

Abstract
Introduction:
The federal Child and Adult Care Food Program (CACFP) improves nutrition and reduces food insecurity among young children by helping cover the food costs for child care providers and families. This nationwide study evaluated the extent and predictors of the CACFP’s utilization among licensed child care centers to identify opportunities for expanding CACFP nutrition support.
Methods:
Administrative data from the CACFP and child care licensing agencies in 47 states and District of Columbia were compiled and geocoded for 93,227 licensed child care centers. CACFP participation was predicted using a multivariable Bayesian spatial logistic regression model in the sample of low-income areas to target CACFP eligible child care centers. Data were collected in 2020–2021 and analyzed in 2022.
Results:
Of all licensed child care centers, 36.5% participated in the CACFP, ranging from 15.2% to 65.3% across states; when restricted to low-income areas, 57.5% participated (range, 15.7%−85.7%). Income differences did not explain the large variation in CACFP participation rates across states. Having at least three CACFP sponsoring agencies per state predicted a 38% higher probability of CACFP participation (OR=1.38; 95% Credible Interval=1.08–1.78).
Conclusions:
Currently CACFP participation rates among licensed child care centers point to program underutilization and unequal access, particularly in some states and regions. Work at the federal and state levels is warranted to expand participation in the program, above all in low-income areas, so that more young children could eat healthfully with the CACFP.
INTRODUCTION
Healthy eating among young children is a promising chronic disease prevention strategy as habits formed in early life often persist during adulthood.1,2 Most young American children do not meet dietary recommendations, with diets high in added sugars, sodium, and saturated fat but low in fiber.3,4 Child care providers, such as child care centers and family daycare homes, can shape young children’s eating habits through the meals and snacks served and the use of appropriate feeding practices.5,6 In the U.S., most young children regularly receive nonparental care,7 making food consumption outside of the home a major target for improving the diets of millions of children.
The Child and Adult Care Food Program (CACFP) is 1 of the 15 federal nutrition assistance programs meant to reduce the food insecurity and improve nutrition. CACFP provided reimbursements for meals and snacks served to participating child care centers, family daycare homes, emergency shelters, after-school programs, and adult daycare centers, reaching 4.58 million individuals in fiscal year (FY) 2022.8 Foods and beverages served must meet specific nutrition standards to get reimbursed, and providers should complete regular training. Targeting benefits to children at risk for food insecurity, CACFP reimburses the child care centers on the basis of the attending children’s household income.9
Although decisions to participate in CACFP are made by care providers, the primary beneficiaries are young children and their families. Through CACFP, children receive nutritious meals and snacks that comply with the CACFP meal patterns aligned with the dietary guidelines for Americans.9 Previous research suggests that CACFP-participating programs often serve more whole grains, vegetables, and milk than nonparticipating programs, and children may have healthier dietary intake when consuming CACFP meals than intake at home or at nonparticipating programs; CACFP may also reduce the prevalence of food insecurity among young children.10–18 CACFP reimbursements also help offset food costs for providers and families. Despite its multiple advantages, CACFP is not used by many eligible child care providers.10
Because participation in nutrition assistance programs is associated with reduced food insecurity and improved nutrition,18–20 it is an important policy goal that all eligible providers and children can access program resources. The U.S. Department of Agriculture (USDA) routinely estimates participation among eligible populations for its larger programs, such as the Supplemental Nutrition Assistance Program (SNAP), with SNAP participation rates varying across states from 56% to 100%.21 Although USDA tracks the number of meals served and daily attendance for CACFP, and state CACFP agencies track individual programs’ compliance with program requirements, no existing system tracks participation among eligible programs. Understanding where and how CACFP is utilized helps point toward an effective strategy to increase CACFP uptake and improve child nutrition.
This study evaluates the rates and predictors of CACFP participation among licensed child care centers across the U.S. to help inform targeted efforts that expand this important program to more children in need. Administrative data from 47 states and the District of Columbia (DC) were collected to (1) estimate CACFP participation rates among licensed child care centers in each state, overall, and in low-income communities, and (2) explore predictors of center-level CACFP participation using Bayesian spatial models. The study hypothesizes that centers located in states with more resources for CACFP and food security in general—measured by the availability of more sponsoring agencies, having licensing and CACFP administered by a single state agency, greater state SNAP participation rates, and having user-friendly agency websites—are more likely to participate in CACFP. In sensitivity analyses, larger centers are expected to have a higher probability of CACFP participation owing to economies of scale.
METHODS
Study Sample
This cross-sectional study compiled data on CACFP-participating and licensed child care centers from 77 state agencies in 47 states and DC. Data was requested from agencies overseeing child care licensing and/or CACFP for centers serving children aged 0–5 years (excluding camps and programs serving only school-age children). When publicly available, lists were downloaded from state agency websites. Data were collected through 2020 and early 2021, but records were requested for the period before March 2020 to reflect the sector before the coronavirus disease 2019 (COVID-19) disruptions. Licensed child care centers were selected as these centers serve 89% of CACFP child participants,8 and data on daycare homes is limited for privacy concerns. Because of incomplete data or nonresponse, 3 states (Alaska, Montana, and North Carolina) were excluded.
