

Abstract
Background:
In developing and developed countries, the prevalence of overweight and obesity has grown. The college phase is a critical period during which healthy behaviors are learned through lifestyle and social environment. College students are prone to increased stress, negatively affecting their daily activities and academic performance.
Objective:
The general study objective was to investigate the prevalence of obesity among Jazan University students.
Methods:
This observational cross-sectional study used a pre-tested self-administered anonymous electronic questionnaire to evaluate the prevalence of obesity among 474 Jazan University students and its association with academic performance, physical activity, and social support. Data were analyzed using the Statistical Package for the Social Sciences, and associations between variables were assessed using the chi-square test.
Results:
Approximately 21% and 9.2% of the male and female students were obese, respectively, and the prevalence of obesity significantly differed between them. The use of one or more tobacco products was significantly associated with the prevalence of obesity (P < 0.001); the prevalence of obesity was substantially higher among the tobacco product users than among the non-users (35.3% vs. 14.4%). The presence of a morbidity was also significantly associated with the prevalence of obesity (P = 0.007); the prevalence of obesity was significantly higher among the students with at least one comorbidity than among the medically free students (28.8% vs. 14.9%). Conversely, obesity was not associated with academic performance and depression. Specifically, the grade point average was not affected across the academic years (P = 0.085 and P = 0.308, respectively).
Conclusion:
Obesity is significantly associated with male sex and the use of one or more tobacco products. This finding warrants the need for strategic and multidisciplinary plans at all levels to encourage healthy behaviors among college students, including an active, healthy lifestyle.
Keywords: Physical activity, Grade point average, University students, Obesity
1. BACKGROUND
According to the World Health Organization, obesity is a worldwide health issue, with about 1.5 billion people overweight in 2008. Overweight and obesity kill more people than underweight in the majority of the world’s population (1, 2). The prevalence of obesity in developing countries has risen in the last 20 years as these countries have become more urbanized, with high consumption of foods with high calories and a more sedentary lifestyle (3, 4). These changes have led to significant modifications in lifestyle and living patterns (5), making them the leading causes of several diseases, including hypertension, diabetes mellitus (DM), obstructive sleep apnea (OSA), hyperlipidemia, and osteoarthritis (6).
Body mass index (BMI) measurements are widely utilized in determining the link between obesity and academic performance. Obese university students are shown to have a higher risk of psychological problems (e.g., anxiety and depression) and social isolation, which can affect their academic performance and need for social support—a factor essential in preventing obesity (7, 8). Contrary to BMI-based obesity, which is linked to CVD and other non-communicable illnesses, waist circumference-based abdominal obesity is linked to increased risks of CVD and DM (9). Dietary change and sedentary behavior also contribute to the rising prevalence of overweight and obesity in developing countries (10, 11).
Numerous studies have evaluated obesity. In one study that examined the demographic, dietary, and physical activity (PA) variables of overall and abdominal obesity among university students in Ghana, male students showed a lower mean BMI than female students. Approximately 5% of students were abdominally obese. The mostly consumed food groups were animal products, cereals, and grains. Over half of students engaged in intense activity, with 67% of them being men ( 10).
Another study of Mexican university students revealed that the frequency of obesity strongly correlated with the use of one or more tobacco products (12). In another previous study among university students in China, the prevalence of obesity was 9.5%, and some factors, including students’ social status, affected the level of obesity (13).
In a study of 842 randomly selected Kuwait University students, obesity was shown to be highly prevalent: 32.0% for grade 1 obesity and 9.8% for grade 2 obesity (14). In Saudi Arabia, several studies have also evaluated obesity among students. One of these studies, which was conducted at Al-Qassim, revealed that 15.7% and 21.8% of university students were obese and overweight, respectively (15). In a study conducted in Riyadh, 31% of students were overweight, while 23.3% were obese (16).
