nighttime but not during the daytime when other sources of air pollution, such as cookstove emissions, likely dominate (Figure S5).
Results of our linear mixed effect models for one-minute and 30-minute averaged data, with and without first-order autocorrelation structure, are presented in Table 3. Results were similar for one- versus 30-minute data, albeit autoregressive results were attenuated, particularly during cooking hours when PM2.5 measurements are elevated and strongly correlated in time. Herein, we present results for 30-minute averaged data (model series b). Our models accounted for about 50% of the total variance in PM2.5, with marginal improvements from Model 1 to Model 4 (conditional R2=0.50 to 0.53, respectively).
Table 3.
Factor change and 95% confidence interval (95%CI) in log-transformed PM2.5 exposure (μg/m3) by time, location, surrounding building density and nearby roadways among children and mothers in the Child Lung Function Study1. Estimated with linear mixed effects models with nested random effects: community and participant ID. Results for model series a) one-minute data, b) 30-minute averaged data and c) 30-minute averaged data with first-order autocorrelation structure within participant.
| a) One-minute | b) 30-minute | c) 30-minute autoregressive | ||
|---|---|---|---|---|
| Factor (95CI)2 | Factor % (95CI) | Factor % (95CI) | ||
|
| ||||
| MODEL 1: Time of day and location | ||||
| Time of day | ||||
| Nighttime (21–4 next day) | REF | REF | REF | |
| Morning cook hours (5–9) | 1.62 (1.6, 1.64) | 1.72 (1.64, 1.81) | 1.44 (1.36, 1.54) | |
| Evening cook hours (16–20) | 2.50 (2.47, 2.52) | 2.74 (2.62, 2.87) | 1.63 (1.54, 1.74) | |
| Other daytime hours | 1.12 (1.11, 1.13) | 1.16 (1.12, 1.21) | 1.18 (1.13, 1.23) | |
| Participant location | ||||
| Outside both boundaries (elsewhere) | REF | REF | REF | |
| Household vicinity | 2.15 (2.12, 2.18) | 2.12 (1.98, 2.28) | 2.17 (1.99, 2.37) | |
| Community boundaries | 1.65 (1.62, 1.68) | 1.60 (1.46, 1.76) | 1.70 (1.54, 1.89) | |
| Harmattan season | ||||
| No | REF | REF | REF | |
| Yes | 3.17 (2.47, 4.08) | 3.20 (2.53, 4.05) | 3.07 (2.44, 3.85) | |
| Participant type | ||||
| Child | REF | REF | REF | |
| Mother | 0.68 (0.55, 0.84) | 0.74 (0.61, 0.91) | 0.77 (0.64, 0.94) | |
| Wearing compliance | ||||
| No | REF | REF | REF | |
| Yes | 1.37 (1.36, 1.39) | 1.36 (1.31, 1.41) | 1.23 (1.19, 1.27) | |
|
| ||||
| Conditional R2 | 0.413 | 0.498 | 0.384 | |
|
| ||||
| MODEL 2: Location-time environment 3 | ||||
|
| ||||
| Household, nighttime | REF | REF | REF | |
| Household, morning cook hrs | 1.58 (1.56, 1.6) | 1.69 (1.61, 1.78) | 1.44 (1.35, 1.53) | |
| Household, evening cook hrs | 2.61 (2.58, 2.63) | 2.84 (2.70, 2.98) | 1.71 (1.61, 1.82) | |
| Household, other daytime hours | 1.10 (1.09, 1.11) | 1.14 (1.10, 1.19) | 1.18 (1.13, 1.23) | |
| Community, morning cook hrs | 1.41 (1.37, 1.44) | 1.49 (1.28, 1.72) | 1.14 (1.00, 1.3) | |
| Community, evening cook hrs | 1.81 (1.76, 1.85) | 1.80 (1.54, 2.10) | 1.37 (1.20, 1.56) | |
| Community, other daytime hours | 0.85 (0.84, 0.87) | 0.89 (0.82, 0.97) | 0.91 (0.83, 1.00) | |
| Another place/time | 0.61 (0.60, 0.62) | 0.62 (0.58, 0.67) | 0.63 (0.57, 0.69) | |
|
| ||||
| Conditional R 2 | 0.414 | 0.499 | 0.385 | |
|
| ||||
| MODEL 3: Surrounding building density 3,4 | ||||
|
| ||||
| Quartiles building density (500m) | ||||
| Q1[0.000,0.011) | REF | REF | REF | |