Different state agencies usually oversee child care licensing and CACFP, and typically do not share records or use compatible databases with one another. Therefore, it was necessary to construct estimates from the raw data by collecting various agencies’ records and merging all lists at the center level, with 2 coders verifying merges. Each center’s residential address was geolocated using the geocode address tool in ArcGIS Pro (version 2.6.3, Redlands, CA: Esri Inc)22 and merged with 2019 census data from the American Community Survey 5-year Estimates.23
CACFP eligibility is restricted to centers that are either nonprofit (irrespective of children’s household income) or if they are for-profit, serve children among whom at least 25% qualify for free or reduced-price meals.9 Because the data on centers’ nonprofit status and children’s household income were not available, CACFP eligibility was assessed based on a center location in an under-resourced area (census tracts where household incomes are low from disinvestments in their communities and other structural barriers). These were defined as low-income areas if the median 2019 household income was below $39,461 per year in contiguous states and DC, $49,321 in Alaska, and $45,399 in Hawaii; based on the federal poverty guidelines for a household of 3 people to qualify for reduced-price meals through CACFP in FY 2019–2020.24 Sensitivity analyses used higher income thresholds based on a household of 4 people.
Measures
To calculate the state CACFP participation rate among licensed child care centers serving young children, the number of licensed CACFP-participating centers was divided by the number of licensed child care centers in the state. License-exempt CACFP-participating programs (e.g., centers located on tribal lands, affiliated with the Department of Defense, or public school–based programs) were excluded. The primary outcome variable CACFP participation was coded as yes/no for each center.
Because no information was available on the characteristics of children at each center, sociodemographic characteristics of center locations were used as proxies of children’s household characteristics, including census-tract median household income, percentage of adults with at least a high-school degree, percentage of non-Hispanic White, and percentage of children aged <5 years.
State-level measures were collected from multiple sources and intended to capture institutional support and barriers to CACFP participation. These included the following: (1) the type of state agency overseeing CACFP (department of education, social/human services, public health/health services, early care and education, or agriculture); (2) whether child care licensing and CACFP were overseen by the same state agency to account for potential administrative efficiencies (yes/no); (3) a statewide number of CACFP-sponsoring agencies working with unaffiliated (or independent) centers—they help reduce the program administrative burdens (sponsors for daycare homes only were not counted);25 (4) state’s dominant political affiliation based on the 2020 Presidential election;26 (5) 7 USDA administrative regions;27 (6) state SNAP and Women, Infants, and Children (WIC) participation rates;21,28 and (7) user-friendliness of the CACFP state agency websites measured on a 1–3 scale representing score tertiles to describe the availability and ease of access to information about CACFP.29
Statistical Analysis
To explore predictors of CACFP participation for an average child care center, given the inherent spatial structure in the distribution of child care centers (e.g., urban clusters), this study used a flexible, Bayesian mixed-effects logistic regression model with a spatial random effect—an extension of a standard stochastic partial differential equation model that allows for seamless modeling of noncontiguous states.30 The following model was estimated:
| (1) |
where pi is the probability that the i-th center participates in CACFP, β0 is an intercept, xik is the value of the k-th covariate at the i-th center, βk is the contribution of the k-th covariate, and si is the spatial effect at the i-th center. Noninformative priors for the β coefficients and weakly informative penalized complexity priors31 were used for the spatial parameters. The model was fitted using integrated nested Laplace approximations32 and the coastline model,30 which is a nonstationary extension of the stochastic partial differential equation representation of the Gaussian-Markov random fields approach.33 The center geolocations were considered using the Universal Transverse Mercator coordinate system. All numerical variables were standardized to have a mean of 0 and an SD of 1.
Given that centers serving high-income children are unlikely to be eligible for CACFP, and the full sample could include centers not eligible for the program, participation predictors were assessed for centers in low-income areas only. Models were fitted to the data with these covariates: the state CACFP agency type; an indicator for CACFP and child care licensing in 1 agency; indicators for having from 1 to 2 CACFP sponsors for unaffiliated centers and ≥3 sponsors; the state’s predominant political affiliation; state SNAP and WIC participation rates; and state website scoring and region indicators. Census-based measures included household income (log scale), percentage of high school graduates or higher, percentage of non-Hispanic White, and percentage of children aged <5 years. Center capacity and availability in 33 states were used as a covariate in sensitivity analyses. All analyses were run in R Core Team (version 4.2.2, Vienna, Austria).34 The University of Connecticut IRB deemed the study exempt from a human subject’s review.
RESULTS
The sample of matched licensing and CACFP records comprised 93,227 centers, of which 17,229 were in low-income areas. Of all the licensed child care centers serving young children in 47 states and DC, 36.5% participated in CACFP. In low-income areas where CACFP coverage was of priority, the mean CACFP participation rate was 57.5%. Higher-income areas had an average CACFP participation rate of 31.8%. Rates varied substantially across states, from 15.2% to 65.3% in the full sample (Figure 1) and from 15.7% to 85.7% in the low-income areas (Figure 2). Similarly, there were differences in CACFP participation rates across USDA regions, with the highest rates observed in the Southeast and the lowest in the West and Mountain Plains regions (Table 1).
Figure 1.
