

Abstract
Background and Aims
Perinatal grief have a significant influence on maternal mental health, hence appropriate tools for assessment are necessary. In this study, we translated and validated the Perinatal Grief Scale in Urdu (PGS‐Urdu) for use in Pakistan, therefore filling the gap in validated tools.
Methods
Data was collected from 165 women using consecutive sampling. Initially, “forward/backward” translation was used. For validity, content validity index and confirmatory factor analysis (CFA) were used respectively, and “Cronbach's‐Alpha” for reliability. In the validity stage, items 8, 11, 23, and 32 of the original scale were eliminated based on feedback from the target groups and the expert panel. For data‐analysis, SPSS 26 and Amos 26 were used.
Results
In analyzing the “Confirmatory factor analysis”, the “all‐fitness indicators” validated the three‐factor structure of 29‐item main scale. Cronbach alpha value was 0.83 for the entire scale The CFA results showed that all fitness indicators, with the exception of four, had loadings greater than 0.20, supporting the main scale's three‐factor structure. With a Cronbach's Alpha value of 0.83 for overall reliability, and varied from 0.81 to 0.87 for the PGS‐U variables. the PGS‐U exhibits an acceptable level of internal consistency.
Conclusion
The PGS‐U identifies women in perinatal grief for medical and social care. This research supports using the Urdu perinatal grief scale in obstetrics and bereavement counseling to reduce maternal mental health issues.
Keywords: perinatal bereavement, perinatal grief scale, perinatal‐loss, validation study
Highlights
Perinatal grief is a major contributor to maternal mental health problems. This study translated and validated the Perinatal Grief Scale (PGS) into Urdu (PGS‐U) for use in Pakistani women with perinatal loss. The PGS‐U was found to be a reliable and valid tool for assessing perinatal grief in Pakistan.
1. INTRODUCTION
Perinatal Loss affects around 10% of mothers globally. It is widely recognized that it has a profound influence on the physical and psychological wellness of the mother. 1 Whereas grieving is a natural, universal, and habitual reaction to an extreme loss. It occurs when an individual exhibits an excessive, ongoing, stressful, mourning process, indicating a severe public health problem that affects the individual, family members, and society. 2 Abortion, ectopic pregnancy, stillbirth, or newborn death account for 20%–25% of all births globally. The average perinatal death rate in Pakistan increased slightly from 60 to 90 thousand live births in 1997 to 63–92/thousand live births in 2004, with more than half being stillbirths, due to which perinatal grief after a loss is now widely acknowledged in Pakistan as a major mental health concern. 3 , 4
Perinatal loss traumatizes women and affects future pregnancies., 5 and has detrimental effects on spousal relationships. 6 Perinatal loss can cause severe depression, anxiety, irritability, and suicide ideation in women. 7 and if these responses are not addresses timely, it results in complications. 8 The issues may predispose women to risks of cardiovascular disease, diabetes, and eating disorders leading to excessive weight gain, and in extreme cases early mortality. 9 All these health conditions also negatively impact future pregnancies, therefore managing the after‐effects of perinatal loss is critical for woman's trauma recovery. 10
The available scarce evidence on grief following perinatal loss shows that women who have experienced perinatal losses face serious mental health issues. Hence, there is no validated tool in Urdu, which is the national language of Pakistan and is widely spoken and understood by everyone. Given that Pakistan has highest rates of perinatal losses in South Asia, it is important that there is a validated measure in Urdu to quantify the scale of perinatal grief. The present research helps to identify a tool to help health professionals identify women with perinatal loss at risk of adverse mental well‐being outcomes. The aim of the translation was to create a culturally appropriate scale in Urdu that preserves the meaning of each Urdu sentence when compared to its English counterpart and is understandable to the women in Pakistan. We also aim to validate this essential tool in Urdu.
2. METHODS
This validation research was based on translating the original “English version of the (short version of perinatal grief scale) SVPGS” using WHODAS 2.0 translation package (version 1.0) 11 The SVPGS were translated from English to Urdu by a professional (MA English), and then backward translated from Urdu to English by another professional (bilingual translator). To aid in the translation process, the focus group approach was employed. To complete the Urdu translation, the panel of seven members comprises bilingual professionals with English language competencies, psychiatry, psychology, clinician, public health (mental health), and gynecology, as well as a native speaker (Pakistan). IBM SPSS 26 was used to analyze the data, while Amox 26 was used to verify it. The validity and reliability of the study were checked by statistical analysis, and for testing reliability, Cronbach's alpha coefficients were calculated. A coefficient of alpha ≥0.70 was counted as good internal consistency reliability. And for validity, factor analysis was done. The translation aimed to produce a perinatal grief scale in Urdu that preserves the meaning of each Urdu sentence with its English counterpart and is understood by women in Pakistan, Figure 1.