| Q2[0.011,0.018) | 0.89 (0.86, 0.91) | 0.90 (0.80, 1.02) | 0.96 (0.84, 1.08) | |
| Q3[0.018,0.032) | 1.42 (1.39, 1.46) | 1.47 (1.31, 1.65) | 1.28 (1.13, 1.45) | |
| Q4[0.032,0.155] | 1.57 (1.53, 1.61) | 1.60 (1.42, 1.80) | 1.36 (1.19, 1.55) | |
| Conditional R2 | 0.426 | 0.518 | 0.396 | |
| MODEL 4: Proximal to roadways 3,4,5 | ||||
| On or nearby (100m) road type? | ||||
| Trunk | No | REF | REF | REF |
| Yes | 1.13 (1.11, 1.14) | 1.16 (1.07, 1.25) | 1.23 (1.15, 1.32) | |
| Secondary | No | REF | REF | REF |
| Yes | 0.93 (0.91, 0.95) | 0.90 (0.81, 1.00) | 1.00 (0.91, 1.11) | |
| Tertiary | No | REF | REF | REF |
| Yes | 1.6 (1.55, 1.66) | 1.68 (1.45, 1.95) | 1.31 (1.13, 1.51) | |
| Unclassified | No | REF | REF | REF |
| Yes | 0.97 (0.95, 0.99) | 0.97 (0.89, 1.06) | 1.02 (0.94, 1.10) | |
| Residential | No | REF | REF | REF |
| Yes | 0.83 (0.81, 0.84) | 0.77 (0.70, 0.85) | 0.93 (0.84, 1.02) | |
| Service | No | REF | REF | REF |
| Yes | 0.69 (0.65, 0.73) | 1.15 (0.87, 1.52) | 1.12 (0.91, 1.38) | |
| Track | No | REF | REF | REF |
| Yes | 1.10 (1.05, 1.15) | 1.27 (1.06, 1.53) | 1.18 (1.01, 1.39) | |
| Footway | No | REF | REF | REF |
| Yes | 1.28 (0.9, 1.82) | 0.54 (0.27, 1.08) | 0.96 (0.65, 1.41) | |
|
| ||||
| Conditional R2 | 0.435 | 0.531 | 0.400 | |
|
| ||||
| Model 4.1: Roadway density (100m) 3,4,5 | ||||
|
| ||||
| Trunk | Zero | REF | REF | REF |
| <median (1, 164m) | 1.07 (1.05, 1.09) | 1.12 (1.03, 1.22) | 1.21 (1.13, 1.31) | |
| ≥median (165, 403m) | 1.18 (1.16, 1.21) | 1.19 (1.08, 1.31) | 1.28 (1.17, 1.41) | |
| Tertiary | Zero | REF | REF | REF |
| <median (3, 168m) | 1.44 (1.38, 1.50) | 1.34 (1.13, 1.59) | 1.21 (1.05, 1.40) | |
| ≥median (169, 263m) | 1.64 (1.58, 1.71) | 1.83 (1.54, 2.19) | 1.62 (1.33, 1.98) | |
| Track | Zero | REF | REF | REF |
| <median (0.3, 104m) | 1.05 (1.00, 1.11) | 1.08 (0.87, 1.34) | 1.18 (0.99, 1.39) | |
| ≥median (105, 344m) | 1.25 (1.17, 1.33) | 1.77 (1.37, 2.28) | 1.31 (1.02, 1.69) | |
| Conditional R2 | 0.430 | 0.523 | 0.404 | |
Includes 259 participant sessions with geo-located PM2.5 measurements
Computed as the exponent of the beta coefficient []
Adjusted for Harmattan season, participant type, and wearing compliance
Additionally adjusted for location-time environment
Additionally adjusted for building density
Model 1.
Exposures on average were 1.72 (95%CI=1.64–1.81) and 2.74 (95%CI=2.62–2.87) times higher during morning and evening cook hours, respectively, relative to nighttime exposure. Relative to exposure outside the community boundaries, PM2.5 exposure was 2.12 (95%CI=1.98–2.28) and 1.60 (95%CI=1.46–1.76) times greater in the household and community, respectively. On average, exposure was over three times higher during the Harmattan season (3.20, 95%CI=2.53–4.05). When the device was worn, exposure on average was 1.36 (95%CI=1.31–1.41) times higher. Exposure among mothers compared to children was lower (0.74, 95%CI=0.61–0.91), controlling for cooking times.
Model 2.
Modeling time and location jointly, we found exposure was greatest during evening cooking hours in respective locations (household: 2.84, 95%CI=2.70–2.98; community: 1.80, 95%CI=1.54–2.10; reference=household, nighttime). Exposure during morning cooking hours was also elevated in the household (1.69, 95%CI=1.61–1.78) and community (1.49, 95%CI=1.28–1.72). Exposure during non-cooking daytime hours was somewhat higher in the household (1.14, 95%CI=1.10–1.19) and lower in the community (0.89, 95%CI=0.82 to 0.97).