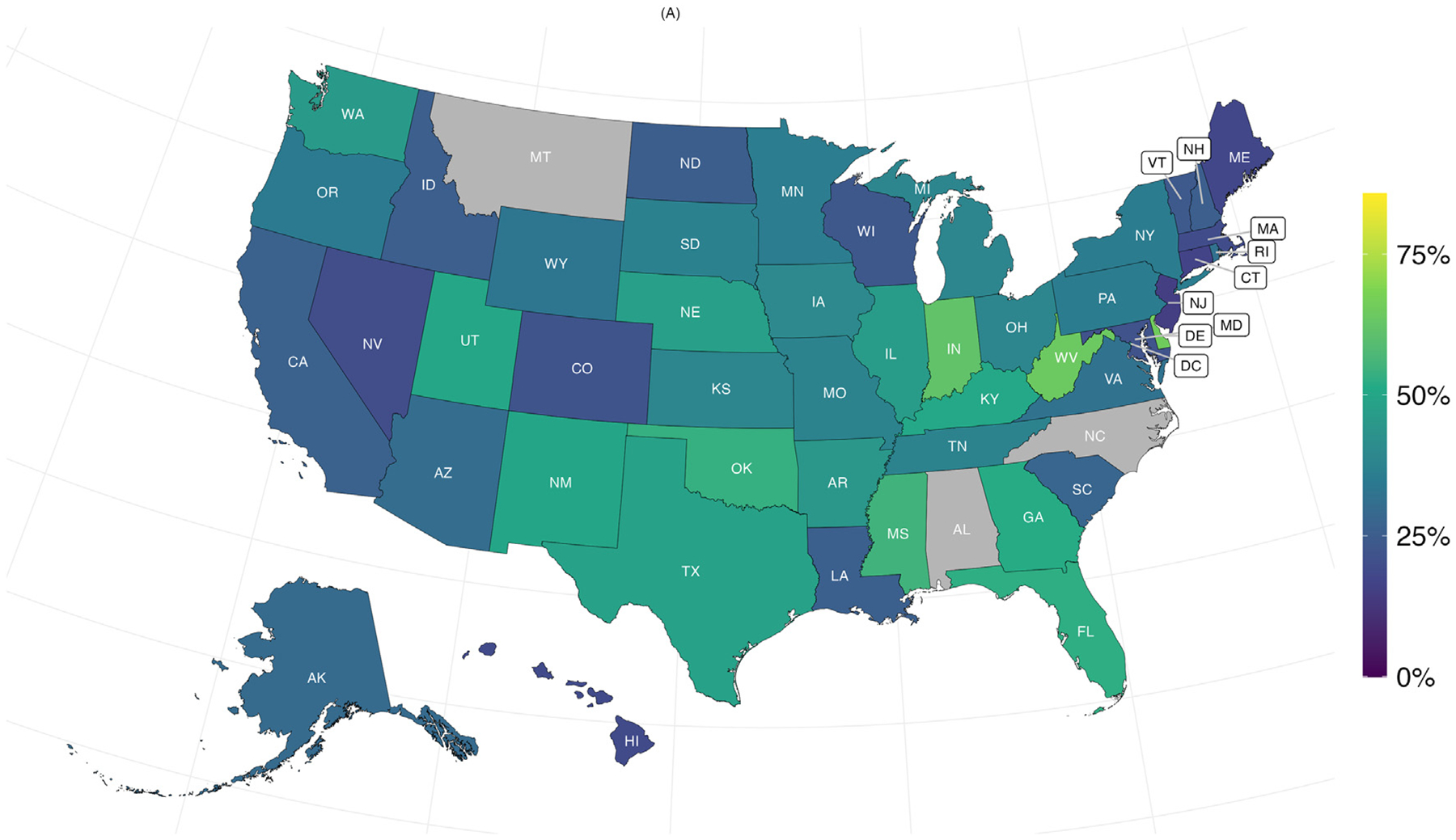
Unadjusted CACFP participation rates among licensed child care centers across states, full sample (N=93,227).
CACFP, Child and Adult Care Food Program.
Figure 2.
