

Abstract
Background:
The term “developmental disability” (DD) is inconsistently defined and applied depending on purpose and across sources, including in legislation.
Objective:
This project aimed to identify existing definitions of disability and DD and to determine the extent to which each definition could be operationalized to produce prevalence estimates using data from U.S. national surveys.
Methods:
Using data among children <18 years from the 2016–2018 National Health Interview Survey (NHIS) and National Survey of Children’s Health (NSCH), we estimated the prevalence of two definitions of disability (Washington Group Short Set on Functioning, American Community Survey) and seven definitions of DD [Health and Human Services (ever/current), Developmental Disabilities Assistance and Bill of Rights Act of 2000 (1+ 2+, or 3+ components), and Diagnostic and Statistical Manual of Mental Disorders, 5th ed (ever/current)]. Complex sample design variables and weights were used to calculate nationally representative prevalence.
Results:
Disability (NHIS: 5.2–6.3%; NSCH: 9.2–11.9%) and DD prevalence (NHIS: 0.6–18.0% and NSCH: 0.2–22.2%) varied depending on the definition and data source. For the same definition, NSCH prevalence estimates tended to be higher than NHIS estimates.
Conclusions:
The substantial variability in estimated prevalence of disability and DD among children in the United States may be in part due to the surveys not representing all components of each definition. Different or additional questions in national surveys may better capture existing definitions of disability and DD. Considering the data collection goals may help determine the optimal definition to provide useful information for public health action.
Keywords: Disability, Developmental disability, Definition, Measurement, Measurement purpose
1. Introduction
Understanding the prevalence of developmental disability (DD) is important for evaluating risk and protective factors and appropriate supports and services for optimal outcomes among children. The term “developmental disability” is defined and applied in different ways depending on purpose and across sources, including in federal and state policies and laws.1–5 Methodological clarity is crucial for appropriately addressing public health questions; the definitions used in surveillance and research shape who may be included in data, and thus should be aligned with the intended use of the data. Without understanding the impact of how DD is defined, comparisons across data sources and analyses may not be meaningful.
The term “disability” itself lacks a singular definition.6 The International Classification of Functioning, Disability, and Health defines disability as “an umbrella term for impairments, activity limitations, and participation restrictions”.7 While this paradigm is widely accepted, the concept is operationalized in different ways, most based on either functional limitations or identified diagnoses. The traditional medical model of disability focuses on a professionally-designated diagnosis, which does not always correlate with uniform functional limitations. For example, one child with autism spectrum disorder (ASD) may be minimally verbal whereas another child with the same diagnosis may be highly verbal with the ability to use complex sentences. On the other hand, disability defined by functional limitations does not rely on an underlying medical diagnosis. For example, a child with a mobility limitation could have a variety of different underlying diagnoses such as cerebral palsy, muscular dystrophy, or an injury. When assessing interventional needs and health equity issues within the community, diagnosis may be less important than how the environment in which someone lives either impedes or improves their ability to function. This latter definition of disability may be more useful for identifying, developing, implementing, and evaluating supports, and is in line with eligibility determinations for services such as special education supports based on functioning in the educational setting.8 However, knowledge of a diagnosis that is leading to functional limitations may help inform treatment and support, so there may often be utility in capturing both functional and diagnostic information.
The addition of the word “developmental” to “disability” compounds the challenge of measurement. DDs are a group of conditions due to an impairment in physical, learning, language, or behavior areas that begin during the developmental period and usually last throughout life.9 However, there is variation in the number, types, and degree of impairments to be considered DDs. For example, the Developmental Disabilities Assistance and Bill of Rights Act of 2000 (DD Act) indicates that in addition to being due to a physical or mental condition manifested before age 22 and expected to continue indefinitely, the person should have substantial functional limitations in 3 or more areas of 7 major life activities and need specialized services and supports for an extended duration, if not for a lifetime.2 The DD Act definition tends to focus on individuals with higher degrees of disability requiring more services and supports. However, children with specific developmental disabilities such as a speech-language impairment or learning disability may still require and benefit from specialized supports but may not qualify as having a DD depending on the context. Also, while the age range encompassing the developmental period is defined as through 18 or 22 years of age, it is less clear whether disability due to injury or illness with later onset is considered a DD. Public health researchers often leverage available data sources that only provide information on reported or documented diagnoses, which does not provide specific information on functional limitations. However, more national surveys have begun measuring disability using questions targeted at categorizing functional limitations.
Recent work highlights the difficulty of measuring disability and DD in surveys. Hagerman et al. evaluated the prevalence of disability based on existing definitions using a single data source, the National Survey of Children’s Health (NSCH).10 They found only a small degree of overlap across the definitions; 23.5% of U.S. children in the sample met one or more definition and only 8.7% of children met all five definitions. Anderson et al. performed a systematic review of studies reporting the prevalence of intellectual or DDs in all ages within the United States since 2000, finding that prevalence varied across years, ages, definitions, and data sources.1 These results are unsurprising given the complexities in defining disability, DD, and functional limitations, particularly during the dynamic periods of childhood and adolescence.
This paper builds upon past work by examining multiple definitions of disability and DD in children, comparing prevalence based on those definitions across multiple national surveys, and using more recent data sources. Our aim was to investigate how different definitions of developmental disabilities impact the estimated prevalence using multiple national, publicly available surveys. We anticipated the best alignment to be among definitions using similar scope of definition (e.g., disability or developmental disability) and data collection purposes (e.g., domains of functional disability or identified diagnoses/conditions).
2. Methods
We identified the following definitions for “disability” and “developmental disability” from expert groups and for governmental purposes, such as policy, laws, and surveillance reports: the Washington Group Short Set on Functioning (WG-SS),11 the American Community Survey Question Set (ACS-6),12 the surveillance definition used in Health and Human Services (HHS) surveillance reports,13–15 the Developmental Disabilities Assistance and Bill of Rights Act of 2000 (DD Act),2 and the definition of neurodevelopmental disabilities in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).3
We examined sources of nationally representative, publicly available health data that were likely to have any information on DD status. For each data source, we assessed the extent to which identified definitions of DD could be fully or partially operationalized for the purpose of prevalence estimation. We assessed the following surveys: the National Health Interview Survey (NHIS), the National Survey of Children’s Health (NSCH), the National Health and Nutrition Examination Survey (NHANES), and the American Community Survey (ACS).
