

Abstract
Purpose
This study aimed to report the projected cancer incidence and mortality for the year 2024 to estimate Korea’s current cancer burden.
Materials and Methods
Cancer incidence data from 1999 to 2021 were obtained from the Korea National Cancer Incidence Database, and cancer mortality data from 1993 to 2022 were acquired from Statistics Korea. Cancer incidence and mortality were projected by fitting a linear regression model to observed age-specific cancer rates against their respective years and multiplying the projected age-specific rates by the anticipated age-specific population for 2024. A joinpoint regression model was used to determine the year in which the linear trend changed significantly; we only used the data of the latest trend for prediction.
Results
In total, 292,221 new cancer cases and 83,770 cancer deaths are expected to occur in Korea in 2024. The most common cancer site is expected to be the thyroid, followed by the colon and rectum, lung, breast, and stomach. These five cancers are expected to represent 55.7% of the overall burden of cancer in Korea. The most common type of cancer leading to death is expected to be lung cancer, followed by liver, colorectal, pancreatic, and stomach cancers.
Conclusion
The age-standardized incidence rates for female breast and prostate cancers are estimated to continue to increase. These up-to-date estimates of the cancer burden in Korea could be an important resource for planning and evaluating cancer-control programs.
Keywords: Incidence, Mortality, Neoplasms, Forecasting, Korea, 2024
Introduction
As the leading cause of death in Korea [1], cancer has been a major public health concern in the country since 1983. 250,000 patients were newly diagnosed with cancer in Korea, and 22% of deaths were due to cancer in 2022 [2]. Although the cancer registration system in Korea is highly efficient and can provide nationwide cancer statistics within a relatively short period, a lag time of at least 2 years is required to collect and analyze data for a specific year. For planning and implementing comprehensive cancer-control programs, it is important to assess the number of new cases and deaths that are expected to occur during the current year. In this study, we report the projected cancer incidence and mortality for the year 2024 based on data from the 1990s to 2021.
Materials and Methods
The Korean Ministry of Health and Welfare initiated a nationwide, hospital-based cancer registry, known as the Korea Central Cancer Registry (KCCR), in 1980. The history, objectives, and activities of the KCCR have been documented in detail elsewhere [3]. Cancer incidence data from 1999 to 2021 were obtained from the Korea National Cancer Incidence Database (KNCI DB). Cancer cases were classified according to the International Classification of Diseases for Oncology, 3rd edition [4] and converted according to the International Classification of Diseases, 10th edition (ICD-10) [5]. Mortality data from 1993 to 2022 were acquired from Statistics Korea [1]. The cause of death was coded and classified according to the ICD-10 [5].
The cancer sites included in this study were (1) all cancer sites combined and (2) the 24 cancer sites as follows: lips, oral cavity, and pharynx (C00-C14), esophagus (C15), stomach (C16), colon and rectum (C18-C20), liver (C22), gallbladder etc. (C23-C24), pancreas (C25), larynx (C32), lung (C33-C34), breast (C50), cervix uteri (C53), corpus uteri (C54), ovary (C56), prostate (C61), testis (C62), kidney (C64), bladder (C67), brain and central nervous system (C70-C72), thyroid (C73), Hodgkin lymphoma (C81), non-Hodgkin lymphoma (C82-C86, C96), multiple myeloma (C90), leukemia (C91-C95), and other and ill-defined sites (remainder of C00-C96).
The population data from 1993 to 2024 were obtained from the resident registration population data, reported by Statistics Korea. Data of the mid-year population (July 1 of the respective year) were used as the denominator to obtain the annual incidence and mortality rates. However, for the year 2024, we used the population data on December 31, 2023, as the mid-2024 resident registration population data were not yet available at the time of the analysis.