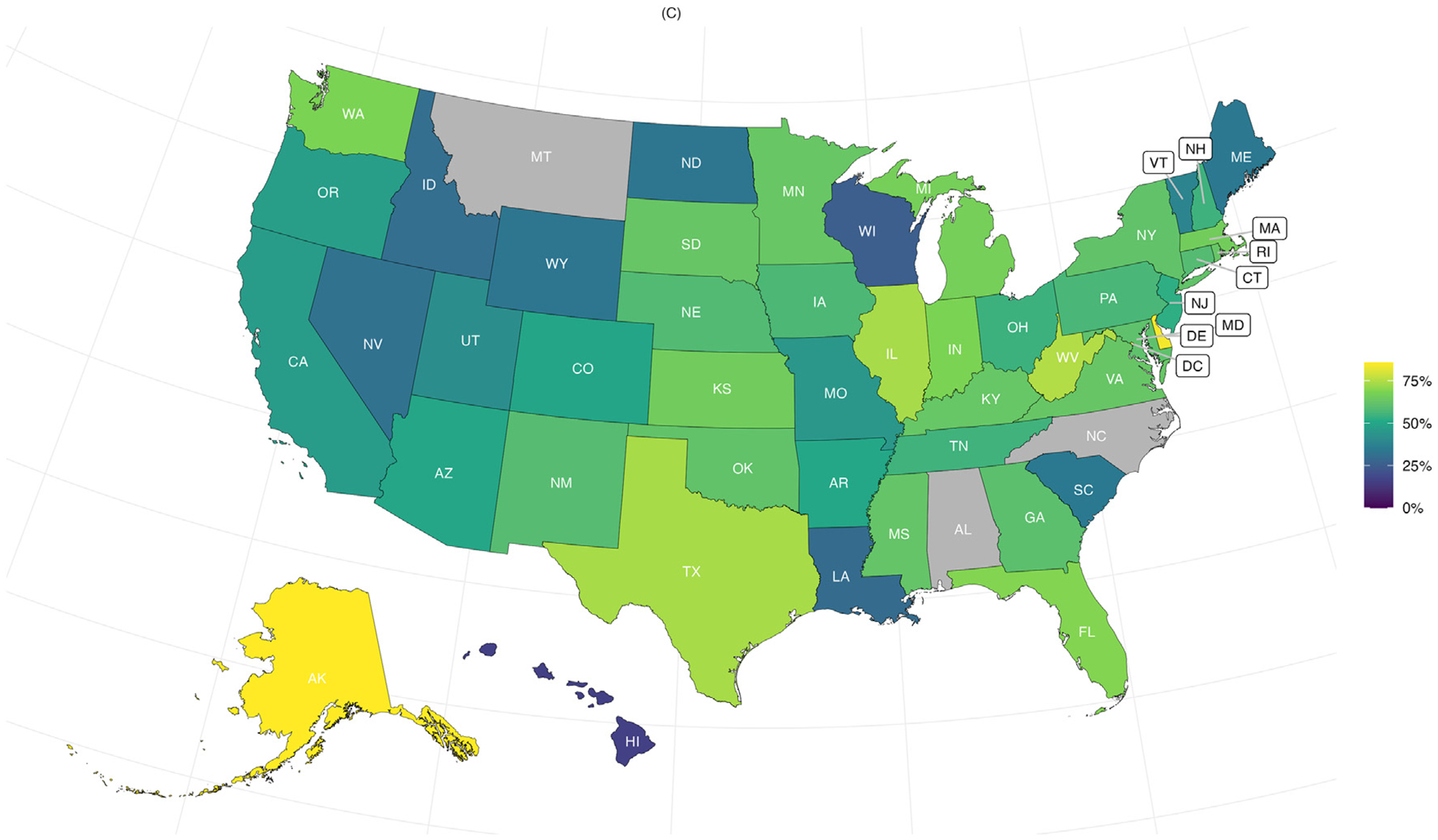
Unadjusted CACFP participation rates among licensed child care centers across states, low-income areas only (n=17,229).
CACFP, Child and Adult Care Food Program.
Table 1.
Unadjusted CACFP Participation Rates Among Licensed Child Care Centers by Region
| USDA regionsa | Full sample, % (N=93,227) |
Low-income areas, % (n=17,229) |
|---|---|---|
| Mid-Atlantic | 29.94 | 59.45 |
| Midwest | 38.83 | 58.93 |
| Mountain Plains | 32.15 | 49.27 |
| Northeast | 27.20 | 58.94 |
| Southeast | 47.63 | 60.46 |
| Southwest | 43.78 | 57.78 |
| West | 28.72 | 45.92 |
| Total | 36.48 | 57.49 |
Note: Boldface indicates statistical significance. A Bayesian model was used to compare the participation rates of different regions to the overall participation rate. To determine statistical significance, the 95% Bayesian credible interval (CI) for the deviations of each region from the grand mean (total) were used in an unadjusted model. A Bonferroni-corrected significance level of 0.63% was used to consider the number of groups compared. If the Bayesian CI associated with a region does not include 0, the result is considered statistically significant.
USDA regions26: Midwest: Iowa, Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin; Mid-Atlantic: District of Columbia, Delaware, Maryland, New Jersey, Pennsylvania, Virginia, and West Virginia; Mountain Plains: Colorado, Kansas, Missouri, Montana, North Dakota, Nebraska, South Dakota, and Wyoming; Northeast: Connecticut, Massachusetts, Maine, New Hampshire, New York, Rhode Island, and Vermont; Southeast: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, Tennessee, and South Carolina; Southwest: Arkansas, Arizona, Louisiana, New Mexico, Oklahoma, Texas, and Utah; and West: Alaska, California, Idaho, Hawaii, Nevada, Oregon, and Washington.
USDA, U.S. Department of Agriculture; CACFP, Child and Adult Care Food Program.
Table 2 displays estimation results for potential predictors of CACFP participation for the sample of low-income areas. At the state level, having at least 3 CACFP sponsors to work with unaffiliated centers predicted a 38% increase in the probability of CACFP participation (OR=1.38; 95% Credible Interval [CI]=1.08–1.78). States with higher SNAP participation rates also had higher rates of CACFP center participation (OR=1.12; 95% CI=1.01–1.24). Census tracts with higher education and higher proportions of non-Hispanic White residents had lower CACFP participation rates. Comparison between observed versus predicted state CACFP participation rates suggests that the Bayesian mixed-effects logistic regression model fits the data well (Appendix Figures 1 and 2, available online).
Table 2.