Each component of the identified definitions was matched with the best fitting variables from selected surveys. Some variables were not exact matches to the definition component but had similar meanings. Other components did not have a suitable survey variable to match and were not able to be incorporated into our prevalence estimates.
2.1. Washington Group short set on functioning (WG-SS)
The WG-SS is a set of six questions designed for people ages five years and older that captures a functional definition of disability (Table 1). Another question set from the Washington Group on Disability Statistics, the Washington Group-United Nations Children’s Fund Child Functioning Module (WG-CFM), measures functional disability across all children, including those under five years of age.16 While the WG-CFM question set would likely better capture DD than the WG-SS question set, the WG-CFM set is significantly longer and has far fewer variable matches across surveys. We determined that any prevalence estimates from the limited data available corresponding to this definition would not be meaningful.
Table 1.
Components of selected definitions of disability or developmental disability and their ability to be fully or partially operationalized in selected national surveys.
| DEFINITION COMPONENTS | NHIS | NSCH |
|---|---|---|
|
| ||
| Disability: Washington Group Short Set on Functioning a | ||
| Do you have difficulty seeing, even if wearing glasses? | Y | Y |
| Do you have difficulty hearing, even if using a hearing aid? | Y | Y |
| Do you have difficulty walking or climbing steps? | Y | Yc |
| Do you have difficulty remembering or concentrating? | N | Yc |
| Do you have difficulty (with self-care such as) washing all over or dressing? | N | Yc |
| Using your usual (customary) language, do you have difficulty communicating, for example understanding or being understood? | N | N |
| Disability: American Community Survey Question Set b | ||
| Are you deaf, or do you have serious difficulty hearing? | Y | Y |
| Are you blind, or do you have serious difficulty seeing even when wearing glasses? | Y | Y |
| 5 years old and over: Because of a physical, mental, or emotional condition, do you have difficulty concentrating, remembering, or making decisions? | N | Yc |
| 5 years old and over: Do you have serious difficulty walking or climbing stairs? | Y | Yc |
| 5 years old and over: Do you have difficulty dressing or bathing? | N | Yc |
| 15 years old and over: Because of a physical, mental, or emotional condition, do you have difficulty doing errands alone such as visiting a doctor’s office or shopping? | N | Y |
| DD: HHS Surveillance Definition | ||
| ADHD (current and ever) | Y | Y |
| Autism Spectrum Disorder (current and ever) | Y | Y |
| Blindness (current and ever) | Y | Y |
| Cerebral Palsy (current and ever) | Y | Y |
| Intellectual Disability (current and ever) | Y | Y |
| Learning Disability (current and ever) | Y | Y |
| Moderate to profound hearing loss (current and ever) | Y | Y |
| Seizures (current and ever) | Y | Y |
| Stuttering or stammering (current and ever) | Y | Y |
| Other developmental delay (current and ever) | Y | Y |
| DD: Developmental Disabilities Assistance and Bill of Rights Act of 2000 | ||
| Self-care | N | Yc |
| Receptive and expressive language | N | N |
| Learning | Yd | Y |
| Mobility | Y | Yc |
| Self-direction | N | N |
| Capacity for independent living | N | N |
| Economic self-sufficiency | N | N |
| DD: DSM-5 Neurodevelopmental Disorder | ||
| Intellectual disability (current and ever) | Y | Y |
| Communication disorders (language, speech sound, stuttering) (current and ever) | Y | Y |
| Autism Spectrum Disorder (current and ever) | Yd | Y |
| ADHD/ADD (current and ever) | Ye | Y |
| Tic disorders (current and ever) | N | Y |
| Learning disorder (current and ever) | Yd | Y |
| Under 5 years old: Global Developmental Delay (current and ever) | Y | Y |
Abbreviations: ADHD = attention deficit/hyperactivity disorder, ADD = attention deficit disorder, DSM = Diagnostic and Statistical Manual of Mental Disorders, DD = developmental disability, HHS=U.S. Department of Health and Human Services, NHIS=National Health Interview Survey, NSCH=National Survey of Children’s Health.
The WG-SS is a standardized question set that was not included in the surveys for sample children during the years included in this analysis. For this analysis we selected variables that were best available approximations for the published Washington Group questions. In both surveys, most questions used for the Washington Group Short Set on Functioning (WG-SS) definition were not asked with severity scale answer choices as the Washington Group had intended. Only the hearing variable in NHIS had a severity scale to choose from, but it offered six answer choices instead of the four choices published by the Washington group.
The ACS-6 is a standardized question set that was not included in the surveys for sample children during the years included in this analysis. For this analysis we selected variables that were best available approximations for the published ACS-6 questions.
These questions in NSCH were only asked of children ages 6–17.
These questions in NHIS were only asked of children ages 3–17.
These questions in NHIS were only asked of children ages 2–17.
The WG-SS refers to a specific list of questions and answer choices, but neither survey asked the exact questions comprising the WG-SS during 2016–2018. Questions with the closest meaning to the official WG-SS were used to approximate this definition The WG-SS was designed to use answer choices on a severity scale from “no difficulty” to “cannot do at all”; however, most variables in both surveys only had “yes” or “no” answer choices. If at least one of the six questions were answered with a “yes”, the participant was considered to have met the WG-SS definition.
2.2. American community survey question set (ACS-6)
Like the WG-SS, the ACS developed a set of six questions to identify individuals meeting a functional definition of disability. This question set can be used to define disability for all ages, though some components are only asked of people in certain age groups (Table 1).12 The ACS-6 refers to a standard list of questions and answer choices, but NHIS did not administer this question set in the sample child section in the years 2016–2018. NHIS included the ACS-6 in a different section of the survey referring to the entire family, so those questions could not be used in calculating prevalence in this analysis because responses could not be definitively linked with the sample child. Variables with the closest meaning to the official ACS-6 questions were selected to represent the components of the ACS-6 definition in NHIS. If at least one of the questions was answered with a “yes”, the participant was considered to have met the ACS-6 definition.
