

Visual Abstract

Keywords: GN, Henoch-Schonlein purpura (IgA vasculitis), kidney biopsy
Abstract
Background
Nephritis is a common manifestation of IgA vasculitis and is morphologically indistinguishable from IgA nephropathy. While MEST-C scores are predictive of kidney outcomes in IgA nephropathy, their value in IgA vasculitis nephritis has not been investigated in large multiethnic cohorts.
Methods
Biopsies from 262 children and 99 adults with IgA vasculitis nephritis (N=361) from 23 centers in North America, Europe, and Asia were independently scored by three pathologists. MEST-C scores were assessed for correlation with eGFR/proteinuria at biopsy. Because most patients (N=309, 86%) received immunosuppression, risk factors for outcomes were evaluated in this group using latent class mixed models to identify classes of eGFR trajectories over a median follow-up of 2.7 years (interquartile range, 1.2–5.1). Clinical and histologic parameters associated with each class were determined using logistic regression.
Results
M, E, T, and C scores were correlated with either eGFR or proteinuria at biopsy. Two classes were identified by latent class mixed model, one with initial improvement in eGFR followed by a late decline (class 1, N=91) and another with stable eGFR (class 2, N=218). Class 1 was associated with a higher risk of an established kidney outcome (time to ≥30% decline in eGFR or kidney failure; hazard ratio, 5.84; 95% confidence interval, 2.37 to 14.4). Among MEST-C scores, only E1 was associated with class 1 by multivariable analysis. Other factors associated with class 1 were age 18 years and younger, male sex, lower eGFR at biopsy, and extrarenal noncutaneous disease. Fibrous crescents without active changes were associated with class 2.
Conclusions
Kidney outcome in patients with biopsied IgA vasculitis nephritis treated with immunosuppression was determined by clinical risk factors and endocapillary hypercellularity (E1) and fibrous crescents, which are features that are not part of the International Study of Diseases of Children classification.
Introduction
IgA vasculitis is characterized by IgA-dominant immune complex deposits affecting the small blood vessels of the skin, gut, and kidney with associated arthralgias or arthritis and cutaneous leukocytoclastic vasculitis. Kidney involvement results in IgA vasculitis nephritis that is morphologically indistinguishable from IgA nephropathy and which share common pathogenic mechanisms, including elevated levels of galactose-deficient IgA1 in the serum resulting in immune complex formation and deposition in glomeruli.1–7 Although IgA vasculitis nephritis is most often observed in children, the frequency of kidney involvement is higher in adults.4,5
The histologic classification of IgA vasculitis nephritis most often used is the International Study of Diseases of Children (ISKDC) system.8 Although ISKDC grading correlates with kidney outcomes, it has several limitations: More than 70% of biopsies fall into just two of six histologic grades (II and III); grades III, IV, and V are distinguished solely by the proportion of glomeruli with crescents, and it does not consider chronic tubulointerstitial or glomerular changes that are associated with poor outcomes in other kidney diseases.8–14 Conversely, the Oxford MEST-C score in IgA nephropathy includes both active and chronic lesions, has been extensively validated to correlate with kidney outcomes independent of clinical variables, and is included in the International IgA Nephropathy Prediction Tool as the Kidney Disease Improving Global Outcomes–recommended method for patient risk stratification.12,15–19 To date, there are limited data on the value of MEST-C in IgA vasculitis nephritis, with variable results as to which lesions are associated with kidney function decline.20–24 Furthermore, the use of traditional kidney outcome measures such as threshold reductions in eGFR or kidney failure is limited by the frequent use of immunosuppression which likely contributes to short-term improvement in kidney function with nonlinear change in eGFR over time, resulting in too few outcome events.25 As a result, the value of MEST-C scores in predicting kidney outcomes in IgA vasculitis nephritis remains unclear.
We used an international cohort of adults and children with IgA vasculitis nephritis from Europe, North America, and Asia with independent pathology review to evaluate the association between MEST-C scores and clinical disease activity at baseline and their association with kidney outcomes independent of clinical risk factors and despite treatment with commonly used immunosuppression. To address the limitations of traditional kidney outcomes in IgA vasculitis nephritis, we used latent class mixed models (LCMMs) to identify groups of patients with different nonlinear eGFR trajectories over time that could then be used to evaluate risk factors associated with different eGFR trajectories.
Methods
Study Population
The study population comprised 23 cohorts of adults or children (N=369) with IgA vasculitis nephritis on kidney biopsy, cutaneous purpura or petechiae, and without another secondary cause. The cohorts were from centers in Japan (N=8), the United States (N=5), Italy (N=5), Germany (N=2), China (N=1), France (N=1), and Finland (N=1). We excluded patients with kidney failure (as defined below) at the time of biopsy or without available eGFR data at biopsy or during follow-up.
Kidney Biopsies
Whole slide images for each biopsy were independently scored by three different pathologists blinded to other study data using the form shown in Supplemental Figure 1 to generate the histology scores shown in Supplemental Table 1, which include MEST-C scores in addition to fibrous crescents as an additional marker of disease chronicity and glomerular thrombotic microangiopathy and fibrinoid necrosis as additional active lesions that can be seen in IgA vasculitis nephritis.12,15,26 Further details are in the Supplemental Methods.
Variable Definitions
BP was normalized to adult values so that they were comparable across the age range in the cohort.27 Proteinuria was standardized to body surface area (g/d per 1.73 m2).28 eGFR was from creatinine values using the full age spectrum formula.29 The use of medications that block the renin–angiotensin system or immunosuppression was categorized on the basis of treatment onset before or after kidney biopsy. Kidney failure was the first occurrence of a permanent reduction in eGFR <15 ml/min per 1.73 m2, dialysis, or kidney transplantation. Additional details are provided in the Supplemental Methods.
Statistical Analysis
Evaluation of histologic risk factors was conducted using a similar approach to that used for the derivation of the MEST-C scores for IgA nephropathy.12,15 The inter-rater reliability for the three pathologists scoring the histologic lesions was assessed using Gwet's first-order or second-order agreement coefficient for ordinal variables.30,31 The correlation of each histologic lesion with eGFR and proteinuria at biopsy was evaluated using Spearman correlation coefficient.32 The association of histologic and clinical variables with kidney outcomes was evaluated using LCMM, an approach used previously to evaluate eGFR trajectories in cohorts with CKD.33–35 Because most of the cohort was treated with immunosuppression after biopsy (N=309, 86%), potentially modifying eGFR trajectory over time, this analysis was conducted only in treated patients. The LCMM approach is conducted in two steps. First, heterogeneity in the patterns of eGFR trajectory over time (with each patient censored at the end of follow-up) is explored using mixed models that contain no variables for patient-level characteristics other than the starting eGFR. This allows for identification of underlying groups, or latent classes, of different eGFR trajectory patterns within the data. We identified two such groups, one characterized by an initial improvement in eGFR followed by a delayed progressive decline (referred to as initial improvement/late decline) and a second characterized by stable eGFR after biopsy (referred to as stable disease). In the second step, logistic regression models were used to evaluate the association of histologic and clinical variables with a two-level categorical outcome defined for each patient on the basis of their latent class group assignment. This allows for the identification of variables associated with either latent class group. The histologic variables and all available clinical variables were considered in unadjusted and multivariable logistic regression models using backwards variable selection with a P value threshold <0.05. Further details are provided in the Supplemental Methods.
Results
The analytic cohort comprised 361 patients with IgA vasculitis nephritis, including 99 adults and 262 children (Tables 1 and 2 and Supplemental Figure 2). The median time from clinical disease onset to kidney biopsy was 2.0 months (interquartile range [IQR], 1.2–5.1), with eGFR and proteinuria at biopsy 103 ml/min per 1.7 m2 and 3.0 g/d, respectively (IQR, 77.4–120.0 and 1.0–7.3, respectively). On the basis of the study inclusion criteria, all patients had cutaneous vasculitis, and 257 (71%) had additional features of extrarenal involvement. Immunosuppression after biopsy was used in 309 patients (86%). Over a median follow-up of 2.7 years (IQR, 1.2–5.1), five patients (1%) died, and 11 (3%) progressed to kidney failure.
Table 1.
