

Abstract
Inspiring New Science to Guide Healthcare in Turner Syndrome (InsighTS) Registry is a national, multicenter registry for individuals with Turner syndrome (TS) designed to collect and store validated longitudinal clinical data from a diverse cohort of patients with TS. Herein, we describe the rationale, design, and approach used to develop the InsighTS registry, as well as the demographics of the initial participants to illustrate the registry’s diversity and future utility. Multiple stakeholder groups have been involved from project conceptualization through dissemination, ensuring the registry serves the priorities of the TS community. Key features of InsighTS include recruitment strategies to facilitate enrollment of participants that appropriately reflect the population of individuals with TS receiving care in the US, clarity of data ownership and sharing, and sustainability of this resource. The registry gathers clinical data on diagnosis, treatment, comorbidities, health care utilization, clinical practices, and quality of life with the goal of improving health outcomes for this population. Future directions include multiple patient-centered clinical-translational research projects that will use the InsighTS platform. This thorough and thoughtful planning will ensure InsighTS is a valuable and sustainable resource for the TS community for decades to come.
Keywords: Turner syndrome, Registry, Health care outcomes, rare disease, monosomy X, sex chromosome aneuploidy
INTRODUCTION
Turner syndrome (TS) is a rare disorder named after Dr. Henry Turner, who described the original case series of women who presented with dysmorphic features and lack of pubertal development in 1938(TURNER, 1938). The underlying cause was subsequently identified to be a missing second sex chromosome, and the broader genetic and phenotypic spectrum is now recognized(Claus H Gravholt et al., 2017). However, despite the rapid advances in genetic techniques, genotype-phenotype correlations and molecular mechanisms of disease in TS remain largely unknown(Viuff et al., 2019). There are few data on the variables that influence health outcomes and even less on targeted interventions for this population. In 2017, the international clinical consensus guidelines(Claus H Gravholt et al., 2017) laid the most recent framework for clinical management of girls and women with TS, with an updated guideline due in 2024, but the evidence substantiating most of these recommendations is far from robust and based mostly on expert opinion. Furthermore, we do not know the extent to which clinicians follow these guidelines or their effectiveness in improving clinical outcomes. Hence, as expressed by stakeholders in the TS community(Sandberg et al., 2019), meaningful research is acutely needed to improve the health and well-being of individuals with TS.
Several challenges impede the research landscape in TS. TS is a rare disease with an incidence of 1 in ~2000 live born females, many of whom experience a delay in diagnosis(Sävendahl & Davenport, 2000). Historically, this has led to publications describing small cohorts at single institutions with ascertainment bias resulting in underpowered studies. One recent U.S. population-based study of the prevalence of karyotype-confirmed diagnosis of TS in the first year of life, utilizing data from seven birth defects surveillance programs reflects the challenges in case ascertainment in the absence of nationalized health care registry data(Martin-Giacalone et al., 2023). Larger scale data have been reported from such registries in European countries(Baena et al., 2004; C H Gravholt et al., 1998); however, neither the racial/ethnic composition nor socioeconomic structure in these countries accurately reflect the U.S. population. Furthermore, treatment protocols and medications prescribed in European countries often do not reflect U.S. clinical practice(Donaldson et al., 2019). Although robust cohorts were studied decades ago through both the National Institute of Health (NIH) and pharmaceutical companies marketing growth hormone (Bolar et al., 2008; Gutin et al., 2012), these registries have since dissolved and there is currently minimal federal or industry commitment to TS research. In 2014, the advocacy organization Turner Syndrome Society of the U.S. (TSSUS) created the patient-centered Turner Syndrome Research Registry (TSRR), designed to collect and store patient-reported data from individuals affected by TS to study disease mechanisms and natural history(Prakash et al., 2019). They envisioned participants would have longitudinal access to the registry for updates over time, researchers could be connected to the pool of potential participants, and researchers would enter newly acquired data back into the registry(Prakash et al., 2019). The TSRR improved the framework for collaborative research between researchers and individuals with TS, particularly for patient-reported outcomes, such as individual experiences, perception of factors contributing to care and/or outcomes, and quality of life. However, there are reliability limitations to a primarily patient-reported registry, including the inability to validate data (even the specific karyotype conferring the diagnosis), quantify test results, and study clinical care including variability in management and response to treatment.