2.3. HHS surveillance definition
Recent HHS surveillance reports use a diagnosis-based definition of DD in prevalence estimates from NHIS.13–15 This definition of DD is based on parental report of diagnosis of one or more of the following conditions: attention-deficit/hyperactivity disorder (ADHD), ASD, blindness, cerebral palsy, intellectual disability, learning disability, moderate to profound hearing loss, seizures, stuttering or stammering, and other developmental delay. For these prevalence estimates, only children ages three through 17 years are included based on the survey methodology.
Two definitions using the HHS surveillance framework were created, one using “ever diagnosed with” and the other using “currently diagnosed with”; the surveys asked both “ever” and “current” questions about most components of the definition. In some instances, only “ever” or “current” was asked of a definition component, but not both. In these cases, we used the available question for both “ever” and “current” prevalence estimates.
2.4. Developmental Disabilities Assistance and bill of Rights Act of 2000 (DD act)
The Developmental Disabilities Assistance and Bill of Rights Act of 2000 (DD Act) was written to ensure “that individuals with developmental disabilities and their families participate in the design of and have access to needed community services, individualized supports, and other forms of assistance …”.2 This legislation’s definition of DD is used by many states’ DD councils and other federal and state entities. The DD Act specifies that a person must meet at least 3 areas of significant functional impairment; these impairments must manifest “before age 22” and be “likely to continue indefinitely”. The DD Act definition had the fewest components that matched with variables in the surveys (Table 1).
2.5. DSM-5 neurodevelopmental disorder
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published in 2013, identifies a category of diagnoses called “neurodevelopmental disorders” (NDDs).3 These diagnoses specify an onset of one or more of the following conditions during the developmental period: intellectual disability, communication disorders, autism spectrum disorder, ADHD and attention-deficit disorder (ADD), tic disorders, learning disorders, and global developmental delay (under age 5 years). As was done for the HHS Surveillance definition, we also estimated prevalence of both “ever” and “current” diagnosis of the conditions.
2.6. Data sources and analysis
We determined that NHIS and NSCH had sufficient data to at least partially calculate prevalence estimates based on each of the selected definitions. Appendix Table 1 shows the NHIS and NSCH survey questions and corresponding variables that were matched to each component of the selected definitions. Data from NHANES and ACS were not analyzed because they did not include questions about some specific diagnoses, including ASD and intellectual disability.
NHIS is a cross-sectional household interview survey designed to be representative of the U.S. non-institutionalized, civilian population and uses a complex sampling plan, which is redesigned after each decennial census.17–20 Data is collected by the U.S. Census Bureau on behalf of the National Center on Health Statistics at the Centers for Disease Control and Prevention. Data is collected via computer-assisted in person interviews at respondents’ homes, with the potential for follow-up by phone if needed. The sampling design is based on clusters of addresses within a defined geographic area. Weights were used in all analyses to account for sampling and participation, and design pseudo-variables (stratum and primary sampling unit with appropriate masking to preserve confidentiality) were used in variance estimation, per NHIS analytical guidelines.
NSCH is a cross-sectional household interview survey designed to be representative of the U.S. non-institutionalized population of children ages 0–17 and uses a complex sampling plan, oversampling young children and children with special health care needs.21–23 One child per household is selected and the respondent is a knowledgeable parent or guardian of the sample child. Since 2016, the NSCH has been conducted by the U.S. Census Bureau on behalf of the Maternal and Child Health Bureau (MCHB), Health Resources and Services Administration (HRSA), and Department of Health and Human Services. Data are collected through self-administered web-based or paper questionnaires. Weights were used in all analyses to account for sampling and participation, and design pseudo-variables were used in variance estimation.
All children 0–17 years were included in the analytic sample, unless limited by the definition or the availability of data. Children missing the minimum information needed to meet a definition were excluded from that prevalence estimate. If a variable was restricted to a certain age range, children outside of that range were counted as negative (i.e., not having that condition). To be classified as not meeting the given disability definition, all variables contributing to the definition had to be non-missing and negative. We analyzed data from the same time period (2016–2018) for comparability across surveys. We chose not to use data from more recent survey years, since NHIS underwent a redesign in 2019 that removed relevant DD diagnoses questions (stuttering/stammering, seizures, cerebral palsy) present in previous years. The earliest annual NSCH survey year was 2016; previously this survey was done sporadically.
During 2016–2018, the NHIS and NSCH response rates were 59.2%–61.9% and 37.4%–43.1%, respectively. The datasets for all children 0–17 years from NHIS included 28,221 participants and from NSCH included 102,341 participants. Children excluded from one prevalence estimate due to missing data or limitations with the definition could be included in other prevalence estimates.
We used R version 1.4.1106 with package srvyr to use survey clustering, stratification, and sampling weights to generate nationally representative prevalence of DD.24 The percentage of children meeting each definition in each survey and accompanying 95% confidence intervals were estimated. We determined a subset of the definitions that most completely matched with available data and assessed potential differences in the distribution of age group, sex, and race/ethnicity across definitions. We also created a Euler plot to visualize the overlap of children in each of these four definition categories.25
3. Results
The estimated prevalence of developmental disabilities varied depending on both the definition and data source used (Table 2). The definition with the lowest prevalence estimates for both surveys was the DD Act, for which a prevalence of approximately one percent was estimated for meeting two or more components (NHIS: 0.6%, NSCH: 1.1%). The highest prevalence estimate for both surveys was the HHS surveillance definition applied to three-to 17-year-olds, when the component conditions were defined based on “ever” having received a diagnosis (NHIS: 18.0%, NSCH: 22.2%). Although statistically significantly different based on non-overlapping confidence intervals, the estimates using a current diagnosis and having ever been diagnosed with one or more conditions included in the HHS surveillance or DSM-5 definitions were similar in magnitude, relative to prevalence estimates based on other definitions.
Table 2.