Description of the analytic cohort at biopsy
| Characteristics at Biopsy | Overall | Adults | Children | Initial Improvement/Late Decline Group | Stable Disease Group |
|---|---|---|---|---|---|
| No. of patients | 361 | 99 | 262 | 91 | 218 |
| Time from clinical onset to biopsy, mo | 2.0 (1.2–5.1) | 2.9 (1.1–9.5) | 1.9 (1.2–3.9) | 1.3 (0.9–2.2) | 2.1 (1.2–5.6) |
| Age, yr | 10.0 (7.0–22.0) | 45.0 (30.0–61.0) | 8.0 (6.0–11.0) | 10.0 (7.0–14.0) | 11.0 (7.0–23.0) |
| Age 18 yr and younger, n (%) | 262 (73) | 0 (0) | 262 (100) | 75 (82) | 154 (71) |
| Male sex, n (%) | 191 (53) | 44 (44) | 147 (56) | 57 (63) | 108 (50) |
| Ethnicity, n (%) | |||||
| Asian | 140 (39) | 66 (67) | 74 (28) | 26 (29) | 85 (39) |
| Black | 6 (2) | 0 (0) | 6 (2) | 1 (1) | 4 (2) |
| White | 207 (57) | 33 (33) | 174 (66) | 62 (68) | 125 (57) |
| Other | 8 (2) | 0 (0) | 8 (3) | 2 (2) | 4 (2) |
| eGFR, ml/min per 1.73 m2 | 103 (77–120) | 88 (61–108) | 110 (84–120) | 84 (59–107) | 109 (85–120) |
| Standardized MAP, mm Hg | 85 (77–95) | 87 (81–99) | 84 (76–93) | 88 (81–96) | 85 (77–95) |
| Proteinuria, g/d | 3.0 (1.0–7.3) | 1.3 (0.6–3.0) | 4.1 (1.5–8.6) | 4.4 (1.6–10.5) | 3.1 (0.9–6.7) |
| Extrarenal noncutaneous disease, n (%) | 257 (71) | 51 (52) | 206 (79) | 75 (82) | 152 (70) |
| Presence of hematuria, n (%) | 348 (96) | 93 (94) | 255 (97) | 88 (97) | 211 (97) |
| Renin–angiotensin system blockade use at biopsy, n (%) | 105 (29) | 36 (37) | 69 (27) | 30 (33) | 60 (28) |
| Immunosuppression use before biopsy, n (%) | 232 (64) | 50 (51) | 182 (70) | 68 (75) | 149 (68) |
| Corticosteroids alone | 181 (78) | 39 (78) | 142 (78) | 53 (78) | 114 (76) |
| Cyclophosphamide±antimetabolitesa | 13 (5) | 2 (4) | 11 (6) | 3 (4) | 10 (7) |
| Antimetabolitesa | 13 (5) | 1 (2) | 12 (7) | 6 (9) | 7 (5) |
| Othera | 25 (12) | 8 (16) | 17 (9) | 6 (9) | 18 (12) |
| Presence of glomerular fibrinoid necrosis, n (%) | 16 (4) | 5 (5) | 11 (4) | 4 (4) | 12 (6) |
| Presence of glomerular TMA, n (%) | 5 (1) | 1 (1) | 4 (2) | 2 (2) | 3 (1) |
| Presence of fibrous crescents, n (%) | 77 (21) | 32 (32) | 45 (17) | 11 (12) | 57 (26) |
| MEST-C scores, n (%) | |||||
| M1 | 131 (36) | 10 (10) | 121 (46) | 42 (46) | 79 (36) |
| E1 | 254 (70) | 61 (62) | 193 (74) | 75 (82) | 148 (68) |
| S1 | 177 (49) | 53 (54) | 124 (47) | 37 (41) | 117 (54) |
| T0 | 346 (96) | 89 (90) | 257 (98) | 87 (96) | 208 (95) |
| T1 or T2 | 15 (4) | 10 (10) | 5 (2) | 4 (4) | 10 (5) |
| C0 | 158 (44) | 45 (46) | 113 (43) | 30 (33) | 90 (41) |
| C1 | 159 (44) | 43 (43) | 116 (44) | 44 (48) | 101 (46) |
| C2 | 44 (12) | 11 (11) | 33 (13) | 17 (19) | 27 (12) |
Data presented for the subgroups on the basis of adults versus children is in the entire cohort (N=361). Data presented for the subgroups on the basis of initial improvement/late decline versus stable eGFR trajectory over time are in the patients treated with immunosuppression after biopsy (N=309). Each patient was assigned to either the initial improvement/late decline or stable disease subgroup of eGFR trajectory on the basis of the highest posterior probability from the latent class mixed model. Data presented as median (interquartile range) or count (frequency). eGFR was using the full age spectrum formula, and mean arterial pressure was standardized to adult values, as outlined in the methods. Proteinuria values in children were standardized to body surface area (1.73 m2). MAP, mean arterial pressure; TMA, thrombotic microangiopathy.
With or without corticosteroids. Antimetabolites include mycophenolate mofetil and azathioprine.
Table 2.
Description of the analytic cohort during follow-up
| Characteristics during Follow-Up | Overall | Adults | Children | Initial Improvement/Late Decline Group | Stable Disease Group |
|---|---|---|---|---|---|
| No. of patients | 361 | 99 | 262 | 91 | 218 |
| Follow-up, yr | 2.7 (1.4–5.1) | 3.4 (1.3–6.7) | 2.5 (1.4–4.7) | 2.5 (1.3–5.2) | 2.7 (1.4–4.9) |
| Renin–angiotensin system blockade use after biopsy, n (%) | 267 (74) | 64 (65) | 203 (78) | 80 (88) | 157 (72) |
| Immunosuppression use after biopsy, n (%) | 309 (86) | 80 (81) | 229 (88) | 91 (100) | 218 (100) |
| Corticosteroids alone | 131 (43) | 61 (76) | 70 (31) | 29 (32) | 102 (47) |
| Cyclophosphamide±antimetabolitesa | 50 (16) | 3 (4) | 47 (20) | 19 (21) | 31 (14) |
| Antimetabolitesa | 78 (25) | 8 (10) | 70 (31) | 28 (31) | 50 (23) |
| Othera | 50 (16) | 8 (10) | 42 (18) | 15 (16) | 35 (16) |
| Duration of immunosuppression use after biopsy, wk | 53 (28–96) | 58 (34–85) | 49 (26–97) | 50 (30–88) | 55 (27–98) |
| Death, n (%) | 5 (1) | 5 (5) | 0 (0) | 0 (0%) | 4 (2) |
| Progression to kidney failure, n (%) | 11 (3) | 2 (2) | 9 (3) | 5 (6) | 6 (3) |
Data presented for the subgroups on the basis of adults versus children are in the entire cohort (N=361). Data presented for the subgroups on the basis of the initial improvement/late decline versus stable eGFR trajectory over time are in the patients treated with immunosuppression after biopsy (N=309). Each patient was assigned to either the initial improvement/late decline or stable disease subgroup of eGFR trajectory on the basis of the highest posterior probability from the latent class mixed model. Data presented as median (interquartile range) or count (frequency).
With or without corticosteroids. Antimetabolites include mycophenolate mofetil and azathioprine. Kidney failure was the first occurrence of dialysis, transplantation, or a permanent reduction in eGFR <15 ml/min per 1.73 m2.
Histologic Characteristics
Histologic characteristics of the cohort are described in Table 1. T1 or T2 scores were infrequent but were more common in adults than children. Measures of disease activity, including M1 (36%), E1 (70%), and C1 or C2 (57%) scores, were relatively frequent, with M1 more common in children but E1 and crescents similar across age groups. Glomerular fibrinoid necrosis (4%) and glomerular thrombotic microangiopathy (1%) were infrequently seen. The E1 and S1 scores had inter-rater reliability values of 0.59 and 0.44, respectively, indicating moderate agreement between pathologists, similar to the scoring for these lesions in IgA nephropathy.26,36 All remaining lesions had inter-rater reliability values >0.6 indicating good or very good agreement between pathologists (Table 3).
Table 3.