In other studies, academic achievement was negatively correlated with BMI and insignificantly related to PA (17). Further, female medical students with a BMI of 21–25 and 26–30 kg/m 2 achieved high grade point averages (GPAs), while those with a BMI of 31–35 and ≥36 kg/m2 achieved low GPAs (18).
To our knowledge, several studies have examined the prevalence of obesity and how it relates to university students’ academic success and PA, but few have evaluated this specific topic in Jazan, Saudi Arabia.
2. OBJECTIVE
The general study objective was to investigate the prevalence of obesity among Jazan University students. The specific objectives were to a) determine the prevalence of obesity, overweight, and underweight among university students; assess the association between obesity; b) PA and c) academic performance; d) assess the awareness of university students of the health risks associated with obesity; and e) investigate the association between social support and risky health behaviors related to obesity.
3. MATERIAL AND METHODSs
Design, Population, and Setting
This observational cross-sectional study was conducted among students at Jazan University in Jazan, Saudi Arabia, from May to August 2022. Students aged >18 years willing to participate in the study were included. Conversely, students aged <18 years studying in other universities were excluded. The participants were recruited via random sampling, which yielded a required sample size of 385 students.
Data Collection
Data were collected using a pre-tested self-administered anonymous electronic questionnaire. The questionnaire was developed in English and translated into Arabic. A pilot study was conducted to evaluate the validity of the questionnaire.
The questionnaire had multiple sections. Section 1 evaluated participant demographics, while section 2 assessed academic performance (i.e., GPA) and PA and their association with obesity. Academic performance was measured using a self-reported grade system scale. The frequency of PA was assessed using the Youth Risk Behavior Survey. Finally, section 3 evaluated social support. Three items were drawn from the Social Support Questionnaire to assess perceived social support. These items reflect perceived tangible and emotional support.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences version 23. Categorical variables were presented as frequencies and percentages and numerical variables as means and standard deviations. The chi-square test was used to test for categorical variables associated with the prevalence of obesity and an independent t-test for numerical variables. P-values of <0.05 were considered significant.
Ethical approval: The study was approved by standing committee for scientific research ethics with reference number of REC43/11/255. All identifying information was removed from the report, and personal data was protected to protect the participants’ privacy.
4. RESULTS
A total of 474 participants were included in the study. Table 1 shows the socio-demographic and academic profiles of the participants. As for age, the mean age of the participants was 22.15 ± 3.64 years. As for sex, 300 (633%) were men, while 174 (36.7%) were women. As for the college, 349 (73.6%) were studying in health-related colleges, while 125 (26.4%) reported studying in non-health-related colleges. As for the use of tobacco products, 51 (10.8%) reported using them, while 423 (89.2%) reported not using them.
Table 1. Socio-Demographic and Academic Profiles of the Participants (N = 474).
| Demographic characteristics | n | % |
|---|---|---|
| Age, year | ||
| Mean | 22.15 | |
| Standard deviation | 3.64 | |
| Sex | ||
| Male | 300 | 63.30 |
| Female | 174 | 36.70 |
| Nationality | ||
| Saudi | 464 | 97.90 |
| Non-Saudi | 10 | 2.10 |
| Place of residency | ||
| Rural area | 238 | 50.20 |
| Urban area | 236 | 49.80 |
| College | ||
| Health-related college | 349 | 73.60 |
| Non-health-related college | 125 | 26.40 |
| Academic year | ||
| First year | 40 | 8.40 |
| Second year | 82 | 17.30 |
| Third year | 132 | 27.80 |
| Fourth year | 67 | 14.10 |
| Fifth year | 30 | 6.30 |
| Sixth year | 44 | 9.30 |
| Internship | 79 | 16.70 |
| Grade point average | ||
| ≤3 | 20 | 4.20 |
| 3–3.5 | 39 | 8.20 |
| 3.5–4 | 76 | 16.00 |
| 4–4.5 | 117 | 24.70 |
| 4.5–4.75 | 100 | 21.10 |
| 4.75–5 | 122 | 25.70 |
| Current use of one or more of the following tobacco products: cigarettes, snuff, or cigars | ||
| Yes | 51 | 10.80 |
| No | 423 | 89.20 |
Table 2 demonstrates the social support profile of the participants. The mean social support score of the participants was 8.26 ± 2.42 (lowest possible score = 3, highest possible score = 12).