Prevalence of disability and developmental disability based on available data from select national surveys.
| Definition | NHIS prevalence % (95% CI) | NSCH prevalence % (95% CI) |
|---|---|---|
|
| ||
| Disability: WG-SS a | 6.3 (5.9–6.7) | 11.9 (11.4–12.5) |
| Disability: ACS b | 5.2 (4.9–5.5) | 9.2 (8.8–9.6) |
| DD: HHS surveillancec, ever | 18.0 (17.3–18.7) | 22.2 (21.6–22.9) |
| DD: HHS surveillancec, current | 16.0 (15.4–16.6) | 18.8 (18.2–19.4) |
| DD: DD Actd, at least 1 component | 7.8 (7.4–8.3) | 7.2 (6.8–7.6) |
| DD: DD Actd, at least 2 components | 0.6 (0.5–0.7) | 1.1 (0.9–1.3) |
| DD: DD Actd, at least 3 components | N/Ae | 0.2 (0.2–0.3) |
| DD: DSM-5f, ever | 14.1 (13.5–14.6) | 17.2 (16.7–17.7) |
| DD: DSM-5f, current | 12.8 (12.3–13.3) | 14.4 (13.9–14.9) |
Abbreviations: WG-SS= Washington Group Short Set on Functioning, ACS=American Community Survey, DD = developmental disability, DSM = Diagnostic and Statistical Manual of Mental Disorders; HHS=U.S. Department of Health and Human Services, NHIS=National Health Interview Survey, NSCH=National Survey of Children’s Health.
Washington Group Short Set on Functioning, ages 5–17.
ACS-6 Question Set, ages 0–17.
Surveillance definition used in HHS surveillance reports, ages 3–17.
Developmental Disabilities Assistance and Bill of Rights Act of 2000, ages 0–17.
Not available because NHIS survey only contained two components of the DD Act definition.
Definition of neurodevelopmental disabilities in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), ages 0–17.
For all definitions except “DD Act, at least one component”, prevalence estimates from NSCH were higher than from NHIS, as would be expected given that there were more variables in NSCH corresponding to the definition components than in NHIS. The biggest difference between surveys was seen for the WG-SS and ACS-6 disability definitions, with NSCH estimates at least 4% points higher than NHIS for both definitions (percentage point difference: WG-SS = 5.6, ACS = 4.0).
Of the four definitions with NSCH data matching the criteria (WG-SS, ACS-6, HHS current, and DSM-5 current), WG-SS and ACS-6 identified lower proportions of younger children than the HHS and DSM-5 definitions. The HHS and DSM-5 definitions had higher proportions of male and white children than WG-SS and ACS-6 (Table 3). Of children that met at least one of the four definitions in NSCH, the greatest overlap between definitions was HHS and DSM, followed by a combination of all four definitions (42.1% and 33.2%, respectively) (Fig. 1).
Table 3.
Demographic information of children meeting disability and developmental disability definitions, NSCH, 2016–2018.
| Characteristics | Disability: WG-SSa, ages 5–17 | Disability: ACS-6b, ages 0–17 | DD: HHSc, ages 3–17, current | DD: DSM-5d, ages 0–17, current |
|---|---|---|---|---|
|
| ||||
| Age (years) | ||||
| 0–5 | 2.2 (1.5–2.9) | 6.4 (5.0–7.7) | 14.0 (12.7–15.3) | 17.8 (16.3–19.3) |
| 6–11 | 48.0 (45.5–50.5) | 45.3 (42.9–47.7) | 42.7 (40.9–44.4) | 40.9 (39.0–42.7) |
| 12–17 | 49.8 (47.3–52.2) | 48.3 (45.9–50.7) | 43.3 (41.6–45.1) | 41.3 (39.5–43.1) |
| Sex | ||||
| Male | 59.2 (56.7–61.7) | 58.8 (56.4–61.3) | 63.7 (61.9–65.4) | 66.5 (64.8–68.3) |
| Female | 40.8 (38.3–43.3) | 41.2 (38.7–43.6) | 36.3 (34.6–38.1) | 33.5 (31.7–35.2) |
| Race & Ethnicity | ||||
| White, non-Hispanic | 47.0 (44.6–49.3) | 47.0 (44.7–49.3) | 51.7 (49.9–53.5) | 52.9 (51.0–54.7) |
| Black, non-Hispanic | 17.1 (15.1–19.0) | 17.0 (15.1–18.9) | 15.4 (14.0–16.8) | 15.6 (14.1–17.1) |
| Hispanic | 27.7 (25.1–30.4) | 27.7 (25.1–30.3) | 24.9 (23.0–26.9) | 23.6 (21.5–25.6) |
| Other, non-Hispanic | 8.2 (7.2–9.2) | 8.3 (7.3–9.3) | 8.0 (7.2–8.8) | 8.0 (7.2–8.8) |
Abbreviations: WG-SS= Washington Group Short Set on Functioning, ACS=American Community Survey, DD = developmental disability, DSM = Diagnostic and Statistical Manual of Mental Disorders, HHS=U.S. Department of Health and Human Services, NSCH=National Survey of Children’s Health.
Washington Group Short Set on Functioning.
ACS-6 Question Set.
Surveillance definition used in HHS surveillance reports.
Definition of neurodevelopmental disabilities in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Fig. 1.