To address some of the limitations and complement the TSRR, a new registry infrastructure was developed to capture clinical data utilizing a network of TS-specialty clinics developed through the work of the advocacy organization, Turner Syndrome Global Alliance (TSGA) (https://tsgalliance.org/). The InsighTS (Inspiring New Science to Guide Healthcare in TS) registry (www.insightsregistry.org) launched in 2020 after establishment of a Steering Committee made up of multiple stakeholders that informed the mission and structure of the project. The Steering Committee prioritized collaboration among TS stakeholders (patients, parents, clinicians, and investigators), sustainability (data sharing policies, funding, etc.), transparency, and diversity (nationally representative), with the overarching goal of improving clinical outcomes for individuals with TS. Examples of the type of knowledge that will be gained include: (1) Prevalence of comorbidities in individuals with TS and the factors associated with these comorbidities, (2) Healthcare utilization among individuals with TS across the lifespan (3) Current clinical practices in caring for individuals with TS, and (4) Variables associated with clinical and quality of life outcomes. In addition, InsighTS will serve as an infrastructure for conducting future quality improvement and evidence-based research initiatives as longitudinal data continues to evolve. Herein, we describe the organization and infrastructure of the InsighTS Registry, including demographic data from the initial participants that illustrate the enormous potential of this growing resource for the TS community.
MATERIALS AND METHODS
Leadership and Structure of InsighTS
A Steering Committee composed of twelve voluntary and diverse stakeholders invested in the TS community including clinicians, researchers, patient advocates and members from the TS community was established to lead the InsighTS registry and ensure the project reflects the interests and priorities of the TS community. Steering Committee members are volunteers who commit to a minimum two-year term and members are appointed by TSGA leadership. The Steering Committee meets every 4-6 weeks via teleconference and is tasked with directing the goals of the project, providing governance, reviewing, and approving protocol amendments, participating in addition of new sites, evaluating data use proposals, and overseeing the dissemination of results arising from the InsighTS Registry. Subcommittees are formed as needed to accomplish tasks. Documents finalized and approved by the Steering Committee to date are available on a centrally accessed website for transparency and include the Steering Committee charter, study protocol and consent forms, data use proposal policy, and publication policy.
The University of Colorado serves as the lead site and data coordinating center for the InsighTS Registry. The lead site is responsible for all administrative aspects of InsighTS including the regulatory assurance through a Single Institutional Review Board (SMART IRB), development and maintenance of the REDCap database(Harris et al., 2009), data management and quality control for all sites, training study personnel including developing and maintaining standard operating procedures (SOPs), organizing Steering Committee meetings, preparation of progress reports, and onboarding new sites approved by the Steering Committee. The REDCap database (Research Electronic Data Capture) is a widely used research and HIPAA compliant web-based application(Harris et al., 2009) that is utilized for the data collection tools and participant-facing surveys in the InsighTS Registry. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources. The InsighTS Registry is approved by the Colorado Multiple Institution Review Board (COMIRB), which serves as the single IRB (SMART IRB) and all local site IRBs have agreed to cede to COMIRB.
Any institution that provides clinical care for TS and has the interest and capacity to recruit patients, comply with regulatory processes, and contribute data to the registry each year is eligible to participate in the registry following approval by the Steering Committee. Drafted legal agreements, regulatory documents, and training resources facilitate efficient and successful onboarding of new sites. Participating sites consent and enroll eligible participants, enter, and validate their own participants’ data, and maintain site-specific documentation. Sites always have full access to their own participants’ data and can submit data use proposals to the Steering Committee to acquire additional data from other sites for specific projects. InsighTS has recently expanded to enroll participants who are not affiliated with a specific clinic in the InsighTS network, as long as the participant’s clinical information may be obtained and verified.
The process for adding new sites starts with the site presenting information about their TS clinic and research team to the Steering Committee. The committee then votes based on site capacity and recruitment pool. Once approved, the lead site coordinates with the new site to complete all onboarding requirements including regulatory and legal approvals and protocol training. Regulatory approval includes submitting for the local site IRB to cede to COMIRB. Legal agreement includes both data and materials transfer between the new site and the University of Colorado. The onboarding process takes approximately three months, after which sites can begin to recruit and enroll eligible participants.
Enrollment Criteria
Inclusion criteria include:
A diagnosis of TS as defined by the TS International Clinical Consensus Guidelines( Claus HGravholt et al., 2017) (a phenotypic female having a karyotype with one X chromosome and a complete or partial absence of the second sex chromosome, and one or more clinical manifestations of TS).
A clinic visit at a participating site within the past 12 months
Or
If self-enrolling online without affiliation with a participating clinic, ability to obtain and verify clinical data
Exclusion criteria include:
Participants are excluded from enrollment if a karyotype or microarray cannot be obtained to confirm the TS diagnosis.
Recruitment and Data Acquisition Processes
Study personnel at participating sites recruit eligible participants either through communications via the electronic health record (EHR) system and/or in-person during clinical visits. The goal for each participating site is to have >80% of eligible patients approached and >50% of eligible participants enroll. Operations data will be requested for each participating site (number of individual patients seen, basic demographics, and non-enrollment log including reasons for decline to consent into the registry, if available) to allow comparison between those patients enrolling and those choosing not to enroll, in an effort to identify any selection biases. Patients meeting eligibility criteria may elect to self-enroll online. After written informed consent (and assent if the participant is a minor) is provided, data are abstracted from the patient’s electronic health record (EHR) by a member of the local clinical research team. If not affiliated with a participating site or data are unavailable, outside medical records are requested and the patient’s family or medical provider may be asked to provide clarification. Outside records are reviewed and verified by trained research staff to ensure enrollment criteria are met before they are entered into the database. The participant’s pertinent medical data is added to the registry database. Any subsequent information from follow-up clinic visits is also added to the registry. Efforts are ongoing to export discrete data elements directly from the EHR into REDCap to minimize the burden of data entry.