Model 3.
Exposures were greater in areas with higher building density, although the second quartile was somewhat lower in reference to the first quartile (Q2=0.90, 95%CI=0.80–1.02; Q3=1.47, 95%CI=1.31–1.65, and Q4=1.60, 95%CI=1.42–1.80); ptrend<0.001. When modeling location-time environment and quartiles of building density jointly, the effect of building density was strongest during cooking hours in both the household and community (Figure 3). For example, the relative percentage increase from Q1 to Q4 during evening cooking hours was 31% and 65% in the household and community, respectively.
Figure 3.
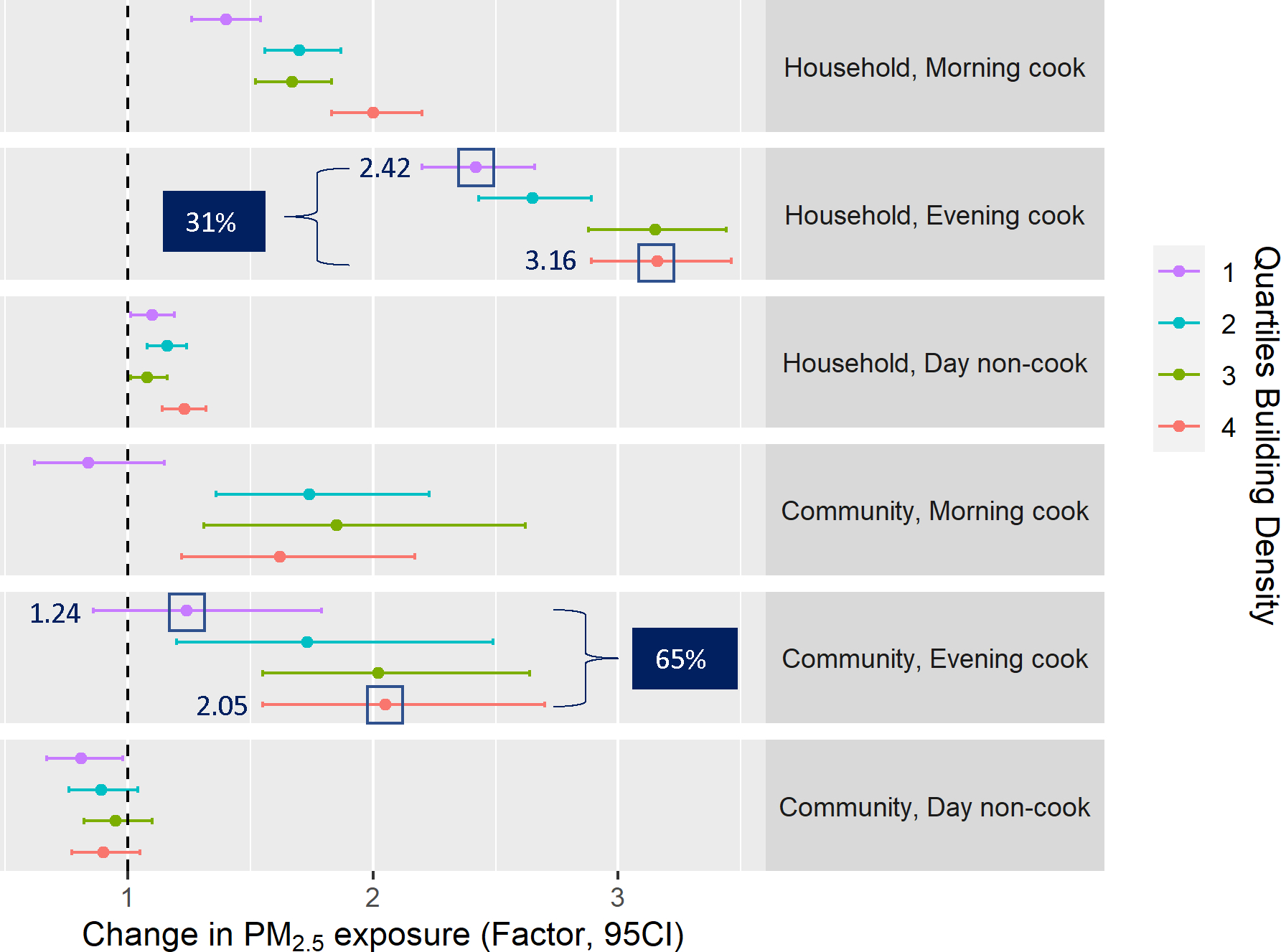
Factor change in 30-minute average log-transformed PM2.5 exposure (μg/m3) and 95% confidence intervals for location-time environments modeled jointly with quartiles of surrounding building density. Reference is exposures during nighttime in the household. Model adjusted for nested random effects community and participant ID and fixed effects Harmattan season, participant type (child or mother) and wearing compliance. Dark blue box shows the relative percentage increase from Q1 to Q4.