Bayesian Logistic Regression Results for Child Care Centers Located in Low-Income Areas (n=17,867)
| Variable | OR (95% CI) |
|---|---|
| Number of CACFP sponsors in state (ref: None) | |
| CACFP sponsors, 1–2 | 0.85 (0.65–1.11) |
| CACFP sponsors, ≥3 | 1.38 (1.08–1.78) |
| State agency administratively responsible for CACFP (ref: Department of Education) | |
| Department/office of social services | 0.88 (0.54–1.42) |
| Department/office of public health | 0.97 (0.74–1.28) |
| Department/office of early care and education | 1.39 (0.80–2.40) |
| Department/office of agriculture | 1.19 (0.86–1.66) |
| Licensing and CACFP in 1 state agency (ref: no) | 0.76 (0.52–1.12) |
| User-friendliness of CACFP state agency website (ref: low range score) | |
| CACFP agency website, middle range score | 1.21 (0.95–1.55) |
| CACFP agency website, high range score | 0.99 (0.74–1.32) |
| State participation in other nutrition assistance programs | |
| State-level SNAP participation rate | 1.12 (1.01–1.24) |
| State-level WIC participation rate | 1.00 (0.91–1.11) |
| Party affiliation (ref: Republican) | 0.85 (0.65–1.13) |
| USDA regionsa (ref: Midwest) | |
| Mid-Atlantic | 1.06 (0.71–1.59) |
| Mountain Plains | 0.89 (0.58–1.36) |
| Northeast | 1.39 (0.88–2.27) |
| Southeast | 0.80 (0.57–1.13) |
| Southwest | 0.74 (0.52–1.07) |
| West | 0.69 (0.47–1.01) |
| Census-tract characteristics | |
| Median household income, log scale | 0.99 (0.95–1.02) |
| Non-Hispanic White, % | 0.84 (0.80–0.89) |
| High school graduates or higher, % | 0.82 (0.78–0.86) |
| Children ages 0–5 years, % | 1.03 (1.00–1.07) |
| Intercept | 1.53 (1.08–2.15) |
Note: Boldface indicates statistical significance, where the 95% Bayesian CI does not include 1. Reference (ref) categories are specified for each binary and categorical variable.
USDA regions26: Midwest: Iowa, Illinois, Indiana, Michigan, Minnesota, Ohio, and Wisconsin; Mid-Atlantic: District of Columbia, Delaware, Maryland, New Jersey, Pennsylvania, Virginia, and West Virginia; Mountain Plains: Colorado, Kansas, Missouri, Montana, North Dakota, Nebraska, South Dakota, and Wyoming; Northeast: Connecticut, Massachusetts, Maine, New Hampshire, New York, Rhode Island, and Vermont; Southeast: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, Tennessee, and South Carolina; Southwest: Arkansas, Arizona, Louisiana, New Mexico, Oklahoma, Texas, and Utah; and West: Alaska, California, Idaho, Hawaii, Nevada, Oregon, and Washington.
CACFP, Child and Adult Care Food Program; CI, credible interval; SNAP, the Supplemental Nutrition Assistance Program; USDA, the U.S. Department of Agriculture; WIC, Women, Infants, and Children.
In sensitivity analyses, adjusting for center capacity among the 33 states where this variable was available did not meaningfully change model results for the state-level predictors. Among the subsample of states with data on center capacity, a 1 standard deviation (around 63 units) higher capacity was associated with 32% higher odds of CACFP participation (OR=1.32; 95% CI=1.26–1.37). Using income thresholds based on poverty status for a household size of 4 also did not change the results. Results of the sensitivity analyses are available upon request.
DISCUSSION
This nationwide study found that CACFP is underutilized. Across 47 states and DC, only 36.5% of all licensed child care centers serving young children participated in CACFP in FY 2019–2020, and only 3 of 5 licensed child care centers in the low-income areas participated in CACFP, despite the likely greater needs in the community. CACFP utilization is even lower in certain states and regions, suggesting additional barriers to program participation. The average CACFP participation rate of 57.5% in low-income areas is considerably lower than the estimated coverage rate of 82% for SNAP20 but similar to the average WIC participation rate of 56.9%.28
There are significant financial implications to this underutilization. Previous research estimated that CACFP underutilization in Connecticut left 20,300 children from low-income households without CACFP-subsidized meals and cost the state $30.7 million in foregone federal funds.10 By providing a food subsidy, these funds could have given an important economic boost to child care providers, who have been hit particularly hard by the COVID-19 pandemic.35
Understanding factors shaping the decisions of child care centers to provide meals and participate in CACFP should be a priority for the USDA, state agencies, and advocates seeking to improve child nutrition and food security. Although some research has explored participation barriers, more is needed.36–39 One study found lack of awareness as a key barrier, with more than half of the non-CACFP centers in 1 state did not even know that CACFP existed.14 Others have found the application process and compliance can be costly and hard to navigate, the administrative paperwork is burdensome, and providers are concerned about insufficient meal reimbursements.10,36–39 There is also little understanding of barriers to serving meals in child care centers, including the availability of food service companies that provide CACFP-compliant meals at affordable rates, limited staffing, equipment and kitchen facilities, local health and state regulations, and interest in center-provided food among parents.