Linear regression models [6] were used to assess time trends and create projections. We first performed a joinpoint regression analysis on the data available to detect the year when significant changes occurred in cancer trends according to sex and cancer site. A joinpoint regression describes changes in data trends by connecting several different line segments on a log scale at “Joinpoints.” This analysis was performed using Joinpoint software (ver. 5.0.2.0, http://surveillance.cancer.gov/joinpoint) from the Surveillance Research Program of the US National Cancer Institute [7]. For the analysis, we arranged to have at least four data points between consecutive joinpoints. Secondly, to predict age-specific cancer rates, a linear regression model was fitted to age-specific rates by 5-year age groups against their respective years, based on the observed cancer incidence data of the latest trends. Finally, we multiplied the projected age-specific rates by the age-specific population to get the projected number of cancer cases and deaths for the year 2024.
We summarized the results using crude rates (CRs) and age-standardized rates (ASRs) of cancer incidence and mortality. ASRs were standardized using the world standard population [8] and expressed per 100,000 persons.
Results
1. Incidence
In total, 292,221 new cancer cases are expected to occur in 2024 (Table 1, Fig. 1); more men (n=152,220) than women (n=141,001) are expected to be affected.
Table 1.
Estimated new cancer cases and deaths by sex during 2024 in Korea
| Site | Estimated new cases |
Estimated deaths |
||||
|---|---|---|---|---|---|---|
| Both sexes | Men | Women | Both sexes | Men | Women | |
| All sites | 292,221 | 152,220 | 140,001 | 83,770 | 50,862 | 32,908 |
| Lip, oral cavity, and pharynx | 4,510 | 3,227 | 2,259 | 1,285 | 930 | 355 |
| Esophagus | 2,832 | 2,467 | 971 | 1,466 | 1,315 | 151 |
| Stomach | 24,769 | 16,268 | 1,023 | 6,291 | 4,076 | 2,215 |
| Colon and rectum | 35,559 | 20,549 | 27,159 | 8,754 | 4,858 | 3,896 |
| Livera) | 13,885 | 10,232 | 141 | 9,146 | 6,641 | 2,505 |
| Gallbladderb) | 7,738 | 4,168 | 2,777 | 5,728 | 3,102 | 2,626 |
| Pancreas | 10,158 | 5,187 | 1,067 | 7,861 | 4,004 | 3,857 |
| Larynx | 1,052 | 994 | 1,774 | 196 | 189 | 7 |
| Lungc) | 34,404 | 22,749 | 13,127 | 18,278 | 13,544 | 4,734 |
| Breast | 30,665 | 129 | 30,536 | 3,039 | 20 | 3,019 |
| Cervix uteri | 2,704 | - | 2,704 | 694 | - | 694 |
| Corpus uteri | 4,013 | - | 4,013 | 461 | - | 461 |
| Ovary | 3,384 | - | 3,384 | 1,466 | - | 1,466 |
| Prostate | 24,115 | 24,115 | - | 2,501 | 2,501 | - |
| Testis | 362 | 362 | - | 18 | 18 | - |
| Kidney | 7,296 | 5,037 | 2,259 | 1,061 | 704 | 357 |
| Bladder | 5,435 | 4,464 | 971 | 1,664 | 1,255 | 409 |
| Brain and CNS | 2,228 | 1,205 | 1,023 | 1,518 | 842 | 676 |
| Thyroid | 37,242 | 10,083 | 27,159 | 337 | 107 | 230 |
| Hodgkin lymphoma | 378 | 237 | 141 | 63 | 39 | 24 |
| Non-Hodgkin lymphoma | 6,548 | 3,771 | 2,777 | 2,498 | 1,427 | 1,071 |
| Multiple myeloma | 2,277 | 1,210 | 1,067 | 1,117 | 570 | 547 |
| Leukemia | 4,196 | 2,422 | 1,774 | 2,236 | 1,312 | 924 |
| Other and ill defined | 26,471 | 13,344 | 13,127 | 6,092 | 3,408 | 2,684 |
CNS, central nervous system.
Includes the liver and intrahepatic bile duct,
Includes the gallbladder and other/unspecified parts of the biliary tract,
Includes the lung and bronchus.
Fig. 1.