Figure 1.

Overview of PGS‐U translation and validation.
2.1. Tool: Perinatal grief scale
The original English version of PGS contained 104 items. Later, items with poor correlation were deleted from the scale, resulting in a 33‐item PGS with a 0.95 alpha coefficient. 12 The 33‐item Likert scale has responses that vary from strongly agree to be 1 to strongly disagree being 5. 13 There are three subscales in the PGS: Active Grief (questions 1–11), including questions on topics such as sobbing for their infant, grief, or mourning the baby as a natural reaction to their loss. The difficulty coping subscale (questions 12–22) reflects the complexities of sorrow, such as a lack of social support, trouble with daily tasks, or a sense of guilt. Despair (questions 23–33) depicts a sense of hopelessness and the impact of prenatal bereavement on a long‐term basis. It has been reported that the severity of the responses increases as one progresses from Active Grief to Difficulty Coping with Despair. There are 11 items in each subscale. On the perinatal grief scale, the total subscale score varies from 33 to 165. A score higher than 90 is identified as having a psychiatric condition, which needs active treatment. 14
2.2. Sample
The hospital‐based validation study was conducted between August to November 2022, in the obstetrics and gynecology department of Rawal General and Dental Hospital (RG& DH) and Railway General Hospital. We used consecutive sampling technique for collecting data. This method helps to get data in consecutive manner that is first come, first served basis. According to the guidelines for validation study, “the respondent‐to‐item ratio” rule is applied, which means that for every 10 items on the questionnaire, there should be 50 respondents. Our questionnaire had 33 items and applying “respondent‐to‐item ratio” rule our estimated sample size was 165 women.
We included women with perinatal loss from the time of conception right through to the loss of a baby who was born alive but died within 28 days after birth (neonatal period) in the past 2 years, aged ≥18 years; women admitted to hospital or visited obstetrics and gynecology OPD, and women identified as a confirmed case of pregnancy loss by the physician. However, women who need emergency medical care, and women with psychotic episodes were excluded from the study.
2.3. Analysis
For the analysis of demographic characteristics we calculated percentages and frequencies (Table 1) using software SPSS version 26. For reliability testing Cronbach's alpha was computed to examine the internal consistency of the scale based on information from 165 women in the target group to establish the reliability of the final version of the PGS‐U.
Table 1.
Demographics of the participants.
| Characteristic | n (%) |
|---|---|
| Age | |
| 18–20 | 7 (4.2%) |
| 21–30 | 104 (63%) |
| 31–40 | 52 (31.5%) |
| 45+ | 2 (1.2%) |
| Education level | |
| No education | 40 (24.2%) |
| Primary | 31 (18.8%) |
| Secondary | 50 (30.3%) |
| Diploma | 13 (7.9%) |
| Degree | 31 (18.8%) |
| Employment status | |
| Unemployed | 130 (78.8%) |
| Employed part time | 35 (21.2%) |
| Pregnancy losses | |
| 1 | 81 (49.1%) |
| 2 or more | 84 (50.9%) |
| Time of loss (trimester) | |
| First trimester | 89 (53.9%) |
| Second trimester | 28 (17%) |
| Third trimester | 21 (12.7%) |
| Forth trimester | 27 (16.4%) |
| Type of loss | |
| Ectopic | 4 (2.4%) |
| Miscarriage | 91 (55.2%) |
| Stillbirth | 19 (11.5%) |
| Abortion | 23 (13.9%) |
| Neonatal death | 28 (17%) |
2.3.1. Qualitative assessment of content validity
Content and construct validity were used to validate the instrument. Content validity was assessed using qualitative and quantitative methodologies. Experts were asked to write about how to improve each item's content, Urdu grammar, amount of words and phrases, sequencing, and instrument structure for qualitative assessment. After getting expert feedback, the research team modified questionnaire items as needed.
