

Abstract
Symptom-system fit theory proposes that problematic behaviors are maintained by the social system (e.g., the couple relationship) in which they occur because they help promote positive relationship functioning in the short-term. Across three daily life studies, we examined whether mixed-gender couples reported more positive relationship functioning on days in which they engaged in more shared problematic behaviors. In two studies (Study 1: 82 couples who smoke; Study 2: 117 couples who are inactive), days of more shared problematic behavior were accompanied by higher daily closeness and relationship satisfaction. A third study with 79 couples post-stroke investigating unhealthy eating failed to provide evidence for symptom-system fit. In exploratory lagged analyses, we found more support for prior-day problematic behavior being associated with next-day daily relationship functioning than vice-versa. Together, findings point to the importance of a systems perspective when studying interpersonal dynamics that might be involved in the maintenance of problematic behaviors.
Keywords: symptom-system fit, daily diary, couples, problematic behaviors, relationship functioning
Humans are by nature social, and a sense of belonging is central to well-being (Allen et al., 2021). However, the need to belong might lead an individual to engage in behavior that is detrimental in the long term (Litt et al., 2012; Troisi & Gabriel, 2011). Symptom-system fit theory (Rohrbaugh et al., 2002; Shoham et al., 2007) describes the phenomenon of shared problematic behavior in couples as a symptom reinforced by immediate benefits for the relationship (the “system”). The current study builds on prior laboratory research and moves on to examine symptom-system fit as it occurs in couples’ everyday lives. Specifically, we investigated three different shared problematic behaviors (i.e., “symptoms”: smoking, sedentary behavior, and unhealthy diet) and how these are associated with indicators of daily relationship functioning. This approach advances the existing literature on functions of interdependent behaviors in couples that has mainly focused on beneficial, positive, and health-promoting behaviors (e.g., Aron et al., 2000; Girme et al., 2014) and has so far rarely considered its simultaneous propensity to encourage problematic behaviors.
Symptom-System Fit Theory: Understanding Problematic Behaviors in Couples
Individuals often engage in behaviors that are pleasurable in the short-term but carry risks for health and well-being in the long run (Ding et al., 2015), henceforth called “problematic behaviors.” Examples include excessive media use, gambling, drugs, risky sexual behavior, and consuming unhealthy foods. Problematic behaviors might be shared among couples because they spend a lot of time with each other and interact frequently (Kiecolt-Glaser & Wilson, 2017). Family systems theory (Bowen, 1978; Butler, 2011; Cox & Paley, 1997) describes individuals as situated within systems, in which individuals cannot be understood in isolation because they are dynamically connected. Taking a systems approach to understand problematic behaviors in couples, symptom-system fit theory (Rohrbaugh et al., 2002; Shoham et al., 2007) contends that partners’ motivation to engage in shared problematic behaviors is shaped by its function within the relationship, that is, to restore or preserve important relationship parameters (e.g., reducing conflict, increasing closeness, or supporting relationship cohesion). The problematic behavior (the “symptom”) thus implicitly contributes to positive relationship functioning in the short-term. In other words, it “fits” the relational system in which it occurs (Rohrbaugh et al., 2002). Following this line of thought, couples might engage in shared behaviors that can be detrimental for health or well-being such as smoking, drinking excessive alcohol, eating unhealthy foods, or being sedentary because, at least in the short-term, these behaviors have immediate interpersonal benefits (Shoham et al., 2007).
Symptom-system fit theory implies that the problematic behavior in question is done together and that it reflects the same behavior, at the same time, in the same space (Shoham et al., 2007). However, there likely is a continuum of shared problematic behaviors. At one end of the continuum, partners may be doing exactly the same behavior together at the same point in time and in the same space (e.g., watching a TV show together). Moving further away from this end of the continuum, partners may engage in the same or a similar behavior at the same time and in the same space but not together (e.g., each partner individually scrolling through social media on their own phones at the same point in time). At the other end of the continuum, partners may do the same or similar behavior but not necessarily situated in the same time and space (e.g., each partner individually spending 6 hrs a day gaming on the computer but at different times and places). We propose that, in principle, all of these behaviors may have important relationship functions (e.g., activating feelings of “we-ness” and shared identity, thereby increasing closeness; Branand et al., 2019). However, we also assume that the strength of implications for the couple may diminish gradually along the sharedness continuum. Here in the current study, the targeted behaviors are operationally defined as shared problematic behaviors at different positions along this spectrum, that is, as the same or similar behaviors that partners engage in together, at the same time, or close in time despite potential negative ramifications for individual health and well-being.
Initial empirical support for symptom-system fit comes from studies investigating alcohol consumption and smoking (Rohrbaugh et al., 2002; Shoham et al., 2007). Researchers observing 63 couples discussing drinking behavior in the lab found evidence that in about half the couples alcohol use served some adaptive function, for example, by increasing intimacy or positive affect (Rohrbaugh et al., 2002). Shoham et al. (2007) observed couples in which one or both partners smoked (single- or dual-smoker couples) during an interaction task in the lab. They found that dual-smoker couples reported increased positive affect when smoking together, while partners in single-smoker couples reported a decrease in positive affect when one partner smoked. Utilizing the same dataset, the authors also investigated the extent to which affective experiences changed in a coordinated fashion (i.e., synchronously) throughout the lab visit (Rohrbaugh et al., 2009). Specifically, an analysis of covariation of moment-to-moment changes in affect between partners indicated that affective synchrony increased from baseline to smoking in dual-smoker couples, whereas it decreased in single-smoker couples. Taken together, these studies suggest that joint smoking might promote positive affective experiences and cohesiveness in dual-smoker couples.
More symptom-system fit for weight and eating behavior (Skoyen et al., 2014, 2018) was shown in couples who used more “we”-talk (indexing higher dyadic cohesion) as compared with couples who used more “I”-talk (indexing higher relational autonomy) while talking about health-relevant lifestyles during a laboratory task. In couples who used eating as an emotion-regulation strategy, more “we“-talk was associated with higher body mass index (BMI) among women (Skoyen et al., 2014). Furthermore, using data from the same sample, raters objectively coded the couple discussion for shared problematic behaviors (e.g., as indicated by a shared unhealthy diet; drinking alcohol together; sharing little regard for health in general; Skoyen et al., 2018). Findings show that shared problematic behaviors were unrelated to BMI for couples with poor relationship quality. However, in couples with high relationship quality, a greater extent of shared unhealthy behavior was associated with higher BMI in women. The authors argued that the observed gender difference might be explained by women more likely adapting to the unhealthy habits of their male partner, than vice versa (Skoyen et al., 2018).
In brief, the above laboratory research indicates that shared problematic behaviors such as unhealthy eating or smoking might be maintained in couples due to their positive relationship functions, at least in the short-term. However, positive relationship functioning has often been measured indirectly (e.g., as affective synchrony: Rohrbaugh et al., 2009; using we-talk: Skoyen et al., 2014), and when it was measured directly (e.g., relationship quality: Skoyen et al., 2018) it was assessed as a stable construct rather than on a time-varying level. This makes it difficult to examine whether for a given couple engaging in shared problematic behaviors goes along with more positive relationship functioning. It is also an open question whether symptom-system fit generalizes across different shared problematic behaviors. There is some evidence that symptom-system fit exists for alcohol consumption (Rohrbaugh et al., 2002), smoking (Rohrbaugh et al., 2009), and shared unhealthy habits in general (Skoyen et al., 2018). Yet, it remains to be tested whether this phenomenon extends to established lifestyle factors that also carry chronic disease risk but appear less saliently risky such as sedentary behavior and unhealthy diet (Roberts & Barnard, 2005). Third, previous research was laboratory-based, either prompting couples to engage in the shared problematic behavior (smoking a cigarette together: Shoham et al., 2007) or by asking partners to talk about a certain topic and coding the conversation for shared problematic behaviors (e.g., Skoyen et al., 2018).
Thus, the present research aims to move beyond existing work by taking the investigation of symptoms and systems out of the lab into daily life and by examining three different problematic behaviors (smoking, sedentary behavior, and unhealthy diet) and their time-varying associations with two indicators of positive relationship functioning (closeness and relationship satisfaction). In experience sampling or daily diary studies, participants are asked to describe experiences, behaviors, and social interactions on a day-to-day basis, sometimes along with wearing objective monitoring devices (e.g., activity trackers). This approach maximizes the ecological validity of findings, particularly because couple interactions that are prompted in the laboratory might differ from partner dynamics occurring at home (Laurenceau & Bolger, 2005). Consequently, an important extension of the existing literature would be to provide evidence for symptom-system fit in an everyday life context. Another benefit of daily life designs is the ability to investigate symptom-system fit as a dynamic process that operates within (in addition to between) couples (Scholz, 2019). Specifically, this allows capturing if the extent to which couples exhibit shared problematic behaviors on a given day covaries with relationship indicators such as feeling close to a partner or how satisfied partners are with their relationship that same day.
Research Overview and Hypotheses
The present research extends prior work on symptom-system fit by examining shared problematic behaviors and indicators of daily relationship functioning as they occur in daily life using data from three couple studies. Symptom-system fit is quantified by the extent to which shared problematic behaviors are associated with short-term benefits for the relationship. We focus on three different shared problematic behaviors that have been shown to be subject to social influence and that are highly correlated in couples (smoking, sedentary behavior, and unhealthy diets; Jeong & Cho, 2018; Meyler et al., 2007). Specifically, we analyzed data from three daily diary studies which collected information on shared problematic behaviors and daily relationship functioning for a period of 14 to 32 days with samples spanning different at-risk populations, ages, and geographical locations (Study 1: 82 Swiss couples who smoke aged 19 to 71 years; Study 2: 117 Swiss inactive couples with excess weight or obesity aged 22 to 75 years; and Study 3: 79 Canadian couples in which at least one partner had had a stroke aged 33 to 88 years).