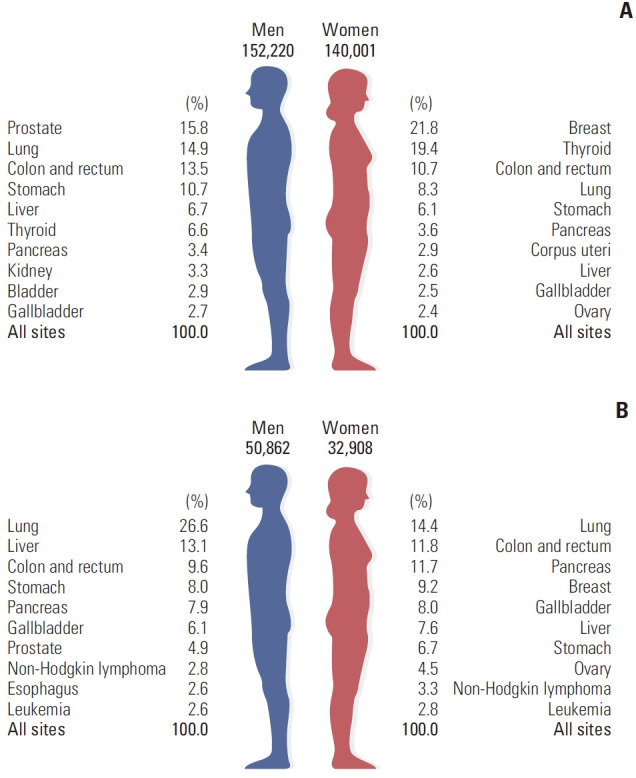
The 10 leading types of estimated new cancer cases and deaths by sex in 2024. (A) Estimated new cases. (B) Estimated deaths.
The projected CRs per 100,000 for all of the sites combined in 2024 are 595.4 cases and 543.5 cases for men and women, respectively (Table 2). The projected ASRs per 100,000 for all of the sites combined are 291.9 cases and 296.6 cases for men and women, respectively. In men, the five leading primary sites of cancer are expected to be the prostate (CR, 94.3; ASR, 39.6), lung (CR, 89.0; ASR, 37.8), colon and rectum (CR, 80.4; ASR, 42.3), stomach (CR, 63.6; ASR, 29.3), and liver (CR, 40.0; ASR, 18.5), accounting for 61.7% of all new cancer cases in 2024. In women, the five leading primary sites are expected to be the breast (CR, 118.5; ASR, 71.3), thyroid (CR, 105.4; ASR, 79.5), colon and rectum (CR, 58.3; ASR, 27.6), lung (CR, 45.3; ASR, 17.7), and stomach (CR, 33.0; ASR, 14.0), accounting for 66.3% of all new cancer cases in 2024 (Fig. 1).
Table 2.
Estimated crude and age-standardized cancer incidences by sex during 2024 in Korea
| Site | Crude incidence rates per 100,000 |
Age-standardized incidence rates per 100,000a) |
||||
|---|---|---|---|---|---|---|
| Both sexes | Men | Women | Both sexes | Men | Women | |
| All sites | 569.4 | 595.4 | 543.5 | 288.6 | 291.9 | 296.6 |
| Lip, oral cavity, and pharynx | 8.8 | 12.6 | 5.0 | 4.5 | 6.5 | 2.6 |
| Esophagus | 5.5 | 9.7 | 1.4 | 2.3 | 4.2 | 0.6 |
| Stomach | 48.3 | 63.6 | 33.0 | 21.2 | 29.3 | 14.0 |
| Colon and rectum | 69.3 | 80.4 | 58.3 | 34.7 | 42.3 | 27.6 |
| Liverb) | 27.1 | 40.0 | 14.2 | 11.5 | 18.5 | 5.2 |
| Gallbladderc) | 15.1 | 16.3 | 13.9 | 5.5 | 6.8 | 4.3 |
| Pancreas | 19.8 | 20.3 | 19.3 | 8.0 | 9.1 | 7.1 |
| Larynx | 2.1 | 3.9 | 0.2 | 0.8 | 1.7 | 0.1 |
| Lungd) | 67.0 | 89.0 | 45.3 | 26.6 | 37.8 | 17.7 |
| Breast | 59.8 | 0.5 | 118.5 | 35.6 | 0.2 | 71.3 |
| Cervix uteri | 5.4 | - | 10.8 | 3.5 | - | 7.0 |
| Cervix uteri | 5.3 | - | 10.5 | 3.4 | - | 6.8 |
| Corpus uteri | 7.8 | - | 15.6 | 4.5 | - | 9.1 |
| Ovary | 6.6 | - | 13.1 | 3.9 | - | 7.8 |
| Prostate | 47.0 | 94.3 | - | 18.2 | 39.6 | - |
| Testis | 0.7 | 1.4 | - | 0.7 | 1.4 | - |
| Kidney | 14.2 | 19.7 | 8.8 | 7.5 | 10.6 | 4.4 |
| Bladder | 10.6 | 17.5 | 3.8 | 4.0 | 7.4 | 1.3 |
| Brain and CNS | 4.3 | 4.7 | 4.0 | 3.0 | 3.4 | 2.7 |
| Thyroid | 72.6 | 39.4 | 105.4 | 53.3 | 28.3 | 79.5 |
| Hodgkin lymphoma | 0.7 | 0.9 | 0.6 | 0.6 | 0.7 | 0.5 |
| Non-Hodgkin lymphoma | 12.8 | 14.8 | 10.8 | 6.9 | 8.5 | 5.5 |