Outcome measures
Outcome data gathered directly from the participants’ EHR and includes, but is not limited to, the following:
TS diagnosis timing and indication for genetic testing
Medical diagnoses (presence, type, date of diagnosis and resolution, if applicable)
Outpatient clinic visits (dates and types)
Surgical procedures (presence, dates, and type)
Hospitalizations (presence and number, date of admission and discharge, reason for admission)
Treatments including medications (presence, number, type, start and discontinuation dates if applicable)
Results of standardized psychological questionnaires and assessments
Laboratory tests type, date, results
Imaging studies and diagnostic tests, type, date, results
Growth parameters and vital sign measurements
All study data are collected from standard of care visits and procedures, apart from an optional blood draw for a 5-10ml sample of blood, if consent is provided and resources are available at the local institution. The sample is processed for storage of plasma, serum, and buffy coat. These specimens are stored in a biorepository at the CU Anschutz campus with a barcode for future studies involving the assessment of hormones, proteins, metabolites, DNA, RNA, and other studies. The biorepository may be expanded to additional tissue types in the future.
Optional procedures participants can select when enrolling include being added to a recruitment list for future TS-related studies and receiving electronic surveys. InsighTS surveys are sent directly via REDCap to the email address with a participant-specific link and include a demographic survey, access to care, and validated questionnaires on child development and neuropsychological health among others. For participants under 18 years, the surveys are sent to a parent or legal guardian.
Data Quality, Management and Sharing
Data are entered and then separately verified by trained research staff following Standard Operating Procedure documents. If research personnel are uncertain of the correct response or there are conflicting data in the medical record, the variable is flagged for “Clinician Review” and a clinician investigator on the team then uses their judgement of the most accurate clinical assessment. Validation parameters available in REDCap, including minimum and maximum ranges, branching logic with clarifying prompts, and missing data reports, have been implemented where possible, in addition to free text response options for those completing chart review and data entry in order to add clarifying details. The team at the lead site evaluates reports for incomplete variables, outliers, or other concerns and initiates a query that needs to be addressed by the local research team.
In congruence with the purpose of developing the InsighTS registry, the data are available for the betterment of the TS community. Summary data are available through a public link. A data-use policy governs the utilization of participant-level data from the InsighTS registry to protect participants and ensure data will be used in a way that benefits the TS community. All survey, demographic, and clinical data in the database are eligible to be used upon approval. In addition, investigators may propose to use the InsighTS registry for the purpose of contacting potentially eligible subjects for new research studies and/or accessing banked biospecimens when available for a subset of participants. The Steering Committee reviews data use proposals for priority, applicability, feasibility, and ability of the study team to appropriately use the data, as well as the impact of the study on the larger TS community. Data use proposals are required to specify community engagement and dissemination of results to the TS community. Upon publication, deidentified data supporting that publication will be shared through REDCap online report dashboards, and approved data repository supplementary files associated with the publication.
Finally, the InsighTS Steering Committee works closely with the TSRR and iTS (European-based clinical TS registry) with the intent to be able to share and merge data when appropriate. All participants enrolling in the InsighTS Registry are assigned a Global Unique Identifier (GUID) through the secure NICHD GUID Tool(Navale et al., 2019; Rubinstein & McInnes, 2015), allowing individual research participants to be linked in multiple studies without releasing personal health information. This facilitates data sharing for future studies, maximize the contribution and minimizing burden for research participants and their families. Finally, we have shared data dictionaries and selected Common Data Elements where applicable to facilitate merging and integration of databases in the future.
Analytic Approach
Analytic plans for specific projects are required in data use requests and are evaluated for appropriateness and scientific rigor prior to approval. For this publication, descriptive data on demographics are continuously assessed as numbers, percentages, medians/ranges, means/standard deviations as appropriate. These data are also provided in monthly reports as well as made public on the public dashboard public link. Demographic variables from the InsighTS Registry are compared to available TSRR registry data using Wilcoxon ranked sum test for continuous data and chi-squared test for categorial data. An alpha of 0.05 was regarded as statistically significant.