Table 2. Social Support Profile of the Participants (N = 474).
| Question | n | % |
|---|---|---|
| 1. If I become sick and need someone to take me to the doctor, I will have a difficult time finding someone. | ||
| Completely true | 71 | 15 |
| Maybe true | 77 | 16.2 |
| Maybe false | 87 | 18.4 |
| Completely false | 239 | 50.4 |
| 2. I feel like there is no one I can share my own concerns and fears with. | ||
| Completely true | 98 | 20.7 |
| Maybe true | 123 | 25.9 |
| Maybe false | 81 | 17.1 |
| Completely false | 172 | 36.3 |
| 3. I feel a strong emotional connection with at least one other person. | ||
| Completely true | 131 | 27.6 |
| Maybe true | 112 | 23.6 |
| Maybe false | 81 | 17.1 |
| Completely false | 150 | 31.6 |
| Social support score (lowest possible score = 3, highest possible score = 12) | ||
| Mean | 8.26 | |
| Standard deviation | 2.42 | |
Table 3 illustrates the PA profile of the participants. Among them, 185 (39%) reported that they never exercised or participated in PA for at least 20 minutes that made them sweat, while 187 (39.5%) reported that they did for 1–3 days, 77 (16.2%) for 4–6 days, and 25 (5.3%) every day. Conversely, 245 (51.7%) reported that they never exercised or participated in PA for at least 20 minutes that did not make them sweat, while 148 (31.2%) reported that they did for 1–3 days, 52 (11%) for 4–6 days, and 29 (6.1%) every day.
Table 3. Physical Activity Profile of the Participants (N = 474).
| Physical Activity Profile of the Participants (N = 474) | ||
|---|---|---|
| Question | n | % |
| In the last 7 days, how many days have you exercised or participated in physical activity for at least 20 minutes that made you sweat? | ||
| 0 days | 185 | 39 |
| 1–3 days | 187 | 39.5 |
| 4–6 days | 77 | 16.2 |
| 7 days (every day) | 25 | 5.3 |
| In the last 7 days, how many days have you exercised or participated in physical activity for at least 20 minutes that did not make you sweat? | ||
| 0 days | 245 | 51.7 |
| 1–3 days | 148 | 31.2 |
| 4–6 days | 52 | 11 |
| 7 days (every day) | 29 | 6.1 |
Table 4 shows the factors associated with the prevalence of obesity. Sex was significantly associated with the prevalence of obesity (P = 0.001), wherein the men had a significantly higher prevalence of obesity than the women (21% vs. 9.2%). The use of one or more tobacco products was also significantly associated with the prevalence of obesity (P < 0.001), whereas the incidence of obesity was substantially greater among tobacco product users than among non-users (35.3% vs. 14.4%). The presence of a morbidity was also significantly associated with the prevalence of obesity (P = 0.007), wherein the incidence of obesity among students with at least one comorbidity was considerably more significant than that of medically free students (28.8% vs. 14.9%).