| Multiple myeloma | 4.4 | 4.7 | 4.1 | 1.8 | 2.1 | 1.6 |
| Leukemia | 8.2 | 9.5 | 6.9 | 5.8 | 6.8 | 4.8 |
| Other and ill defined | 51.6 | 52.2 | 51.0 | 24.3 | 26.8 | 22.2 |
CNS, central nervous system.
Age adjusted to the world standard population,
Includes the liver and intrahepatic bile duct,
Includes the gallbladder and other/unspecified parts of the biliary tract,
Includes the lung and bronchus.
The five most common cancer sites expected in 2024 according to sex and age group are shown in Table 3. Leukemia and thyroid cancer are expected to be the most common forms of cancer in both sexes for those aged 0-14 years and 15-34 years, respectively. Colorectal cancer is predicted to be the most prevalent cancer in men aged 35-64 years, while prostate cancer is expected to be more frequent in men aged 65 years and above. Breast cancer is predicted to be the most common cancer in women aged 35-64 years, whereas lung cancer is expected to be the most common form in women aged 65 years and above. According to the projection, the incidences of stomach, lung, liver, colorectal, and prostate cancers will increase gradually with age for men (Fig. 2A). In women, the age-specific incidence rates for stomach, colo rectal, liver, lung, and cervical cancers denote an increasing trend with age; however, the incidences of breast and thyroid cancers in women are expected to level off after the age of 45 and 50 years, respectively (Fig. 2B).
Table 3.
Estimated cancer incidence by age group and sex during 2024 in Korea
| Rank | Age group (yr) |
|||
|---|---|---|---|---|
| 0-14 | 15-34 | 35-64 | ≥ 65 | |
| Men | ||||
| 1 | Leukemia (4.9) | Thyroid (30.7) | Colon and rectum (81.5) | Prostate (454.6) |
| 2 | Non-Hodgkin lymphoma (3.3) | Colon and rectum (13.1) | Thyroid (57.5) | Lunga) (408.2) |
| 3 | Brain and CNS (2.4) | Leukemia (4.2) | Stomach (54.5) | Colon and rectum (228.8) |
| 4 | Liver (0.3) | Non-Hodgkin lymphoma (3.4) | Lunga) (42.4) | Stomach (223.8) |
| 5 | Kidney (0.2) | Testis (3.4) | Prostat (37.7) | Liverb) (139.8) |
| Women | ||||
| 1 | Leukemia (4.2) | Thyroid (91.6) | Breast (193.3) | Lunga) (140.4) |
| 2 | Brain and CNS (2.0) | Breast (14.1) | Thyroid (157.9) | Colon and rectum (139.1) |
| 3 | Non-Hodgkin lymphoma (1.6) | Colon and rectum (8.6) | Colon and rectum (58.6) | Breast (124.9) |
| 4 | Thyroid (1.1) | Cervix uteri (5.2) | Lunga) (33.4) | Stomach (91.9) |
| 5 | Ovary (0.8) | Ovary (4.0) | Stomach (29.1) | Pancreas (68.3) |
CNS, central nervous system.