Given the positive association between the number of sponsoring agencies serving centers and CACFP participation, addressing the issue of limited or unavailable sponsors for centers is another possible venue to target in the CACFP expansion efforts. Although centers could work directly with the state for all administrative paperwork, doing so through a sponsor could make the process easier, especially for smaller centers with more limited resources. Sponsoring agencies provide important technical assistance and training, including access to software, development of qualifying menus, documentation maintenance, and access to qualifying food, which could greatly reduce the burden of program participation.38,39 Despite the sponsors’ critical role in supporting CACFP, particularly for small centers, several states do not have any sponsoring agencies for unaffiliated centers or have only 1 sponsor.25
This study identified a common lack of cross-agency identifiers across state administrative databases. Very few CACFP state agencies include a state license number in their computer system, so that an automatic link with the list of licensed child care centers would be feasible and participation rates could be calculated quickly. Some licensing agencies include questions about CACFP participation, but it is self-reported and prone to error. There are other important gaps in the existing administrative data systems, which limit the ability of state agencies or researchers to measure program reach and impact. Data on the type of food service provided (i.e., meals and snacks served) are not routinely collected. Many agencies do not have information on the nonprofit status of their programs, which is a major factor in determining CACFP eligibility. Some CACFP state agencies do not include physical addresses of participating providers, which precludes analyses of how well CACFP can reach providers in specific communities. State agencies are encouraged to invest in developing modern electronic databases and address these data gaps to provide real-time data on program participation, eligibility, and reach.
Policymakers could play an important role in expanding access to CACFP. At the federal level, CACFP does not appear to receive the attention and funding that other nutrition assistance programs do. For example, CACFP does not have important flexibilities of the school meal programs, including the Community Eligibility Provision that allows serving free meals to all children in high-poverty areas without laborious collection of household income data. Extending the Community Eligibility Provision flexibility to CACFP-participating child care programs in high-poverty areas would remove a major participation burden reported by CACFP providers14 and improve equity across the USDA programs. State policymakers could help state agencies by providing adequate funding to administer CACFP effectively, including through modernized data collection and extensive outreach. Child care providers could benefit substantially from small grants to cover costs of applying for CACFP and/or remaining in compliance, software fees, updating kitchen facilities and/or equipment, and assistance with finding food service vendors.
Limitations
This study has several important strengths, including the use of administrative data for 93,227 geolocated centers and, to the best of our knowledge, the first ever compiled data on CACFP participation among licensed child care centers nationwide (except for 3 states). The unique strengths of the estimated model remove spatial confounding that enables more accurate estimation of non-spatial effects, accounts for the effects of unobserved covariates,40 reduces bias, and provides stability to the directionality of fixed effects coefficients.41 Model comparisons using information criteria (widely applicable information criterion42) indicate a superior model fit for the spatial random effect models.
Limitations included lack of data in 3 states and reliance on administrative data, which may have varied in quality. There was no information on CACFP eligibility, instead relying on the census-tract income of center locations as a proxy. Some children do not reside in the area where they attend daycare; however, residents in low-income areas may not have the means to travel to other areas for child care, so the area income may be a reasonable proxy for household income. Furthermore, the records had to be manually merged across state agencies, which could introduce errors owing to the large scope of data, however, 2 raters checked work. The model relied on a variety of state and census-tract covariates collected from multiple sources. Data on center capacity were not available for states, restricting the ability to evaluate its relationship with CACFP participation in all states. This study did not include daycare homes and after-school programs, which should be considered in future research on access to CACFP. Future analyses should study program access across different racial/ethnic communities and rural/urban settings.
CONCLUSIONS
Many licensed child care centers serving low-income areas do not utilize CACFP’s financial and training support for child nutrition and health, raising questions about unique barriers that the program has for its participants. The large variation in CACFP participation rates across states, after accounting for income differences, suggests some states developed effective strategies to reduce program barriers and increase participation. Future research should focus on understanding productive ways to expand CACFP so that millions of young children have access to nutritious foods while child care providers feel supported in providing the best nutritional environment for children in their care.
Supplementary Material
ACKNOWLEDGMENTS
The authors thank all state agencies that provided data for this analysis. They gratefully acknowledge research assistance in data merging by Xiaohan Sun, Hang Zhao, and Prakhar Jain, map generation by Katherine Zavez, and contributions to the website scoring development by Judy Prager and Melissa McCann.
The authors dedicate this article in memory of Dr. Dianne S. Ward, an extraordinary researcher, professor, mentor, and human being, whose pioneering work in child care nutrition has pushed this field forward in a major way. Dianne dedicated her career to improving the lives of young children and care providers as well as bringing more researchers and practitioners into the field. Her legacy will have a far and wide reach for years to come.
This study was funded by a grant from Healthy Eating Research, a national program of the Robert Wood Johnson Foundation (Grant Number 77232). Any opinions, findings, conclusions, or recommendations expressed here are those of the authors and do not necessarily reflect the views of the foundation.
No financial disclosures have been reported by the authors of this paper.
Footnotes
CREDIT AUTHOR STATEMENT
Tatiana Andreyeva: Conceptualization, Methodology, Data curation, Writing – original draft, Writing – review & editing, Supervision, Funding acquisition. Timothy E. Moore: Conceptualization, Methodology, Data curation, Formal analysis, Software, Writing – review & editing. Lucas da Cunha Godoy: Methodology, Data curation, Formal analysis, Software, Writing – review & editing. Erica L. Kenney: Writing – review & editing.
SUPPLEMENTAL MATERIAL
Supplemental materials associated with this article can be found in the online version at https://doi.org/10.1016/j.amepre.2023.09.008.