Table 4. Factors Associated with the Prevalence of Obesity.
| Factor | P-value | ||
|---|---|---|---|
| With obesity | Without obesity | ||
| Age, year (mean, standard deviation) | 22.8 ± 3.81 | 22.02 ± 3.59 | 0.083 |
| Sex (n, %) | 0.001* | ||
| Male | 63 (21%) | 237 (79%) | |
| Female | 16 (9.2%) | 158 (90.8%) | |
| Nationality (n, %) | 0.253 | ||
| Saudi | 76 (16.4%) | 388 (83.6%) | |
| Non-Saudi | 3 (30%) | 7 (70%) | |
| Place of residency (n, %) | 0.565 | ||
| Rural area | 42 (17.6%) | 196 (82.4%) | |
| Urban area | 37 (15.7%) | 199 (84.3%) | |
| College (n, %) | 0.545 | ||
| Health-related college | 56 (16%) | 293 (84%) | |
| Non-health-related college | 23 (18.4%) | 102 (81.6%) | |
| Academic year (n, %) | 0.308 | ||
| First year | 5 (12.5%) | 35 (87.5%) | |
| Second year | 11 (13.4%) | 71 (86.6%) | |
| Third year | 18 (13.6%) | 114 (86.4%) | |
| Fourth year | 15 (22.4%) | 52 (77.6%) | |
| Fifth year | 5 (16.7%) | 25 (83.3%) | |
| Sixth year | 12 (27.3%) | 32 (72.7%) | |
| Internship | 13 (16.5%) | 66 (83.5%) | |
| Grade point average (n, %) | 0.085 | ||
| ≤3 | 6 (30%) | 14 (70%) | |
| 3–3.5 | 10 (25.6%) | 29 (74.4%) | |
| 3.5–4 | 14 (18.4%) | 62 (81.6%) | |
| 4–4.5 | 23 (19.7%) | 94 (80.3%) | |
| 4.5–4.75 | 12 (12%) | 88 (88%) | |
| 4.75–5 | 14 (11.5%) | 108 (88.5%) | |
| Current use of one or more of the following tobacco products: cigarettes, snuff, or cigars | <0.001* | ||
| Yes | 18 (35.3%) | 33 (64.7%) | |
| No | 61 (14.4%) | 362 (85.6%) | |
| Presence of comorbidities | 0.007* | ||
| Medically free | 62 (14.9%) | 353 (85.1%) | |
| At least one comorbidity | 17 (28.8%) | 42 (71.2%) | |
| Presence of hypertension | 0.111 | ||
| Yes | 3 (37.5%) | 5 (62.5%) | |
| No | 76 (16.3%) | 390 (83.7%) | |
| Presence of diabetes mellitus | 0.395 | ||
| Yes | 2 (28.6%) | 5 (71.4%) | |
| No | 77 (16.5%) | 390 (83.5%) | |
| Presence of depression | 0.261 | ||
| Yes | 6 (25%) | 18 (75%) | |
| No | 73 (16.2%) | 377 (83.3%) | |
| In the last 7 days, how many days have you exercised or participated in physical activity for at least 20 minutes that made you sweat? | 0.795 | ||
| 0 days | 31 (16.8%) | 154 (83.2%) | |
| 1–3 days | 28 (15%) | 159 (85%) | |
| 4–6 days | 15 (19.5%) | 62 (80.5%) | |
| 7 days (every day) | 5 (20%) | 20 (80%) | |
| In the last 7 days, how many days have you exercised or participated in physical activity for at least 20 minutes that did not make you sweat? | 0.228 | ||
| 0 days | 47 (19.2%) | 198 (80.8%) | |
| 1–3 days | 24 (16.2%) | 124 (83.3%) | |
| 4–6 days | 4 (7.7%) | 48 (92.3%) | |
| 7 days (every day) | 4 (13.8%) | 25 (86.2%) | |
| Social support score (mean, standard deviation) | 8.37 ± 2.38 | 8.24 ± 2.43 | 0.665 |
| *Significant at <0.05 | |||
Figure 1 displays the medical history of the participants. A total of 415 (87.6%) participants were medically free, while 59 (12.4%) had at least one comorbidity. Among the participants, 24 (5.1%) had depression; 8 (1.7%) had hypertension; 7 (1.5%) had DM; and 22 (4.6%) had other comorbidities.
Figure 1. Medical history of the participants.