In line with symptom-system fit theory (Rohrbaugh et al., 2002), we expected that couples would report higher closeness and relationship satisfaction on days when they engaged in more shared problematic behaviors (Research Question #1). The association between shared problematic behaviors and daily relationship functioning might be bidirectional. Engaging in shared problematic behaviors might enhance closeness, but couples might also be more likely to seek out shared problematic behaviors when they feel closer to each other. Thus, we further explored lagged relationships between the variables (Research Question #2). Hypotheses were preregistered at https://doi.org/10.17605/OSF.IO/69ZDE.
Method
This project analyzed existing data from three independently conducted couple studies (see Table 1 for an overview). Detailed information on study designs can be found in Lüscher et al. (2017) and Lüscher and Scholz (2017) for Study 1, Scholz and Berli (2014) and Berli et al. (2016) for Study 2, and Pauly et al. (2021) for Study 3.
Table 1.
An Overview of Study Characteristics.
| Characteristic | Study 1 | Study 2 | Study 3 |
|---|---|---|---|
| Target population | Couples who smoke | Inactive couples with excess weight or obesity | Couples with at least one partner having had a stroke |
| Time of data collection | February 2012 to June 2014 | March 2012 to June 2014 | March 2017 to November 2019 |
| Number of couples analyzed | 82 | 117 | 79 |
| Age | 19 to 71 years, M = 39 years | 22 to 75 years, M = 46 years | 33 to 88 years, M = 67 years |
| Relationship duration | M = 12 years | M = 19 years | M = 35 years |
| Study country | Switzerland | Switzerland | Canada |
| Daily diary design | 32 days | 28 days | 14 days |
| Shared problematic behavior | Assessed as self-reported number of cigarettes smoked together | Assessed as objectively measured shared sedentary behavior (hourly data aggregated over evenings on weekdays or all day on weekends) | Assessed as number of servings of foods high in fat, sugar, and/or salt that both partners reported (separately) in an evening food log |
| Individual problematic behavior | 7.5 cigarettes per day (SD = 5.3) | 3.6 hours sedentary per day (SD = 1.0; only evenings for weekdays) | 1.7 servings of foods high in fat, sugar, and/or salt per day (SD = 1.3) |
| Correlation of average individual problematic behavior between partners | r = .69, p < .001 | r = .80, p < .001 | r = .24, p = .003 |
| Average time spent together | M = 7.3 hrs per day, SD = 3.0 | M = 7.0 hrs per day, SD = 2.7 | n/a |
| ICC closeness | 0.27 | 0.43 | 0.52 |
| ICC relationship satisfaction | 0.31 | 0.45 | 0.50 |
Note. The ICC for binary outcomes in Study 1 reports the analysis of variance estimator. ICC = intraclass correlation.
Study 1
Participants and Procedure
The Study 1 sample consists of 82 mixed-gender couples who smoke aged 19 to 71 years (Mage = 39.0, SD = 14.5; 23% with college degree; M relationship duration = 11.8 years, SD = 12.5; Lüscher & Scholz, 2017). Participants resided in the German-speaking part of Switzerland 1 and were recruited via advertisements placed online and in newspapers, public advertisements, and a market research agency. During the time of the study, almost 30% of the Swiss population was smoking, with cigarette use being more prevalent among men versus women and among individuals with less education (Swiss Federal Statistical Office, 2020). Participants took part in two in-lab sessions, in between which they completed a 32-day daily diary protocol that included brief electronic surveys every evening (adherence: M = 27.2 completed diaries, SD = 5.5). During the first in-lab session, couples agreed on a jointly set quit date which fell on day 11 of the diary period. Participants gave written informed consent and received 100 Swiss Francs for completing the daily diary protocol. Ethics approval for the study was granted by the Faculty of Human Sciences Ethics Committee at the University of Bern, Switzerland.
Measures
Shared Problematic Behavior
Each day, participants reported the number of cigarettes they had smoked together with their partner (M = 3.6 cigarettes, SD = 3.7). From the original sample of 83 couples (cf. Lüscher et al., 2017), one couple was excluded because the partners never reported smoking any cigarettes together. This was done because including participants who have no variance on the day-level predictor can threaten the validity of multilevel analysis (Ram et al., 2017).
Daily Relationship Functioning 2
Daily closeness was measured each day by participants rating whether they felt not at all close (0) or very close (1) to their partner that day (M = 0.8, SD = 0.2; Impett et al., 2005; rbtwpartners = .28, p < .001). Daily relationship satisfaction was measured by asking participants to rate their experience of their relationship each day on a 3-point Likert-type scale ranging from 1 = horrible, 2 = ok, to 3 = wonderful (item adapted from the DAS-7; Hunsley et al., 2001). Because participants rarely endorsed the first answer option (4%), the two answer choices “horrible” and “ok” were collapsed, resulting in a dichotomous answer format (0 = horrible or ok, 1 = wonderful; M = 0.4, SD = 0.3; rbtwpartners = .31, p < .001).
Study 2
Participants and Procedure
Study 2 uses data from 117 mixed-gender couples aged 22 to 75 years (Mage = 45.9, SD = 13.7; 25% with a college degree; M relationship duration = 18.9 years, SD = 14.3) from the German-speaking part of Switzerland who were inactive and had excess weight or obesity and took part in a randomized controlled trial (study protocol: Scholz & Berli, 2014; main findings: Berli et al., 2016). Participants were recruited through advertisements in newspapers and on webpages, flyers, and mailing lists and assigned to one of two experimental groups: an intervention group (n = 58 couples) or a control group (n = 59 couples). At a baseline assessment, participants completed questionnaires, were equipped with technical devices, and received information about physical activity recommendations for adults. Participants of the intervention group were asked to set specific behavioral goals as part of the intervention. The following day, participants started a 28-day diary period during which they wore accelerometers and completed short end-of-day surveys. For the initial 14 days, participants of the intervention group received a brief action control text message every weekday. Adherence to the daily protocol was high (average completion rate: 26.3 days out of 28, SD = 4.1). Participating couples received 100 Swiss Francs for completing the diary study. The study was approved by the institutional review board of the Faculty of Human Sciences of the University of Bern, Switzerland, and participants gave full informed consent.
Measures
Shared Problematic Behavior
Physical activity was assessed using triaxial GT3X+ monitors (ActiGraph, Pensacola, FL). Using the ActiLife 6 software, sedentary behavior was calculated for every waking hour, using a cut-point of <150 cpm (Carr & Mahar, 2012). In the next step, we removed hours of the day in which the device was not worn for a duration of 60 min (14% of hours) and deleted days on which partners did not have at least 10 hr of joint valid wear time (19% of days), with non-wear time being defined as ≥90 min of no detected movement (Choi et al., 2011). An indicator of hourly shared sedentary behavior was created, denoting the lowest common denominator of sedentary time (e.g., if one partner had 40 min and the other partner had 30 min of sedentary time in a particular hour, shared sedentary behavior was 30 min). To aggregate data on the day level, shared sedentary behavior was averaged over the evening hours (later than 5 pm) for weekdays and over all available waking hours for weekend days (M = 3.0 hrs/day, SD = 0.9). This was done to account for the fact that daytime sedentary behavior on a weekday may be performed as part of work. Of the 121 couples who participated in the trial (cf. Berli et al., 2016), one couple dropped out and data of three couples were excluded during data cleaning because physical activity devices were swapped between partners (n = 1), one partner was missing physical activity data (n = 1), or no shared sedentary time was recorded (n = 1; Ram et al., 2017).
Daily Relationship Functioning
To measure daily closeness, each evening participants rated how close they felt to their partner, on a 5-point Likert-type scale ranging from 1 = today not at all close to 5 = today very close (M = 3.7, SD = 0.7; Impett et al., 2005; rbtwpartners = .40, p < .001). Daily relationship satisfaction was measured by asking how participants experienced their relationship today on a 7-point Likert-type scale from 1 = today horrible to 7 = today wonderful (M = 5.2, SD = 0.9; Hunsley et al., 2001; rbtwpartners = .42, p < .001).
Study 3
Participants and Procedure
The sample of Study 3 comprised 79 mixed-gender couples aged 33 to 88 years (Mage = 66.9, SD = 10.4; 34% with college degree; M relationship duration: 34.8 years, SD = 16.3) from Southern British Columbia, Canada, with at least one partner having a history of stroke. On average, the stroke had happened 4.7 years prior to participation (range: 0–30 years, SD = 6.1). Participants were recruited via advertisements in public spaces and online, talks at stroke recovery groups, and contacting participants of stroke recovery programs. The study focused on health behaviors in couples post stroke and included a baseline session, a 14-day daily diary period, and an exit session. As part of the 14-day observational period, participants completed morning surveys, evening surveys, and took pictures of their food intake. Participants showed good adherence to the daily diary protocol (M = 12.6 completed diaries out of 14, SD = 2.6). For reimbursement, participants had the choice to keep one tablet per couple or receive CAD $100 each instead. The study was ethics approved by the University of British Columbia, Canada and participants provided informed consent.
Measures
Shared Problematic Behavior
Throughout the 14-day diary period, participants were asked to take pictures of all foods and drinks they consumed. Each evening, participants were instructed to revisit the pictures they took that day to complete a nutrition log. Specifically, they were told:
We are interested in how many servings of foods high in fat, sugar or salt you had. For example, this could be chocolate, pastries, chips, pizza, or ice cream. Most premade meals are high in salt as well. About ½ cup of those kinds of food is one serving.