Model 4.
Exposures were significantly higher by a factor of 1.16, 1.68 and 1.27 when near a trunk, tertiary or track road, respectively; exposures were somewhat lower when near a secondary, residential or footway road. We observed further increases in exposure when near a higher density (≥median segment length) of trunk (1.19, 95%CI=1.08–1.31), tertiary (1.83, 95%CI=1.54–2.19) or track (1.77, 95%CI=1.37–2.28) road.
In our analysis stratified by the Harmattan season, we found the change in PM2.5 exposure during cooking times was more pronounced among sessions conducted outside the Harmattan season (Table S4). Likewise, the effect of being proximal to a road was more pronounced during the non-Harmattan versus Harmattan season (trunk=1.10 versus 1.07, tertiary=1.88 versus 1.27, track=1.20 versus 1.14, respectively). However, the effect of building density was stronger during the Harmattan season (FactorQ1vsQ4=2.23, 95%CI=1.80–2.75) versus non-Harmattan season (FactorQ1vsQ4=1.28, 95%CI=1.09–1.49).
DISCUSSION
Our study described patterns of personal exposure to PM2.5 among mothers and children living in rural Ghana by location, time of day, as well as geographic features including building density and nearby roadways. We found that PM2.5 exposure was elevated in the morning and evening cooking hours. Exposure during cooking times was elevated both within the household and community. We found higher building density was associated with higher exposure, and that the effect was strongest during typical cooking hours. Finally, we report that PM2.5 exposure is greater when proximal to roadways.
To our knowledge, this is the first study to describe both spatial and temporal patterns of personal exposure to PM2.5 in communities that primarily rely on solid fuels for domestic cooking and energy. We demonstrated that exposures in the community follow patterns observed in the household during typical hours of cooking. Few studies have reported that air pollution levels in the community are influenced by solid fuel use in households4–6. A comparison of ambient PM2.5 measurements collected at the center of two rural communities in Nepal found community levels were 37% higher during hours of cooking relative to a background site (i.e., forest region)4. In comparison to exposure in the household at nighttime, we report exposures were 49–80% greater (Factor=1.49–1.80) in the community during cooking hours.
We found exposures were greater in areas with higher building density, and that this effect was strongest during typical cooking hours. Further, we found building density influenced both levels within the household vicinity (50m buffer) and the community during hours of cooking. This provides evidence that neighboring home activities not only contribute to outdoor PM2.5 levels, but could also influence levels in other households especially in more densely populated communities. This aligns with a study conducted in Bangladesh, which found that when a household used solid fuels for cooking, PM2.5 levels increased in both the surrounding outdoor environment, as well as within neighboring households that used cleaner fuels6.
We observed exposures were higher at the fourth quartile of building density when including buildings with 80%+ detection confidence (median/average= 70/148 μg/m3) versus 70%+ confidence (median/average= 63/133 μg/m3). Buildings detected with a higher degree of confidence tend to be larger in size, which may imply a greater presence of multi-family compounds in our defined 80%+ confidence range. Multi-family compounds are common in our study region and often feature shared courtyards typically used for simultaneous cooking activities, which may significantly contribute to nearby PM2.5 exposure. While definitively distinguishing multi-family homes is challenging due to a lack of detailed building information (e.g., number of rooms), future work to enhance our dataset by describing building contour and size could enable us to differentiate multi-family compounds and further understand their impact on PM2.5 exposure in communities.
We found evidence that PM2.5 exposure is greater when near a trunk, tertiary or track road. This highlights that traffic-related exposures, in addition to solid fuel use, may be an important contributor to personal exposure in rural settings10–14. The Techiman-Tamale Rd (N-10), extending north to south from the city center of Kintampo, is the primary trunk road in our study region and is likely an important source of vehicle exhaust43. Proximity to a trunk road increased PM2.5 exposure by a factor of 1.16. Being near a tertiary road had a greater impact on exposure (Factor=1.68). The tertiary roads within our study region are typically smaller, unpaved roads leading to communities and may be an important source of resuspended dust44. Likewise, track roads, which are often unpaved and used for agricultural activities, increased exposure by a factor of 1.27. Our findings align with a study in Bogotá, Colombia, which found unpaved roads emitted about five times more PM10 and twice as much PM2.5 per kilometer compared to paved roads45. However, proximity to other road types (e.g., secondary, residential, unclassified, service and footway) did not increase exposure and may be due to characteristics not captured by our approach, such as traffic volume.
