

ABSTRACT
Background and Objectives:
Although immunization against coronavirus disease 2019 (COVID-19) is ongoing, adverse reactions to these vaccinations have been observed in isolated cases. We aimed to report different neurological complications developed after COVID-19 vaccination.
Materials and Methods:
In our case series study, we report all cases of CNS demyelination following COVID-19 immunization. Clinical evaluation, brain MRI, and CSF analysis for oligoclonal bands and IgG index were performed for all patients. Other investigations were performed for selected patients, including spine MRI, EEG, VEP, and aquaporin-4.
Results:
Eighteen patients (eight males and ten females) with no history of COVID-19 infection had neurological manifestations (vertigo, ataxia, recurrent attacks of loss of consciousness, optic neuritis, and myelitis) starting within 14 days after Pfizer (n = 12) and AstraZeneca (n = 6) vaccination. MRI was obtained during the acute stage of the disease. The most common presenting symptoms were optic neuritis and hemiparesis. Sixteen patients had altered signal intensity and multiple variable-sized, round to ill-defined oval lesions suggestive of MS. Two showed findings compatible with transverse myelitis
Conclusion:
This study identified CNS demyelination complications after COVID-19 vaccination. The COVID-19 vaccination could result in CNS complications, possibly connected to a post-vaccination inflammatory process. We recommend continuous post-marketing monitoring for adverse reactions in individuals who received the vaccines to establish a connection and guarantee the long-term safety of COVID-19 vaccines.
KEYWORDS: COVID-19, demyelination, myelitis, vaccines
INTRODUCTION
The current COVID-19 pandemic, caused by coronavirus 2 (SARS-CoV-2), is a global epidemiological alarm that necessitated the introduction of large-scale vaccine production. Given the great diversity of previous coronavirus epidemics, developing a scalable, technologically adaptable, and diverse platform to manufacture vaccines has been essential. These vaccinations must meet high effectiveness, safety, and tolerability standards.[1] The spike protein or its components serve as the basis for protein vaccinations. The inactivated SARS-CoV-2 virus is also used in numerous vaccinations. Additionally, reports of facial palsy (190 patients), Guillain–Barré syndrome (GBS; 32 patients), stroke (17 patients), transverse myelitis (nine patients), and acute disseminated encephalomyelitis (six patients) have been included in the vaccine-adverse event reporting system (VAERS) database. we investigated all cases of CNS demyelination following COVID-19 immunization in our case series analysis.
MATERIALS AND METHODS
This prospective observational study was conducted at Al-Azhar University Tertiary Hospital, Al-Azhar University-Assiut branch, Egypt, from the first of June 2021 to the end of February 2022. We included all patients with no history of COVID-19 infection who presented with different neurological manifestations within two weeks after receiving the first or second dose of the COVID-19 vaccine. All patients underwent a thorough medical examination, including a detailed history of their age, sex, occupation, smoking, and positive family history of MS or other demyelinating diseases. Additionally, details of the COVID-19 vaccine (Pfizer or AstraZeneca vaccine) and the number and date of doses were recorded. A complete neurological evaluation was performed, including the onset, course, and duration of neurological manifestations. The mental state; cranial nerves; motor, sensory, cerebellar function; and gait are all examined during a neurological examination. A brain MRI was performed for all patients, along with a spine MRI for selected patients (sagittal and axial non-contrast T1 images, axial T2 and T2 FLAIR images, and axial and coronal post-contrast T1 images were the basis for all patients). These showed images suggestive of the demyelinating disorder. In clinical practice, a lumbar puncture and CSF assessment of IgG oligoclonal bands and the IgG index in CSF are usually performed in patients suspected of having a demyelinating condition. Other investigations, such as EEG, VEP, and Aquaporin-4 (AQP-4), were performed for selected patients. AQP-4 is one of the largest molecules in the brain and is involved in several pathophysiological processes, including neuroinflammation. SPSS was used to execute appropriate statistical analyses, and the outcomes were tabulated. Significance was defined as P < 0.05.
RESULTS
The study was carried out on 18 patients who presented with different neurological disorders after the first or second dose of the COVID-19 vaccine. There were eight men (44.44%) and ten women (55.56%) with a mean age of 34.78 ± 7.13 years, ranging from 23 to 44 years. The mean duration between the onset of symptoms and the date of the last dose of the COVID-19 vaccine was 7.67 ± 3.83 days, ranging from 2–14 days. Regarding the type of vaccine, 12 patients (66.67%) received the Pfizer vaccine, and the remaining six (33.33%) received the AstraZeneca vaccine. Eight patients (44.44%) developed neurological manifestations after the first dose of the vaccine, and the remaining ten (55.56%) developed them after the second dose [Table 1].