Servings of shared unhealthy foods were calculated as the minimum number of servings that was recorded by both partners each day (M = 1.0, SD = 0.8). From 86 couples providing daily diary data (cf. Pauly et al., 2021), seven couples were excluded because they reported no shared unhealthy food consumption (Ram et al., 2017).
Daily Relationship Functioning
To indicate daily closeness, participants responded to the question “How close did you feel to your partner today?” each evening on a visual-analogue scale, ranging from 0 (“not at all”) to 100 (“very much”; M = 78.7, SD = 15.8; rbtwpartners = .31, p < .001). Using the same response scale, participants also reported how satisfied they were with their relationship with their partner today (daily relationship satisfaction; M = 80.5, SD = 14.9; rbtwpartners = .30, p < .001).
Statistical Analyses
Mixed models were used to account for the interdependence among couple members’ daily observations, using a two-intercept, two-level statistical model for distinguishable dyads as indicated for heterosexual couples (Bolger & Laurenceau, 2013). Because Study 1 outcomes were binary, data were analyzed in the R software (R Core Team, 2020) using binomial generalized linear mixed models (glmmTMB package, Brooks et al., 2017). Data from Study 2 and 3 were analyzed using the nlme package in R (Pinheiro et al., 2020). All models accounted for auto-correlation (lag1). Level 1 (i.e., day-level) predictors were within-person centered, and the person mean across the daily diary period was grand-mean centered and included as a covariate at Level 2 (i.e., the couple level). Models included random intercepts for men and women as well as the random slope for shared problematic behavior. As recommended by Bolger and Laurenceau (2013), study day was included as a covariate on the day level. In line with the preregistration and because these two variables have been associated with relationship functioning and behaviors that are related to health and well-being (Berrigan et al., 2003; Luong et al., 2011), models controlled for age and education. In addition, we controlled for the average amount of time couples spent together in Studies 1 and 2 (participants reported how many hours per day they usually spend with their partner on a workday; no data available for Study 3). In our analysis, symptom-system fit was indicated by the slope representing the strength of day-to-day associations between shared problematic behavior and daily relationship functioning. As this slope was treated as random, models estimated a separate symptom-system fit score for each participant for the two daily relationship functioning indicators (closeness and satisfaction).
For the exploratory analyses, we analyzed lead-lag relationships (i.e., bidirectional predictive effects) using multilevel dynamic structural equation models with days nested within persons (Asparouhov et al., 2018) in Mplus 8 (Muthén & Muthén, 1998–2017). Models (see S-Figure 1 in the online supplementary material) estimate autoregressive paths between measurement occasions, that is, the predictive effect of prior-day shared problematic behavior for next-day shared problematic behavior (α1) and the predictive effect of prior-day relationship functioning for next-day relationship functioning (β1). Importantly, models also estimate cross-lagged paths between variables on consecutive days, predicting current-day shared problematic behaviors by previous-day relationship functioning (α2) and current-day relationship functioning by previous-day shared problematic behaviors (β2). We used Bayes estimation with Mplus default diffuse priors and Markov Chain Monte Carlo (MCMC) algorithms. Separate models were estimated for male and female participants. Furthermore, for shared smoking we used a binary indicator (0 = no shared cigarettes that day, 1 = at least one shared cigarette that day) because models including a variable indicating the number of shared cigarettes had convergence issues due to violation of the stationarity assumption.
Statistical Power
We calculated statistical power to detect day-to-day associations between shared problematic behavior and relationship functioning using the simr package in R (Monte Carlo simulation; Green & MacLeod, 2016), following procedures suggested by Arend and Schäfer (2019). Assuming small standardized effect sizes (.10), a small standardized random slope variance (.01), and a medium intraclass correlation (ICC = .30), we had >85% power to detect a Level 1 effect in all studies (Study 1: 99.9%, Study 2: 99.9%, and Study 3: 86.4%).
Transparency and Openness
This project’s hypotheses and analytical plan (secondary analysis of existing data) were preregistered. Analysis scripts and full model results are available at https://osf.io/vmh6c/?view_only=588311d713d84991bc82890999f0e47a. The dependent nature of the data (couples) and the small sample size both constitute formidable risks that participants could be able to have their data identified by their partner. Thus, to protect participants’ confidentiality, data are available for researchers upon request only.
Results
Descriptive statistics and intercorrelations are described in Table 2. Older participants showed greater shared problematic behavior in Study 2 (i.e., sedentary behavior; r = .29, p < .001) and reported higher average closeness in Study 3 (r = .18, p = .024) and lower relationship satisfaction in Study 1 (r = –.23, p = .005). Average levels of closeness and relationship satisfaction were highly correlated within participants in all studies (rs = .66–.94, ps < .001).
Table 2.
Means, Standard Deviations, and Intercorrelations of Central Study Variables (Study 1: N = 82 Couples, Study 2: N = 117 Couples, Study 3: N = 79 Couples).
| Variable | Study 1, M (SD) | Study 2, M (SD) | Study 3, M (SD) | 1 Study 1/2/3 |
2 Study 1/2/3 |
3 Study 1/2/3 |
4 Study 1/2/3 |
5 Study 1/2/3 |
|---|---|---|---|---|---|---|---|---|
| 1. Age | 39.04 (14.54) | 45.91 (13.76) | 66.92 (10.42) | .95**/.94**/.88** | –.02/.00/–.03 | .07/.29**/–.08 | –.09/–.02/.18* | –.23**/–.09/.11 |
| 2. Education (college degree) | 23% | 25% | 34% | .25**/.23*/.31* | .17*/–.01/–.11 | .08/–.04/–.05 | .07/–.03/–.04 | |
| 3. Shared problematic behavior | 3.62 (3.75) | 2.97 (0.86) | 1.03 (0.78) | n/a | .14/.01/–.01 | .11/.02/–.03 | ||
| 4. Daily closeness | 0.78 (0.23) | 3.69 (0.67) | 78.65 (15.79) | .48**/.46**/.36** | .66**/.94**/.90** | |||
| 5. Daily relationship satisfaction | 0.43 (0.29) | 5.24 (0.91) | 80.49 (14.91) | .51**/.45**/.41** |
Note. Daily measures were aggregated to person-level means. Shared problematic behavior is shared smoking (number of cigarettes per day) in Study 1, shared sedentary behavior (hours per day) in Study 2, and shared consumption of unhealthy foods (servings of foods high in fat, sugar, and/or salt per day) in Study 3. Daily closeness scored from 0 to 1 in Study 1, from 1 to 5 in Study 2, and from 0 to 100 in Study 3. Daily relationship satisfaction scored from 0 to 1 in Study 1, from 1 to 7 in Study 2, and from 0 to 100 in Study 3. Correlations between partners are presented in the diagonal.
p < .05. **p < .01.
Same-Day Associations Between Shared Problematic Behavior and Relationship Functioning in Daily Life
Results from mixed models examining symptom-system fit with respect to shared smoking (Study 1), shared sedentary behavior (Study 2), and shared unhealthy diet (Study 3) can be found in Table 3. As expected, partners were more likely to report high closeness on days on which they shared a greater number of cigarettes with each other (b = 0.25/0.20, standard error [SE] = 0.04/0.04, p < .001 for men/women; see Figure 1). Furthermore, partners were more likely to report high relationship satisfaction on days on which they smoked more cigarettes together (b = 0.18/0.21, SE = 0.03/0.04, p < .001). On the couple level, men who smoked more cigarettes together with their partner reported higher average closeness (b = 0.24, SE = 0.09, p = .010) and satisfaction (b = 0.14, SE = 0.07, p = .041), as compared with men who smoked less cigarettes together with their partner.
Table 3.
Results From Mixed Models Examining Daily Closeness and Relationship Satisfaction (Study 1: N = 82 Couples, Study 2: N = 117 Couples, Study 3: N = 79 Couples).
| Variable | Study 1 | Study 2 | Study 3 | |||
|---|---|---|---|---|---|---|
| Daily closeness: b (SE) | Daily relationship satisfaction: b (SE) | Daily closeness: b (SE) | Daily relationship satisfaction: b (SE) | Daily closeness: b (SE) | Daily relationship satisfaction: b (SE) | |
| Fixed effects male/female | ||||||
| Intercept | 2.33*** (0.34)/ 2.06*** (0.36) | –1.29*** (0.28)/ –0.88*** (0.32) | 3.55*** (0.22)/ 3.50*** (0.23) | 5.00*** (0.31)/ 5.06*** (0.30) | 78.06*** (2.27)/ 74.61*** (2.28) | 81.11*** (2.03)/ 77.55*** (2.22) |
| Daily shared problematic behavior |
0.25*** (0.04)/
0.20*** (0.04) |
0.18*** (0.03)/
0.21*** (0.04) |
0.06*** (0.01)/
0/06*** (0/01) |
0.07*** (0.01)/
0.07*** (0.01) |
0.74 (0.83)/ 1.16 (0.77) |
–0.23 (0.87)/ 0.49 (0.70) |
| Person mean shared problematic behavior |
0.24** (0.09)/
0.01 (0.08) |
0.14* (0.07)/ 0.01 (0.07) |
0.01 (0.01)/ 0.01 (0.01) |
0.01 (0.01)/ 0.01 (0.01) |
0.33 (2.19)/ –0.47 (2.38) |
0.07 (1.96)/ –0.99 (2.34) |
| Random effects male/female | ||||||
| Intercept person | 2.05***/ 2.31*** | 1.93***/ 2.32*** | 0.57***/ 0.59*** | 0.81***/ 0.77*** | 14.02***/ 15.69*** | 12.34***/ 15.35*** |
| Daily shared problematic behavior | 0.18***/0.11*** | 0.13***/0.17*** | 0.05***/0.07*** | 0.08***/0.10*** | 4.17***/3.52*** | 4.76***/2.80*** |
| Correlation intercept male/female | 0.57*** | 0.68*** | 0.39*** | 0.34*** | 0.39*** | 0.51*** |
| Residual | n/a | n/a | 0.72*** | 0.93*** | 14.44*** | 14.25*** |
| R 2 m / R 2 c | 0.25/0.69 | 0.19/0.66 | 0.10/0.46 | 0.10/0.48 | 0.03/0.54 | 0.02/0.51 |
Note. Models for Study 1 are based on 4396 observations nested within 82 couples. Models for Study 2 are based on 4547 observations nested within 117 couples. Models for Study 3 are based on 1855 observations nested within 79 couples. Models control for study day, age, and education in Studies 1–3, and average time spent together in Studies 1 and 2 (no data for Study 3). Coefficients <|0.01| were rounded to 0.01 and −0.01. Bold font denotes significant coefficients. R2m = marginal R squared (variance explained by fixed effects). R2c = conditional R squared (variance explained by fixed and random effects).
p < .05. **p < .01. ***p < .001.