RESULTS
Following Children’s Hospital Colorado, five geographically diverse, nationally recognized, multidisciplinary TS clinics were onboarded as the inaugural InsighTS consortium, including Children’s Hospital of Philadelphia, Children’s National Hospital in Washington DC, Lurie Children’s Hospital in Chicago, University of North Carolina at Chapel Hill, and University of Texas Health Science Center in Houston. Five additional sites have joined the InsighTS consortium since inception including the University of Kansas Medical Center, Cincinnati Children’s Hospital and Medical Center, Seattle Children’s Hospital, University of California San Diego, and University of Iowa. The geographic distribution of all participating sites to date is depicted in Figure 1.
Figure 1:
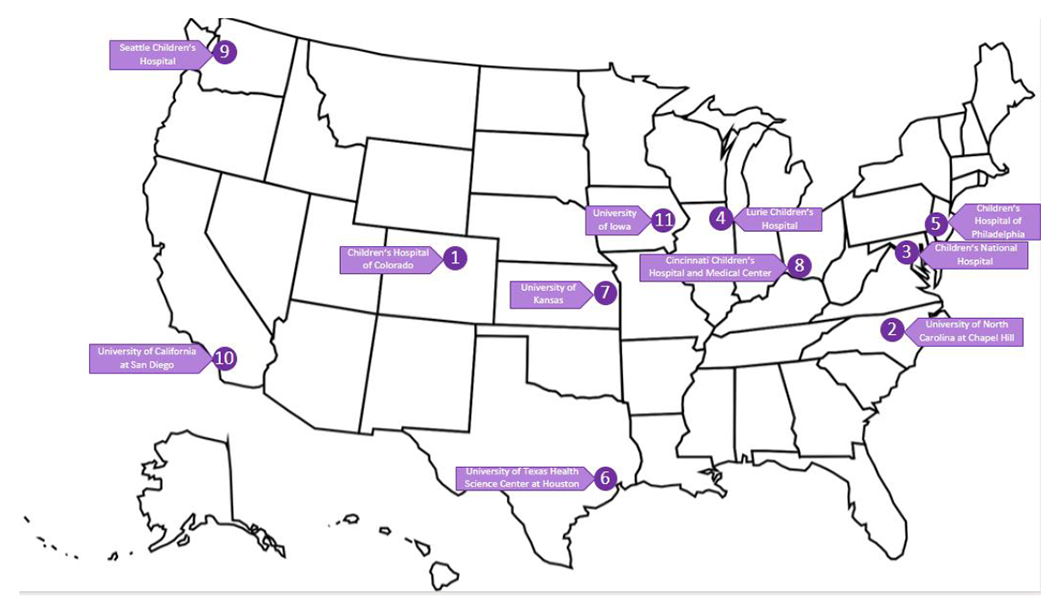
Geographic distribution of sites through the InsighTS Registry
A total of 405 participants have consented to participate in the InsighTS registry as of 03/20/2023, with the majority agreeing to the optional procedures available to them (Figure 2). The rate of enrollment has averaged 13 participants per month (Figure 3). Demographic data for the InsighTS cohort compared to data available from the TSRR are presented in Table 1. The majority of InsighTS participants were <18 years at the time of enrollment (86%), reflecting that most participants have been recruited from pediatric institutions. The self-reported race and ethnicity distribution was more diverse than the TSRR, with a higher percentage of non-white and Hispanic participants (p<0.001 for both race and ethnicity). Diagnostic information, including karyotype, has been confirmed for 61% of participants in InsighTS (the remainder are under review). Approximately two-thirds of participants were diagnosed with TS postnatally, at a median age of 6.0 years (range: 0-37.9). InsighTS participants were less likely to have non-mosaic 45,X and more likely to have mosaic or more complex TS karyotypes compared to self-reported data in the TSRR (p<0.001).
Figure 2.