Table 1.
Demographic data of the studied patients
| Variable | Number | Percent |
|---|---|---|
| Sex | ||
| Male | 8 | 44.44% |
| Female | 10 | 55.56% |
| Age (years) (Mean±SD) | 34.78±7.13 | |
| Time between the dose of vaccine and symptom (days) (Mean±SD) | 7.67±3.83 | |
| Type of vaccine | ||
| Pfizer | 12 | 66.67% |
| AstraZeneca | 6 | 33.33% |
| Number of doses of vaccine | ||
| First dose | 8 | 44.44% |
| Second dose | 10 | 55.56% |
Four patients (22.22%) presented with optic neuritis, three (16.67%) with hemiparesis, three (16.67%) with paraparesis, three (16.67%) with seizures (GTC and myoclonic), two (11.11%) with ataxia, one (5.56%) with hemihypesthesia, one (5.56%) with headache, and one (5.56%) with tinnitus [Table 2]. Sixteen patients (88.89%) had brain MRI findings suggestive of a demyelinating disorder [Figures 1 and 2], and two (11.11%) had a normal brain MRI but with the spine MRI showing a picture of transverse myelitis [Figure 3]. In the results of the oligoclonal band in CSF and serum, ten patients (55.56%) had a positive oligoclonal band in the CSF only, and the remaining eight (44.44%) had negative results. VEP was performed for ten patients. The results showed that four (22.22%) had prolonged P 100 latency, and the remaining six had normal P 100 latency. AQP-4 was performed for three patients and was negative [Tables 3 and 4].
Table 2.
Clinical presentation of the patients in the present study
| Variable | Number | Percent |
|---|---|---|
| Optic neuritis | 4 | 22.22% |
| Hemiparesis | 4 | 22.22% |
| Paraparesis | 3 | 16.67% |
| Seizures | 3 | 16.67% |
| Ataxia | 2 | 11.11% |
| Headache | 1 | 5.56% |
| Tinnitus | 1 | 5.56% |
Figure 1.
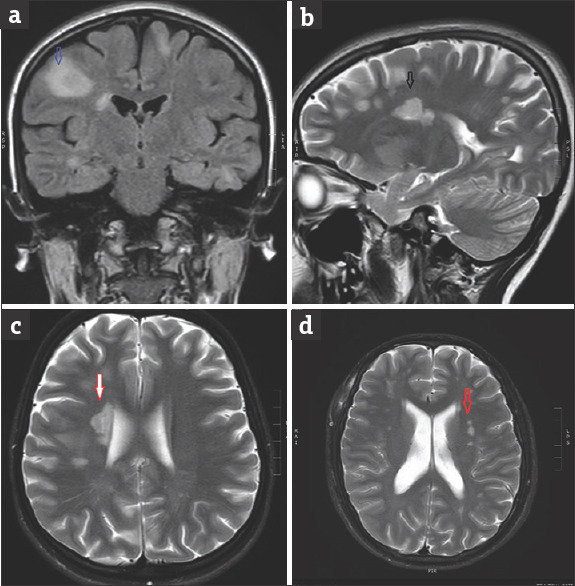
Case number 1: Coronal FLAIR (a), Sagittal T2 (b), and axial T2 (c and d) of the brain at the ventricular level supra tentorial region show multiple hyperintense foci seen at the deep white matter periventricular and perpendicular on the right lateral wall (red and black arrows) and subcortical lesions also noted (blue arrow) with mild edema
Figure 2.
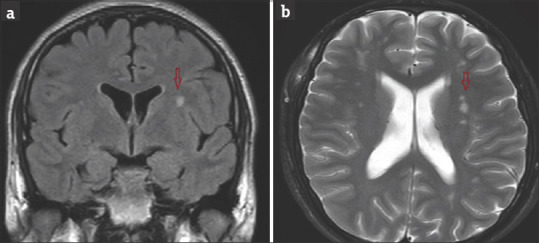
Case no 3: Coronal FLAIR (a) and Axial T2 (b) of the brain at the ventricular level there are multiple abnormal high signal foci at the periventricular white matter prominent at the left side (red arrows) with no edema or mass effect
Figure 3.

Case no 9: Sagittal T2 (a), Sagittal T1 (b), and axial T2 (c) of the spine show a long segment of intramedullary hyperintense signal with mild increase cord caliber expansion with the corresponding hypointense signal on T1 suggestive of transverse myelitis (yellow arrows)
Table 3.