Includes the lung and bronchus,
Includes the liver and intrahepatic bile duct.
Fig. 2.
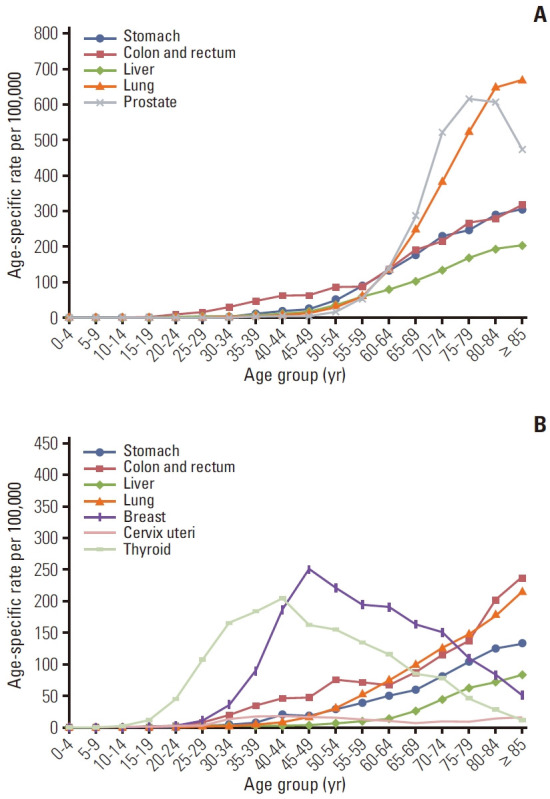
Projected age-specific incidences of major cancers during 2024 in Korea. (A) Men. (B) Women.
2. Mortality
It is estimated that 83,770 cancer deaths will occur in Korea during 2024 (Table 1, Fig. 1). The projected CRs per 100,000 for all of the sites combined in 2024 for men and women are 199.0 cases and 127.8 cases, respectively, whereas the projected ASRs per 100,000 for all sites combined for men and women are expected to be 83.8 cases and 43.3 cases, respectively (Table 4). The predicted five leading cancer sites causing mortality in men are the lung (CR, 53.0; ASR, 21.1), liver (CR, 26.0; ASR, 11.4), colon and rectum (CR, 19.0; ASR, 8.2), stomach (CR, 15.9; ASR, 7.0), and pancreas (CR, 15.7; ASR, 6.7). During the same period, lung cancer (CR, 18.4; ASR, 5.5) is projected to be the leading cause of cancer death in women, followed by colon and rectal (CR, 15.1; ASR, 4.4), pancreatic (CR, 15.0; ASR, 4.7), breast (CR, 11.7; ASR, 5.8), and gallbladder (CR, 10.2; ASR, 2.7) cancers.
Table 4.