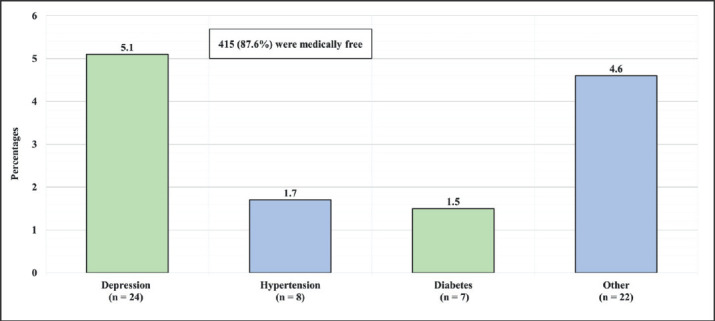
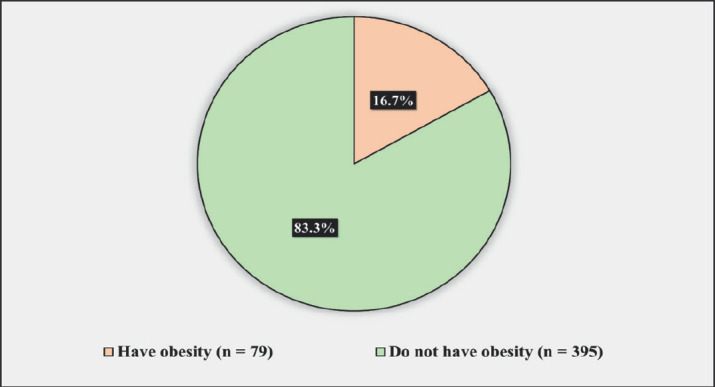
Figure 2 presents the prevalence of obesity among the participants. Approximately 16.7% of the participants had obesity, while 83.3%
Figure 2. Prevalence of obesity among the participants.
5. DISCUSSION
The prevalence of obesity among the participants was strongly affected by sex, wherein obesity was substantially more prevalent among the men than among the women (21% vs. 9.2%). This finding is consistent with reports from Saudi Arabia and other Gulf countries, Middle East countries, and other international countries.
In a study conducted among 701 male King Saud University students, 31% of the study sample was overweight (BMI of 25–30 kg/m2), and 23.3% was obese (BMI of ≥30 kg/m2). Only 45.8% had a normal body weight (BMI of <25 kg/m2) (16). In another study performed among 357 male Qassim University students aged 18–24 years, the average BMI of participants was 24.6 kg/m2, with a standard deviation of 5.2. Approximately 57.4% had a normal weight; 21.8% were overweight; 15.7% were obese; and 5% were underweight (15 ).
A study conducted in Egypt among 398 male and female university students revealed that 28.9% of students were overweight; 11.8%, obese; 55.8%, of normal weight; and 3.5%, underweight (19). Conversely, an exploratory research conducted among 842 Kuwait University students showed that the prevalence of grades 1 and 2 obesity was 32.0% and 9.8%, respectively. These rates are comparable to those recorded in Arabian Gulf countries but higher than the 8% and 1% reported in European countries (14). Similar findings were found in two studies in Ghana and China, where the prevalence of obesity was low: 9.5% (95% CI = 7.7%, 11.3%) and 5%, respectively (10-13 ).
Our study did not find an association between obesity and academic performance and depression. Specifically, the GPA was not affected across the academic years. These findings are consistent with other reports from Saudi Arabia and Sri Lanka. In Saudi Arabian studies, academic achievement was found to be negatively correlated with BMI and insignificantly related to PA (17). Female medical students with BMIs of 21–25 and 26–30 kg/m2 had excellent GPAs, whereas those with BMIs of 31–35 and ≥36 kg/m 2 had poor GPAs (18). In a different study, BMI was used to evaluate the relationship between obesity and academic achievement at the University of Kelaniya in Sri Lanka. Obese university students were shown to be more likely to have psychological problems (e.g., anxiety and depression) and social isolation, which affected their academic performance and need for social support—a crucial factor in preventing obesity (7, 8). Another study conducted among 1,122 university students in Mexico found that students with changed eating habits had higher levels of impulsivity (e.g., difficulties in stopping eating, odds ratio [OR] = 4.2) and depression (e.g., problems eating at regular times, OR = 6.98) (12 ).