Results of investigations
| Variable | Number | Percent |
|---|---|---|
| MRI finding | ||
| Demyelinating patches in brain only | 14 | 77.78% |
| Demyelinating patches in brain and spinal cord | 2 | 11.11% |
| Demyelinating patches in spinal cord only | 2 | 11.11% |
| Oligoclonal band in CSF | ||
| Positive in CSF | 10 | 55.56% |
| Negative in CSF | 8 | 44.44% |
| VEP (number of patients 10) | ||
| Prolonged P 100 latency | 6 | 60% |
| Normal P 100 latency | 4 | 40% |
Table 4.
Comparison between Pfizer and AstraZeneca
| Variable | Pfizer (n=12) | AstraZeneca (n=6) | P | ||
|---|---|---|---|---|---|
|
|
|
||||
| Number | Percent | Number | Percent | ||
| Sex | |||||
| Male | 4 | 22.22% | 4 | 22.22% | 0.201 |
| Female | 8 | 44.44% | 2 | 11.11% | |
| Age: years (Mean±SD) | 34.67±6.62 | 35.0±8.7 | 0.929 | ||
| Duration: days (Mean±SD) | 7.17±3.38 | 8.67±4.8 | 0.451 | ||
| Number of doses | |||||
| First dose | 4 | 22.22% | 4 | 22.22% | 0.325 |
| Second dose | 8 | 44.44% | 2 | 11.11% | |
| Oligoclonal band | |||||
| Positive | 6 | 33.33% | 4 | 22.22% | 0.437 |
| Negative | 6 | 33.33% | 2 | 11.11% | |
| Clinical presentation | |||||
| Optic neuritis | 4 | 22.22% | 0 | 00% | |
| Hemiparesis | 3 | 16.67% | 1 | 5.56% | |
| Paraparesis | 1 | 5.56% | 2 | 11.11% | |
| Seizures | 2 | 11.11% | 1 | 5.56% | |
| Ataxia | 1 | 5.56% | 1 | 5.56% | 0.165 |
| Headache | 1 | 5.56% | 0 | 00% | |
| Tinnitus | 0 | 00% | 1 | 5.56% | |
DISCUSSION
COVID-19 vaccinations are an essential component of the pandemic’s management. Like every vaccination, COVID-19 has potential adverse effects, most often low-grade fever, muscular pains, and infrequent neurological disorders. Our study included 18 patients who presented with different neurological disorders after the first or second dose of the COVID-19 vaccine within 14 days. Four patients (22.22%) presented with optic neuritis, three (16.67%) with hemiparesis, three (16.67%) with paraparesis, three (16.67%) with epilepsy (GTC and myoclonic), two (11.11%) with ataxia, one (5.56%) with hemihypesthesia, one (5.56%) with headache, and one (5.56%) with tinnitus. Optic neuritis is the most prevalent ocular severe adverse event following immunizations and the most frequent isolated inflammatory condition of CNS.[2,3] Some recent studies have reported a possible correlation between CNS autoimmune inflammation and COVID-19 vaccines. Voysey et al.[4] reported three cases of ATM; one was diagnosed with idiopathic demyelination, and the other two patients had pre-existing MS.[4] Ismaila et al.[3] reported 32 cases of CNS demyelination following all types of approved COVID-19 vaccines. Twelve (37.5%) of them had transverse myelitis, three (9.4%) had optic neuritis, three (9.4%) had GTC convulsions, and two (6.3%) had headache.[3] The optic nerve, brain, and spinal cord involvement caused new neurologic symptoms in all patients that appeared 1–21 (mean 13.7) days after immunization. These symptoms included limb weakness, paresthesias, sphincter dysfunction, dysmetria, gait instability, and visual loss. The patients’ mean age was 39.1 and ranged from 24 to 64 years. Five were females (71.4%). Four had previously received an RRMS or CIS diagnosis of demyelinating illness.[5] According to Goss et al., the most frequent neurological symptoms following the COVID-19 vaccine were headache, dizziness, muscular pain, and paresthesias. A few isolated reports have occurred of tinnitus, tremor, dysphonia, seizures, diplopia, and herpes zoster reactivation. The VAERS has reported facial palsy (190 patients), GBS (32 patients), stroke (17 patients), transverse myelitis (nine patients), and acute disseminated encephalomyelitis (six patients). In this study, the mean duration between the date of the dose of vaccine and the onset of symptoms was 7.67 ± 3.83 days, ranging from 2–14 days; 55.56% of patients were females, and 44.44% were males. The mean age of patients was 34.78 ± 7.13 years, ranging from 23–44 years. Overall, 66.67% of the patients received the Pfizer vaccine and 33.33% the AstraZeneca vaccine; 44.44% developed neurological manifestations after the first and 55.56% after the second dose. According to Ismail et al.,[3] neurological problems often begin to manifest during the first two weeks. The vast majority of instances involved women. The median age of the patients was 44 years (24–78 years), and the interval between immunization and the onset of clinical symptoms was nine days (1–30 days). Only 28.1% of patients experienced neurological symptoms after receiving the second vaccine dosage, which closely agrees with our findings and data from the literature, which show that around 83% of immune-mediated disorders affect women.