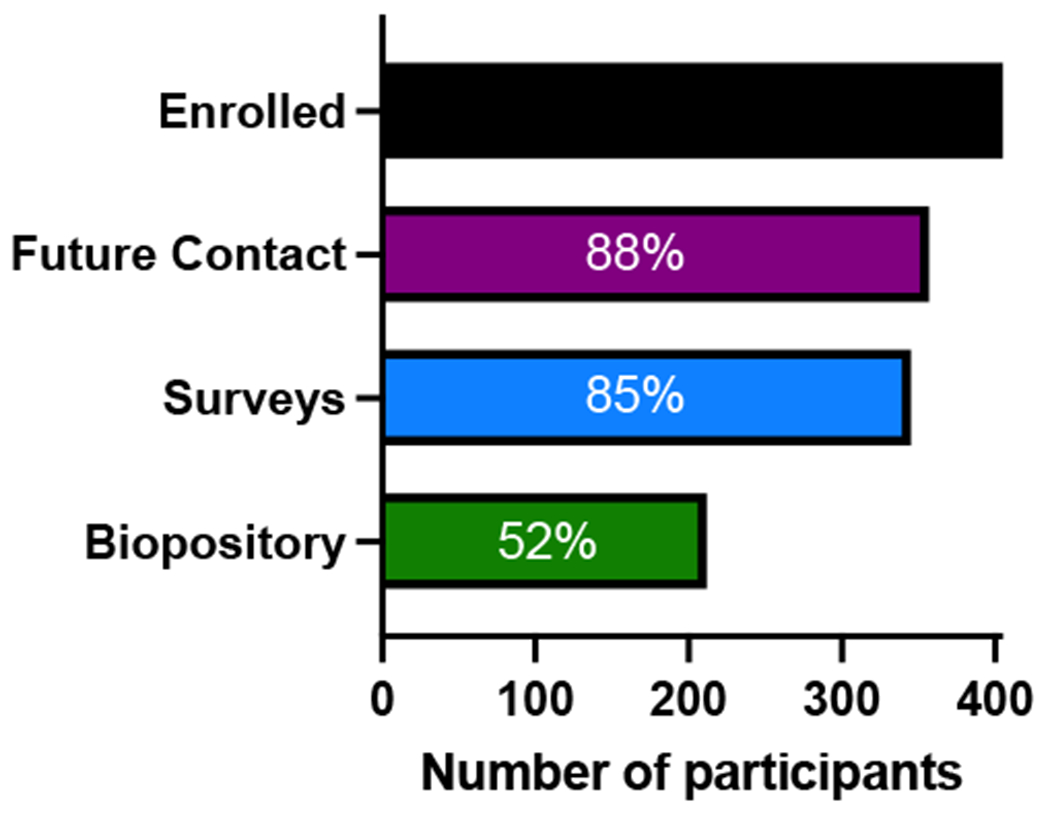
Optional procedures elected during the consent process for the 405 enrolled participants. Not all sites have the resources and/or approval for the biorepository.
Figure 3: Cumulative Recruitment to InsighTS Registry by Site.
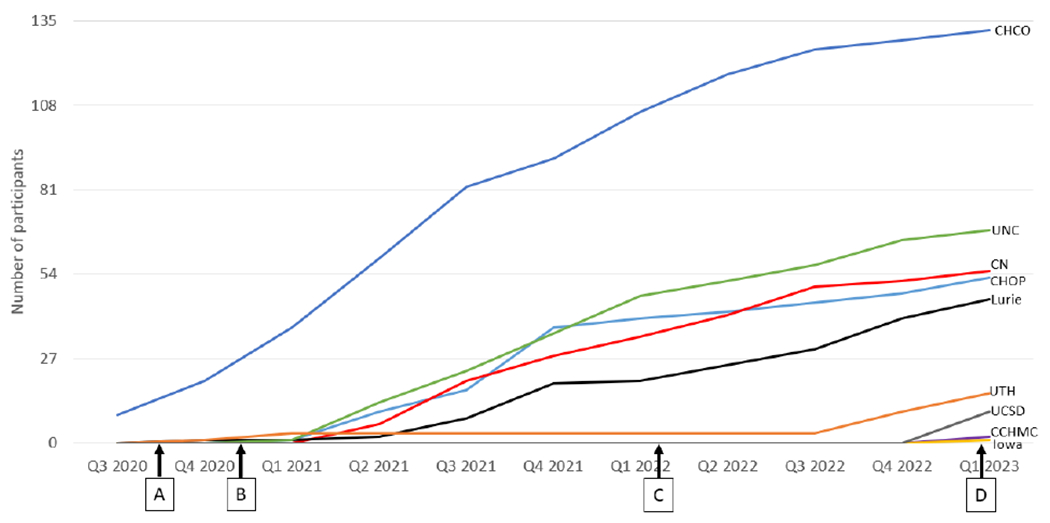
Children’s Hospital of Colorado (CHCO) A. University of Texas Houston (UTH) approved Sept. 2020 B. Approved Dec. 2020: Children’s National Hospital (CN), Children’s Hospital of Philadelphia (CHOP), Lurie Children’s, University of North Carolina (UNC) C. Cincinnati Children’s Hospital and Medical Center (CCHMC) approved Feb 2022 D. University of Iowa approved Jan 2023 and University of California San Diego (UCSD) approved Feb 2023. No participants have been recruited at Kansas University Medical Center and Seattle Children’s Hospital as of 03/20/2023.
Table 1.