Inter-rater reliability for histology features
| Histology Features | Inter-Rater Reliability (95% CI) |
|---|---|
| Presence of fibrous crescents | 0.93 (0.91 to 0.95) |
| Presence of glomerular TMA | 0.93 (0.91 to 0.96) |
| Presence of glomerular fibrinoid necrosis | 0.90 (0.87 to 0.93) |
| M1 | 0.71 (0.65 to 0.77) |
| E1 | 0.59 (0.52 to 0.65) |
| S1 | 0.44 (0.37 to 0.51) |
| T0 | 0.98 (0.98 to 0.99) |
| T1 or T2 | |
| C0 | 0.80 (0.77 to 0.84) |
| C1 | |
| C2 |
Each biopsy was reviewed independently by three different pathologists. The inter-rater reliability reflects the agreement between pathologists, with values 0.41–0.59 indicating moderate and values ≥0.6 indicating good or very good agreement. CI, confidence interval; TMA, thrombotic microangiopathy.
The correlations between histologic lesions and eGFR and proteinuria at biopsy are shown graphically in Figure 1, with Spearman correlation coefficients in Supplemental Table 2. eGFR at biopsy was lower in patients with higher T and C scores, although the magnitude of the Spearman correlation coefficients suggested a weak correlation (<0.3). Proteinuria at biopsy was greater in patients with higher M, E, and C scores, and in those with glomerular fibrinoid necrosis, while proteinuria was lower in those with higher T scores, with the Spearman correlation coefficients suggesting weak (<0.3) or moderate (0.3–0.39) correlation. Other histologic lesions were not associated with eGFR or proteinuria at biopsy. The relative changes in proteinuria and eGFR according to categories of histologic lesions were similar when evaluated separately in adults versus children (Supplemental Figure 3).
Figure 1.

Proteinuria and eGFR at biopsy on the basis of histologic lesions. Data are presented as median values (squares) and 25th/75th percentiles (whiskers). Proteinuria is presented on a log (base 2) scale. TMA, thrombotic microangiopathy.
Trajectories of eGFR Over Time
Trajectories of eGFR were analyzed in the subgroup of 309 patients treated with immunosuppression after biopsy because treatment modified eGFR trajectory (Supplemental Figure 4), and those treated with immunosuppression had worse clinical and histologic characteristics (Supplemental Table 3). LCMM analysis was used to identify patterns of eGFR trajectories over time based only on heterogeneity in the data and as such is agnostic to any a priori assumptions regarding potential risk factors or anticipated outcomes. Two distinct subgroups with different eGFR trajectories were identified (Figure 2). One group was characterized by an initial improvement followed by a decline in eGFR starting 3–4 years after biopsy (initial improvement/late decline), and a second was characterized by stable eGFR after biopsy (stable disease). The composite outcome of a 30% decline in eGFR or kidney failure occurred in 24 patients (8%) and was more frequent in the initial improvement/late decline compared with the stable disease subgroup with a 5-year risk of 15% (95% confidence interval [CI], 4% to 25%) versus 3% (95% CI, 0% to 6%; P < 0.0001, Figure 3) and a hazard ratio of 5.84 (95% CI, 2.37 to 14.4; P = 0.0001). This confirms the eGFR trajectories identified by LCMM were associated with an established outcome in kidney disease. As shown in Tables 1 and 2, the initial improvement/late decline group had more children (83% versus 71%), male patients (63% versus 50%), and extrarenal noncutaneous disease (82% versus 67%), with lower eGFR at biopsy (84 versus 109 ml/min per 1.73 m2). There was no difference in the type of immunosuppression use between the two groups.
Figure 2.
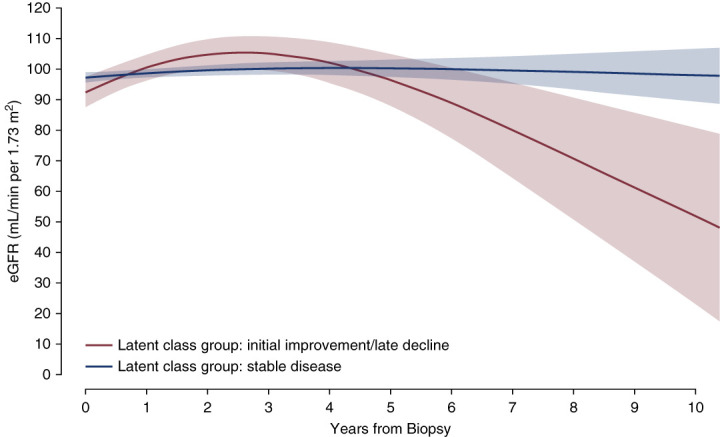
Two subgroups of eGFR trajectories over time that were identified in the cohort. Among those patients treated with immunosuppression after biopsy, two subgroups were identified using LCMMs that did not include any patient-level variables other than starting eGFR. As such, these subgroups were identified on the basis of heterogeneity within the data and are agnostic to any clinical or histologic characteristics. For illustration, this figure is based on a model with starting eGFR at biopsy 101 ml/min per 1.73 m2 (which corresponds to the median eGFR at biopsy in those treated with immunosuppression). The shaded bands represent 95% CIs. CI, confidence interval; LCMM, latent class mixed model.
Figure 3.
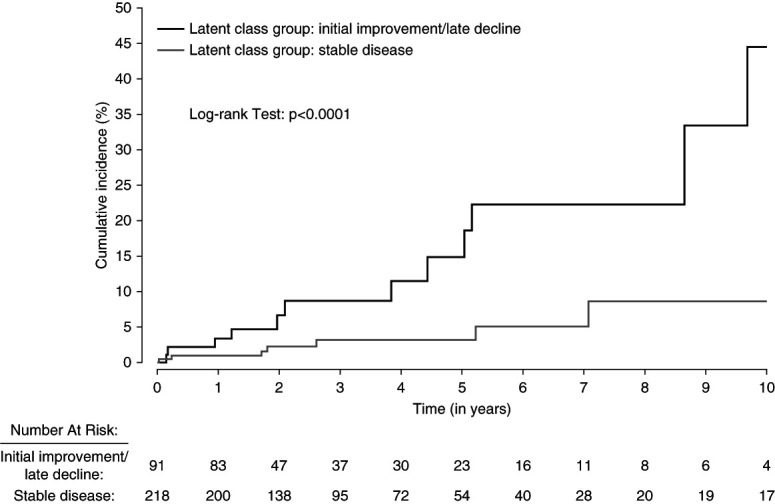
Cumulative incidence of a 30% decrease in eGFR or kidney failure in the initial improvement/late decline versus stable disease subgroups of eGFR trajectory. This was performed in the subgroup of patients treated with immunosuppression after biopsy. Time at risk starts at kidney biopsy. The outcome was the first occurrence of a permanent decline in eGFR by 30% from the value at biopsy or kidney failure (first occurrence of dialysis, transplantation, or a permanent reduction in eGFR <15 ml/min per 1.73 m2). Each patient was assigned to either the initial improvement/late decline or stable disease subgroup of eGFR trajectory on the basis of the highest posterior probability from the LCMM.
The association between clinical and histologic characteristics and eGFR trajectory subgroups is shown in Table 4 for unadjusted and multivariable models. An odds ratio (OR) >1 indicates an association with the initial improvement/late decline group, and an OR <1 indicates an association with the stable disease group. In the multivariable model, age at biopsy 18 years and younger (OR, 2.70), male sex (OR, 1.80), presence of extrarenal noncutaneous disease (OR, 2.53), and E1 score (OR, 2.27) were each associated with the initial improvement/late decline eGFR trajectory. Higher eGFR at biopsy (OR, 0.96) and the presence of fibrous crescents (OR, 0.27) were associated with stable disease. Other variables, including cellular or fibrocellular crescents (C1 and C2 scores), were not associated with either subgroup in the multivariable model.
Table 4.