2.3.2. Quantitative assessment of content validity
The Content Validity Index (CVI) supplied item validation data for quantitative assessment. Each questionnaire item was grouped in an excel spreadsheet and given individually to the panel of experts. After consulting experts, data was extracted and CVI was estimated using the method for each of the three parameters. The mean values and total CVI for each item were calculated last. After measuring the CVI for each item, the acceptability of each item was evaluated according to the following criteria: acceptable items (scores of >0.79), items needing adjustment (scores of 0.70–0.79), and unsatisfactory items (scores). 15
For the PGS‐U's qualitative content validity, eleven experts—one family physician, one mental health expert, two psychologists, one psychiatrist, one gynaecologist, one public health professional, and four women responsed to the questionnaire's content, scale wording, item allocation, and item scaling. The content validity index (CVI) was utilized for quantitative assessment, while the replies were used for qualitative assessment. Thus, the same experts were asked to evaluate all PGS‐U questions on a 4‐point Likert scale using three criteria, including relevancy. For instance, we asked experts to rate the topic on a “4‐point Likert‐scale” from 1 to 4. The four relevance scores ranged from 1 (not‐relevant) to 4 (highly‐relevant). CVI was determined for each item using the formula such as: [CVI = The No of raters providing a “3” or “4” rating/Total number of raters]. 16 Using recommendations by the previous researchers CVI 0.70 was deemed undesirable, CVI between 0.70 and 0.78 needed adjustment and modification, and CVI 0.79 was deemed acceptable. 17 After receiving experts' opinions, modest adjustments were made to a few areas and revisions made with as minimal changes to the original version of PGS as possible. Following that, we revised the pre‐final PGS‐U based on comments from the expert panel's viewpoints. The PGS‐U was finalized in preparation for construct validity.
2.4. Construct validity
We carried out a confirmatory factor analysis (also known as CFA) to investigate the construct validity of the PGS‐U 18 The number of components was previously known by the model's original author since the (CFA) look for a preset model based on earlier ideas and research; 19 It helps to determine which particular items make up subscales of which factors. The criteria also decide if the questions measure the desired indices. There are many goodness‐of‐fit indexes that determine model compatibility. The current analysis used AMOS 26 software for CFA to adjust expected factors. “Goodness‐of‐fit indices” used included (“Root Mean Square Error of Approximation”), known as (“RMSEA”), “Goodness‐of‐Fit index” (“GFI”), and the “Comparative Fit Index” (“CFI”). RMSEA readings below 0.08 are acceptable. CFI and GFI should be closer to 1 since this is preferable. 20
3. ETHICAL APPROVAL
The institutional review board, Ethical committee Rawal General and Dental Hospital (RG & DH) (Main Lehtrar Road, Khanapul Khanna Islamabad, Islamabad Capital Territory) and Railway General Hospital (Railway Carriage Factory Road, Railway Scheme 7, Rawalpindi, Punjab) provided ethical approvals. Consent from participants of the study and permission from one of the co‐authors of the original PGS (Judith N. Lasker of Lehigh University) was taken before the research via email.
4. RESULTS
In our sample, more than half (55.2%) of women suffered a miscarriage, 17.0% had neonatal mortality, and 11.5% had a stillbirth. In the first trimester, more than half (53.9%) of the losses were recorded, followed by 17% and 12% in the second and third trimesters, respectively. Most women (63%) were between the ages of 21 and 30, while 31.5% were older than 40. One‐third (30%) of women had an elementary education, while just 18% held a bachelor's degree. Only 17% of women were full‐time employees, while the majority (78%) were housewives.
A pilot study was done on 20 women, almost 10% of the population, with a Cronbach alpha of 0.8. While the Cronbach's alpha of 165 women was 0.83 for the total scale and 0.87, 0.80, and 0.83 for the subscales of the “Active Grief”, “Difficulty Coping” and “Despair” respectively shown in (Table 2). Cronbach's alpha coefficients for perinatal grief scale Urdu version subscales were higher than 0.70, which is the minimum standard for reliability. 21
Table 2.
Comparison of PGS‐U reliability with original and Persian Version.
The CVI of 29 items in the pre‐final PGS Urdu version was greater than 0.79, hence they were regarded as suitable items. Only four items (#8, #11, #23, and #32) had CVI scores less than 0.79, with several unclear wording and phrases, therefore modifications were proposed. The preliminary version of the “PGS Urdu” was sent to experts for review after considering experts' views about items with poor CVI scores. During the process of reexamination, all items acquired acceptable scores and were validated except #8, #11, #23, and #32. All four elements with low scores were removed from the first scale and the procedure was carried on without them. Finally, a final version of the PGS with 29 questions spread over three subscales was developed: “Difficulty of Coping,” with 9 items; “Active Grief,” with 11 items; and “Despair,” with 9 items.