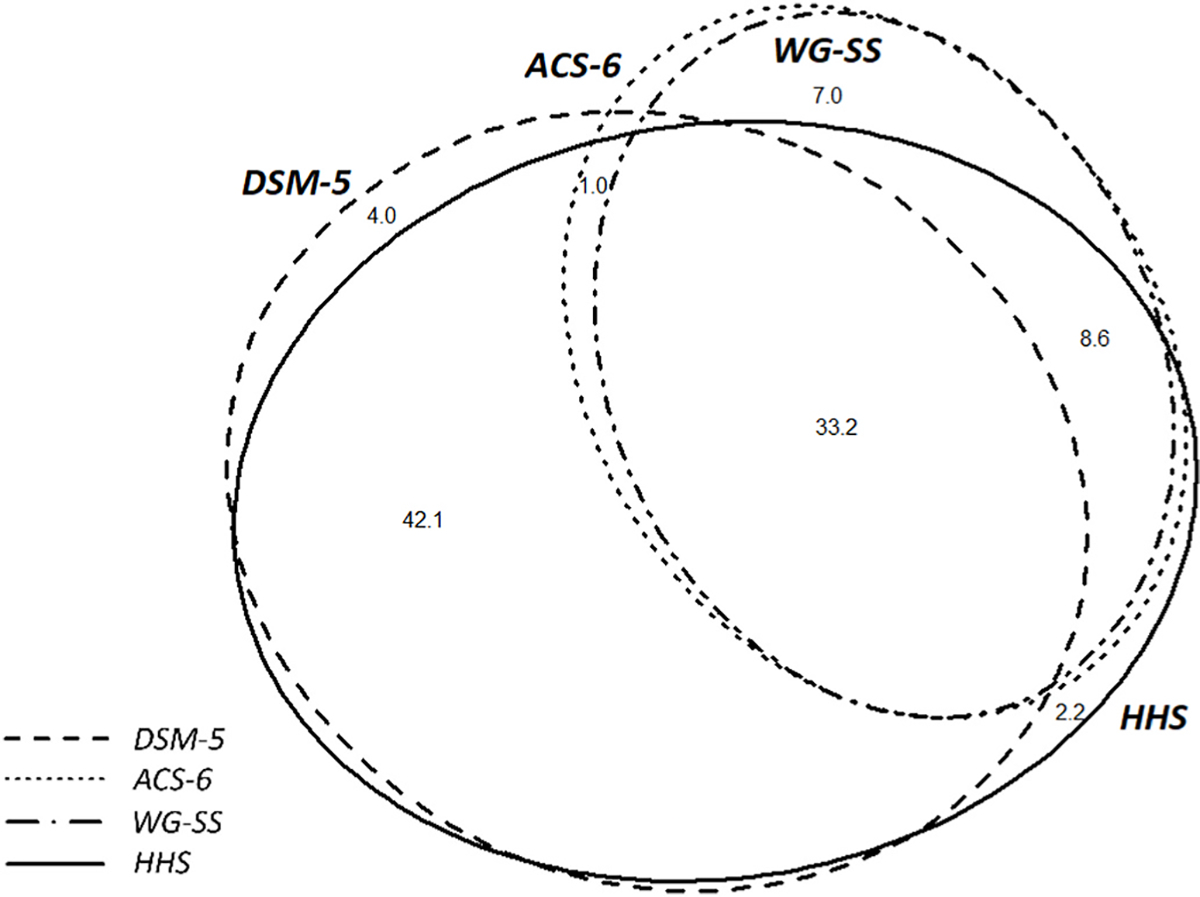
Percent of overlap across disability and developmental disability definitions among U.S. children meeting at least one definition: WG-SS*, ACS-6†, HHS‡ (current), DSM-5§ (current), NSCH, 2016–2018.
Abbreviations: ACS=American Community Survey, WG-SS= Washington Group Short Set on Functioning, DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, HHS=U.S. Department of Health and Human Services, NSCH=National Survey of Children’s Health.
Rates less than 1% were not included in this diagram.
* Washington Group Short Set on Functioning measuring disability, ages 5–17.
† ACS-6 Question Set measuring disability, ages 0–17.
‡ Surveillance definition used in HHS surveillance reports measuring developmental disability, ages 3–17.
§ Definition of neurodevelopmental disabilities in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), measuring developmental disability, ages 0–17.
4. Discussion
Prevalence of DD varied both across each definition and between the two national surveys. General disability definitions in both surveys had lower prevalence than most DD definitions and NSCH prevalence estimates were higher than NHIS. One likely reason for this inconsistency is that different numbers of components of existing definitions are captured by existing variables on the NHIS and NSCH. The WG-SS and ACS-6 question sets have been criticized for not including people with intellectual and developmental disabilities, and, although less impactful for children’s disability prevalence, people with psychiatric- or chronic condition-associated disability.26 Another explanation for variation across definitions is that not every person with a diagnosed DD (HHS and DSM-5 definitions) would necessarily have functional limitations as defined by WG-SS, ACS-6, and DD Act definitions. The reverse may also be true, in that a diagnosis-based definition is unlikely to capture everyone experiencing functional limitations. Additionally, the surveys do not capture the level of supports and intensity of functional limitations or the role of treatment and other accommodations in preventing functional limitations in those with diagnosed conditions who would otherwise experience them. Moreover, some definitions could only be applied to older children. While some of these definitions of DD may have utility in policy or service eligibility, they are not captured well in national surveys, making it challenging to plan for service needs.
The WG-SS uses a functional framework to approximate rates of disability from national censuses and surveys. The difference in prevalence between NHIS (6.3%) and NSCH (11.9%) may be due in part to the difference in definition components represented. Three of the six components were not available in the years included in this analysis in NHIS, while only one was not available in NSCH. This question set does not allow specification of whether the functional limitation experienced is due to a developmental-related impairment. The lack of age of onset is less relevant when examining data on children given that the functional limitations are being measured during the child or adolescent period and likely represent a DD; however, the WG-SS in its current state cannot specifically measure DD among adults, it is a useful reference point and an example of how to operationalize a functional framework.
The ACS-6 questions operate similarly to the WG-SS in that they also allow measures of functioning to be used to estimate rates of disability in national surveys. Three of the six components were not available in the sample child section in NHIS, while the definition was fully represented in NSCH. Again, the difference in prevalence in NHIS (5.2%) and NSCH (9.2%) may be explained by the missing components of the definition in the NHIS.
The HHS surveillance definition is used to report the prevalence of DD by using diagnoses that are commonly categorized as DDs. All components of the definition were present in both surveys. Those that meet the HHS definition are considered to have a DD, though whether the child is experiencing specific functional limitations due to their diagnosis is not captured by this definition. Although the estimates for ever having been diagnosed with a DD condition versus currently having the condition were similar in magnitude, the absolute differences (2.0% and 3.4% for NHIS and NSCH, respectively) translate to thousands of children in the U.S., and therefore it is important to consider the impact of excluding children who do not currently have a diagnosis from prevalence estimates. Families with lower socioeconomic status or from poorer school districts may not have access to resources including health care to obtain diagnoses, which may account for some of the greater prevalence of white children in the HHS and DSM-5 definitions (Table 3).27
The DD Act is the only functional-based definition specific to DD examined. While the definition used in the DD Act is useful from a policy perspective (e.g., provides a broad definition of people who can receive services from state programs that the DD Act authorizes such as family support programs, and state protection and advocacy systems),6 it has limitations for quantifying public health data. First, only two and three of the seven definition components are met in NHIS and NSCH, respectively. Second, many of the components are not sufficiently specific for operationalizing in surveys. For example, the component “self-direction” is not further explained elsewhere in the legislation and is open to different interpretations. Finally, many components are not relevant across all age groups. For example, economic self-sufficiency and independent living are not applicable markers of development for young children. Because of how few definition components were represented in the surveys, we measured the prevalence of at least one, two, and three components of the DD Act definition met. The “at least three” DD Act definition was the lowest prevalence reported at 0.2% (95% CI: 0.2%, 0.3%) in NSCH. However, as noted above, even this small estimate represents thousands of children in the United States. In addition, the lack of survey questions aligning with the DD Act definition shows a significant gap in tools for evaluating the need and use of this important DD legislation. Even more so for adults with DD, the DD Act definition is important in defining eligibility to essential services and supports and having better population-based estimates of individuals meeting the various components of the definition would be an important tool for State and local policy and service organizations. Future work should evaluate the possibilities for operationalizing the DD Act in public health surveillance.