Association between clinical and histologic characteristics and initial improvement/late decline versus stable disease subgroups of eGFR trajectory over time
| Variables | Initial Improvement/Late Decline Group, N (%)a | Stable Disease Group, N (%)a | Unadjusted Models | Multivariable Model | ||
|---|---|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | |||
| Age, yr | ||||||
| 18 and younger | 75 (33) | 154 (67) | 1.95 (1.06 to 3.60) | 0.03 | 2.70 (1.27 to 5.73) | 0.01 |
| Older than 18 | 16 (20) | 64 (80) | Ref | Ref | Ref | Ref |
| Sex | ||||||
| Male | 57 (35) | 108 (65) | 1.71 (1.04 to 2.82) | 0.04 | 1.80 (1.01 to 3.21) | 0.04 |
| Female | 34 (24) | 110 (76) | Ref | Ref | Ref | Ref |
| Time from clinical onset to biopsy, per month | — | 0.71 (0.58 to 0.86) | <0.001 | — | — | |
| Ethnicity | ||||||
| White | 62 (33) | 125 (67) | 1.59 (0.95 to 2.67) | 0.08 | — | — |
| Non-White | 29 (24) | 93 (76) | Ref | Ref | — | — |
| eGFR at biopsy, per 10 ml/min per 1.73 m2 | — | 0.76 (0.69 to 0.84) | <0.001 | 0.68 (0.60 to 0.77) | <0.001 | |
| Standardized MAP at biopsy, per 10 mm Hg | — | 1.25 (1.01 to 1.54) | 0.04 | — | — | |
| Proteinuria at biopsy, per g/d | — | 1.02 (1.00 to 1.05) | 0.04 | — | — | |
| Extrarenal noncutaneous disease | ||||||
| Present | 75 (33) | 152 (67) | 2.04 (1.10 to 3.75) | 0.02 | 2.53 (1.22 to 5.24) | 0.01 |
| Absent | 16 (20) | 66 (80) | Ref | Ref | Ref | Ref |
| Hematuria | ||||||
| Present | 88 (29) | 211 (71) | 0.97 (0.25 to 3.85) | 0.97 | — | — |
| Absent | 3 (30) | 7 (70) | Ref | Ref | — | — |
| Renin–angiotensin system blockade use at biopsy | ||||||
| Yes | 30 (33) | 60 (67) | 1.29 (0.76 to 2.19) | 0.34 | — | — |
| No | 60 (28) | 155 (72) | Ref | Ref | — | — |
| Immunosuppression use before biopsy | ||||||
| Yes | 68 (31) | 149 (69) | 1.37 (0.79 to 2.38) | 0.26 | — | — |
| No | 23 (25) | 69 (75) | Ref | Ref | — | — |
| Glomerular fibrinoid necrosis | ||||||
| Present | 4 (25) | 12 (75) | 0.79 (0.25 to 2.52) | 0.69 | — | — |
| Absent | 87 (30) | 206 (70) | Ref | Ref | — | — |
| Glomerular TMA | ||||||
| Present | 2 (40) | 3 (60) | 1.61 (0.27 to 9.80) | 0.61 | — | — |
| Absent | 89 (29) | 215 (71) | Ref | Ref | — | — |
| Fibrous crescents | ||||||
| Present | 11 (16) | 57 (84) | 0.39 (0.19 to 0.78) | 0.008 | 0.27 (0.12 to 0.61) | 0.002 |
| Absent | 80 (33) | 161 (67) | Ref | Ref | Ref | Ref |
| M-score | ||||||
| M1 | 42 (35) | 79 (65) | 1.51 (0.92 to 2.48) | 0.10 | — | — |
| M0 | 49 (26) | 139 (74) | Ref | Ref | — | — |
| E-score | ||||||
| E1 | 75 (34) | 148 (66) | 2.22 (1.21 to 4.08) | 0.01 | 2.27 (1.13 to 4.53) | 0.02 |
| E0 | 16 (19) | 70 (81) | Ref | Ref | Ref | Ref |
| S-score | ||||||
| S1 | 37 (24) | 117 (76) | 0.59 (0.36 to 0.97) | 0.04 | — | — |
| S0 | 54 (35) | 101 (65) | Ref | Ref | — | — |
| T-score | ||||||
| T1 or T2 | 4 (29) | 10 (71%) | 0.96 (0.29 to 3.13) | 0.94 | — | — |
| T0 | 87 (29) | 208 (71) | Ref | Ref | — | — |
| C-score | ||||||
| C2 | 17 (39) | 27 (61) | 1.89 (0.91 to 3.94) | 0.23 | — | — |
| C1 | 44 (30) | 101 (70) | 1.31 (0.76 to 2.25) | — | — | |
| C0 | 30 (25) | 90 (75) | Ref | Ref | — | — |
This analysis was performed in those patients treated with immunosuppression after biopsy. Each patient was assigned to either the initial improvement/late decline or stable disease subgroup of eGFR trajectory on the basis of the highest posterior probability from the latent class mixed model. The outcome of the logistic regression models is assignment to the initial improvement/late decline subgroup. As such, an odds ratio >1 indicates an association with the initial improvement/late decline group and an odds ratio <1 indicates an association with the stable disease group. The multivariable model was based on backwards variable selection with a P value threshold <0.05. CI, confidence interval; MAP, mean arterial pressure; OR, odds ratio; Ref, reference group; TMA, thrombotic microangiopathy.
Number (%) of patients in each latent class subgroup within each category of the variable (not provided for continuous variables).
Sensitivity Analyses
The multivariable logistic regression model for the association between histologic and clinical variables and subgroups of eGFR trajectory was repeated using forward variable selection, which produced the same results as in Table 4. The model was repeated using least absolute shrinkage and selection operator (LASSO) regression (which shrinks beta-coefficients to protect against overfitting, Supplemental Table 4), with similar results except proteinuria at biopsy and T1 or T2 scores were retained in the model but with very small effect sizes (OR, 1.00 and 0.98, respectively). Interaction terms were added between each of age and ethnicity and the other variables in the multivariable model, none of which were significant (Supplemental Figure 5). This suggests the association between each risk factor and the eGFR trajectory subgroups was not different in adults versus children or on the basis of ethnicity. Proteinuria over time in the eGFR trajectory subgroups is shown in Supplemental Figure 6. Proteinuria in both groups decreased in the first year after biopsy, but there was a larger increase starting at 3 years in the initial improvement/late decline group.
Discussion
Using a large international cohort of adults and children with biopsy-proven IgA vasculitis nephritis, we found that MEST-C scores correlate with eGFR and proteinuria at the time of biopsy. Because most patients (86%) were treated with immunosuppression after biopsy, as expected in this type of vasculitis, we focused on identifying factors associated with kidney outcomes despite treatment. We used a data-driven approach to identify two subgroups with different eGFR trajectories over time. One was characterized by stable kidney function, suggesting that immunosuppression was sufficient to prevent disease progression. The second was characterized by an initial improvement followed by a later decline in eGFR, which was associated with a nearly six-fold higher risk of a 30% decrease in eGFR or kidney failure and suggests that immunosuppression may have initially improved disease activity but was insufficient to prevent long-term decline in kidney function. Endocapillary hypercellularity (E1 score) was associated with the initial improvement/late decline eGFR trajectory independent of clinical risk factors. The other MEST-C scores, most notable cellular or fibrocellular crescents (C1/C2) which feature prominently in the ISKDC classification, were not associated with either eGFR trajectory in treated patients.
Our results have implications on the histologic classification of IgA vasculitis nephritis. The ISKDC is the most common scoring system for kidney biopsies with IgA vasculitis nephritis. While ISKDC grading correlates with kidney outcomes in children with IgA vasculitis nephritis by unadjusted analysis, the classification discriminates children with good versus poor outcomes less well than a sum score of glomerular, tubulointerstitial, and vascular parameters.8–10,37 Similarly, in a study of 250 adults with IgA vasculitis nephritis, 79% of whom had ISKDC grades II or III, increasing ISKDC grade was associated with the risk of kidney failure or eGFR <30 ml/min per 1.73 m2 by unadjusted analysis, but not in a multivariable analysis including clinical and additional histologic parameters.11 ISKDC grading is based primarily on two of the MEST-C parameters: mesangial hypercellularity and crescents, with the proportion of glomeruli with crescents differentiating grades III, IV, and V. By contrast, interstitial fibrosis/tubular atrophy and endocapillary hypercellularity are barely considered, except for grade VI (membranoproliferative) which is extremely rare. One study of 61 Korean adults with IgA vasculitis nephritis showed that E1, T1/2, and crescents in ≥50% of glomeruli were associated with a higher risk of a ≥30% decline in eGFR or kidney failure.20 Conversely, pediatric studies from China, Turkey, and the United States showed that only chronic lesions, including S1 and in some cases T1/T2, were associated with disease progression or failure to achieve proteinuria remission.21–24 Our findings build on this literature demonstrating the value of MEST-C scoring in IgA vasculitis nephritis. We showed that among patients treated with immunosuppression, E1 lesions had a strong association with an initial improvement followed by progressive decline in kidney function independent of clinical risk factors, and the LASSO model raised the possibility the T-score may also be associated with outcome, although only 4% of patients had T>0, possibly reflecting the short interval between clinical symptoms and biopsy. Cellular or fibrocellular crescents, which dominate the ISKDC system, were not associated with kidney outcome, although these results may have been affected by restricting the analysis to treated patients because the C1 lesion may be responsive to immunosuppression in IgA nephropathy.26,38,39 A somewhat surprising result was the association of fibrous crescents with the stable disease group. Fibrous crescents in our cohort were not correlated with active crescents (C-score) and possibly reflect previous damage with more indolent disease at the time of biopsy. Taken together, our findings, particularly for E1, provide the strongest evidence to date supporting inclusion of MEST-C scores in reports of kidney biopsies with IgA vasculitis nephritis.