Figure 1.

Associations of Shared Problematic Behaviors With Daily Closeness and Relationship Satisfaction.
Note. The figure shows associations of shared problematic behavior (panels a/b: shared smoking; panels c/d: shared sedentary behavior; panels e/f: shared consumption of unhealthy foods) with daily closeness and relationship satisfaction. Gray areas depict confidence bands around the estimated slopes. Wpc = within-person centered. It can be obtained that higher levels of shared problematic behaviors were associated with higher daily closeness and relationship satisfaction among partners in Study 1 and Study 2.
Study 2 replicated these findings, showing that partners reported higher closeness on days on which they exhibited greater shared sedentary behavior (b = 0.06/0.06, SE = 0.01/0.01, p < .001 for men/women; Figure 1). They also reported higher relationship satisfaction on these days (b = 0.07/0.07, SE = 0.01/0.01, p < .001 for men/women; Figure 1). Contrary to expectations, partners’ daily reports of closeness and relationship satisfaction did not differ on days when they jointly consumed more or less unhealthy foods (Study 3, see Table 3 and Figure 1).
Random slopes indicated that participants significantly differed in the extent to which they showed symptom-system fit with respect to smoking (closeness: σ = 0.18/0.11, p < .001 for men/women, relationship satisfaction: σ = 0.13/0.17, p < .001) and sedentary behavior (closeness: σ = 0.05/0.07, p < .001, relationship satisfaction: σ = 0.08/0.10, p < .001). Please see Figure 2 for a graphical display of participants’ variation in their symptom-system fit indices. For most participants, shared problematic behavior was positively associated with daily relationship functioning, whereas only a small number of partners was estimated to exhibit a negative correlation in Study 1 (closeness: 0.6%, satisfaction: 2.4%) and Study 2 (closeness: 2.1%; satisfaction: 6.8%). Partners who showed symptom-system fit for one outcome (daily closeness) were also more likely to show symptom-system fit for the other outcome (daily relationship satisfaction: Study 1: r = .29, p < .001; Study 2: r = .77, p < .001).
Figure 2.
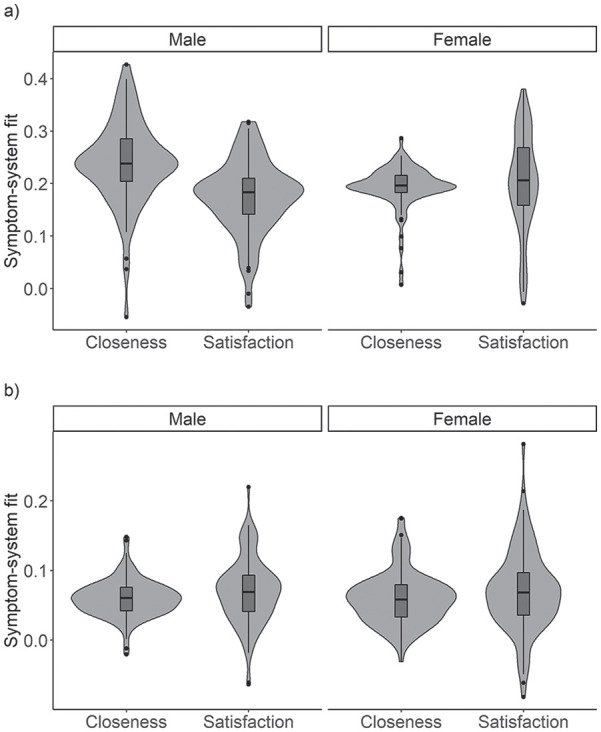
Variation in Symptom-System Fit Between Participants.
Note. The figure demonstrates the distribution of symptom-system fit between male and female participants; boxplots are displayed in dark gray within the violin plots. Panel a shows differences in how strongly shared smoking was associated with daily closeness or relationship satisfaction (both scored out of 1); panel b shows differences in how strongly shared sedentary behavior was associated with daily closeness (scored out of 5) or relationship satisfaction (scored out of 7). It can be obtained that for most participants, shared problematic behavior was positively associated with daily relationship functioning.
Sensitivity Analyses
Because participants in Study 1 were asked to quit smoking on day 11 of the daily diary phase, we tested whether findings hold when controlling for the study phase (0 = before quit date, 1 = after quit date). Findings did not differ when including the study phase as a covariate. We also tested whether symptom-system fit differed prior to as compared with after the quit date. We did not find any differences in associations of shared smoking with daily closeness or relationship satisfaction before (day 1 to 10), as compared with after (day 11 to day 32) the quit date. For further sensitivity analyses in Study 1, we included a covariate that indicated the number of cigarettes smoked by oneself without a partner. The pattern of findings does not change.
For Study 2, we conducted sensitivity analyses with respect to participants being part of the intervention or control group. Findings did not differ when including group membership (0 = control group, 1 = intervention group) as a covariate nor were there any significant differences in symptom-system fit between groups. Findings also remain the same if models are run including only couples in the control group (n = 59 out of 117 couples). For further sensitivity analyses in Study 2, we included a covariate that indicated whether participants were employed in jobs that might include after-hours work (e.g., working in the hospital or as a truck driver; 11.7% of participants). The pattern of results remains unchanged.
For Study 3, participants were asked to not just self-report their food intake but they also took pictures of everything they consumed. Four trained research assistants coded the pictures for shared unhealthy food consumption (i.e., whether participants were eating the same unhealthy foods). Analyses using this variable to predict daily closeness and relationship satisfaction also yielded non-significant findings for symptom-system fit with respect to shared unhealthy diet (equivalent to the self-report).
Lagged Associations Between Shared Problematic Behavior and Daily Relationship Functioning
Findings from multilevel dynamic structural equation models examining autoregressive and cross-lagged associations between shared problematic behaviors and daily relationship functioning can be found in Table 4 for Studies 1 and 2 and Supplementary Table S1 in the online supplementary material for Study 3. In Study 1, there were significant autoregressive effects of shared smoking (bs = 0.71–0.75, SD’s = 0.03–0.06, p <.001). Furthermore, previous-day relationship functioning statistically predicted next-day relationship functioning (bs = 0.13–0.18, SD = 0.05, ps <.001–.017) with the exception of the autoregressive parameter not being significant for closeness in male participants. With respect to cross-lagged parameters, men and women more likely reported high relationship satisfaction following days when they had smoked together (b = 0.14/0.16, SD = 0.05/0.05, p < .001 for men/women). Men also more likely reported high closeness on these days (b = 0.23, SE = 0.07, p < .001). The reverse temporal direction (previous-day relationship functioning predicting later shared problematic behavior) was not significant for daily relationship satisfaction and only significant in women for daily closeness (b = −0.11, SE = 0.05, p < .001).
Table 4.
Results From Dynamic Structural Equation Models Including Shared Problematic Behavior and Daily Relationship Functioning (Study 1: N = 82 Couples, Study 2: N = 117 Couples).