[5] This has been linked to women having higher immune responses to both self- and foreign antigens than men.[6] In our study, 55.56% of patients had a positive oligoclonal band in CSF only and negative in serum, indicating that COVID-19 vaccination induces activation of symptoms of MS. Three cases of reactivation or new-onset demyelinating illness have been documented, according to Voysey[4] following immunization with the Oxford-AstraZeneca vaccine. Following the exclusion of pertinent differential diagnoses, we determined the diagnosis of relapse MS using the 2017 McDonald criteria. Although the precise mechanism of demyelination following COVID-19 vaccinations is still not fully known, a combination of vaccine-related variables and patient susceptibility plays a significant role. Some individuals may experience an unintended immune reaction as a result of the resemblance between the proteins of the viruses used for vaccination and self-antigens (such as myelin).[7] Another factor is the use of immunologic adjuvants, which are substances that increase immune responses to certain antigens and can mimic evolutionarily conserved chemicals that activate both the innate and adaptive immune systems.[8] TLR7 and TLR8 activation also results in the production of type I interferon, potent T and B cell responses, and the activation of bystander autoreactive cells.[9] This bystander activation and cytokine secretion by macrophages might lead to local inflammation and the recruitment of more T-helper cells.[10]
CONCLUSION
In this study, CNS demyelination was identified as a complication after receiving COVID-19 vaccination. COVID-19 vaccines could result in neurological consequences, probably due to an immunogenic process initiated by the vaccine in exposed individuals. Physicians and neurologists should be aware of these uncommon but severe adverse effects. We recommend continuing post-marketing monitoring for these individuals to establish the association and assure the safety of COVID-19 vaccines. Large-scale prospective studies are required to investigate the potential connections between COVID-19 vaccination and CNS demyelination, searching for novel ways to improve vaccination and increase its safety profile.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.AlJamaan F, Temsah MH, Alhasan K, Alenezi S, Alhaboob A, Alrabiaah A, et al. SARS-CoV-2 variants and the global pandemic challenged by vaccine uptake during the emergence of the delta variant: A national survey seeking vaccine hesitancy causes. J Infect Public Health. 2022;15:773–80. doi: 10.1016/j.jiph.2022.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cheng JY, Margo CE. Ocular adverse events following vaccination: Overview and update. Surv Ophthalmol. 2022;67:293–306. doi: 10.1016/j.survophthal.2021.04.001. [DOI] [PubMed] [Google Scholar]
- 3.Ismail II, Salama S. A systematic review of cases of CNS demyelination following COVID-19 vaccination. J Neuroimmunol. 2022;362:577765. doi: 10.1016/j.jneuroim.2021.577765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397:99–111. doi: 10.1016/S0140-6736(20)32661-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Angum F, Khan T, Kaler J, Siddiqui L, Hussain A. The prevalence of autoimmune disorders in women: A narrative review. Cureus. 2020;12:e8094. doi: 10.7759/cureus.8094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Somers EC, Thomas SL, Smeeth L, Hall AJ. Are individuals with an autoimmune disease at higher risk of a second autoimmune disorder? Am J Epidemiol. 2009;169:749–55. doi: 10.1093/aje/kwn408. [DOI] [PubMed] [Google Scholar]
- 7.García-Grimshaw M, Ceballos-Liceaga SE, Hernández-Vanegas LE, et al. Neurologic adverse events among 704,003 first-dose recipients of the BNT162b2 mRNA COVID-19 vaccine in Mexico: A nationwide descriptive study. Clin Immunol. 2021;229:108786. doi: 10.1016/j.clim.2021.108786. doi: 10.1016/j.clim.2021.108786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vera-Lastra O, Medina G, Cruz-Dominguez Mdel P, Jara LJ, Shoenfeld Y. Autoimmune/inflammatory syndrome induced by adjuvants (Shoenfeld's syndrome): Clinical and immunological spectrum. Expert Rev Clin Immunol. 2013;9:361–73. doi: 10.1586/eci.13.2. [DOI] [PubMed] [Google Scholar]
- 9.Velikova T, Georgiev T. SARS-CoV-2 vaccines and autoimmune diseases amidst the COVID-19 crisis. Rheumatol Int. 2021;41:509–18. doi: 10.1007/s00296-021-04792-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Aharon-Maor A, Shoenfeld Y. The good, the bad and the ugly of vaccination. Isr Med Assoc J. 2000;2:225–7. [PubMed] [Google Scholar]