The findings of the present study indicate CFI is 0.900, and RMSEA is 0.058 as shown in Table 3. To provide the most applicable model of (PSG‐U), a CFA was carried out to test the construct‐ validity using information obtained from 165 recruited women. Corrective indices were considered to arrive at a better result and improve the model. When analyzing outcomes of the CFA, covariance was applied to items D4 (PGS item no 17) and D7 (PGS item no 22), D6 (PGS item no 20), and D7 (PGS20), respectively shown in (PGS‐U attached) An observable performable covariance was used for the achievement of the desired goals. The (Table 3) shows results for CFA, and the graphic displays the model in (Figure 2). The conceptual model was constructed using AMOS version 26. This model shows that none of the 29 goods demonstrated any loading lower than 0.20, which was also used as a criterion. In the PGS‐U, four items had loadings lower than 0.20 on all three factors. These included item no. 8, which stated, “You have considered suicide since the loss.” item no. 11, item no. 23, and item no. 32, which considered bereaved parents synonymous to being a “Second‐Class Citizen.” Because their CVI was much lower than the requirement of 0.70, all of these questions were disqualified before CFA. 22 Only 29 items were subjected to the CFA test.
Table 3.
CFA fit indices.
Figure 2.
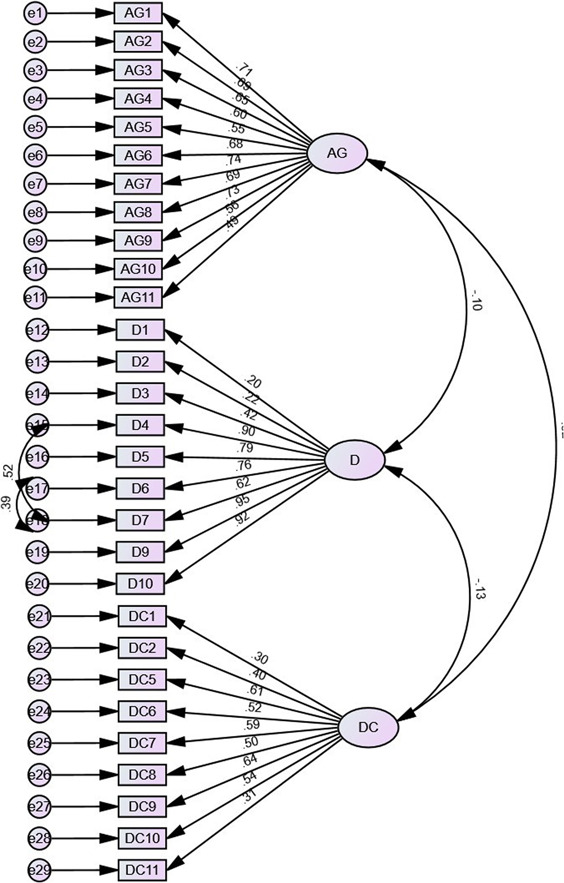
Structural model of PGS‐U on AMOS.
5. DISCUSSION
The goal of the current research was to provide a detailed account of the steps taken throughout the translation and cultural adaptation of the PGS into Urdu. The PGS went through a successful process of translation and adaptation on our end. In the process of developing the PGS‐U, four of the original items that comprised the scale were removed. Throughout the whole process of translating and culturally adapting PGS, we did not run across any significant obstacles. Even while it was not required to make significant modifications to the original form, we did make some small adjustments to some of the questions to make it easier for mothers to comprehend and to make it more culturally acceptable for Pakistani mothers. The comments received from experts were based on the opinions that were given by the target group during the validity stage. Item #2, which was “Do You find it hard to get along with certain people?”, was changed to “Do you feel difficulty in meeting certain people”. Some participants had problems understanding item 9 (“Do You take medicine for your nerves?”) which was then changed to, “Do you take drugs/medicines to comfort yourself?” and item #18 (Do you try to laugh, but nothing seems funny anymore?) changed to, “Don't you feel happy despite the effort?”