REFERENCES
- 1.Birch LL, Fisher JO. Development of eating behaviors among children and adolescents. Pediatrics. 1998;101(3 Pt 2):539–549. 10.1542/peds.101.S2.539. [DOI] [PubMed] [Google Scholar]
- 2.Lumeng JC, Taveras EM, Birch L, Yanovski SZ. Prevention of obesity in infancy and early childhood: a National Institutes of Health workshop. JAMA Pediatr. 2015;169(5):484–490. 10.1001/jamapediatrics.2014.3554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bailey RL, Jun S, Eldridge AL. The 2016 Feeding Infants and Toddlers Study (FITS): dietary intakes and practices of children in the United States from birth to 48 months. Nestlé Nutr Inst Workshop Ser. 2019;91:99–109. 10.1159/000493701. [DOI] [PubMed] [Google Scholar]
- 4.Liu J, Micha R, Li Y, Mozaffarian D. Trends in food sources and diet quality among US children and adults, 2003–2018. JAMA Netw Open. 2021;4(4):e215262. 10.1001/jamanetworkopen.2021.5262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kaphingst KM, Story M. Child care as an untapped setting for obesity prevention: state child care licensing regulations related to nutrition, physical activity, and media use for preschool-aged children in the United States. Prev Chronic Dis. 2009;6(1):A11. [PMC free article] [PubMed] [Google Scholar]
- 6.Larson N, Ward DS, Neelon SB, Story M. What role can child-care settings play in obesity prevention? A review of the evidence and call for research efforts. J Am Diet Assoc. 2011;111(9):1343–1362. 10.1016/j.jada.2011.06.007. [DOI] [PubMed] [Google Scholar]
- 7.de Brey C, Snyder TD, Zhang A, Dillow SA. Digest of education statistics 2019. NCES 2021–009. National Center for Education Statistics. Stat. 2021. [Google Scholar]
- 8.US Department of Agriculture, Food and Nutrition Service. Child nutrition tables. National level annual summary tables: FY 1969–2022 Child and adult care food - participation, meals and costs. https://www.fns.usda.gov/pd/child-nutrition-tables. Accessed June 19, 2023. [Google Scholar]
- 9.US Department of Agriculture, Food and Nutrition Service. Child and Adult Care Food Program (CACFP). https://www.fns.usda.gov/cacfp. Accessed September 28, 2023.
- 10.Andreyeva T, Sun X, Cannon M, Kenney EL. The Child and Adult Care Food Program: barriers to participation and financial implications of underuse. J Nutr Educ Behav. 2022;54(4):327–334. 10.1016/j.jneb.2021.10.001. [DOI] [PubMed] [Google Scholar]
- 11.Logan C, Connor P, LeClair L, et al. Study of nutrition and activity in child care settings: summary of findings. Alexandria, VA: USDA, Food and Nutrition Service, Office of Policy Support; 2021. Prepared by Abt Associates, Contract No. AG-3198-C-14–0017 https://fns-prod.azureedge.us/sites/default/files/resource-files/SNACS-Summary-of-Findings.pdf. [Google Scholar]
- 12.Ritchie LD, Boyle M, Chandran K, et al. Participation in the Child and Adult Care Food Program is associated with more nutritious foods and beverages in child care. Child Obes. 2012;8(3):224–229. 10.1089/chi.2011.0061. [DOI] [PubMed] [Google Scholar]
- 13.Korenman S, Abner KS, Kaestner R, Gordon RA. The Child and Adult Care Food Program and the nutrition of preschoolers. Early Child Res Q. 2013;28(2):325–336. 10.1016/j.ecresq.2012.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andreyeva T, Henderson KE. Center-reported adherence to nutrition standards of the Child and Adult Care Food Program. Child Obes. 2018;14(6):421–428. 10.1089/chi.2018.0076. [DOI] [PubMed] [Google Scholar]
- 15.Andreyeva T, Kenney EL, O’Connell M, Sun X, Henderson KE. Predictors of nutrition quality in early child education settings in Connecticut. J Nutr Educ Behav. 2018;50(5):458–467. 10.1016/j.jneb.2017.12.016. [DOI] [PubMed] [Google Scholar]
- 16.Erinosho T, Vaughn A, Hales D, Mazzucca S, Gizlice Z, Ward D. Participation in the Child and Adult Care Food Program is associated with healthier nutrition environments at family child care homes in Mississippi. J Nutr Educ Behav. 2018;50(5):441–450. 10.1016/j.jneb.2017.11.004. [DOI] [PubMed] [Google Scholar]
- 17.Zaltz DA, Hecht AA, Pate RR, Neelon B, O’Neill JR, Benjamin-Neelon SE. Participation in the Child and Adult Care Food Program is associated with fewer barriers to serving healthier foods in early care and education. BMC Public Health. 2020;20(1):856. 10.1186/s12889-020-08712-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kenney EL, Tucker K, Plummer RS, Mita C, Andreyeva T. The Child and Adult Care Food Program and young children’s health: a systematic review. Nutr Rev. 2023:nuad016. 10.1093/nutrit/nuad016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mabli J, Worthington J. Supplemental Nutrition Assistance Program participation and child food security. Pediatrics. 2014;133(4):610–619. 10.1542/peds.2013-2823. [DOI] [PubMed] [Google Scholar]
- 20.Oronce CIA, Miake-Lye IM, Begashaw MM, Booth M, Shrank WH, Shekelle PG. Interventions to address food insecurity among adults in Canada and the US: a systematic review and meta-analysis. JAMA Health Forum. 2021;2(8):e212001. 10.1001/jamahealthforum.2021.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.US Department of Agriculture, Food and Nutrition Service. SNAP participation rates by state, all eligible people (FY 2018). https://www.fns.usda.gov/usamap. Accessed June 19, 2023.