Exposures were more than three times greater during the Harmattan season, underscoring the need to account for seasonality differences. When restricting to sessions in the non-Harmattan season, the impact of cooking periods and proximity to roadways on exposure was more pronounced. Dust during the Harmattan season is an important source of air pollution, and therefore higher background levels may diminish the relative changes due to other sources. On the contrary, the influence of building density on exposure was more marked during the Harmattan season. Although we can only speculate, regions with greater building density may experience higher PM2.5 levels during the Harmattan season due to altered pollutant dispersion, lower vegetation or other community-wide burning activities, like trash burning or bush burning.
Our findings have important implications for the design of policies that aim to reduce the burden of disease from household and outdoor air pollution. Our findings underscore the importance of prioritizing community-wide transitions to cleaner fuel use in the household. This includes community-wide initiatives to reduce inequities in access to clean fuels, often driven by education, employment and income17. Otherwise, even if wealthier households switch to cleaner cookstoves, they and the rest of the community remain at risk of unsafe exposure levels if other households continue to use solid fuels. Our observations of increased exposure near roadways and in areas with high building density highlight the potential benefits of development initiatives such as road surfacing and sustainable urban planning (e.g., incorporation of greenspaces and greenways)46–49. However, the successful implementation of these initiatives depends on an understanding of the local context and residents’ needs, effective public education and policy advocacy, and the strengthening of institutional capacities47–49. It should also be noted that the generalizability of our findings may be somewhat limited by the specific characteristics of our study communities. These communities, while rural and small, feature closely spaced households which may not be representative of other rural settings. In addition, household cooking often occurs outside near the house, which may not be representative of other communities that use solid fuels for cooking.
The use of personal measurements provided a more accurate assessment of exposure levels near the breathing zone, but is dependent upon wearer compliance and is subject to exposure measurement and location error. Our study evaluated patterns of personal exposure to PM2.5 at a fine temporal and spatial resolution. Geolocated exposure data at a one-minute resolution allowed us to quantify geographic features within small spatial scales, such as roadways within 100m, a distance that is relevant to the decay of vehicle emissions. However, the fine resolution of our data also introduced spatial and temporal autocorrelation in our models of PM2.5 exposure. Spatial dependency, observed at a small distance of 200 meters, was mostly explained by our covariates of interest. We reduced temporal autocorrelation by aggregating data to 30-minutes. A first-order autoregressive model fully resolved temporal autocorrelation, but likely underestimated the change in exposure during cooking hours when lagged PM2.5 measurements are strongly correlated.
While we defined the household vicinity based on patterns of PM2.5 exposure near the home in an effort to account for outside cooking activities, the size of each household’s vicinity is likely to vary and could result in misclassification when evaluating household versus community exposures. We quantified roadway and building density using buffer sizes around each GPS location based on previous literature7, 9, 36–38, 42, but exploration of various buffer sizes may provide insight into PM2.5 dispersion. While not readily available, the integration of meteorological variables, such as precipitation, wind speed and direction, could improve the precision of our effect estimates and overall model performance. Wind speed and direction, in particular, play a significant role in pollutant dispersion, and their integration could provide a more nuanced understanding of the influence of roadways on personal PM2.5 exposure. Our models demonstrated moderate explanatory power, ranging from a conditional R2 of 0.38 to 0.53, which would likely improve with the addition of meteorological conditions.
In our geospatial analysis of personal PM2.5 exposure among mothers and children in rural Ghana, we found that exposure was elevated within the household vicinity and the community during the morning and evening hours when solid fuels are typically used for cooking. Additionally, exposures on average were greater in areas with the highest versus lowest building density, and the effect of building density on PM2.5 exposure was pronounced during hours of cooking. We report that roadways also contribute to elevated PM2.5 exposure, particularly main and unpaved roads leading to rural communities. Our study provides evidence that, in some settings at least, policies intended to promote cleaner fuel use will be most effective at reducing household and ambient air pollution if implemented at the community-level. Future work should consider the role of solid fuel use in the household on air pollution levels in the community, and investigate other community-wide burning activities, such as trash burning and bush burning during the dry season.
Supplementary Material
IMPACT STATEMENT.
Household air pollution from cooking with solid fuels in sub-Saharan Africa is a major environmental concern for maternal and child health. Our study advances previous knowledge by quantifying the impact of household cooking activities on air pollution levels in the community, and identifying two geographic features, building density and roadways, that contribute to maternal and child daily exposure. Household cooking contributes to higher air pollution levels in the community especially in areas with greater building density. Findings underscore the need for equitable clean household energy transitions that reach entire communities to reduce health risks from household and outdoor air pollution.