The present study found that the use of one or more tobacco products was also significantly associated with the prevalence of obesity, wherein the prevalence of obesity was substantially higher among the tobacco product users than among the non-users (35.3% vs. 14.4%). In a previous study conducted in Iran, about 12.4% of university students had a BMI of >25 kg/m2, and there was a significant association between BMI and smoking habits (20).
Herein, the presence of a morbidity was also significantly associated with the prevalence of obesity (Figure 1 and 2), wherein the prevalence of obesity was significantly higher among the students with at least one comorbidity than among the medically free students (28.8% vs. 14.9%). This finding coincides with that of two previous studies: One study conducted in Saudi Arabia found an increasing prevalence of both overweight and obesity, which are the main causes of several other diseases, including hypertension, DM, OSA, hyperlipidemia, and osteoarthritis, among Saudi children, adolescents, and adults in the last few decades (6). Another study suggested that obesity raises the overall risk of CVD and DM (9).
Finally, most of our participants did not follow physical exercise recommendations. They stated that they had never engaged in PA for at least 20 min, which would have resulted in sweating or not. The current results are supported by previous reports showing that the prevalence of obesity in developing countries has risen in the last 20 years as these countries have become more urbanized, with high consumption of foods with high calories and a more sedentary lifestyle (3-5). Therefore, college students must be encouraged by healthcare providers to increase their PA for optimum health benefits.
As with any other cross-sectional study, the fact that the data were collected from only one university—Jazan University—limits the generalizability of the results, indicating that the sample might not represent students from other universities. Further, the students’ GPA was based on self-reports, increasing the likelihood of human error. Hence, acquiring an official GPA report from students’ official records might minimize the possibility of human mistakes. Similarly, the anthropometric measurements were self-reported. Nevertheless, to our best knowledge, this study is the first to investigate the prevalence of obesity among university students in Jazan. The findings may be used as a basis to establish educational programs to prevent or minimize obesity and provide solutions for losing weight and maintaining a good GPA. The study may also be utilized as a foundation for subsequent studies.
6. CONCLUSION
The prevalence of obesity was substantially higher among the male students than among the female students; among the tobacco product users than among the non-users; and among the students with at least one comorbidity than among the medically free students. The growing prevalence of obesity among college students is an alarming sign that demands an urgent need to educate students about the health risks linked to obesity. Moreover, this finding indicates the need for strategic and multidisciplinary plans at all levels, including the community, Ministry of Health, and Ministry of Education, to find ways to encourage healthy behaviors among college students, such as an active, healthy lifestyle.
Authors contribution:
The all authors were involved in all steps of preparation this article. Final proofreading was made by the first author.
Conflict of interest:
None to decalre.
Financial support and sponsorship:
Nil.