IgA vasculitis nephritis may be mild and self-limiting, particularly in children who often enter remission spontaneously; however, when the kidney disease is sufficiently severe to warrant a kidney biopsy, the histologic features are similar in adults and children, and progression may occur at any age.11,40–42 Our report is the first focusing on factors associated with disease progression in patients receiving immunosuppression. To increase cohort size and address the analytic limitations of previous studies in IgA vasculitis nephritis, we included both adults and children.20–24 However, our interaction analysis suggested the effects of clinical and histologic factors associated with eGFR trajectories were not different between adults and children (Supplemental Figure 5). Adults were more likely to be treated after biopsy with corticosteroids alone compared with combination immunosuppression therapy in children (Table 1). However, types of immunosuppression use before or after biopsy were not different on the basis of eGFR trajectories (Tables 1 and 2), and immunosuppression use before biopsy was not associated with trajectory groups using logistic regression (Table 4). Therefore, differences in treatment between adults and children did not seem to confound our results. In our cohort, children were more likely than adults to have an initial improvement in kidney function on immunosuppression followed by a decline several years later. In Supplemental Figure 6, proteinuria decreased with treatment in the first year after biopsy, but then increased to a larger extent in the initial improvement/late decline eGFR trajectory group starting 3 years after biopsy, which corresponds to the approximate time point at which kidney function started to decline (Figure 2). This pattern has been similarly observed in patients with IgA nephropathy treated with glucocorticoids in the TESTING and NefIgARD trials43,44 and suggests that in patients with IgA vasculitis nephritis, immunosuppression treatment may produce a short-term benefit; there remains a risk of recurrent or residual disease resulting in increasing proteinuria and long-term kidney function decline.
There are important limitations to consider. As with many previous studies of IgA vasculitis nephritis, there were too few kidney outcome events on the basis of threshold reductions in eGFR to support robust multivariable model estimation evaluating histologic and clinical variables. This is likely due to a nonlinear trajectory of kidney function over time, as observed in our data. We addressed this challenge by using LCMM to identify trajectories of eGFR over time which were used as the outcome variable. Alternative analysis strategies were considered but deemed inappropriate as described in the Supplemental Methods. We confirmed the eGFR trajectories were associated with an established surrogate outcome in kidney disease (≥30% decline in eGFR or kidney failure), and our primary results were unchanged after accounting for overfitting using LASSO regression. The most important limitation is the median duration of follow-up of 2.7 years, highlighting the need to validate our results in cohorts with longer follow-up to characterize the implications of a delayed decline in eGFR. This relatively short follow-up likely reflects in part a common misconception of IgA vasculitis as an acute and often self-limited vasculitis rather than a potentially progressive disease, despite findings from two smaller, single-center studies of children with IgA vasculitis and over 20 years of follow-up that show similar outcomes as seen in our analysis in children presenting with nephritic or nephrotic syndromes, which were common in our cohort.45,46
In conclusion, our findings indicate the clinical course of biopsied patients with IgA vasculitis nephritis treated with immunosuppression is determined primarily by active histologic lesions, most notably endocapillary hypercellularity (E1) which is not part of the ISKDC classification. These results support including the MEST-C scores in kidney biopsy reports of IgA vasculitis nephritis. Patients with IgA vasculitis nephritis who have a good initial response to immunosuppression remain at risk for developing late disease progression and therefore require long-term follow-up and possibly a different therapeutic approach.
Supplementary Material
Acknowledgments
We would like to acknowledge the Steering Committee and Scientific Committee of the International IgA Nephropathy Research Group as follows: Steering Committee: Sean Barbour, Jonathan Barratt, Daniel Cattran, Rosanna Coppo, Mark Haas, Vivek Jha, Renato Monteiro, Yusuke Suzuki, Heather Reich, Vladimir Tesar, and Hong Zhang. Scientific Committee: Laureline Berthelot, Hitoshi Suzuki, Jürgen Flöge, Jan Novak, Ian Roberts, Krzysztof Kiryluk, Jicheng Lv, and Julio Saez Rodriguez. We would also like to acknowledge the following collaborators who contributed to this work: Giovanni Montini, Pediatric Nephrology, Dialysis and Transplant Unit, Fondazione IRCCS Ca’ Granda-Ospedale Maggiore Policlinico, Milano, Italy; M. Colleen Hastings, Department of Pediatrics, University of Tennessee Health Sciences Center, Memphis, Tennessee; Francesco Emma, Division of Nephrology, Bambino Gesù Children's Hospital–IRCCS, Rome, Italy; Enrico Vidal, Pediatric Nephrology Unit, Department of Women's and Child's Health, University-Hospital of Padova, Italy; Georges Deschenes, Department of Pediatric Nephrology, Assistance Publique-Hôpitaux de Paris Robert-Debré, University of Paris, Paris, France.
Footnotes
See related editorial, “Prognostic Scoring in IgA Vasculitis,” on pages 409–411.
Disclosures
C.E. Alpers reports Consultancy: AstraZeneca, Mantra Bio, Novartis, Travere, and Variant Bio; and Research Funding: Sana. I. Bajema reports Employer: Pathan Laboratories Rotterdam and University Medical Center Groningen; Consultancy: Aurinia, Boehringer Ingelheim, CatBio, GSK, Hansa, Novartis, Otsuka, Toleranzia, Vera, and Vifor; Advisory or Leadership Role: C3 Glomerulopathy review board (Novartis, The Netherlands) and Glomerular Disease Council (Vifor Pharma); and Other Interests or Relationships: Director of Bajema Institute of Pathology, Past President of Renal Pathology Society, and Vice President of European Vasculitis Society (EUVAS). S.J. Barbour reports Consultancy: Achillion, Alexion, BeiGene, BioCryst, Eledon, HIBio, Inception Sciences, Novartis, Pfizer, Roche, Vera, and Visterra; Research Funding: Alexion, Novartis, and Roche; and Honoraria: Kirin. J.U. Becker reports Consultancy: Sanofi. H.T. Cook reports Consultancy: Alexion Pharmaceuticals, Apellis Pharmaceuticals, and Novartis; and Research Funding: Alexion Pharmaceuticals. R. Coppo reports Consultancy: Amgen, Anylam, Argenx, Bayer, Calliditas, Chinook, Menarini, Novartis, Ostuka-Visterra, Purespring, Reata, Stadapharm; Honoraria: Amgen, Bayer, Chinook, Menarini, Novartis, Purespring, Stadapharm, and Travere; Patents or Royalties: UpToDate; Advisory or Leadership Role: Nephrology Dialysis Transplantation Editorial Board and Pediatric Nephrology Associate Editor; and Speakers Bureau: Stadpharm and Travere. F.C. Fervenza reports Consultancy: Alexion Pharmaceuticals, Amgen, ByoCryst Pharmaceuticals, Galapagos, GSK, Morphosys AG, Novartis, Otsuka, Takeda, Travere, and Zyversa Therapeutics; Research Funding: Chemocentryx, Genentech, Hoffman La Roche, Janssen Pharmaceutical, Morphosys, Retrophin, and