Estimated crude and age-standardized cancer mortality rates by sex during 2024 in Korea
| Site | Crude mortality rates per 100,000 |
Age-standardized mortality rates per 100,000a) |
||||
|---|---|---|---|---|---|---|
| Both sexes | Men | Women | Both sexes | Men | Women | |
| All sites | 163.2 | 199.0 | 127.8 | 60.8 | 83.8 | 43.3 |
| Lip, oral cavity, and pharynx | 2.5 | 3.6 | 1.4 | 1.0 | 1.6 | 0.5 |
| Esophagus | 2.9 | 5.1 | 0.6 | 1.1 | 2.2 | 0.2 |
| Stomach | 12.3 | 15.9 | 8.6 | 4.8 | 7.0 | 3.0 |
| Colon and rectum | 17.1 | 19.0 | 15.1 | 6.1 | 8.2 | 4.4 |
| Liverb) | 17.8 | 26.0 | 9.7 | 6.8 | 11.4 | 2.9 |
| Gallbladderc) | 11.2 | 12.1 | 10.2 | 3.7 | 4.9 | 2.7 |
| Pancreas | 15.3 | 15.7 | 15.0 | 5.6 | 6.7 | 4.7 |
| Larynx | 0.4 | 0.7 | 0.0 | 0.1 | 0.3 | 0.0 |
| Lungd) | 35.6 | 53.0 | 18.4 | 12.3 | 21.1 | 5.5 |
| Breast | 5.9 | 0.1 | 11.7 | 2.9 | 0.0 | 5.8 |
| Cervix uteri | 1.4 | - | 2.7 | 0.7 | - | 1.3 |
| Corpus uteri | 0.9 | - | 1.8 | 0.4 | - | 0.8 |
| Ovary | 2.9 | - | 5.7 | 1.3 | - | 2.5 |
| Prostate | 4.9 | 9.8 | - | 1.4 | 3.7 | - |
| Testis | 0.0 | 0.1 | - | 0.0 | 0.1 | - |
| Kidney | 2.1 | 2.8 | 1.4 | 0.8 | 1.2 | 0.4 |
| Bladder | 3.2 | 4.9 | 1.6 | 1.0 | 1.9 | 0.4 |
| Brain and CNS | 3.0 | 3.3 | 2.6 | 1.6 | 1.9 | 1.3 |
| Thyroid | 0.7 | 0.4 | 0.9 | 0.2 | 0.2 | 0.2 |
| Hodgkin lymphoma | 0.1 | 0.2 | 0.1 | 0.1 | 0.1 | 0.0 |
| Non-Hodgkin lymphoma | 4.9 | 5.6 | 4.2 | 1.8 | 2.4 | 1.3 |
| Multiple myeloma | 2.2 | 2.2 | 2.1 | 0.8 | 0.9 | 0.7 |
| Leukemia | 4.4 | 5.1 | 3.6 | 1.9 | 2.4 | 1.4 |
| Other and ill defined | 11.9 | 13.3 | 10.4 | 4.5 | 6.0 | 3.4 |
CNS, central nervous system.
Age adjusted to the world standard population,
Includes the liver and intrahepatic bile duct,
Includes the gallbladder and other/unspecified parts of the biliary tract,
Includes the lung and bronchus.
The predicted age-specific mortality rates of the leading causes of cancer-associated death in men and women in 2024 are shown in detail in Fig. 3. According to age, Korean men and women aged at least 60 years are expected to have the highest mortality rates due to lung cancer.
Fig. 3.
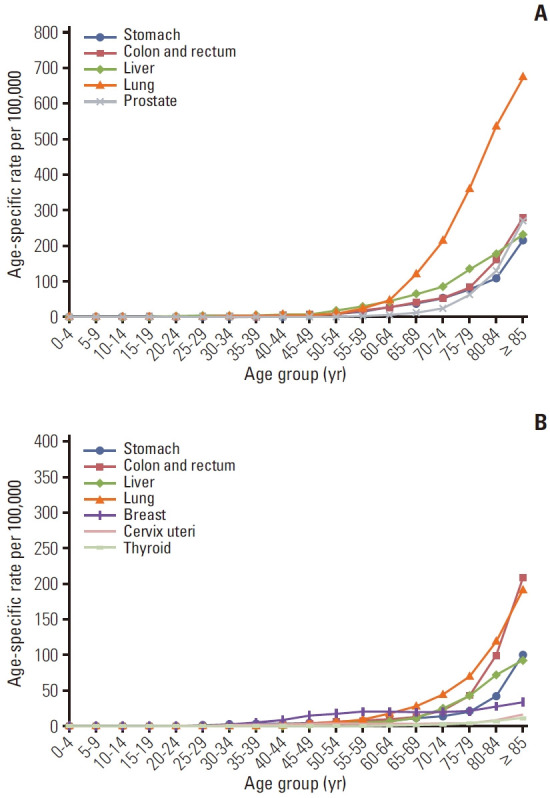
Projected age-specific mortality rates of major cancers during 2024 in Korea. (A) Men. (B) Women.