ACKNOWLEDGEMENTS:
The authors are grateful to the mothers and their children who participated in the study. The authors would also like to thank the community leaders in the study area for their support.
FUNDING:
This work was supported by the National Institute of Environmental Health Sciences (NIEHS) Grants R01 ES026991, P30 ES009089, R01 ES019547, R21 HD094229, R01 ES024489, R01 ES034433, K23 HL1353449, and T32 ES007322.
Footnotes
COMPETING INTERESTS: The authors declare no competing interests.
ETHICAL APPROVAL: The protocol for this study was approved by the Kintampo Health Research Center Institutional Ethics Committee, and the Institutional Review Board for Human Subjects Research at Columbia University Medical Center and Mount Sinai.
DATA AVAILABILITY STATEMENT:
The datasets generated during and/or analyzed during the current study are not publicly available because this analysis included geolocated information considered to be personally identifiable information (PII). However, the authors have created a GitHub repository demonstrating the development of community boundaries as well as estimating surrounding building density and nearby roadways using a simulated GPS trajectory [https://github.com/dmedgyesi/GeospatialGhana]
REFERENCES
- 1.Bennitt F, Wozniak S, Causey K, Burkart K, Brauer M Estimating disease burden attributable to household air pollution: new methods within the Global Burden of Disease Study. The Lancet Global Health 2021; 9. [Google Scholar]
- 2.Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet 2017; 389: 1907–1918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.HEI Household Air Pollution–Ghana Working Group. Contribution of Household Air Pollution to Ambient Air Pollution in Ghana. Health Effects Institute 2019; Communication 19. [Google Scholar]
- 4.Adhikari S, Mahapatra PS, Pokheral CP, Puppala SP Cookstove Smoke Impact on Ambient Air Quality and Probable Consequences for Human Health in Rural Locations of Southern Nepal. Int J Environ Res Public Health 2020; 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Downward GS, Hu W, Rothman N, Reiss B, Wu G, Wei F et al. Outdoor, indoor, and personal black carbon exposure from cookstoves burning solid fuels. Indoor Air 2016; 26: 784–795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Weaver AM, Gurley ES, Crabtree-Ide C, Salje H, Yoo EH, Mu L et al. Air pollution dispersion from biomass stoves to neighboring homes in Mirpur, Dhaka, Bangladesh. BMC Public Health 2019; 19: 425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Clougherty JE, Wright RJ, Baxter LK, Levy JI Land use regression modeling of intra-urban residential variability in multiple traffic-related air pollutants. Environmental Health 2008; 7: 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fuks KB, Weinmayr G, Basagaña X, Gruzieva O, Hampel R, Oftedal B et al. Long-term exposure to ambient air pollution and traffic noise and incident hypertension in seven cohorts of the European study of cohorts for air pollution effects (ESCAPE). Eur Heart J 2017; 38: 983–990. [DOI] [PubMed] [Google Scholar]
- 9.Requia WJ, Koutrakis P Mapping distance-decay of premature mortality attributable to PM2.5-related traffic congestion. Environmental Pollution 2018; 243: 9–16. [DOI] [PubMed] [Google Scholar]
- 10.Baumgartner J, Zhang Y, Schauer JJ, Huang W, Wang Y, Ezzati M Highway proximity and black carbon from cookstoves as a risk factor for higher blood pressure in rural China. Proceedings of the National Academy of Sciences 2014; 111: 13229–13234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ni K, Carter E, Schauer JJ, Ezzati M, Zhang Y, Niu H et al. Seasonal variation in outdoor, indoor, and personal air pollution exposures of women using wood stoves in the Tibetan Plateau: Baseline assessment for an energy intervention study. Environment International 2016; 94: 449–457. [DOI] [PubMed] [Google Scholar]
- 12.Carter E, Archer-Nicholls S, Ni K, Lai AM, Niu H, Secrest MH et al. Seasonal and Diurnal Air Pollution from Residential Cooking and Space Heating in the Eastern Tibetan Plateau. Environmental Science & Technology 2016; 50: 8353–8361. [DOI] [PubMed] [Google Scholar]
- 13.Van Vliet ED, Asante K, Jack DW, Kinney PL, Whyatt RM, Chillrud SN et al. Personal exposures to fine particulate matter and black carbon in households cooking with biomass fuels in rural Ghana. Environ Res 2013; 127: 40–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lai AM, Clark S, Carter E, Shan M, Ni K, Yang X et al. Impacts of stove/fuel use and outdoor air pollution on chemical composition of household particulate matter. Indoor Air 2020; 30: 294–305. [DOI] [PubMed] [Google Scholar]