Travere; Honoraria: UpToDate; and Advisory or Leadership Role: JASN, Kidney International, Nephrology; Nephrology Dialysis Transplantation, and UpToDate. A.B. Fogo reports Consultancy: Novartis; Research Funding: Bayer, Boehringer Ingelheim, and Palatin; Honoraria: GSK and Novartis; Advisory or Leadership Role: Noncompany: Advisory GSK; Associate Editor Kidney International, Atlas of Renal Pathology editor for American Journal of Kidney Diseases, Current Opinion Nephrology and Hypertension guest editor for yearly pathology focus; Editorial Board for American Journal of Physiology-Renal Physiology, JASN, The American Journal of Pathology; Subject Editor Nephrology Dialysis Transplantation; and Other Interests or Relationships: Noncompany: Associate Editor Kidney International, Atlas Renal Pathology editor American Journal of Kidney Diseases, Editorial Board for American Journal of Physiology-Renal Physiology, JASN, and The American Journal of Pathology, Immediate Past-President ISN, speaker at various national nephrology meetings, and Subject Editor Nephrology Dialysis Transplantation. S. Fujimoto reports Research Funding: Asahi Kasei Medical Co., Ltd., Kissei-Pharm. Co., Ltd., Kyowa-Kirin. Co., Ltd., Otsuka Pharmaceutical Co., Ltd., and Torii Pharmaceutical Co., Ltd; Advisory or Leadership Role: Kyowa-Kirin. Co., Ltd.; and Other Interests or Relationships: Nikkiso Co., Ltd. D. Geetha report Consultancy: Aurinia, Calliditas, ChemoCentryx, Consultant Otsuka, Consultant to Amgen, and GSK. M. Haas reports Consultancy: Argenx, AstraZeneca, CareDx, Novartis, Travere, and Vera Therapeutics; and Honoraria: Argenx, CareDx, Novartis, Travere, Vera Therapeutics. J.C. Jennette reports Employer: Sangamo Therapeutics, Inc. K. Joh reports Research Funding: Grant-in-Aid for Progressive Renal Diseases Research, Research on Rare and Intractable Disease, from the Ministry of Health, Labor and Welfare of Japan. N. Messias reports Employer: Arkana Laboratories and Washington University in Saint Louis/BJC Healthcare; Consultancy: Guidepoint Consulting and Novartis; Ownership Interest: Amazon, Apple, Meta, Microsoft, NextEra Energy, Rio Tinto, and Roblox Corporation; and Advisory or Leadership Role: Spouse-Provident Mental Health—not paid. R.C. Monteiro reports Ownership Interest: Inatherys SAS; Research Funding: Moderna; Honoraria: Novartis; Patents or Royalties: Inatherys and Medarex; Advisory or Leadership Role: Inatherys; and Speakers Bureau: Novartis. S. Nakatani reports Honoraria: Astellas Pharma Inc., Bayer Yakuhin, Chugai Pharmaceutical, Kyowa Kirin, MSD, Ono Pharmaceutical, Otsuka Pharmaceutical, Sanwa Kagaku Kenkyusho, and Torii Pharmaceutical. R.D. Nelson reports Research Funding: Abbvie, Akebia, Amgen, Otsuka, and Roche; and Advisory or Leadership Role: Dent Disease Foundation (nonprofit). F. Pagni reports Speakers Bureau: Amgen, MSD, Novartis, and Roche. L. Peruzzi reports Honoraria: Alexion and Alnylam. E. Pillebout reports Consultancy: AstraZeneca, Bayer, Boehringer, and Chinook. I.S.D. Roberts reports Consultancy: Novartis, Q32Bio, and Travere Therapeutics; Advisory or Leadership Role: President BDIAP; and Other Interests or Relationships: Director of UK Renal Pathology (unpaid). D. Santoro reports Consultancy: Alexion, Astellas, Fresenius, GSK, Otsuka, Vifor CSL, and Vifor Pharma; and Advisory or Leadership Role: George Clinical. M. Seidl reports Consultancy: Recordati (formerly EUSAPharm); and Ownership Interest: Amtech, Biontech, and Curevac. V. Tesar reports Consultancy: AstraZeneca, Bayer, Boehringer-Ingelheim, Calliditas, Eli Lilly, Fresenius Medical Care, GSK, Novartis, Omeros, Otsuka, Swixx BioPharma, and Travere; Honoraria: For consultancy as follows: AstraZeneca, Bayer, Boehringer-Ingelheim, Calliditas, Eli Lilly, Fresenius Medical Care, Novartis, Omeros, Swixx Biopharma, and Travere; and Advisory or Leadership Role: member of the scientific advisory board of B. Braun, Fresenius Medical Care and member of the steering committee of clinical trials sponsored by Calliditas, Novartis, Omeros, Otsuka, and Travere. L.T. Weber reports Consultancy: Alexion Pharmaceuticals, Alnylam Pharmaceuticals, Chiesi GmbH, and Novartis Germany; Research Funding: Chiesi GmbH; Honoraria: Alexion Pharmaceuticals, Alnylam Pharmaceuticals, Chiesi GmbH, Novartis Germany, Orphan Europe, and Pfizer Pharma GmbH; Advisory or Leadership Role: Chairman of the German Society for Pediatric Nephrology; Editorial Board: Clinical Nephrology, Der Nephrologe, Monatsschrift Kinderheilkunde, and Pediatric Nephrology; Member of Alexion advisory board “aHUS”; Member of Alnylam advisory board “Primary Hyperoxaluria”; and Member of Chiesi advisory board “Cystinosis”; Speakers Bureau: Chiesi GmbH; and Other Interests or Relationships: Chrokokids, DGfN, DTG, ESPN/IPNA, GPN, IPTA, and Nephrokids. S. Wenderfer reports Consultancy: Alnylam, AstraZeneca, and Novartis; Advisory or Leadership Role: Editorial Board, Pediatric Nephrology (unpaid); and Other Interests or Relationships: Co-chair, Glomerular working group, Pediatric Nephrology Research Consortium and Co-chair of Lupus Nephritis working group, Childhood Arthritis and Rheumatology Research Alliance (CARRA). R.J. Wyatt reports Ownership Interest: Associated Banc Corp, Ericsson, Exxon Mobil, and Walgreen Boot AllianceCirrus Logic. T. Yokoo reports Advisory or Leadership Role: Board of Directors of Japanese Society for Nephrology and Editorial Board Member of “Human Cell”. H. Zhang reports Consultancy: Calliditas, Chinook, Novartis, Omeros, and Ostuka; and Advisory or Leadership Role: Calliditas, Chinook, Novartis, Omeros, and Ostuka. L. Zand reports Research Funding: Genentech and Janssen pharmaceuticals; and Advisory or Leadership Role: Calliditas Therapeutics and Travere Pharmaceuticals. All remaining authors have nothing to disclose.
Funding
This work was supported by the International IgA Nephropathy Network Research Group (www.iigann.org/our-research), the Immunonephrology Working Group of the European Renal Association, and a mini grant from the Department of Pathology and Laboratory Medicine, Cedars-Sinai Medical Center (M. Haas).
Author Contributions
Conceptualization: Sean J. Barbour, Rosanna Coppo, Mark Haas, Evangeline Pillebout.
Data curation: Charles E. Alpers, Carmen Avila-Casado, Ingeborg Bajema, Antonella Barreca, Jan U. Becker, Jessica M. Comstock, Giovanni Conti, H. Terence Cook, Rosanna Coppo, Virgilius Cornea, Maria D'Armiento, Eric Daugas, Jie Ding, Francesca Diomedi-Camassei, Karen Eldin, Franco Ferrario, Fernando C. Fervenza, Agnes B. Fogo, Shouichi Fujimoto, Duvuru Geetha, Mark Haas, Agnes Hackl, Loren Herrera Hernandez, Jean Hou, Daisuke Ichikawa, J. Charles Jennette, Kensuke Joh, Ritsuko Katafuchi, Mikael Koskela, Mercury Lin, Zhi-Hong Liu, Laura Lucchetti, Dita Maixnerova, Antonio Mastrangelo, Marco Materassi, Nidia Messias, Renato C. Monteiro, Luisa Murer, Shinya Nakatani, JoAnn H. Narus, Raoul D. Nelson, Matti Nuutinen, Andrea Onetti Muda, Fabio Pagni, Catherine Park, Carmine Pecoraro, Licia Peruzzi, Evangeline Pillebout, Martin Pohl, Ian S.D. Roberts, Avi Rosenberg, Maria Luisa Russo, Aurelie Sannier, Domenico Santoro, Maximilian Seidl, Sufang Shi, Yuko Shima, Maria Fernanda Soares, Baige Su, Yusuke Suzuki, Ito Takafumi, Vladimir Tesar, Heikki Tokola, Nobuo Tsuboi, Suxia Wang, Lutz T. Weber, Scott Wenderfer, Robert J. Wyatt, Takashi Yokoo, Norishige Yoshikawa, Ladan Zand, Caihong Zeng, Hong Zhang, Xuhui Zhong.