| Study 1 | Study 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Closeness | Relationship satisfaction | Closeness | Relationship satisfaction | |||||
| Variable | b (Posterior SD) | 95% CI [LL; UL] | b (Posterior SD) | 95% CI [LL; UL] | b (Posterior SD) | 95% CI [LL; UL] | b (Posterior SD) | 95% CI [LL; UL] |
| Autoregressive paths male/female | ||||||||
| Shared Probl. Behavior t–1
– Shared Probl. Behaviort (α1) |
0.74 (0.06)/ 0.72 (0.03) |
[0.62, 0.83]/ [0.66, 0.79] |
0.75 (0.04)/ 0.71 (0.05) |
[0.67, 0.83]/ [0.60, 0.78] |
0.24 (0.02)/ 0.24 (0.02) |
[0.19, 0.28]/ [0.19, 0.28] |
0.24 (0.02)/ 0.24 (0.02) |
[0.20, 0.29]/ [0.20, 0.28] |
| Daily Rel. Functioningt–1
– Daily Rel. Functioningt (β1) |
0.02 (0.06)/ 0.13 (0.05) |
[–0.12, 0.13]/ [0.01, 0.22] |
0.13 (0.05)/ 0.18 (0.05) |
[0.03, 0.23]/ [0.09, 0.29] |
0.17 (0.02)/ 0.21 (0.03) |
[0.13, 0.22]/ [0.15, 0.25] |
0.16 (0.02)/ 0.20 (0.03) |
[0.12, 0.21]/ [0.15, 0.25] |
| Cross-lagged paths male/female | ||||||||
| Daily Rel. Functioningt–1
– Shared Probl. Behaviort (α2) |
–0.08 (0.05)/ –0.11 (0.05) |
[–0.17, 0.03]/ [–0.20, –0.02] |
–0.05 (0.04)/ –0.06 (0.04) |
[–0.14, 0.02]/ [–0.14, 0.04] |
0.01 (0.02)/ –0.01 (0.03) |
[–0.04, 0.06]/ [–0.07, 0.03] |
0.02 (0.02)/ –0.01 (0.02) |
[–0.02, 0.07]/ [–0.06, 0.03] |
| Shared Probl. Behaviort–1
– Daily Rel. Functioningt (β2) |
0.23 (0.07)/ 0.07 (0.05) |
[0.06, 0.34]/ [–0.04, 0.17] |
0.14 (0.05)/ 0.16 (0.05) |
[0.04, 0.23]/ [0.06, 0.28] |
0.06 (0.02)/ 0.08 (0.02) |
[0.02, 0.11]/ [0.03, 0.12] |
0.07 (0.03)/ 0.07 (0.02) |
[0.02, 0.12]/ [0.03, 0.11] |
| Residual variances within male/female | ||||||||
| Shared Probl. Behavior | n/a | n/a | n/a | n/a | 0.91/0.91 | [0.87, 0.94]/ [0.87, 0.94] |
0.90/0.90 | [0.86, 0.94]/ [0.87, 0.94] |
| Daily Rel. Functioning | n/a | n/a | n/a | n/a | 0.81/0.78 | [0.78, 0.84]/ [0.74, 0.81] |
0.79/0.77 | [0.76, 0.82]/ [0.73, 0.81] |
| Within-level R2 male/female | ||||||||
| Shared Probl. Behavior | .63/.63 | [.51, .71]/ [.57, .71] |
.64/.62 | [.55, .73]/ [.54, .69] |
.09/.09 | [.06, .13]/ [.06, .13] |
.10/.10 | [.06, .14]/ [.06, .13] |
| Daily Rel. Functioning | .28/.25 | [.22, .35]/ [.18, .31] |
.25/.28 | [.19, .30]/ [.22, .34] |
.18/.22 | [.16, .22]/ [.19, .26] |
.21/.23 | [.18, .24]/ [.19, .27] |
Note. Results from Mplus MCMC Bayes estimation, significance (in bold) is based on the Credibility Interval (CI) not containing zero. b = averaged individually standardized estimate; CI = credibility interval; LL = lower level; UL = upper level; Probl. = problematic; Rel. = relationship.
In Study 2, shared sedentary behavior (b = 0.24, SD = 0.02, p <.001), daily closeness (b’s = 0.17–0.21, SD = 0.02, p <.001), and daily relationship satisfaction (bs = 0.16–0.20, SD’s = 0.02 to 0.03, p <.001) showed significant autoregressive effects over time. With respect to cross-lagged parameters, men and women reported higher closeness (b = 0.06/0.08, SD = 0.02/0.02, p = .004/.001 for men/women) and higher relationship satisfaction (b = 0.07/0.07, SD = 0.02/0.02, p = .001/<.001 for men/women) following days with greater shared sedentary behavior. There was no evidence for the reverse temporal association, that is, previous-day closeness or relationship satisfaction predicting next-day shared sedentary behavior.
In Study 3, auto-regressive parameters were significant for shared consumption of unhealthy foods (bs = 0.16–0.17, SD’s = 0.05 to 0.06, ps <.001–.001), daily closeness (bs = 0.27–0.29, SD’s = 0.05–0.06, ps = .001–.002), and daily relationship satisfaction (bs = 0.27–0.29, SD’s = 0.05–0.06, ps = .001–.002). All cross-lagged parameters were not significant.
Discussion
Three studies observed shared problematic behaviors and daily relationship functioning in the everyday lives of mixed-gender couples for a 14- to 32-day period. Two studies provided evidence for our hypothesis that on days when couples engage in more shared problematic behaviors, they also report higher closeness and higher relationship satisfaction (Study 1: smoking and Study 2: sedentary behavior). No evidence for symptom-system fit was found in the third study with a different type of sample and a different focus on behavioral risk, namely, shared consumption of unhealthy foods in adults who have experienced a stroke and their partners. Our second question regarding lagged associations was tested with exploratory analyses and revealed, again for Study 1 and 2, stronger evidence for prior-day shared problematic behavior linking with next-day relationship functioning than prior-day relationship functioning linking with next-day shared problematic behavior.
Recall that we had hypothesized that one explanation for individuals engaging in behaviors that are bad for them in the long term might be that they are guided by relationship motives. Symptom-system fit theory suggests that shared problematic behavior in romantic partners is a symptom that fits within and serves the larger system (the couple) because it is associated with benefits for the relationship on a short-term timeframe, for example, by promoting a temporary sense of unity with the partner or enhancing other relationship parameters (Rohrbaugh et al., 2002; Shoham et al., 2007). Prior research on symptom-system fit has been confined to a limited number of shared problematic behaviors, has mostly indirectly measured relationship functioning, and has been conducted in the laboratory. Our study addresses these important research gaps by investigating symptom-system fit with respect to three different shared problematic behaviors in a daily life context. Importantly, we examined the proposed theoretical mechanism at the level at which it is thought to occur, that is, within couples, by linking everyday shared problematic behaviors with concurrent changes in indicators of positive relationship functioning. In the following, we discuss how our novel results both replicate and extend the existing literature on social dynamics and problematic behaviors and suggest directions for future study.
Why Couples Engage in Shared Problematic Behavior
When choosing romantic partners, individuals tend to be drawn to people who are similar to them (assortative mating; Luo, 2017). Over time, partners often become even more similar to each other, which can partly be explained by social learning processes, exposure to similar environments, and shared resources (Ask et al., 2013). However, shared (problematic) behaviors might also be purposely sought out based on relationship-specific motives. What is it about problematic behaviors in particular that makes individuals use them to create or maintain a romantic bond? One explanation might be that these types of behaviors are often viewed as “indulgent” (e.g., Taylor et al., 2014). Problematic behaviors have hedonic, pleasurable short-term effects but also carry long-term harm for health and well-being. The joint engagement in recreational activities helps strengthen and stabilize the relationship, in part because it allows partners to share positive emotions (Girme et al., 2014; Walsh et al., 2017). Shared novel, exciting activities are thought to be particularly beneficial for relationship functioning because of their “risky” or “arousing” nature, deviating from security and routine (e.g., trying out a new restaurant not knowing if the food is good; Aron et al., 2000; Harasymchuk et al., 2021). It is also possible that the willingness to put up with long-term health or well-being risk when engaging in shared problematic behavior with the partner may make “indulging together” a unique experience that brings partners closer. Future research could test this assumption by examining whether subjective perceptions of the “riskiness” of the problematic behavior moderate symptom-system fit.
Another motive that may cause couples to engage in shared problematic behaviors could be emotion regulation. Problematic behaviors, including alcohol consumption, smoking, or eating comfort foods are often used to relieve stress or reduce negative affect (Cooper et al., 1995; Dalton & Hammen, 2018). In the couple context, individuals might choose to engage in these behaviors with their significant other because they want to improve their own or their partner’s affective well-being or because it helps them regulate negative emotionality that exists between them (e.g., to distract from interpersonal tension, avoid conflict; Skoyen et al., 2013, 2014).
Of note, the problematic behaviors considered in the three studies varied along the continuum of shared problematic behaviors described in the introduction. Study 1 directly asked about a specific behavior that couples engaged in together at the same time and in the same space (smoking a cigarette together), whereas Studies 2 and 3 measured behaviors occurring in the same timeframe (same hour: Study 2, same day: Study 3) that may or may not have been exactly the same (e.g., both partners engaging in sedentary activities that are slightly different) or done in the same space. It is an empirical question where the critical threshold of the sharedness spectrum is situated. What constitutes the same or similar behaviors? For example, one partner watching TV and the other partner scrolling through social media on their phone (shared sedentary activities) might operate differently than one partner smoking and the other partner drinking alcohol (shared substance use). In addition, what counts as shared time? Does the behavior need to occur in the same hour, on the same day, within the same week? Finally, does shared space mean engaging in the shared behavior in the same room, the same house, or even virtually in the same space? Future studies could use objective measures of the physical proximity of partners (e.g., via bluetooth) and need to test whether associations with daily relationship functioning are stronger for behaviors that are higher up on this continuum of shared behaviors.
In the current studies, we investigated three different shared problematic behaviors: smoking, sedentary behavior, and unhealthy diet. Symptom-system fit theory does not make behavior-specific predictions. Yet, each of these three shared problematic behaviors might play a very distinct and idiographic role in the couple relationship, which we discuss in the following.
Differences in Symptom-System Fit by the Behavior Under Study
Study 1
In Study 1, we found that couples were more likely to report high closeness and relationship satisfaction on days on which they smoked more cigarettes together. Behaviors that can lead to physiological dependence such as smoking and alcohol consumption might be more likely to be shared in couples due to conditioning effects: The more often partners smoke together, the more they might serve as each other’s social cue to light up a cigarette (Dimoff & Sayette, 2017). Furthermore, any reinforcement that occurs due to immediate relationship benefits (such as intimacy with the partner) could be particularly pronounced when it comes to addictive substances (Testa et al., 2019). Smoking is a behavior that is highly interdependent in couples; individuals are over three times more likely to smoke if their partner smokes (Di Castelnuovo et al., 2009). It could be that being a dual-smoker couple becomes engrained in the couple’s identity (Doherty & Whitehead, 1986). A shared identity, which is created through blurred boundaries between the self and the partner, is thought to be essential for positive relationship functioning and predicts commitment as well as relationship maintenance (Aron & Fraley, 1999; Branand et al., 2019). Thus, smoking cigarettes together might serve to activate this cognitive representation of being alike and “we-ness,” thereby increasing self-other overlap and closeness. Future studies on symptom-system fit are needed to test the role of biological dependence and shared identity for smoking behavior in couples.