The DSM-5 is a tool for qualified health professionals to diagnose mental illnesses.3 By definition, the DSM-5 provides diagnoses-based prevalence estimates, similar to the HHS surveillance definition, although the DSM-5 does not include the “blindness” and “loss of hearing” components that the HHS does. The DSM-5 is considered the standard for diagnosing many DDs and is designed for clinicians to use in diagnosis; it therefore may be appropriate for diagnosis-specific public health surveillance but not other types of public health surveillance needs.
There are several limitations of our analysis. We conducted a targeted review, rather than a systematic review, of DD definitions. There were many elements of each of the definitions that were not available in national surveys, and several definitions were approximated based on available data. For example, the DD Act includes in its definition of DD functional limitations in self-direction, independent living capacity, and economic self-sufficiency, which can be challenging to measure in surveys. In addition, information on children was reported by their parent or other caregiver, which may not always accurately reflect the experience of the child about whom they are reporting (e.g., a parent may not recognize that a child has difficulty concentrating, remembering, or making decisions). We focused only on national survey data and did not assess service or healthcare data. In addition, we considered data from only two national surveys because most surveys did not have DD-related criteria to measure.
These data highlight the importance of understanding how DD is defined, as variation among who is captured by these definitions may have implications for conclusions drawn from the data. Consistent disability data including people with DDs from both functional and diagnostic perspectives are important for efforts to identify, address, and monitor health disparities. As expected, the functional disability measures (ACS-6 and WG-SS) and the diagnosed/identified DD conditions (HHS and DSM-5) definitions were most aligned (Fig. 1). The functional disability definitions were intended to represent limitations in functional domains associated with broader disability and not to measure specific developmental disabilities. They were also less likely to be endorsed at younger ages indicating limited utility for population-based prevalence estimation among young children. The use of reported diagnoses or conditions were specific to developmental disabilities; however, the inclusion or exclusion of specific conditions does not offer a comprehensive picture of all conditions considered to impact a child’s core developmental domains. While reporting diagnosed conditions may provide more robust prevalence estimates, they are more likely to be influenced by identification and diagnostic disparities.
5. Conclusion
The substantial variability in the estimated prevalence of DD among children in the United States depends on both the definition and the data source used. Neither the diagnosis-based nor functional limitation-based definitions meet all needs and available nationally representative surveys are limited in their capacity to collect data that meet all definitions. Future work is needed to better align the population prevalence of specific conditions with the presence of differential functioning in core domains as noted by the DD Act, and to consider the availability and validity of these data across the lifespan. Different measures are needed for different purposes; understanding which aspects of DD should be measured to meet a given need is vital. It is important to clearly establish the goals of data collection and analysis in order to use the correct definitions. Though this issue is complex, deliberately selecting appropriate DD and disability definitions is essential for providing the most useful data possible to inform the needs of an often-overlooked group of people who face significant health inequities.
Appendix
Appendix Table 1.
| Definition components | NHIS variables | NSCH variables |
|---|---|---|
|
| ||
| Disability: Washington Group Short Set on Functioning * | ||
| 5years old and over: Do you have difficulty seeing, even if wearing glasses? | Any trouble seeing even when wearing glasses or contact lenses? (CVISION) | Does child have blindness or problems with seeing, even with glasses? (BLINDNESS) |
| 5 years old and over: Do you have difficulty hearing, even if using a hearing aid? | Which statement best describes hearing without a hearing aid: excellent, good, a little trouble hearing, moderate trouble, a lot of trouble, or deaf? (CHEARST1) | Does child have deafness or problems with hearing? (K2Q43B) |
| 5 years old and over: Do you have difficulty walking or climbing steps? | Impairment or health problem that limits ability to crawl, walk, run, play? (IHMOB) | Does child have serious difficulty walking or climbing stairs? (WALKSTAIRS, ages 6–17) |
| 5 years old and over: Do you have difficulty remembering or concentrating? | n/a | Does child have serious difficulty concentrating, remembering, or making decisions because of a physical, mental, or emotional condition? (MEMORYCOND, ages 6–17) |
| 5 years old and over: Do you have difficulty (with self-care such as) washing all over or dressing? | n/a | Does child have difficulty dressing or bathing? (DRESSING, ages 6–17) |
| 5 years old and over: Using your usual (customary) language, do you have difficulty communicating, for example understanding or being understood? | n/a | n/a |
| Disability: American Community Survey Question Set # | ||
| Are you deaf, or do you have serious difficulty hearing? | Which statement best describes hearing without a hearing aid: excellent, good, a little trouble hearing, moderate trouble, a lot of trouble, or deaf? (CHEARST1) | Does child have deafness or problems with hearing? (K2Q43B) |
| Are you blind, or do you have serious difficulty seeing even when wearing glasses? | Any trouble seeing even when wearing glasses or contact lenses? (CVISION) | Does child have blindness or problems with seeing, even with glasses? (BLINDNESS) |
| 5 years old and over: Because of a physical, mental, or emotional condition, do you have difficulty concentrating, remembering, or making decisions? | n/a | Does child have serious difficulty concentrating, remembering, or making decisions because of a physical, mental, or emotional condition? (MEMORYCOND, ages 6–17) |
| 5 years old and over: Do you have serious difficulty walking or climbing stairs? | Impairment or health problem that limits ability to crawl, walk, run, play? (IHMOB) | Does child have serious difficulty walking or climbing stairs? (WALKSTAIRS, ages 6–17) |
| 5 years old and over: Do you have difficulty dressing or bathing? | n/a | Does child have difficulty dressing or bathing? (DRESSING, ages 6–17) |