Formal analysis: Sean J. Barbour, Lee Er.
Investigation: Sean J. Barbour, Rosanna Coppo, Mark Haas.
Methodology: Sean J. Barbour, Rosanna Coppo, Mark Haas.
Resources: Sean J. Barbour.
Supervision: Sean J. Barbour, Rosanna Coppo, Mark Haas.
Writing – original draft: Sean J. Barbour, Rosanna Coppo, Mark Haas, Evangeline Pillebout.
Writing – review & editing: Charles E. Alpers, Carmen Avila-Casado, Ingeborg Bajema, Sean J. Barbour, Antonella Barreca, Jan U. Becker, Jessica M. Comstock, Giovanni Conti, H. Terence Cook, Rosanna Coppo, Virgilius Cornea, Maria D'Armiento, Eric Daugas, Jie Ding, Francesca Diomedi-Camassei, Karen Eldin, Lee Er, Franco Ferrario, Fernando C. Fervenza, Agnes B. Fogo, Shouichi Fujimoto, Duvuru Geetha, Mark Haas, Agnes Hackl, Loren Herrera Hernandez, Jean Hou, Daisuke Ichikawa, J. Charles Jennette, Kensuke Joh, Ritsuko Katafuchi, Mikael Koskela, Mercury Lin, Zhi-Hong Liu, Laura Lucchetti, Dita Maixnerova, Antonio Mastrangelo, Marco Materassi, Nidia Messias, Renato C. Monteiro, Luisa Murer, Shinya Nakatani, JoAnn H. Narus, Raoul D. Nelson, Matti Nuutinen, Andrea Onetti Muda, Fabio Pagni, Catherine Park, Carmine Pecoraro, Licia Peruzzi, Evangeline Pillebout, Martin Pohl, Ian S.D. Roberts, Avi Rosenberg, Maria Luisa Russo, Aurelie Sannier, Domenico Santoro, Maximilian Seidl, Sufang Shi, Yuko Shima, Maria Fernanda Soares, Baige Su, Yusuke Suzuki, Ito Takafumi, Vladimir Tesar, Heikki Tokola, Nobuo Tsuboi, Suxia Wang, Lutz T. Weber, Scott Wenderfer, Robert J. Wyatt, Takashi Yokoo, Norishige Yoshikawa, Ladan Zand, Caihong Zeng, Hong Zhang, Xuhui Zhong.
Supplemental Material
This article contains the following supplemental material online at http://links.lww.com/CJN/B854.
Supplemental Table 1. Histologic lesions that were evaluated on kidney biopsy.
Supplemental Table 2. Correlation between histologic lesions and eGFR and proteinuria at biopsy.
Supplemental Table 3. Description of the analytic cohort on the basis of immunosuppression exposure postbiopsy.
Supplemental Table 4. Multivariable model results for the association between clinical and histologic characteristics and initial improvement/late decline versus stable disease subgroups of eGFR trajectory over time using LASSO regression.
Supplemental Figure 1. Scoring sheet used for histologic evaluation of kidney biopsies.
Supplemental Figure 2. Derivation of the analytic cohort.
Supplemental Figure 3. Proteinuria and eGFR at biopsy on the basis of histologic lesions separately in adults and children.
Supplemental Figure 4. Trajectories of eGFR over time on the basis of immunosuppression exposure.
Supplemental Figure 5. Interaction results for potential effect modification between adult versus children and ethnicity with other clinical and histologic risk factors for an initial improvement/late decline versus stable disease subgroups of eGFR trajectory over time.
Supplemental Figure 6. Proteinuria after kidney biopsy in the initial improvement/late decline versus stable disease subgroups of eGFR trajectory.
References
- 1.Davin JC, Coppo R. Henoch-Schonlein purpura nephritis in children. Nat Rev Nephrol. 2014;10(10):563–573. doi: 10.1038/nrneph.2014.126 [DOI] [PubMed] [Google Scholar]
- 2.Hastings MC Rizk DV Kiryluk K, et al. IgA vasculitis with nephritis: update of pathogenesis with clinical implications. Pediatr Nephrol. 2022;37(4):719–733. doi: 10.1007/s00467-021-04950-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Allen AC, Willis FR, Beattie TJ, Feehally J. Abnormal IgA glycosylation in Henoch-Schonlein purpura restricted to patients with clinical nephritis. Nephrol Dial Transplant. 1998;13(4):930–934. doi: 10.1093/ndt/13.4.930 [DOI] [PubMed] [Google Scholar]
- 4.Saulsbury FT. Henoch-Schonlein purpura in children. Report of 100 patients and review of the literature. Medicine (Baltimore). 1999;78(6):395–409. doi: 10.1097/00005792-199911000-00005 [DOI] [PubMed] [Google Scholar]
- 5.Tancrede-Bohin E, Ochonisky S, Vignon-Pennamen MD, Flageul B, Morel P, Rybojad M. Schonlein-Henoch purpura in adult patients. Predictive factors for IgA glomerulonephritis in a retrospective study of 57 cases. Arch Dermatol. 1997;133(4):438–442. doi: 10.1001/archderm.133.4.438 [DOI] [PubMed] [Google Scholar]
- 6.Haas M. IgA nephropathy and IgA vasculitis (Henoch-Schonlein purpura) nephritis. In: Jenette JC, Olsen JL, Silva FG, D’Agati VD, eds. Hepinstall’s Pathology of the Kidney, 7th ed. Wolters-Kluwer; 2015:463–523. [Google Scholar]
- 7.Heineke MH, Ballering AV, Jamin A, Ben Mkaddem S, Monteiro RC, Van Egmond M. New insights in the pathogenesis of immunoglobulin A vasculitis (Henoch-Schonlein purpura). Autoimmun Rev. 2017;16(12):1246–1253. doi: 10.1016/j.autrev.2017.10.009 [DOI] [PubMed] [Google Scholar]
- 8.Koskela M Ylinen E Ukonmaanaho EM, et al. The ISKDC classification and a new semiquantitative classification for predicting outcomes of Henoch-Schonlein purpura nephritis. Pediatr Nephrol. 2017;32(7):1201–1209. doi: 10.1007/s00467-017-3608-5 [DOI] [PubMed] [Google Scholar]
- 9.Scharer K, Krmar R, Querfeld U, Ruder H, Waldherr R, Schaefer F. Clinical outcome of Schonlein-Henoch purpura nephritis in children. Pediatr Nephrol. 1999;13(9):816–823. doi: 10.1007/s004670050707 [DOI] [PubMed] [Google Scholar]
- 10.Edstrom Halling S, Soderberg MP, Berg UB. Predictors of outcome in Henoch-Schonlein nephritis. Pediatr Nephrol. 2010;25(6):1101–1108. doi: 10.1007/s00467-010-1444-y [DOI] [PubMed] [Google Scholar]
- 11.Pillebout E, Thervet E, Hill G, Alberti C, Vanhille P, Nochy D. Henoch-Schonlein Purpura in adults: outcome and prognostic factors. J Am Soc Nephrol. 2002;13(5):1271–1278. doi: 10.1097/01.ASN.0000013883.99976.22 [DOI] [PubMed] [Google Scholar]
- 12.Cattran DC Coppo R Cook HT, et al.; Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int. 2009;76(5):534–545. doi: 10.1038/ki.2009.243 [DOI] [PubMed] [Google Scholar]
- 13.Coppo R Troyanov S Bellur S, et al. Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments. Kidney Int. 2014;86(4):828–836. doi: 10.1038/ki.2014.63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Haas M, Rastaldi MP, Fervenza FC. Histologic classification of glomerular diseases: clinicopathologic correlations, limitations exposed by validation studies, and suggestions for modification. Kidney Int. 2014;85(4):779–793. doi: 10.1038/ki.2013.375 [DOI] [PubMed] [Google Scholar]
- 15.Roberts ISD Cook HT Troyanov S, et al.; Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76(5):546–556. doi: 10.1038/ki.2009.168 [DOI] [PubMed] [Google Scholar]
- 16.Barbour SJ Espino-Hernandez G Reich HN, et al. The MEST score provides earlier risk prediction in lgA nephropathy. Kidney Int. 2016;89(1):167–175. doi: 10.1038/ki.2015.322 [DOI] [PubMed] [Google Scholar]