Study 2
Extending Study 1 findings on smoking, we found that days with more shared sedentary behavior (as assessed by an activity monitoring device) were linked with increased closeness and relationship satisfaction in inactive couples with excess weight or obesity. Our study did not measure what kind of activities couples engaged in during shared sedentary time, which could comprise eating meals together or shared sedentary leisure activities (e.g., watching TV or other media and screen-based pastimes; Gomillion et al., 2017). Shared sedentary activities might create opportunities to unwind and connect as a couple, and time that is spent in each other’s presence while feeling relaxed could put couples in a state of mind that more likely leads to positive appraisals of one’s relationship (Finucane & Horvath, 2000; Padilla-Walker et al., 2019). Moreover, engaging in relaxing activities as a couple could enable physical intimacy (e.g., cuddling up on the couch together while watching a show), thereby enhancing closeness (Gomillion et al., 2017). Shared media consumption could also facilitate communication in couples, for example, by prompting an exchange about issues raised in the media content (Alberts et al., 2005); these elicited conversations could, in turn, help build intimacy. Conversely, media consumption could be a way to avoid discussing conflict-ridden topics or could cover up a lack of other shared interests. Thus, it would be an important extension of the current study to examine what couples do when being sedentary together and to identify which kind of couple dynamics need to be targeted when trying to reduce sedentary time.
Study 3
In couples after stroke (Study 3), we did not find any differences in daily closeness or relationship satisfaction on days on which couples reported more or less shared unhealthy food consumption. This is rather surprising given that prior literature gives ample reason to speculate on the existence of symptom-system fit with respect to shared unhealthy foods, highlighting the role of food consumption for social bonding (Alley et al., 2013; Gregersen & Gillath, 2020). For example, the sharing of food is thought to be an important indicator of relationship closeness because it signals caretaking behavior and increases intimacy (Alley et al., 2013). One reason for the nonsignificant findings could be that we assumed that any reported servings of unhealthy foods in the evening diary that matched the partner’s report were consumed together, although this could have happened at different times throughout the day. Furthermore, an accurate measure of shared servings of foods high in fat, sugar, and/or salt could have been biased by partners differing in their understanding of what type of foods fall into the category of being high in fat, sugar, and/or salt and in their understanding of what a “serving size” comprises (which was instructed as half a cup). Consequently, future studies could build on our findings using other methods to measure dietary intake such as food records, in which participants explicitly report which foods were shared with the partner.
Study 3 differed from Studies 1 and 2 (cf. Table 1) in that the samples of Studies 1 and 2 were from a different country, younger, had a shorter average relationship duration, and had formed an intention to change their problematic behavior. Thus, Study 3 findings might have been more strongly influenced by ceiling effects because older participants’ relatively high levels of relationship functioning fluctuated less from day to day. It could also be that symptom-system fit might be a couple dynamic that is more prevalent in younger adults or in those with shorter relationship duration because behavioral patterns are less established and more subject to social motivations. Furthermore, problematic behaviors might exert their positive effects on relationship functioning due to their “risky” or “indulgent” nature. This effect might have been particularly pronounced in Studies 1 and 2 whose participants joined a study targeted at changing the respective behavior, enhancing the experience of a shared engagement in a “forbidden” activity. Average levels of smoking and sedentary behavior were highly correlated between partners (r = .69 and .80, respectively), whereas the correlation was only small to medium-sized for unhealthy diet (r = .24). Consequently, it might also be that the former behavior is less likely part of a shared couple identity. Finally, the three behaviors differ in their underlying agency. Sitting and smoking are behaviors that individuals can voluntarily choose to engage in, or not. Eating, however, is necessary for survival, and one partner of the couple might take the main responsibility for providing food (e.g., by shopping and cooking). This might make it less likely that partners’ joint consumption of certain foods is guided by relationship motives.
Lagged Associations Between Shared Problematic Behavior and Daily Relationship Functioning
Symptom-system fit theory proposes that couples are motivated to engage in shared problematic behaviors because they have subsequent benefits for the relationship, such as increasing closeness (Rohrbaugh et al., 2002; Shoham et al., 2007). Thus, a causal pathway from shared problematic behavior to better short-term relationship functioning is assumed. However, one may also imagine that the opposite causal direction could apply. For example, when partners feel closer to each other, they might be more motivated to engage in activities together, including shared problematic behaviors. In our exploratory analyses examining these two predictive directions, we found more support for the former as compared to the latter pathway. Specifically, prior-day engagement in shared smoking and shared sedentary behavior statistically predicted next-day closeness and relationship satisfaction (the cross-lagged association between shared smoking and closeness was only significant in male partners). Conversely, prior-day closeness or relationship satisfaction was not associated with next-day shared smoking or shared sedentary behavior with one exception: Female partners were less, not more, likely to report shared smoking on days following high closeness. Future research could build on our findings by investigating lead-lag associations of shared problematic behavior and relationship functioning in finer time resolution (e.g., with hourly assessments), and explore the underlying mechanisms, for example, by also assessing relationship-specific motivations for engaging in certain problematic behaviors.
Study Limitations and Future Directions
Findings from our studies are correlational and need to be supplemented with experimental research. In addition, we assessed daily relationship functioning using only one item each to indicate closeness and relationship satisfaction, to limit participant burden in the daily diary design. Future research could build on our findings by including more comprehensive measures of daily relationship quality and shared problematic behaviors, also extending the investigation to different (non health-related) behaviors, including excessive gaming, problematic online buying, and other high-risk activities. We also acknowledge that relationship satisfaction shows limited variability on a daily level, particularly in long-term relationships (Totenhagen et al., 2016). The way daily relationship functioning is measured (which was different across the three studies; e.g., 7-point Likert-type scale vs. 0–100 slider scale) can influence the extent to which responses vary within persons and should be carefully considered in future study designs.
A limitation with respect to our samples is that all three studies recruited from at-risk populations (couples who smoke, inactive couples with excess weight or obesity, couples in which one partner has had a stroke). Thus, it remains an open question whether findings generalize to couples who do not exhibit these risk profiles. Furthermore, in two of the studies couples were part of a behavior change intervention. Consequently, findings might not represent how these couples would have behaved outside of the intervention setting. Also, we solely examined mixed-gender couples. As there is an indication that behavioral concordance might be more pronounced among same-gender as compared with mixed-gender marriages (Holway et al., 2018), future research needs to replicate our findings among other union types. Our participants had been with their partner for a very long time, on average. Longitudinal research is needed to examine how symptom-system fit evolves from relationship initiation and how and under what circumstances it exerts positive or negative influences on long-term individual and relationship outcomes. Future research could also examine if the shared problematic behaviors develop over time or are part of the initial couple culture. If the problematic behaviors are part of the assortative mating process instead of developing over time after relationship formation, they might be differently related to the couple’s identity. Replacing these problematic behaviors with beneficial behaviors might need different intervention approaches.
While we present evidence for the immediate relationship benefits of problematic behaviors in the short-term, future research needs to test associations of shared problematic behaviors with long-term relationship quality. On the one hand, repeated engagement in pleasurable shared activities and accumulation of transient increases in positive relationship parameters (e.g., closeness) could promote relationship quality over time (Girme et al., 2014; Walsh et al., 2017). Thus, couples who exhibit greater symptom-system fit might report higher long-term relationship quality. On the other hand, some couples might choose to engage in shared problematic behavior as a replacement for another, negative interpersonal behavior, relieve relationship distress, or escape a negative interpersonal situation (such as having an argument; Skoyen et al., 2013). The use of shared problematic behaviors to prevent negative interpersonal dynamics could undermine long-term relationship functioning (Rohrbaugh et al., 2002).
Finally, future research could shed light on moderating factors of symptom-system fit. For example, relationship-specific or general self-esteem has been linked to relationship dynamics and problematic behaviors (Hamilton & DeHart, 2017; Mund et al., 2015). Specifically, individuals low in self-esteem might turn to problematic behaviors such as drinking alcohol more often in response to relationship difficulties (Hamilton & DeHart, 2017). What is not known is whether low self-esteem or feelings of insecurity in the relationship could also drive couples to engage in more shared problematic behaviors because they feel a higher need to affirm relationship stability.
Conclusion
The current research advances our understanding of problematic behavior from a social perspective by demonstrating how shared problematic behavior in couples might maintain and be maintained by its relationship function. Results suggest that shared problematic behaviors with the partner including shared smoking and shared sedentary behavior go along with enhanced closeness and relationship satisfaction on a daily level. Lagged analyses provide stronger evidence for shared problematic behavior preceding better daily relationship functioning, rather than better daily relationship functioning preceding more shared problematic behavior. Findings imply that behavior theories might benefit from including relationship-specific motives to explain problematic behavior, paying attention to the fact that shared problematic behaviors might be one of the ways in which couples keep up their relationship. Concordantly, they suggest that efforts to change problematic behaviors could be more effective when addressing the relationship system in which they occur.