Demographic Information at the time of enrollment for the InsighTS Cohort compared with the TSRR registry(Prakash et al., 2019)
| Insights Registry N=405 | TSRR Registry N=1173 | p-value | |||
|---|---|---|---|---|---|
|
| |||||
| Age in years (Median, IQR) | 10.4 (4-15) | 26 (11-40) | <0.001 | ||
|
| |||||
| N | % | N | % | ||
|
| |||||
| Race | <0.001 | ||||
| American Indian or Alaskan Native | 4 | 1.0 | 8 | 0.7 | |
| Asian | 25 | 6.2 | 33 | 2.8 | |
| Black or African American | 35 | 8.6 | 29 | 2.5 | |
| Native Hawaiian or other Pacific Islander | 2 | 0.5 | 1 | 0.09 | |
| White | 276 | 68.1 | 861 | 73.6 | |
| Other | 42 | 10.4 | 78 | 6.7 | |
| Unknown | 21 | 5.2 | 162 | 13.8 | |
|
| |||||
| Ethnicity | <0.001 | ||||
| Hispanic | 86 | 21.2 | 91 | 7.8 | |
| Not Hispanic | 278 | 68.6 | 862 | 73.5 | |
| Unknown | 41 | 10.1 | 220 | 18.7 | |
|
| |||||
| Payor at time of enrollment | |||||
| Medicare/Medicaid | 96 | 23.7 | NA | NA | |
| Private insurance | 206 | 50.9 | NA | NA | |
| Military | 10 | 2.5 | NA | NA | |
| No coverage/self-pay | 3 | 0.7 | NA | NA | |
| 2 or more insurances | 23 | 5.7 | NA | NA | |
| Other | 7 | 2.7 | NA | NA | |
| Unknown | 60 | 14.8 | 1173 | 100 | |
|
| |||||
| Karyotype Known | 248 | 61.2 | 425 | 36.2 | <0.001 |
|
| |||||
| Karyotype Category 1 | <0.001 | ||||
| Monosomy X (45,X) | 98 | 39.5 | 273 | 64.2 | |
| 45,X/46,XX | 39 | 15.7 | 48 | 11.3 | |
| 45,X/47,XXX or 45,X/46,XX/47,XXX | 21 | 8.5 | 2 | 0.5 | |
| 45,X/46,XY or 46,X with isochromosome Y, ring Y, or deletion Y w/ or w/o 45,X mosaicism | 16 | 6.5 | 20 | 4.7 | |
| 46,X with deletion on X chromosome w/ or w/o 45,X mosaicism | 9 | 3.7 | 0 | 0 | |
| 46,X with ring X w/ or w/o 45,X mosaicism | 22 | 8.9 | 1 | 0.2 | |
| 45,X or 46,X with isochromosome Xq or isodicentric Xp w/ or w/o 45,X mosaicism | 26 | 10.4 | 3 | 0.7 | |
| Other karyotypes | 17 | 6.8 | 78 | 18.4 | |
|
| |||||
| Timing of Turner Syndrome Diagnosis 1 | <0.001 | ||||
| Prenatal confirmed | 65 | 24.9 | 80 | 13.4 | |
| Prenatal screen, confirmed postnatally | 29 | 11.1 | NA2 | NA2 | |
| Postnatal | 167 | 64.0 | 516 | 86.6 | |
Percents calculated from the total of those with available data. InsighTS data are confirmed by medical record review, TSRR are self-reported.
TSRR did not have this category.
DISCUSSION
The InsighTS Registry is a collaborative effort among TS stakeholders to collect and store prospective clinical data in a centralized database, representing a large and diverse group of individuals with TS in the US. The InsighTS Registry is committed to improving the diversity, equity, and representation of patient community voices in every phase of research planning, implementation, and dissemination. Within a short amount of time, InsighTS has enrolled >400 individuals with TS across the US, representing a wide geographical, racial, ethnic, and socioeconomic sample. InsighTS is continuing to enroll participants and collecting new data, with the expectation of serving as a resource for natural history studies for individuals with TS for decades to come. Indeed, rare disease registries are recognized as important contributors to evidence-based personalized medicine, and help enhance diagnostic and therapeutic strategies to improve patient care for rare diseases under real-world conditions15.
InsighTS is the only U.S. multi-center study independent of industry-initiated trials and represents a diverse and nationally representative cohort of individuals with TS, as reflected in the cohort demographics that approximate the 2020 US population census data16. Prior natural history cohorts have been investigator-initiated, limited to single institutions, and comprised of motivated participants willing and able to travel for participation in research17. In contrast, the InsighTS registry is driven by a team of stakeholders from the TS community and enables participants to enroll in their local clinics or even online, with common data elements from their EHR populated into the research database. We hope that targeting >80% of patients seen in these dedicated clinics for enrollment, coupled with online self-enrollment option will provide a greater opportunity within the TS community and expand access for participants from a wider age range, geographic location, and severity on the clinical spectrum to meaningfully contribute to research without undue burden on the participants.