REFERENCES
- 1.Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000:i–xii. 1–253. [PubMed] [Google Scholar]
- 2.Alqarni SS. A Review of Prevalence of Obesity in Saudi Arabia. J Obes Eat Disord. 2016;2(2):25. [Google Scholar]
- 3.Haidar YM, Cosman BC. Obesity epidemiology. Clinics in colon and rectal surgery. 2011;24(4):205–210. doi: 10.1055/s-0031-1295684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Peltzer K, Pengpid S, Samuels TA, Özcan NK, Mantilla C, Rahamefy OH, Gasparishvili A. Prevalence of overweight/obesity and its associated factors among university students from 22 countries. International journal of environmental research and public health. 2014;11(7):7425–7441. doi: 10.3390/ijerph110707425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bani IA, Hashim TJ. Knowledge of nutrition and coronary heart disease in Riyadh, Saudi Arabia. Journal of community health. 1999;24(6):467–473. doi: 10.1023/a:1018798723532. [DOI] [PubMed] [Google Scholar]
- 6.Memish ZA, El Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S, Al Rabeeah AA. Peer reviewed: obesity and associated factors—Kingdom of Saudi Arabia. 2014;2013 doi: 10.5888/pcd11.140236. Preventing chronic disease: 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wehigaldeniya WGDS, Oshani PAL, Kumara IMNS. Height, weight, body mass index (BMI) and academic performance (AP) of university students in Sri Lanka: with special reference to the University of Kelaniya. International Journal of Scientific and Research Publications. 2017;7(2):217–219. [Google Scholar]
- 8.So WY, Swearingin B, Robbins J, Lynch P, & Ahmedna M. Relationships between body mass index and social support, physical activity, and eating habits in African American university students. Asian nursing research. 2012;6(4):152–157. doi: 10.1016/j.anr.2012.10.004. [DOI] [PubMed] [Google Scholar]
- 9.Folsom AR, Kaye SA, Sellers TA, Hong CP, Cerhan JR, Potter JD, Prineas RJ. Body fat distribution and 5-year risk of death in older women. JAMA. 1993;269(4):483–487. [PubMed] [Google Scholar]
- 10.Mogre V, Nyaba R, Aleyira S. Lifestyle risk factors of general and abdominal obesity in students of the school of medicine and health science of the University of Development Studies, Tamale, Ghana. International Scholarly Research Notices. 2014 doi: 10.1155/2014/508382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Azadbakht L, Esmaillzadeh A. Dietary and non-dietary determinants of central adiposity among Tehrani women. Public health nutrition. 2008;11(5):528–534. doi: 10.1017/S1368980007000882. [DOI] [PubMed] [Google Scholar]
- 12.Lazarevich I, Irigoyen-Camacho ME, del Consuelo Velázquez-Alva M. Obesity, eating behaviour and mental health among university students in Mexico City. Nutricion hospitalaria. 2013;28(6):1892–1899. [PubMed] [Google Scholar]
- 13.Yang T, Yu L, Barnett R, Jiang S, Peng S, Fan Y, L L. Contextual influences affecting patterns of overweight and obesity among university students: a 50 universities population-based study in China. International Journal of Health Geographics. 2017;16(1):1–13. doi: 10.1186/s12942-017-0092-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ai-Isa AN. Obesity among Kuwait University students: an explorative study. The journal of the Royal Society for the Promotion of Health. 1999;119(4):223–227. doi: 10.1177/146642409911900404. [DOI] [PubMed] [Google Scholar]
- 15.Al-Rethaiaa AS, Fahmy AEA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutrition journal. 2010;9(1):1–10. doi: 10.1186/1475-2891-9-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Turki YA. Overweight and obesity among university students, Riyadh, Saudi Arabia. Middle East J Fam Med. 2007;5(2):1–3. [Google Scholar]
- 17.Alhazmi A, Aziz F, Hawash MM. Association of BMI, Physical Activity with Academic Performance among Female Students of Health Colleges of King Khalid University, Saudi Arabia. International journal of environmental research and public health. 2021;18(20):10912. doi: 10.3390/ijerph182010912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Al-Rethaiaa AS, Fahmy AEA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutrition journal. 2010;9(1):1–10. doi: 10.1186/1475-2891-9-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Genena DM, Salama AA. Obesity and eating habits among university students in Alexandria, Egypt: A cross sectional study. World journal of nutrition and health. 2017;5(3):62–68. [Google Scholar]
- 20.Nojomi M, Najamabadi S. Obesity among university students, Tehran, Iran. Asia Pacific journal of clinical nutrition. 2006;15(4):516–520. [PubMed] [Google Scholar]