In contrast to the findings of earlier research, various translators of the (PGS) have incorporated a variety of cultural considerations into their work. Using the translation and the back translation procedure to translate the tool from English to Czech, the item on the Likert scale changed “not disagree, and “not agree” to “I don't know” because this expression is more frequently used by Czech people. 25 Translated version of PGS in Swedish used 5‐choice Likert‐scale with 10‐possible options, on Likert‐scale for their research in Sweden since their population was more familiar with this number of alternatives. This was done because the number of choices on the original scale was 5. Since the Urdu word for “grief” already exists, no modifications are required. 26
In the validity evaluation, items #8, #11, #23, and #32 were not relevant even after being reevaluated based on the views of the women who were a part of the target group and the opinions of the experts. Simplicity, relevancy, and clarity are three criteria of the CV1 assessment 27 As a result, items #8, #11, #23, and #32 were deleted from the PGS Urdu version, and the process resumed without them. In a previous study, which also included the translation of this scale into other languages, the Persian version of the scale provided a report regarding the deletion of items at this stage; before the “confirmatory factor analysis”. As a result, the deletion of four items at this stage is comparable to research that has been done in the past. The results of the CFA analysis in this research indicate that the model fitness measures were appropriate. Persian version of the perinatal grief scale showed similar results to our study. 31 items had CVI lower than 0.79 in PGS Persian version. Whereas, construct validity also showed similar results with PGS‐U, CFI for both the PGS‐ U and PGS Persian version is 0.86. Whereas RMSEA of the Persian version is 0.06 whereas the Urdu version has less than 0.05 which is more appropriate. 27 The Urdu version of PGS has three factors, one is Active grief which has 11 questions, Difficulty coping having 9 questions moreover, Despair has 9 questions. However, in the Czech version of PGS, EFA was assessed based on maximum likelihood with varimax rotation. Exploratory factor analysis (EFA) came first in the study taken out in Spanish version of PGS 28 Then came the confirmatory factor analysis (CFA). The findings of this phase suggest that 19 of the 33 items on the primary scale had an appropriate factor indicated on two of the factors. Then, the CFA was conducted, and the scale was validated by two factors: “Active Grief,” with 13 questions, and “Difficulty Coping/Despair,” with 6 items for each component. Before going on to a confirmatory component analysis, Biatric and colleagues started their investigation with an exploratory factor analysis. The two‐factor structure of the scale was validated by removing four items from the scale and placing the remaining questions on the subscales (“Active Grief” and “Complicated Grief”). 29
In the present analysis, the data that were collected during the reliability stage of the scale revealed that the PGS‐U had a high degree of stability. Because of this, the alpha coefficients that the Reliability coefficient produced for the overall scale as well as the subscales that were labeled “Active grieving,” “Difficulty Coping,” and “Despair” were appropriate.
6. LIMITATIONS OF THE STUDY
Analogous to other studies, this study also has several limitations. Small sample size was the limitation in the study. Data was only collected from the hospitals instead of the general population due to time constraint. The results of the research may have limited applicability to women in other areas or countries, since it was done only with a specific set of women in a particular region of Pakistan. The reliability of the PGS‐Urdu might be impacted by cultural disparities among Urdu‐speaking groups. It is crucial to investigate the applicability of the scale to various cultural groupings. Furthermore, the PGS‐Urdu was compared to other existing Urdu scales or measures assessing perinatal grief. It would be valuable to understand how the PGS‐Urdu compares to similar tools in terms of reliability and validity.
7. RECOMMENDATIONS
Promote the use of the translated and approved PGS‐Urdu in Pakistani clinical settings. The availability and validity of the tool to measure perinatal grief in Pakistani women should be disclosed to clinicians and other healthcare professionals. Give healthcare professionals instruction on how to administer and interpret the PGS‐Urdu. This will guarantee that experts have all they need to apply the instrument efficiently, which will enhance the identification and assistance of women going through perinatal grief. Establish public health initiatives to increase understanding of prenatal loss and its effects on the mental health of mothers. Promote the availability of the PGS‐Urdu, a culturally validated instrument for perinatal grief assessment, and stress the value of early intervention and support‐seeking. Promote further studies on the PGS‐Urdu's applicability in Pakistan's varied demographics. To make sure it is widely applicable, look at its usefulness in various geographical locations, socioeconomic situations, and cultural contexts. Work together to include the PGS‐Urdu into the programs of mental health organizations and support groups. This may provide a comprehensive strategy for perinatal mental health assistance by fusing community‐based treatments, counseling, and evaluation instruments. Encourage the use of culturally validated instruments in perinatal mental health assessments and their integration into national health strategies. This will highlight how crucial it is to treat perinatal loss as a crucial aspect of providing healthcare to mothers.