InsighTS is not the first registry for the TS population. The TSRR was established under a funded initiative with Genetic Alliance using the platform for engaging everyone responsibly (PEER) and has since transitioned to a new platform11. The TSRR focuses on patient provided data via surveys, which prioritize the patient voice, but is by design, subjective11. InsighTS requires clinician-validated data, which is a more reliable approach for accurate diagnostic and medical outcome data. The comparison of missing/unreported data between InsighTS and TSRR supports this difference. In addition, the karyotype categories in InsighTS are similar to those reported in previous studies, while the proportion of those in the TSRR reporting a non-mosaic 45,X is much higher than expected, likely reflecting that many individuals do not actually know their specific karyotype. There are other notable differences between the registry cohorts as well, with InsighTS participants significantly younger and more likely to be prenatal diagnosed, reflecting a change since non-invasive prenatal screening for fetal aneuploidies has become standard of care. The registry will also likely help ascertain the differences in clinical outcomes for those diagnosed incidentally or prenatally compared with those diagnosed later.
Limitations
One of the initial limitations was the reliance on academic centers to recruit patients but we have tried to overcome the issue with the approval for individuals to self-enroll online and then request their physicians to provide clinical data. The current sites are mostly pediatric (in contrast to the TSRR registry that contains predominantly adult participants) but there are ongoing efforts to bring additional adult TS clinics on board. In addition, we are also diversifying the Steering Committee with the inclusion of a geneticist and persons with TS. The EHR, even when verified by the treating physicians, may still contain errors of omission or commission that may impact the quality of the data. Another limitation is the lack of funding for sites to enter data, such that data collection is dependent on investigator time. We continue to explore sources of funding for coordinators as it will help with data collection and support more TS clinics to participate in this registry. Additional efforts are also ongoing to improve the diversity in age, racial/ethnic identification, and geography (including rural individuals) and address inequities in research by improving engagement with the TS community.
Future Directions
InsighTS has a goal of recruitment of at least 500 individuals by 2024 and 1,000 by 2026, with intention to improve age, racial, ethnic, socioeconomic, and geographic diversity to best represent the US TS population. To achieve these goals, InsighTS remains open to new participating sites in addition to the recent change to include online enrollment with validated medical records. To facilitate continued growth and sustainability, we plan to secure additional funding to enable direct and ongoing data capture from different electronic medical record systems across institutions. InsighTS intends to support a breadth of future research initiatives, including cross-sectional, natural history, and comparative effectiveness research that will inform best care practices for patients with TS. Several specific research projects have already been developed and approved to use InsighTS data, including early anxiety recognition, comparison of prenatal and postnatal echocardiograms in prenatally diagnosed individuals, study of outcomes and complications related to cardiac surgery, and unique features of individuals with a 47,XXX cell line18. The established foundation of InsighTS will enable unprecedented patient-centered research for individuals with TS and will serve as a model for rare disease registries nationwide.
CONCLUSIONS
The InsighTS Registry, a clinical research registry for individuals with TS developed by all stakeholder perspectives is large, diverse, and nationally representative. InsighTS provides opportunities for the TS community to 1) participate in clinical research 2) propose research projects utilizing the data collected or could be obtained under the existing infrastructure (any EHR data, survey data for those agreeing to participate, and a subset of biorepository samples) by submitting data use proposals to the Steering Committee 3) facilitate the dissemination of information and results from clinical studies to flow back to the community. InsighTS is poised to serve as a resource uniting participants and researchers in the TS community and providing a conduit for future longitudinal assessment of natural history outcomes research as well as clinical trials that will ultimately shape clinical care guidelines and improve care for individuals with TS.
ACKNOWLEDGEMENTS
We are grateful to Turner Syndrome Global Alliance (TSGA) for their perseverance, leadership, and financial investment in InsighTS. We are thankful for all the TS advocacy organizations, including TSGA and Turner Syndrome Society of the US (TSSUS), that support the patient community and educate individuals with TS and their families on the value of research. The authors thank the participants who have enrolled in the InsighTS registry thus far and the families who have invested in this collaborative effort. We thank the coordinators and principal investigators at each participating institution who have helped with recruitment and TSGA for advertising the registry on their websites and social media platforms.
CONFLICT OF INTEREST STATEMENT
In addition to contribution to the InsighTS Registry, several authors contribute to Turner syndrome industry studies including those sponsored by Ascendis (SD, JL, WB, IGL, KK), Pfizer (VB), Lumos (VB) and Novo Nordisk (IGL). These companies did not have any involvement in the development of the InsighTS Registry or preparation of this manuscript.
JL has received consultant funds from Ascendis. S.P. is supported by a gift from the Turner Syndrome Society of the United States and a grant from the National Science Foundation (2129088). CTP is supported by a K12 grant (HD27748). SD is supported by grants from NIH (NICHD and NIDDK), Boettcher Foundation, TSGA, and CU SOM Department of Pediatrics.