| 15 years old and over: Because of a physical, mental, or emotional condition, do you have difficulty doing errands alone such as visiting a doctor’s office or shopping? | n/a | Does child have difficulty doing errands alone such as visiting a doctor’s office or shopping, because of a physical, mental, or emotional condition? (ERRANDALONE) |
| DD: HHS Surveillance Definition | ||
| ADHD |
Ever: Has doctor or health professional ever told you that child had ADHD/ADD? (ADD2) Current: Does child currently have ADHD/ADD? (ADD2N) |
Ever: Has a doctor or health care provider ever told you that child has ADHD/ADD? (K2Q31A) Current: Does the child currently have ADHD/ADD? (K2Q31B) |
| Autism Spectrum Disorder |
Ever: Has a doctor or health professional ever told you that child had Autism, Asperger’s, pervasive developmental disorder, or autism spectrum disorder? (AUTISM) Current: Does child currently have Autism, Asperger’s, pervasive developmental disorder, or autism spectrum disorder? (AUTISMN) |
Ever: Has a doctor or health care provider ever told you that child has Autism or Autism Spectrum Disorder? (K2Q35A) Current: Does the child currently have Autism? (K2Q35B) |
| Blindness | Ever, Current: Is child blind or unable to see at all? (CBLIND) | Ever, Current: Does child have blindness or problems with seeing, even with glasses? (BLINDNESS) |
| Cerebral Palsy | Ever, Current: Has a doctor or health professional ever told you that child had Cerebral Palsy? (CCONDRR2) |
Ever: Has a doctor or health care provider ever told you that child has Cerebral Palsy? (K2Q61A) Current: Does the child currently have Cerebral Palsy? (K2Q61B) |
| Intellectual Disability |
Ever: Has a doctor or health professional ever told you that child had an intellectual disability? (AMR2R) Current: Does the child currently have an intellectual disability? (AMR2RN) |
Ever: Has a doctor, health care provider, or educator ever told you that child has intellectual disability? (K2Q60A) Current: Does the child currently have intellectual disability? (K2Q60B) |
| Learning Disability | Ever, Current: Has a representative from a school or a health professional ever told you that child had a learning disability? (LEARND) |
Ever: Has a doctor, health care provider, or educator ever told you that child has a learning disability? (K2Q30A) Current: Does the child currently have a learning disability? (K2Q30B) |
| Moderate to profound hearing loss | Ever, Current: Which statement best describes child’s hearing without hearing aid? (CHEARST1) | Ever, Current: Does the child have deafness or problems with hearing? (K2Q43B) |
| Seizures | Ever, Current: During the past 12 months, has child had seizures? (SEIZE2) |
Ever: Has a doctor or health care provider ever told you that child has epilepsy or seizure disorder? (K2Q42A) Current: Does the child currently have epilepsy or seizure disorder? (K2Q42B) |
| Stuttering or Stammering | Ever, Current: During the past 12 months, has child had stuttering or stammering? (STUTTER) |
Ever: Has a doctor, health care provider, or educator ever told you that child has a speech or other language disorder? (K2Q37A) Current: Does the child currently have a speech disorder? (K2Q37B) |
| Other developmental delay |
Ever: Has a doctor or health professional ever told you that child had any other developmental delay? (AODD2) Current: Does child currently have any other developmental delay? (AODD2N) |
Ever: Has a doctor, health care provider, or educator ever told you that the child has developmental delay? (K2Q36A) Current: Does the child currently have developmental delay? (K2Q36B) |
| DD: Developmental Disabilities Assistance and Bill of Rights Act of 2000 | ||
| Self-care | n/a | Does child have difficulty dressing or bathing? (DRESSING, ages 6–17) |
| Receptive and expressive language | n/a | n/a |
| Learning | Has a representative from a school or a health professional ever told you that child had a learning disability? (LEARND, ages 3–17) | Has a doctor, health care provider, or educator ever told you that child has a learning disability? (K2Q30A) |
| Mobility | Impairment or health problem that limits ability to crawl, walk, run, play? (IHMOB) | Does child have serious difficulty walking or climbing stairs? (WALKSTAIRS, ages 6–17) |
| Self-direction | n/a | n/a |
| Capacity for independent living | n/a | n/a |
| Economic self-sufficiency | n/a | n/a |
| DD: DSM-5 | ||
| Intellectual disability |
Ever: Has a doctor or health professional ever told you that child had an intellectual disability? (AMR1R, AMR2R) Current: Does child currently have an intellectual disability? (AMR1RN, AMR2RN) |
Ever: Has a doctor, health care provider, or educator ever told you that child has intellectual disability? (K2Q60A) Current: Does the child currently have intellectual disability? (K2Q60B) |
| Communication disorders (language, speech sound, stuttering) | Ever, Current: During the past 12 months, has child had stuttering or stammering? (STUTTER, ages 3–17) |
Ever: Has a doctor, health care provider, or educator ever told you that child has a speech or other language disorder? (K2Q37A) Current: Does the child currently have a speech disorder? (K2Q37B) |
| Autism Spectrum Disorder |
Ever: Has a doctor or health professional ever told you that child had Autism, Asperger’s, pervasive developmental disorder, or autism spectrum disorder? (AUTISM, ages 2–17) Current: Does child currently have Autism, Asperger’s, pervasive developmental disorder, or autism spectrum disorder? (AUTISMN, ages 2–17) |
Ever: Has a doctor or health care provider ever told you that child has Autism or Autism Spectrum Disorder? (K2Q35A) Current: Does the child currently have Autism? (K2Q35B) |
| ADHD/ADD |
Ever: Has doctor or health professional ever told you that child had ADHD/ADD? (ADD2, ages 2–17) Current: Does child currently have ADHD/ADD? (ADD2N, ages 2–17) |
Ever: Has a doctor or health care provider ever told you that child has ADHD/ADD? (K2Q31A) Current: Does the child currently have ADHD/ADD? (K2Q31B) |
| Tic disorders | n/a |
Ever: Has a doctor or health care provider ever told you that child has Tourette Syndrome?” (K2Q38A) Current: Does the child currently have Tourette Syndrome? (K2Q38B) |
| Learning disorder | Ever, Current: Has a representative from a school or a health professional ever told you that child had a learning disability? (LEARND, ages 3–17) |
Ever: Has a doctor, health care provider, or educator ever told you that child has a learning disability? (K2Q30A) Current: Does the child currently have a learning disability? (K2Q30B) |
| Under 5 years old: Global Developmental Delay |
Ever: Has a doctor or health professional ever told you that child had any other developmental delay? (AODD1, AODD2) Current: Does child currently have any other developmental delay? (AODD1N, AODD2N) |
Ever: Has a doctor, health care provider, or educator ever told you that the child has developmental delay? (K2Q36A) Current: Does the child currently have developmental delay? (K2Q36B) |
Abbreviations: ADHD = Attention deficit/hyperactivity disorder, ADD = Attention deficit disorder, DD = developmental disability.