Conclusion
A total of 292,221 new cancer cases and 83,770 cancer deaths are expected to occur in Korea during 2024. Prostate cancer is predicted to be the most common type of cancer among men, followed by lung, colorectal, stomach, and liver cancers. Lung, liver, colorectal, stomach, and pancreatic cancers are expected to be the most common causes of cancer deaths among men. In women, the five leading primary cancer sites are expected to be the breast, thyroid, colon and rectum, lung, and stomach, while lung, colorectal, pancreatic, breast, and gallbladder cancers are projected to be the most common causes of cancer deaths.
Cancer is currently one of the foremost public health concerns in Korea. The burden of most types of cancers will continue to grow with the increasing age of the population. The current projections of cancer incidence and mortality for 2024 represent an important resource for planning and evaluating cancer-control programs.
As the estimates in this study are model-based, these results should be interpreted with caution. Due to coronavirus disease 2019 epidemic, following a year-on-rear decline of cancer incidence in 2020, there was a substantial increase in the number of cancer cases in 2021. Moreover, changes in the diagnostic criteria for colorectal and stomach cancers led to a significant increase in the number of those cancers in 2021. As a result, it may be affected by the predict of 2024, so attention should be paid to the interpretation.
Acknowledgments
The authors would like to thank the tumor registrars (health information managers) of the KCCR-affiliated hospitals and non-KCCR-affiliated hospitals for the assistance with data collection, abstraction, and coding. Additionally, we acknowledge the cooperation of the National Health Insurance Service and Statistics Korea for their support with the data.
This work was supported by the National Cancer Center research grant (No. 2211110).
Footnotes
Author Contributions
Conceived and designed the analysis: Jung KW.
Collected the data: Jung KW, Kong HJ, Kim HJ, Park EH, Yun EH, Kim JE.
Contributed data or analysis tools: Jung KW, Kong HJ, Kim HJ, Park EH, Yun EH, Kim JE.
Performed the analysis: Jung KW.
Wrote the paper: Jung KW.
Interpretation and review: Kang MJ, Park EH, Yun EH, Kim HJ, Kim JE, Im JS, Seo HG.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
References
- 1. Statistics Korea [Internet]. Daejeon: Statistics Korea; 2024 [cited 2024 Feb 8]. Available from: http://kosis.kr.
- 2.Hong S, Won YJ, Lee JJ, Jung KW, Kong HJ, Im JS, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2018. Cancer Res Treat. 2021;53:301–15. doi: 10.4143/crt.2021.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shin HR, Won YJ, Jung KW, Kong HJ, Yim SH, Lee JK, et al. Nationwide cancer incidence in Korea, 1999-2001: first result using the National Cancer Incidence Database. Cancer Res Treat. 2005;37:325–31. doi: 10.4143/crt.2005.37.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. World Health Organization. International Classification of Diseases for Oncology (ICD-O), 3rd ed., 2nd rev. [Internet]. Geneva: World Health Organization; 2019 [cited 2024 Feb 10]. Available from: https://iris.who.int/handle/10665/96612.
- 5.World Health Organization . International statistical classification of diseases and related health problems, 10th rev. [Internet] Geneva: World Health Organization; 2009 [cited 2024 Feb 10]. Available from: https://iris.who.int/handle/10665/44081. [Google Scholar]
- 6. Boyle P, Parkin DM. Statistical methods for registries. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, editors. Cancer registration: principles and methods. IARC Scientific Publication No. 95. Lyon: IARC Press; 1991. p. 126-58. [PubMed] [Google Scholar]
- 7.National Cancer Institute . Bethesda, MD: National Cancer Institute; Joinpoint regression program, version 5.0.2.0 [Internet] 2024 [cited 2024 Feb 10]. Available from: http://surveillance.cancer.gov/joinpoint/ [Google Scholar]
- 8.Segi M. Cancer mortality for selected sites in 24 countries (1950-1957) Sendai: Tohoku University School of Medicine; 1960. [Google Scholar]