Supplemental Material
Supplemental material, sj-docx-1-psp-10.1177_01461672221143783 for Let’s Enjoy an Evening on the Couch? A Daily Life Investigation of Shared Problematic Behaviors in Three Couple Studies by Theresa Pauly, Janina Lüscher, Corina Berli, Christiane A. Hoppmann, Rachel A. Murphy, Maureen C. Ashe, Wolfgang Linden, Kenneth M. Madden, Denis Gerstorf and Urte Scholz in Personality and Social Psychology Bulletin
Compared with the rest of Switzerland, German-speaking regions (about 63% of the Swiss population) tend to have higher economic prosperity as indicated by gross domestic product per capita and lower unemployment rates than non-German-speaking regions (Swiss Federal Statistical Office, 2021).
Originally, the items were planned to be rated on a 6-point and 7-point Likert-type scale for closeness and relationship satisfaction, respectively. The 2- and 3-point scales resulted from a programming error.
Footnotes
Authors’ Note: This project’s hypotheses and analytical plan (secondary analysis of existing data) were preregistered. Analysis scripts and full model results are available at https://osf.io/vmh6c/?view_only=a64335766d784ac9bc946ad6462e0749. The dependent nature of the data (couples) and the small sample size both constitute formidable risks that participants could be able to have their data identified by their partner. Thus, to protect participants’ confidentiality, data are available for researchers upon request only.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swiss National Science Foundation (Studies 1 and 2: grant # PP00P1_133632/1 to US) and the Heart and Stroke Foundation of Canada (grant # G-16-00012717 to CH, MA, RM, DG, WL, and KM). Theresa Pauly gratefully acknowledges support from the Swiss Government Excellence Scholarship, the University of Zurich (Forschungskredit, grant# FK-21-078), and the Swiss National Science Foundation (grant # CR12I1_166348/1). Christiane Hoppmann and Maureen Ashe gratefully acknowledge the support of the Canada Research Chairs Program. Rachel Murphy’s time was supported by the Michael Smith Foundation for Health Research (grant #17644).
ORCID iDs: Theresa Pauly  https://orcid.org/0000-0002-6855-1787
https://orcid.org/0000-0002-6855-1787
Maureen C. Ashe
https://orcid.org/0000-0002-6820-4435
Urte Scholz
https://orcid.org/0000-0003-0184-5921
Supplemental Material: Supplemental material is available online with this article.
References
- Alberts J. K., Yoshimura C. G., Rabby M., Loschiavo R. (2005). Mapping the topography of couples’ daily conversation. Journal of Social and Personal Relationships, 22(3), 299–322. 10.1177/0265407505050941 [DOI] [Google Scholar]
- Allen K.-A., Kern M. L., Rozek C. S., McInereney D., Slavich G. M. (2021). Belonging: A review of conceptual issues, an integrative framework, and directions for future research. Australian Journal of Psychology, 73(1), 87–102. 10.1080/00049530.2021.1883409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alley T. R., Brubaker L. W., Fox O. M. (2013). Courtship feeding in humans? The effects of feeding versus providing food on perceived attraction and intimacy. Human Nature, 24(4), 430–443. 10.1007/s12110-013-9179-7 [DOI] [PubMed] [Google Scholar]
- Arend M. G., Schäfer T. (2019). Statistical power in two-level models: A tutorial based on Monte Carlo simulation. Psychological Methods, 24(1), 1–19. 10.1037/met0000195 [DOI] [PubMed] [Google Scholar]
- Aron A., Fraley B. (1999). Relationship closeness as including other in the self: Cognitive underpinnings and measures. Social Cognition, 17(2), 140–160. 10.1521/soco.1999.17.2.140 [DOI] [Google Scholar]
- Aron A., Norman C. C., Aron E. N., McKenna C., Heyman R. E. (2000). Couples’ shared participation in novel and arousing activities and experienced relationship quality. Journal of Personality and Social Psychology, 78(2), 273–284. 10.1037//0022-3514.78.2.273 [DOI] [PubMed] [Google Scholar]
- Ask H., Idstad M., Engdahl B., Tambs K. (2013). Non-random mating and convergence over time for mental health, life satisfaction, and personality: The Nord-Trøndelag Health Study. Behavior Genetics, 43(2), 108–119. 10.1007/s10519-012-9578-2 [DOI] [PubMed] [Google Scholar]
- Asparouhov T., Hamaker E. L., Muthén B. (2018). Dynamic structural equation models. Structural Equation Modeling, 25(3), 359–388. 10.1080/10705511.2017.1406803 [DOI] [PubMed] [Google Scholar]
- Berli C., Stadler G., Inauen J., Scholz U. (2016). Action control in dyads: A randomized controlled trial to promote physical activity in everyday life. Social Science & Medicine, 163, 89–97. 10.1016/j.socscimed.2016.07.003 [DOI] [PubMed] [Google Scholar]
- Berrigan D., Dodd K., Troiano R. P., Krebs-Smith S. M., Barbash R. B. (2003). Patterns of health behavior in U.S. adults. Preventive Medicine, 36(5), 615–623. 10.1016/S0091-7435(02)00067-1 [DOI] [PubMed] [Google Scholar]
- Bolger N., Laurenceau J.-P. (2013). Intensive longitudinal methods: An introduction to diary and experience sampling research. Gilford Press. [Google Scholar]
- Bowen M. (1978). Family therapy in clinical practice. Jason Aronson. [Google Scholar]
- Branand B., Mashek D., Aron A. (2019). Pair-bonding as inclusion of other in the self: A literature review. Frontiers in Psychology, 10, Article 2399. 10.3389/fpsyg.2019.02399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks M. E., Kristensen K., van Benthem K. J., Magnusson A., Berg C. W., Nielsen A., Skaug H. J., Maechler M., Bolker B. M. (2017). glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. The R Journal, 9(2), 378–400. https://journal.r-project.org/archive/2017/RJ-2017-066/index.html [Google Scholar]
- Butler E. A. (2011). Temporal interpersonal emotion systems: The “TIES” that form relationships. Personality and Social Psychology Review, 15(4), 367–393. 10.1177/1088868311411164 [DOI] [PubMed] [Google Scholar]
- Carr L. J., Mahar M. T. (2012). Accuracy of intensity and inclinometer output of three activity monitors for identification of sedentary behavior and light-intensity activity. Journal of Obesity, 2012, Article 460271. 10.1155/2012/460271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi L., Liu Z., Matthews C. E., Buchowski M. S. (2011). Validation of accelerometer wear and nonwear time classification algorithm. Medicine and Science in Sports and Exercise, 43(2), 357–364. 10.1249/MSS.0b013e3181ed61a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper M. L., Frone M. R., Russell M., Mudar P. (1995). Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality and Social Psychology, 69(5), 990–1005. 10.1037/0022-3514.69.5.990 [DOI] [PubMed] [Google Scholar]
- Cox M. J., Paley B. (1997). Families as systems. Annual Review of Psychology, 48, 243–267. 10.1146/annurev.psych.48.1.243 [DOI] [PubMed] [Google Scholar]
- Dalton E. D., Hammen C. L. (2018). Independent and relative effects of stress, depressive symptoms, and affect on college students’ daily health behaviors. Journal of Behavioral Medicine, 41(6), 863–874. 10.1007/s10865-018-9945-4 [DOI] [PubMed] [Google Scholar]
- Di Castelnuovo A., Quacquaruccio G., Donati M. B., de Gaetano G., Iacoviello L. (2009). Spousal concordance for major coronary risk factors: A systematic review and meta-analysis. American Journal of Epidemiology, 169(1), 1–8. 10.1093/aje/kwn234 [DOI] [PubMed] [Google Scholar]
- Dimoff J. D., Sayette M. A. (2017). The case for investigating social context in laboratory studies of smoking. Addiction, 112(3), 388–395. 10.1111/add.13503 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding D., Rogers K., van der Ploeg H., Stamatakis E., Bauman A. E. (2015). Traditional and emerging lifestyle risk behaviors and all-cause mortality in middle-aged and older adults: Evidence from a large population-based Australian cohort. PLOS Medicine, 12(12), Article e1001917. 10.1371/journal.pmed.1001917 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doherty W. J., Whitehead D. A. (1986). The social dynamics of cigarette smoking: A family systems perspective. Family Process, 25(3), 453–459. 10.1111/j.1545-5300.1986.00453.x [DOI] [PubMed] [Google Scholar]
- Finucane M. O., Horvath C. W. (2000). Lazy leisure: A qualitative investigation of the relational uses of television in marriage. Communication Quarterly, 48(3), 311–321. 10.1080/01463370009385599 [DOI] [Google Scholar]
- Girme Y. U., Overall N. C., Faingataa S. (2014). “Date nights” take two: The maintenance function of shared relationship activities. Personal Relationships, 21(1), 125–149. 10.1111/pere.12020 [DOI] [Google Scholar]
- Gomillion S., Gabriel S., Kawakami K., Young A. F. (2017). Let’s stay home and watch TV. Journal of Social and Personal Relationships, 34(6), 855–874. 10.1177/0265407516660388 [DOI] [Google Scholar]
- Green P., MacLeod C. J. (2016). SIMR: An R package for power analysis of generalized linear mixed models by simulation. Methods in Ecology and Evolution, 7(4), 493–498. 10.1111/2041-210X.12504 [DOI] [Google Scholar]
- Gregersen S. C., Gillath O. (2020). How food brings us together: The ties between attachment and food behaviors. Appetite, 151, Article 104654. 10.1016/j.appet.2020.104654 [DOI] [PubMed] [Google Scholar]