- 17.Barbour SJ Coppo R Zhang H, et al. Evaluating a new international risk-prediction Tool in IgA nephropathy. JAMA Intern Med. 2019;179(7):942–952. doi: 10.1001/jamainternmed.2019.0600 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang Y Guo L Wang Z, et al. External validation of international risk-prediction models of IgA nephropathy in an asian-Caucasian cohort. Kidney Int Rep. 2020;5(10):1753–1763. doi: 10.1016/j.ekir.2020.07.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kidney Disease Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 clinical Practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4S):S1–S276. doi: 10.1016/j.kint.2021.05.021 [DOI] [PubMed] [Google Scholar]
- 20.Kim CH Lim BJ Bae YS, et al. Using the Oxford classification of IgA nephropathy to predict long-term outcomes of Henoch-Schonlein purpura nephritis in adults. Mod Pathol. 2014;27(7):972–982. doi: 10.1038/modpathol.2013.222 [DOI] [PubMed] [Google Scholar]
- 21.Huang X Ma L Ren P, et al. Updated Oxford classification and the international study of kidney disease in children classification: application in predicting outcome of Henoch-Schonlein purpura nephritis. Diagn Pathol. 2019;14(1):40. doi: 10.1186/s13000-019-0818-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cakici EK Gur G Yazilitas F, et al. A retrospective analysis of children with Henoch-Schonlein purpura and re-evaluation of renal pathologies using Oxford classification. Clin Exp Nephrol. 2019;23(7):939–947. doi: 10.1007/s10157-019-01726-5 [DOI] [PubMed] [Google Scholar]
- 23.Jimenez A, Chen A, Lin JJ, South AM. Does MEST-C score predict outcomes in pediatric Henoch-Schonlein purpura nephritis?. Pediatr Nephrol. 2019;34(12):2583–2589. doi: 10.1007/s00467-019-04327-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Xu K Zhang L Ding J, et al. Value of the Oxford classification of IgA nephropathy in children with Henoch-Schonlein purpura nephritis. J Nephrol. 2018;31(2):279–286. doi: 10.1007/s40620-017-0457-z [DOI] [PubMed] [Google Scholar]
- 25.Barbour SJ Coppo R Er L, et al. Updating the international IgA nephropathy prediction Tool for use in children. Kidney Int. 2021;99(6):1439–1450. doi: 10.1016/j.kint.2020.10.033 [DOI] [PubMed] [Google Scholar]
- 26.Trimarchi H Barratt J Cattran DC, et al. Oxford classification of IgA nephropathy 2016: an update from the IgA nephropathy classification working group. Kidney Int. 2017;91(5):1014–1021. doi: 10.1016/j.kint.2017.02.003 [DOI] [PubMed] [Google Scholar]
- 27.Wuhl E, Witte K, Soergel M, Mehls O, Schaefer F.; German Working Group on Pediatric Hypertension. Distribution of 24-h ambulatory blood pressure in children: normalized reference values and role of body dimensions. J Hypertens. 2002;20(10):1995–2007. doi: 10.1097/00004872-200210000-00019 [DOI] [PubMed] [Google Scholar]
- 28.Hogan MC Reich HN Nelson PJ, et al. The relatively poor correlation between random and 24-hour urine protein excretion in patients with biopsy-proven glomerular diseases. Kidney Int. 2016;90(5):1080–1089. doi: 10.1016/j.kint.2016.06.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pottel H Hoste L Dubourg L, et al. An estimated glomerular filtration rate equation for the full age spectrum. Nephrol Dial Transplant. 2016;31(5):798–806. doi: 10.1093/ndt/gfv454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gwet KL. Handbook of Inter-rater Reliability: The Definitive Guide to Measuring the Extent of Agreement Among Raters, 4 ed. Advanced Analytics LLC; 2014. [Google Scholar]
- 31.Hallgren KA. Computing inter-rater reliability for observational data: an overview and tutorial. Tutor Quant Methods Psychol. 2012;8(1):23–34. doi: 10.20982/tqmp.08.1.p023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dancey CP, Reidy J. Statistics without Maths for Psychology: Using SPSS for Windows, 4 ed. Prentice Hall; 2007. [Google Scholar]
- 33.Herle M Micali N Abdulkadir M, et al. Identifying typical trajectories in longitudinal data: modelling strategies and interpretations. Eur J Epidemiol. 2020;35(3):205–222. doi: 10.1007/s10654-020-00615-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nguena Nguefack HL Page MG Katz J, et al. Trajectory modelling techniques useful to epidemiological Research: a comparative narrative review of approaches. Clin Epidemiol. 2020;12:1205–1222. doi: 10.2147/CLEP.S265287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Boucquemont J Loubere L Metzger M, et al. Identifying subgroups of renal function trajectories. Nephrol Dial Transplant. 2017;32(suppl 2):ii185–ii193. doi: 10.1093/ndt/gfw380 [DOI] [PubMed] [Google Scholar]
- 36.Bellur SS Roberts ISD Troyanov S, et al. Reproducibility of the Oxford classification of immunoglobulin A nephropathy, impact of biopsy scoring on treatment allocation and clinical relevance of disagreements: evidence from the VALidation of IGA study cohort. Nephrol Dial Transplant. 2019;34(10):1681–1690. doi: 10.1093/ndt/gfy337 [DOI] [PubMed] [Google Scholar]
- 37.Koskela M Ylinen E Autio-Harmainen H, et al. Prediction of renal outcome in Henoch-Schonlein nephritis based on biopsy findings. Pediatr Nephrol. 2020;35(4):659–668. doi: 10.1007/s00467-019-04415-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Haas M Verhave JC Liu ZH, et al. A multicenter study of the predictive value of crescents in IgA nephropathy. J Am Soc Nephrol. 2017;28(2):691–701. doi: 10.1681/ASN.2016040433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Trimarchi H, Haas M, Coppo R. Crescents and IgA nephropathy: a delicate marriage. J Clin Med. 2022;11(13):3569. doi: 10.3390/jcm11133569 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Peruzzi L, Coppo R. IgA vasculitis nephritis in children and adults: one or different entities? Pediatr Nephrol. 2021;36(9):2615–2625. doi: 10.1007/s00467-020-04818-7 [DOI] [PubMed] [Google Scholar]
- 41.Kusumoto Y, Takebayashi S, Taguchi T, Harada T, Naito S. Long-term prognosis and prognostic indices of IgA nephropathy in juvenile and in adult Japanese. Clin Nephrol. 1987;28(3):118–124. PMID: 3665204 [PubMed] [Google Scholar]
- 42.Coppo R Andrulli S Amore A, et al. Predictors of outcome in Henoch-Schonlein nephritis in children and adults. Am J Kidney Dis. 2006;47(6):993–1003. doi: 10.1053/j.ajkd.2006.02.178 [DOI] [PubMed] [Google Scholar]
- 43.Lv J Wong MG Hladunewich MA, et al. Effect of oral methylprednisolone on decline in kidney function or kidney failure in patients with IgA nephropathy: the TESTING randomized clinical trial. JAMA. 2022;327(19):1888–1898. doi: 10.1001/jama.2022.5368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lafayette R Kristensen J Stone A, et al. Efficacy and safety of a targeted-release formulation of budesonide in patients with primary IgA nephropathy (NefIgArd): 2-year results from a randomised phase 3 trial. Lancet. 2023;402(10405):859–870. doi: 10.1016/S0140-6736(23)01554-4 [DOI] [PubMed] [Google Scholar]
- 45.Goldstein AR, White RH, Akuse R, Chantler C. Long-term follow-up of childhood Henoch-Schonlein nephritis. Lancet. 1992;339(8788):280–282. doi: 10.1016/0140-6736(92)91341-5 [DOI] [PubMed] [Google Scholar]
- 46.Ronkainen J, Nuutinen M, Koskimies O. The adult kidney 24 years after childhood Henoch-Schonlein purpura: a retrospective cohort study. Lancet. 2002;360(9334):666–670. doi: 10.1016/S0140-6736(02)09835-5 [DOI] [PubMed] [Google Scholar]