AUTHOR CONTRIBUTIONS
Maryam Nisa: Conceptualization. Seema Laila: Writing–original draft. Muhammad Muzzamil: Writing–original draft. Anum Ghafoor: Writing–original draft. Najma Zakir: Resources; data curation. Tehzeeb Zulfiqar: Methodology; supervision. Abid Malik: Writing–original draft; writing–review & editing. Abdullah Malikzai: Writing–original draft; writing–review & editing.
CONFLICT OF INTEREST STATEMENT
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
TRANSPARENCY STATEMENT
The lead author Abdullah Malikzai affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
ACKNOWLEDGEMENTS
We received no funding for this paper.
Nisa M, Laila S, Muzzamil M, et al. “Translation, cultural adaptation, and validation of perinatal grief scale in Urdu: addressing a gap in the research of perinatal loss in Pakistan–Cross‐sectional validation study”. Health Sci Rep. 2024;7:e1999. 10.1002/hsr2.1999
DATA AVAILABILITY STATEMENT
All data included in manuscript.
REFERENCES
- 1. Delgado L, Cobo J, Giménez C, et al. Initial impact of perinatal loss on mothers and their partners. Int J Environ Res Public Health. 2023;20(2):1304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Paris GF, De Montigny F, Pelloso SM. Cross‐cultural adaptation and validation evidence of the perinatal grief scale. Texto Contexto Enferm. 2017;26(1). 10.1590/0104-07072017005430015 [DOI] [Google Scholar]
- 3. Bhutta ZA, Rehman S. Perinatal care in Pakistan: a situational analysis. J Perinatol Off J California Perinatal Assoc. 1997;17(1):54‐59. [PubMed] [Google Scholar]
- 4. Jalil F. Perinatal health in Pakistan: a review of the current situation. Acta Paediatr. 2004;93(10):1273‐1279. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1651-2227.2004.tb02923.x [DOI] [PubMed] [Google Scholar]
- 5. Charrois EM, Bright KS, Wajid A, Mughal MK, Hayden KA, Kingston D. Effectiveness of psychotherapeutic interventions on psychological distress in women who have experienced perinatal loss: a systematic review protocol. Syst Rev. 2020;9(1):125. Available from: 10.1186/s13643-020-01387-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Avelin P, Rådestad I, Säflund K, Wredling R, Erlandsson K. Parental grief and relationships after the loss of a stillborn baby. Midwifery. 2013;29(6):668‐673. Available from: https://www.sciencedirect.com/science/article/pii/S0266613812001076 [DOI] [PubMed] [Google Scholar]
- 7. Nynas J, Narang P, Kolikonda MK, Lippmann S. Depression and anxiety following early pregnancy loss: recommendations for primary care providers. Prim Care Companion CNS Disord. 2015;17(1). Available from: 10.4088/PCC.14r01721 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zisook S, Shear K. Grief and bereavement: what psychiatrists need to know. World Psychiatr [Internet]. 2009;8(2):67‐74. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2691160/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Rahmati M, Saei Ghare Naz M, Azizi F, Ramezani Tehrani F. Pregnancy loss and subsequent risk of prediabetes, diabetes and metabolic syndrome in couples: Tehran lipid and glucose study. J Transl Med. 2022;20(1):372. Available from: 10.1186/s12967-022-03578-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Egerup P, Mikkelsen AP, Kolte AM, et al. Pregnancy loss is associated with type 2 diabetes: a nationwide case–control study. Diabetologia. 2020;63(8):1521‐1529. Available from: 10.1007/s00125-020-05154-z [DOI] [PubMed] [Google Scholar]
- 11. Setubal MS, Bolibio R, Jesus RC, et al. A systematic review of instruments measuring grief after perinatal loss and factors associated with grief reactions. Palliat Support Care. 2021;19(2):246‐256. [DOI] [PubMed] [Google Scholar]
- 12. Toedter LJ, Lasker JN, Alhadeff JM. The perinatal grief scale: development and initial validation. Am J Orthopsychiatry. 1988;58(3):435‐449. [DOI] [PubMed] [Google Scholar]