- Hamilton H. R., DeHart T. (2017). Drinking to belong: The effect of a friendship threat and self-esteem on college student drinking. Self and Identity, 16(1), 1–15. 10.1080/15298868.2016.1210539 [DOI] [Google Scholar]
- Harasymchuk C., Walker D. L., Muise A., Impett E. A. (2021). Planning date nights that promote closeness: The roles of relationship goals and self-expansion. Journal of Social and Personal Relationships, 38(5), 1692–1709. 10.1177/02654075211000436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holway G. V., Umberson D., Donnelly R. (2018). Health and health behavior concordance between spouses in same-sex and different-sex marriages. Social Currents, 5(4), 319–327. 10.1177/2329496517734570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hunsley J., Best M., Lefebvre M., Vito D. (2001). The seven-item short form of the Dyadic Adjustment Scale: Further evidence for construct validity. The American Journal of Family Therapy, 29(4), 325–335. 10.1080/01926180126501 [DOI] [Google Scholar]
- Impett E. A., Gable S. L., Peplau L. A. (2005). Giving up and giving in: The costs and benefits of daily sacrifice in intimate relationships. Journal of Personality and Social Psychology, 89(3), 327–344. 10.1037/0022-3514.89.3.327 [DOI] [PubMed] [Google Scholar]
- Jeong S., Cho S.-I. (2018). Concordance in the health behaviors of couples by age: A cross-sectional study. Journal of Preventive Medicine and Public Health = Yebang Uihakhoe Chi, 51(1), 6–14. 10.3961/jpmph.17.137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiecolt-Glaser J. K., Wilson S. J. (2017). Lovesick: How couples’ relationships influence health. Annual Review of Clinical Psychology, 13, 421–443. 10.1146/annurev-clinpsy-032816-045111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laurenceau J.-P., Bolger N. (2005). Using diary methods to study marital and family processes. Journal of Family Psychology, 19(1), 86–97. 10.1037/0893-3200.19.1.86 [DOI] [PubMed] [Google Scholar]
- Litt D. M., Stock M. L., Lewis M. A. (2012). Drinking to fit in: Examining the need to belong as a moderator of perceptions of best friends’ alcohol use and related risk cognitions among college students. Basic and Applied Social Psychology, 34(4), 313–321. 10.1080/01973533.2012.693357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo S. (2017). Assortative mating and couple similarity: Patterns, mechanisms, and consequences. Social and Personality Psychology Compass, 11(8), Article e12337. 10.1111/spc3.12337 [DOI] [Google Scholar]
- Luong G., Charles S. T., Fingerman K. L. (2011). Better with age: Social relationships across adulthood. Journal of Social and Personal Relationships, 28(1), 9–23. 10.1177/0265407510391362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lüscher J., Scholz U. (2017). Does social support predict smoking abstinence in dual-smoker couples? Evidence from a dyadic approach. Anxiety, Stress, and Coping, 30(3), 273–281. 10.1080/10615806.2016.1270448 [DOI] [PubMed] [Google Scholar]
- Lüscher J., Stadler G., Scholz U. (2017). A daily diary study of joint quit attempts by dual-smoker couples: The role of received and provided social support. Nicotine & Tobacco Research, 20(1), 100–107. 10.1093/ntr/ntx079 [DOI] [PubMed] [Google Scholar]
- Meyler D., Stimpson J. P., Peek M. K. (2007). Health concordance within couples: A systematic review. Social Science & Medicine, 64(11), 2297–2310. 10.1016/j.socscimed.2007.02.007 [DOI] [PubMed] [Google Scholar]
- Mund M., Finn C., Hagemeyer B., Zimmermann J., Neyer F. J. (2015). The dynamics of self–esteem in partner relationships. European Journal of Personality, 29(2), 235–249. 10.1002/per.1984 [DOI] [Google Scholar]
- Muthén L. K., Muthén B. O. (1998. –2017). Mplus user’s guide (8th ed.). [Google Scholar]
- Padilla-Walker L. M., Coyne S. M., Memmott-Elison M. K. (2019). Media and the family. In Fiese B. H., Celano M., Deater-Deckard K., Jouriles E. N., Whisman M. A. (Eds.), APA handbook of contemporary family psychology: Foundations, methods, and contemporary issues across the lifespan (pp. 365–378). American Psychological Association. [Google Scholar]
- Pauly T., Ashe M. C., Murphy R., Gerstorf D., Linden W., Madden K. M., Hoppmann C. A. (2021). Active with whom? Examining the social context of physical activity in individuals after stroke and their partners. Frontiers in Public Health, 9, Article754046. 10.3389/fpubh.2021.754046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinheiro J., Bates D., DebRoy S., Sarkar D. (2020). nlme: Linear and nonlinear mixed effects models (R package version 3.1-148). https://CRAN.R-project.org/package=nlme
- R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org
- Ram N., Brinberg M., Pincus A. L., Conroy D. E. (2017). The questionable ecological validity of ecological momentary assessment: Considerations for design and analysis. Research in Human Development, 14(3), 253–270. 10.1080/15427609.2017.1340052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts C. K., Barnard R. J. (2005). Effects of exercise and diet on chronic disease. Journal of Applied Physiology, 98(1), 3–30. 10.1152/japplphysiol.00852.2004 [DOI] [PubMed] [Google Scholar]
- Rohrbaugh M. J., Shoham V., Butler E., Hasler B. P., Berman J. S. (2009). Affective synchrony in dual- and single-smoker couples: Further evidence of “symptom-system fit”? Family Process, 48(1), 55–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rohrbaugh M. J., Shoham V., Racioppo M. W. (2002). Toward family level attribute × treatment interaction research. In Liddle H. A., Santisteban D. A., Levant R. F., Bray J. H. (Eds.), Family psychology: Science-based interventions (pp. 215–237). American Psychological Association. 10.1037/10438-011 [DOI] [Google Scholar]
- Scholz U. (2019). It’s time to think about time in health psychology. Applied Psychology: Health and Well-Being, 11(2), 173–186. 10.1111/aphw.12156 [DOI] [PubMed] [Google Scholar]
- Scholz U., Berli C. (2014). A Dyadic Action Control Trial in Overweight and Obese Couples (DYACTIC). BMC Public Health, 14, Article 1321. 10.1186/1471-2458-14-1321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shoham V., Butler E. A., Rohrbaugh M. J., Trost S. E. (2007). Symptom-system fit in couples: Emotion regulation when one or both partners smoke. Journal of Abnormal Psychology, 116(4), 848–853. 10.1037/0021-843X.116.4.848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skoyen J. A., Kogan A. V., Novak S. A., Butler E. A. (2013). Health behavior and emotion regulation in couples. In Newman M. L., Roberts N. A. (Eds.), Health and social relationships: The good, the bad, and the complicated (pp. 121–142). American Psychological Association. 10.1037/14036-006 [DOI] [Google Scholar]
- Skoyen J. A., Randall A. K., Mehl M. R., Butler E. A. (2014). “We” overeat, but “I” can stay thin: Pronoun use and body weight in couples who eat to regulate emotion. Journal of Social and Clinical Psychology, 33(8), 743–766. 10.1521/jscp.2014.33.8.743 [DOI] [Google Scholar]
- Skoyen J. A., Rentscher K. E., Butler E. A. (2018). Relationship quality and couples’ unhealthy behaviors predict body mass index in women. Journal of Social and Personal Relationships, 35(2), 224–245. 10.1177/0265407516680909 [DOI] [Google Scholar]
- Swiss Federal Statistical Office. (2020). Schweizerische Gesundheitsbefragung 2017: Tabakkonsum [Swiss health survey 2017: Tobacco consumption]. https://www.bfs.admin.ch/bfs/fr/home/actualites/quoi-de-neuf.assetdetail.11907022.html
- Swiss Federal Statistical Office. (2021). Regional comparison of selected indicators, 2021. https://www.bfs.admin.ch/bfs/en/home/statistics/regional-statistics/regional-portraits-key-figures/cantons/data-explanations.assetdetail.15864481.html
- Taylor C., Webb T. L., Sheeran P. (2014). ‘I deserve a treat!’: Justifications for indulgence undermine the translation of intentions into action. The British Journal of Social Psychology, 53(3), 501–520. 10.1111/bjso.12043 [DOI] [PubMed] [Google Scholar]
- Testa M., Wang W., Derrick J. L., Leonard K. E. (2019). Marijuana use episodes and partner intimacy experiences: A daily report study. Cannabis, 2(1), 19–28. 10.26828/cannabis.2019.01.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Totenhagen C. J., Butler E. A., Curran M. A., Serido J. (2016). The calm after the storm: Relationship length as associated with couple’s daily variability. Journal of Social and Personal Relationships, 33(6), 768–791. 10.1177/0265407515597562 [DOI] [Google Scholar]
- Troisi J. D., Gabriel S. (2011). Chicken soup really is good for the soul: “Comfort food” fulfills the need to belong. Psychological Science, 22(6), 747–753. 10.1177/0956797611407931 [DOI] [PubMed] [Google Scholar]
- Walsh C. M., Neff L. A., Gleason M. E. J. (2017). The role of emotional capital during the early years of marriage: Why everyday moments matter. Journal of Family Psychology, 31(4), 513–519. 10.1037/fam0000277 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-psp-10.1177_01461672221143783 for Let’s Enjoy an Evening on the Couch? A Daily Life Investigation of Shared Problematic Behaviors in Three Couple Studies by Theresa Pauly, Janina Lüscher, Corina Berli, Christiane A. Hoppmann, Rachel A. Murphy, Maureen C. Ashe, Wolfgang Linden, Kenneth M. Madden, Denis Gerstorf and Urte Scholz in Personality and Social Psychology Bulletin