- 22.Arc GIS Pro Version 2.6.3 Redlands, CA: Esri Inc. [Google Scholar]
- 23.US Census Bureau. American Community Survey: Data Profiles: 2015 – 2019 ACS 5-Year Data Profile: 2019. https://www.census.gov/acs/www/data/data-tables-and-tools/data-profiles/2019/. Accessed September 28, 2023.
- 24.US Department of Agriculture, Food and Nutrition Service, Child nutrition programs: income eligibility guidelines. https://www.fns.usda.gov/cn/income-eligibility-guidelines. Accessed September 28, 2023.
- 25.National CACFP Sponsors Association. Find a food program sponsor. https://info.cacfp.org/sponsor. Accessed June 19, 2023.
- 26.Wikipedia. Political party strength in U.S. states https://en.wikipedia.org/wiki/Political_party_strength_in_U.S._states. Accessed September 28, 2023.
- 27.US Department of Agriculture, Food and Nutrition Service (FNS). FNS Regional Offices. https://www.fns.usda.gov/fns-regional-offices. Accessed June 19, 2023.
- 28.US Census Bureau. Current Population Survey Annual Social and Economic Supplement (CPS-ASEC). State-Level WIC Number Eligible and Number of Participants https://www.fns.usda.gov/wic/eligibility-and-coverage-rates-2018#5. Accessed June 21, 2023, 2018; 2019.
- 29.McCann M, Prager J, Andreyeva T. The Child and Adult Care Food Program: evaluation of state agency websites; 2022. https://uconn-ruddcenter.org/wp-content/uploads/sites/2909/2022/06/CACFP_FactSheet-062722.pdf. Accessed June 19, 2023.
- 30.Bakka H, Vanhatalo J, Illian JB, Simpson D, Rue H. Non-stationary Gaussian models with physical barriers. Spat Stat. 2019;29(3):268–288. 10.1016/j.spasta.2019.01.002. [DOI] [Google Scholar]
- 31.Simpson D, Rue H, Riebler A, Martins TG, Sørbye SH. Penalising model component complexity: a principled, practical approach to constructing priors. Stat Sci. 2017;32(1):1–28. 10.1214/16-STS576. [DOI] [Google Scholar]
- 32.Rue H, Martino S, Chopin N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J R Stat Soc B. 2009;71(2):319–392. 10.1111/j.1467-9868.2008.00700.x. [DOI] [Google Scholar]
- 33.Lindgren F, Rue H, Lindström J. An explicit link between Gaussian fields and Gaussian Markov random fields: the stochastic partial differential equation approach. J R Stat Soc B. 2011;73(4):423–498. 10.1111/j.1467-9868.2011.00777.x. [DOI] [Google Scholar]
- 34.R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2021. https://www.R-project.org/. [Google Scholar]
- 35.Bauer KW, Chriqui JF, Andreyeva T, et al. A safety net unraveling: feeding young children during COVID-19. Am J Public Health. 2021;111(1):116–120. 10.2105/AJPH.2020.305980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lee DL, Homel Vitale EH, Marshall SK, Hecht C, Beck LT, Ritchie LD. Child and Adult Care Food Program participation benefits, barriers and facilitators for independent child care centers in California. Nutrients. 2022;14(21):4449. 10.3390/nu14214449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Erinosho T, Jana B, Loefstedt K, Vu M, Ward D. Facilitators and barriers to family child care home participation in the U.S. Child and Adult Care Food Program (CACFP). Prev Med Rep. 2022;30:102022. 10.1016/j.pmedr.2022.102022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Heinz H, Bell D, Martinez J, Cunningham M, Maunders B, Jimenez EY. New Mexico sponsors identify time and money as factors affecting home-based provider Child and Adult Care Food Program engagement. J Nutr Educ Behav. 2022;54(10):947–956. 10.1016/j.jneb.2022.05.007. [DOI] [PubMed] [Google Scholar]
- 39.Jana B, Loefstedt K, Vu M, Ward D, Erinosho T. It has a lot to do with the cumbersome paperwork”: barriers and facilitators of center-based early care and education program participation in the Child and Adult Care Food Program. J Acad Nutr Diet. 2023;123(8):1173–1186.e1. 10.1016/j.jand.2023.03.014. [DOI] [PubMed] [Google Scholar]
- 40.Paradinas I, Illian J, Smout S. Understanding spatial effects in species distribution models. PLOS ONE 18(5): e0285463. 10.1371/journal.pone.0285463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Finley AO, Datta A, Cook BC, Morton DC, Andersen HE, Banerjee S. Efficient algorithms for Bayesian nearest neighbor Gaussian processes. J Comput Graph Stat. 2019;28(2):401–414. 10.1080/10618600.2018.1537924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Watanabe S Asymptotic equivalence of Bayes cross validation and widely application information criterion in singular learning theory. J Mach Learn Res. 2010;11:3571–3594. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.