- 13. Theut SK, Pedersen FA, Zaslow MJ, Cain RL, Rabinovich BA, Morihisa JM. Perinatal loss and parental bereavement. Am J Psychiatry. 1989;146(5):635‐639. [DOI] [PubMed] [Google Scholar]
- 14. Hutti MH, dePacheco M, Smith M. A study of miscarriage: development and validation of the perinatal grief intensity scale. J Obstet Gynecol Neonatal Nurs. JOGNN. 1998;27(5):547‐555. [DOI] [PubMed] [Google Scholar]
- 15. Beutel M, Deckardt R, Schaudig K, Franke S, Zauner R. Grief, depression and anxiety after spontaneous abortion: a study of systematic evaluation and factors of influence. Psychother Psychosom Med Psychol. 1992;42(5):158‐166. [PubMed] [Google Scholar]
- 16. Potvin L, Lasker J, Toedter L, Potvin L, Lasker J, Toedter L. Measuring grief a short version of the perinatal grief scale. J Psychopathol Behav Assess [Internet]. 1989;11(1):29‐46. Available from https://eurekamag.com/research/007/539/007539085.php [Google Scholar]
- 17. Adolfsson A. Meta‐analysis to obtain a scale of psychological reaction after perinatal loss: focus on miscarriage. Psychol Res Behav Manag [Internet]. 2011;4:29‐39. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3218782/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Capitulo K, Ramirez M, Grigoroff‐Aponte B, Vahey D. Psychometric testing of the new Spanish short version of the perinatal grief scale to measure perinatal grief in Spanish‐speaking parents. Hisp Health Care Int. 2010;8:125‐135. [Google Scholar]
- 19. Yan E, Tang CSK, Chung T. Validation of the perinatal grief scale for use in Chinese women who have experienced recent reproductive loss. Death Stud. 2010;34(2):151‐171. [DOI] [PubMed] [Google Scholar]
- 20. Köneş M, Mecdi M, Aslan E, Yıldız H. The perinatal grief scale (33‐item short version): validity and reliability of the Turkish version. Anatol J Psychiatry. 2016;18:1. [Google Scholar]
- 21. Tavakol M, Dennick R. Making sense of Cronbach's alpha. Int J Med Educ [Internet]. 2011;2:53‐55. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4205511/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Toedter LJ, Lasker JN, Janssen HJ. International comparison of studies using the perinatal grief scale: a decade of research on pregnancy loss. Death Stud. 2001;25(3):205‐228. [DOI] [PubMed] [Google Scholar]
- 23. Das MK, Arora NK, Gaikwad H, et al. Grief reaction and psychosocial impacts of child death and stillbirth on bereaved North Indian parents: a qualitative study. PLoS ONE [Internet]. 2021;16(1):e0240270. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7840017/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Xue T, Guan T, Geng G, Zhang Q, Zhao Y, Zhu T. Estimation of pregnancy losses attributable to exposure to ambient fine particles in south Asia: an epidemiological case‐control study. Lancet Planet Health. 2021;5(1):e15‐e24. [DOI] [PubMed] [Google Scholar]
- 25. Ratislavová K, Kalvas F, Jiří B. Validation of the Czech version of the perinatal grief scale. Cent Eur J Nurs Midwifery. 2015;6:191‐200. [Google Scholar]
- 26. Ravaldi C, Bettiol A, Crescioli G, et al. Italian translation and validation of the perinatal grief scale. Scand J Caring Sci. 2020;34(3):684‐689. [DOI] [PubMed] [Google Scholar]
- 27. Amiri P, Bahaadinbeigy K, Asadi F, Rahmati S, Mazhari S. Validation of the persian version of the perinatal anxiety screening scale (PASS) among antenatal and postnatal women. BMC Pregnancy Childbirth [Internet]. 2022;22:883. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9706838/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Fernández‐Alcántara M, Madrid‐Valero JJ, Esteban‐Burgos AA, Congost‐Maestre N, Oliver‐Roig A, Cabañero‐Martínez MJ. Spanish adaptation of the perinatal grief intensity scale. J Reprod Infant Psychol. 2024:1‐12. [DOI] [PubMed] [Google Scholar]
- 29. Adolfsson A, Larsson PG. Translation of the short version of the perinatal grief scale into Swedish. Scand J Caring Sci. 2006;20:269‐273. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data included in manuscript.