- 15.Chillrud SN, Ae-Ngibise KA, Gould CF, Owusu-Agyei S, Mujtaba M, Manu G et al. The effect of clean cooking interventions on mother and child personal exposure to air pollution: results from the Ghana Randomized Air Pollution and Health Study (GRAPHS). Journal of Exposure Science & Environmental Epidemiology 2021; 31: 683–698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jack DW, Ae-Ngibise KA, Gould CF, Boamah-Kaali E, Lee AG, Mujtaba MN et al. A cluster randomised trial of cookstove interventions to improve infant health in Ghana. BMJ Global Health 2021; 6: e005599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bofah RO, Appiah-Konadu P, Ngwu FN Transition to cleaner cooking energy in Ghana. Clean Energy 2022; 6: 957–966. [Google Scholar]
- 18.Lee AG, Kaali S, Quinn A, Delimini R, Burkart K, Opoku-Mensah J et al. Prenatal Household Air Pollution Is Associated with Impaired Infant Lung Function with Sex-Specific Effects. Evidence from GRAPHS, a Cluster Randomized Cookstove Intervention Trial. American Journal of Respiratory and Critical Care Medicine 2018; 199: 738–746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Quinn AK, Ae-Ngibise KA, Jack DW, Boamah EA, Enuameh Y, Mujtaba MN et al. Association of Carbon Monoxide exposure with blood pressure among pregnant women in rural Ghana: Evidence from GRAPHS. Int J Hyg Environ Health 2016; 219: 176–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Quinn AK, Ae-Ngibise KA, Kinney PL, Kaali S, Wylie BJ, Boamah E et al. Ambulatory monitoring demonstrates an acute association between cookstove-related carbon monoxide and blood pressure in a Ghanaian cohort. Environ Health 2017; 16: 76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Boamah-Kaali E, Jack DW, Ae-Ngibise KA, Quinn A, Kaali S, Dubowski K et al. Prenatal and Postnatal Household Air Pollution Exposure and Infant Growth Trajectories: Evidence from a Rural Ghanaian Pregnancy Cohort. Environmental Health Perspectives; 129: 117009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Adams C, Riggs P, Volckens J Development of a method for personal, spatiotemporal exposure assessment. J Environ Monit 2009; 11: 1331–1339. [DOI] [PubMed] [Google Scholar]
- 23.Jack DW, Asante KP, Wylie BJ, Chillrud SN, Whyatt RM, Ae-Ngibise KA et al. Ghana randomized air pollution and health study (GRAPHS): study protocol for a randomized controlled trial. Trials 2015; 16: 420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Carrión D, Prah R, Gould CF, Agbokey F, Mujtaba M, Pillarisetti A et al. Using longitudinal survey and sensor data to understand the social and ecological determinants of clean fuels use and discontinuance in rural Ghana. Environ Res Commun 2020; 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Daouda M, Mujtaba MN, Yang Q, Seyram K, Lee AG, Tawiah T et al. Prediction of personal exposure to PM2.5 in mother-child pairs in rural Ghana. Journal of Exposure Science & Environmental Epidemiology 2022; doi 10.1038/s41370-022-00420-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kaali S, Jack DW, Prah RKD, Chillrud SN, Mujtaba MN, Kinney PL et al. Poor early childhood growth is associated with impaired lung function: Evidence from a Ghanaian pregnancy cohort. Pediatr Pulmonol 2022; 57: 2136–2146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chakrabarti B, Fine PM, Delfino R, Sioutas C Performance evaluation of the active-flow personal DataRAM PM2.5 mass monitor (Thermo Anderson pDR-1200) designed for continuous personal exposure measurements. Atmospheric Environment 2004; 38: 3329–3340. [Google Scholar]
- 28.Arnold TB. leaderCluster: Leader Clustering Algorithm. In: R package version 1.2., 2014. [Google Scholar]
- 29.Sirko W, Kashubin S, Ritter M, Annkah A, Bouchareb YSE, Dauphin Y et al. Continental-scale building detection from high resolution satellite imagery. arXiv 2021; https://arxiv.org/abs/2107.12283. [Google Scholar]
- 30.Open Buildings A dataset of building footprints to support social good applications. Google Research, Ghana 2021; https://sites.research.google/open-buildings/. [Google Scholar]
- 31.Density-Based Clustering Based on Hierarchical Density Estimates. Berlin, Heidelberg. Springer Berlin Heidelberg, 2013. [Google Scholar]