Footnotes
WEBSITES
Turner Syndrome Global Alliance (TSGA) (https://tsgalliance.org/)
InsighTS (Inspiring New Science to Guide Healthcare in TS) registry (www.insightsregistry.org)
InsighTS Summary Data (public link)
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available on the public dashboard public link
REFERENCES
- Baena N, De Vigan C, Cariati E, Clementi M, Stoll C, Caballín MR, & Guitart M (2004). Turner syndrome: evaluation of prenatal diagnosis in 19 European registries. American Journal of Medical Genetics. Part A, 129A(1), 16–20. 10.1002/ajmg.a.30092 [DOI] [PubMed] [Google Scholar]
- Bolar K, Hoffman AR, Maneatis T, & Lippe B (2008). Long-term safety of recombinant human growth hormone in turner syndrome. The Journal of Clinical Endocrinology and Metabolism, 93(2), 344–351. 10.1210/jc.2007-1723 [DOI] [PubMed] [Google Scholar]
- Donaldson M, Kriström B, Ankarberg-Lindgren C, Verlinde S, van Alfen-van der Velden J, Gawlik A, van Gelder MMHJ, & Sas T. (2019). Optimal Pubertal Induction in Girls with Turner Syndrome Using Either Oral or Transdermal Estradiol: A Proposed Modern Strategy. Hormone Research in Paediatrics, 91(3), 153–163. 10.1159/000500050 [DOI] [PubMed] [Google Scholar]
- Gravholt CH, Juul S, Naeraa RW, & Hansen J. (1998). Morbidity in Turner syndrome. Journal of Clinical Epidemiology, 51(2), 147–158. 10.1016/s0895-4356(97)00237-0 [DOI] [PubMed] [Google Scholar]
- Gravholt Claus H, Andersen NH, Conway GS, Dekkers OM, Geffner ME, Klein KO, Woelfle J, Backeljauw PF, & der Velden J. van. (2017). Clinical practice guidelines for the care of girls and women with Turner syndrome: proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. European Journal of Endocrinology, 177(3), G1–G70. 10.1530/EJE-17-0430 [DOI] [PubMed] [Google Scholar]
- Gutin L, Collier S, Bakalov VK, & Bondy C (2012). Trends in GH use in a Turner syndrome natural history study. Pediatric Endocrinology Reviews: PER, 9 Suppl 2(Suppl 2), 725–727. [PMC free article] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, & Conde JG (2009). Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin-Giacalone BA, Lin AE, Rasmussen SA, Kirby RS, Nestoridi E, Liberman RF, Agopian AJ, Carey JC, Cragan JD, Forestieri N, Leedom V, Boyce A, Nembhard WN, Piccardi M, Sandidge T, Shan X, Shumate CJ, Stallings EB, Stevenson R, & Lupo PJ (2023). Prevalence and descriptive epidemiology of Turner syndrome in the United States, 2000-2017: A report from the National Birth Defects Prevention Network. American Journal of Medical Genetics. Part A, 191(5), 1339–1349. 10.1002/ajmg.a.63181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Navale V, Ji M, Vovk O, Misquitta L, Gebremichael T, Garcia A, Fann Y, & McAuliffe M (2019). Development of an informatics system for accelerating biomedical research. F1000Research, 8, 1430. 10.12688/f1000research.19161.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prakash SK, Lugo-Ruiz S, Rivera-Dávila M, Rubio NJ, Shah AN, Knickmeyer RC, Scurlock C, Crenshaw M, Davis SM, Lorigan GA, Dorfman AT, Rubin K, Maslen C, Bamba V, Kruszka P, & Silberbach M (2019). The Turner syndrome research registry: Creating equipoise between investigators and participants. American Journal of Medical Genetics. Part C, Seminars in Medical Genetics, 181(1), 135–140. 10.1002/ajmg.c.31689 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubinstein YR, & McInnes P (2015). NIH/NCATS/GRDR® Common Data Elements: A leading force for standardized data collection. Contemporary Clinical Trials, 42, 78–80. 10.1016/j.cct.2015.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandberg DE, Singer D, Bugajski B, Gebremariam A, Scerbak T, Dooley Maley KL, Scurlock C, Culin D, Eder S, & Silberbach M (2019). Research priorities of people living with Turner syndrome. American Journal of Medical Genetics. Part C, Seminars in Medical Genetics, 181(1), 43–51. 10.1002/ajmg.c.31676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sävendahl L, & Davenport ML (2000). Delayed diagnoses of Turner’s syndrome: proposed guidelines for change. The Journal of Pediatrics, 137(4), 455–459. 10.1067/mpd.2000.107390 [DOI] [PubMed] [Google Scholar]
- TURNER HH (1938). A SYNDROME OF INFANTILISM, CONGENITAL WEBBED NECK, AND CUBITUS VALGUS1. Endocrinology, 23(5), 566–574. 10.1210/endo-23-5-566 [DOI] [PubMed] [Google Scholar]
- Viuff M, Skakkebaek A, Nielsen MM, Chang S, & Gravholt CH (2019). Epigenetics and genomics in Turner syndrome. American Journal of Medical Genetics. Part C, Seminars in Medical Genetics, 181(1), 68–75. 10.1002/ajmg.c.31683 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are openly available on the public dashboard public link