The WG-SS is a standardized question set that was not included in the surveys for sample children during the years included in this analysis. For this analysis we selected variables that were best available approximations for the published Washington Group questions.
The ACS-6 is a standardized question set that was not included in the surveys for sample children during the years included in this analysis. For this analysis we selected variables that were best available approximations for the published ACS-6 questions.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. This research was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and CDC (for Lauren Russell).
References
- 1.Anderson LL, Larson SA, MapelLentz S, Hall-Lande J. A systematic review of U.S. Studies on the prevalence of intellectual or developmental disabilities since 2000. Intellect Dev Disabil. 2019;57(5):421–438. [DOI] [PubMed] [Google Scholar]
- 2.The developmental disabilities assistance and Bill of Rights Act of 2000. U.S.C. §. 2000;42, 15001. [Google Scholar]
- 3.Diagnostic and Statistical Manual of Mental Disorders. fifth ed. American Psychiatric Association;2013. [Google Scholar]
- 4.Accardo P, Whitman B. Dictionary of Developmental Disabilities Terminology. third ed. Brookes Publishing Company;2011. [Google Scholar]
- 5.McKenzie K, Milton M, Smith G, Ouellette-Kuntz H. Systemic review of the prevalence and incidence of intellectual disabilities: current trends and issues. Current Developmental Disorders Reports. 2016;3:104–115. [Google Scholar]
- 6.Altman BM. Definitions, concepts, and measures of disability. Ann Epidemiol. 2014;24(1):2–7. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. International Classification of Functioning, Disability, and Health. Geneva, Switzerland: World Health Organization;2001. [Google Scholar]
- 8.Individuals with Disabilities Education Act, 20 U.S.C. § 1400. 2004. [Google Scholar]
- 9.Crocker A, Rubin L. Developmental Disabilities: Delivery of Medical Care for Children and Adults. Lea & Febiger; 1989. [Google Scholar]
- 10.Hagerman TK, Houtrow A. Variability in prevalence estimates of disability among children in the national survey of children’s health. JAMA Pediatr. 2021;175(3):307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.The Washington Group on Disability Statistics. The Washington Group Short Set on Functioning. WG-SS);2022. https://www.washingtongroup-disability.com/fileadmin/uploads/wg/Documents/Questions/Washington_Group_Questionnaire__1_-_WG_Short_Set_on_Functioning.pdf.
- 12.United States Census Bureau. How Disability Data Are Collected from the American Community Survey;2021. https://www.census.gov/topics/health/disability/guidance/data-collection-acs.html.
- 13.Cogswell M, Coil E, Tian LH, et al. Health needs and use of services among children with developmental disabilities- United States, 2014–2018. MMWR (Morb Mortal Wkly Rep). 2022;71(12):453–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Boulet SL, Boyle CA, Schieve LA. Health care use and health and functional impact of developmental disabilities among US children. Arch Pediatr Adolesc Med. 2009;163(1):19–26, 1997–2005. [DOI] [PubMed] [Google Scholar]
- 15.Zablotsky B, Black LI, Maenner MJ, et al. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics. 2019;144(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.The Washington Group on Disability Statistics. WG/UNICEF Child Functioning Module (CFM);2020. https://www.washingtongroup-disability.com/question-sets/wg-unicef-child-functioning-module-cfm/.2023.
- 17.CDC - National Center for Health Statistics. About the National Health Interview Survey. https://www.cdc.gov/nchs/nhis/about_nhis.htm#sample_design.2023.
- 18.CDC - National Center for Health Statistics National Health Interview Survey. Public-use Data File and Documentation; 2016. https://www.cdc.gov/nchs/nhis/1997-2018.htm.2023.
- 19.CDC - National Center for Health Statistics National Health Interview Survey. Public-use Data File and Documentation;2017. https://www.cdc.gov/nchs/nhis/1997-2018.htm.2023.
- 20.CDC - National Center for Health Statistics National Health Interview Survey. Public-use Data File and Documentation;2018. https://www.cdc.gov/nchs/nhis/1997-2018.htm.2023.
- 21.The United States Census Bureau. 2016 National Survey of Children’s Health Methodology Report. Public-use data file and documentation;2016. https://www.census.gov/content/dam/Census/programs-surveys/nsch/tech-documentation/methodology/2016-NSCH-Methodology-Report.pdf.2023.
- 22.The United States Census Bureau. 2017 National Survey of Children’s Health Methodology Report. Public-use data file and documentation;2017. https://www.census.gov/content/dam/Census/programs-surveys/nsch/tech-documentation/methodology/2017-NSCH-Methodology-Report.pdf.2023.
- 23.The United States Census Bureau. 2018 National Survey of Children’s Health Methodology Report. Public-use data file and documentation;2018. https://www2.census.gov/programs-surveys/nsch/technical-documentation/methodology/2018-NSCH-Methodology-Report.pdf.2023.
- 24.Freedman Ellis G, Schneider B. Srvyr: ‘dplyr’ -Like Syntax for Summary Statistics of Survey Data. 2022. R package version 1.1.2. [Google Scholar]
- 25.Larsson J _eulerr: Area-Proportional Euler and Venn Diagrams with Ellipses. R Package;2022. version 7.0.0. [Google Scholar]
- 26.Hall JP, Kurth NK, Ipsen C, Myers A, Goddard K. Comparing measures of functional difficulty with self-identified disability: implications for health policy. Health Aff. 2022;41(10):1433–1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Blumberg SJ, Zablotsky B, Avila RM, Colpe LJ, Pringle BA, Kogan MD. Diagnosis lost: differences between children who had and who currently have an autism spectrum disorder diagnosis. Autism. 2016. Oct;20(7):783–795. [DOI] [PMC free article] [PubMed] [Google Scholar]