- 32.Ester M, Kriegel H-P, Sander J, Xu X. A density-based algorithm for discovering clusters in large spatial databases with noise. In: Proceedings of the Second International Conference on Knowledge Discovery and Data Mining. Portland, Oregon: AAAI Press, 1996. pp 226–231. [Google Scholar]
- 33.Hahsler M, Piekenbrock M, Doran D dbscan: Fast Density-Based Clustering with R. Journal of Statistical Software 2019; 91: 1 – 30. [Google Scholar]
- 34.Gombin J, Vaidyanathan R, Agafonkin V. concaveman: A Very Fast 2D Concave Hull Algorithm. In: R package version 1.1.0., 2020. [Google Scholar]
- 35.Pebesma E Simple Features for R: Standardized Support for Spatial Vector Data. The R Journal 2018; 10: 439–446. [Google Scholar]
- 36.Poplawski K, Gould T, Setton E, Allen R, Su J, Larson T et al. Intercity transferability of land use regression models for estimating ambient concentrations of nitrogen dioxide. Journal of Exposure Science & Environmental Epidemiology 2009; 19: 107–117. [DOI] [PubMed] [Google Scholar]
- 37.Amini H, Taghavi M, Naddafi K, Nabizadeh R, Yunesian M Correlation of air pollutants with land use and traffic measures in Tehran, Iran: A preliminary statistical analysis for land use regression modeling. Journal of Advances in Environmental Health Research 2013; 1: 1–8. [Google Scholar]
- 38.Coker ES, Amegah AK, Mwebaze E, Ssematimba J, Bainomugisha EA land use regression model using machine learning and locally developed low cost particulate matter sensors in Uganda. Environ Res 2021; 199: 111352. [DOI] [PubMed] [Google Scholar]
- 39.Padgham M, Rudis B, Lovelace R, Salmon M osmdata. Journal of Open Source Software 2017; 2. [Google Scholar]
- 40.Kim-Blanco P, Cîrlugea B-M, de Sherbinin A. Quality assessment of crowd-sourced data: OpenStreetMap roads validation in the developing countries of West Africa. 2018. [Google Scholar]
- 41.Herfort B, Lautenbach S, Porto de Albuquerque J, Anderson J, Zipf A The evolution of humanitarian mapping within the OpenStreetMap community. Scientific Reports 2021; 11: 3037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Baumann LM, Robinson CL, Combe JM, Gomez A, Romero K, Gilman RH et al. Effects of distance from a heavily transited avenue on asthma and atopy in a periurban shantytown in Lima, Peru. J Allergy Clin Immunol 2011; 127: 875–882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Brugge D, Durant JL, Rioux C Near-highway pollutants in motor vehicle exhaust: A review of epidemiologic evidence of cardiac and pulmonary health risks. Environmental Health 2007; 6: 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Samiksha S, Sunder Raman R, Nirmalkar J, Kumar S, Sirvaiya R PM10 and PM2.5 chemical source profiles with optical attenuation and health risk indicators of paved and unpaved road dust in Bhopal, India. Environmental Pollution 2017; 222: 477–485. [DOI] [PubMed] [Google Scholar]
- 45.Pachón JE, Galvis B, Lombana O, Carmona LG, Fajardo S, Rincón A et al. Development and Evaluation of a Comprehensive Atmospheric Emission Inventory for Air Quality Modeling in the Megacity of Bogotá. Atmosphere 2018; 9: 49. [Google Scholar]
- 46.Mikou M, Rozenberg J, Koks EE, Fox CJE, Peralta Quiros T Assessing rural accessibility and rural roads investment needs using open source data. World Bank Policy Research Working Paper 2019. [Google Scholar]
- 47.Takyi E, Mensah H, Aazore FK, Nalumu DJ, Abu JJ Understanding the Urban Planning-Green Space Depletion Nexus: Insights from the Kwabre East Municipality, Ghana. Urban Forum 2022; doi 10.1007/s12132-022-09471-x. [DOI] [Google Scholar]
- 48.Diko SK, Hollstein LM Towards an alternative interpretation of the socio-cultural dimensions of urban greenspace planning in the Global South: Evidence from the Kumasi Metropolis of Ghana. Journal of Urban Affairs 2023; 45: 522–545. [Google Scholar]
- 49.Abass K, Appiah DO, Afriyie K Does green space matter? Public knowledge and attitude towards urban greenery in Ghana. Urban Forestry & Urban Greening 2019; 46: 126462. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available because this analysis included geolocated information considered to be personally identifiable information (PII). However, the authors have created a GitHub repository demonstrating the development of community boundaries as well as estimating surrounding building density and nearby roadways using a simulated GPS trajectory [https://github.com/dmedgyesi/GeospatialGhana]