

Abstract
Background
This study aims to compare the range of motion (ROM) of reverse shoulder arthroplasty lateralised by bony increased offset (BIO-RSA) using a standard 38-mm (mm) component to regular reverse shoulder arthroplasty (RSA) lateralised by using a 42-mm glenoid component. The secondary aims are to compare patient-reported and radiographic outcomes between the two groups.
Materials and Methods
All patients with a BIO-RSA and size 38 glenosphere were retrospectively identified and matched to patients with a regular RSA and size 42 glenosphere. Matched patients were invited for a follow-up visit. ROM was assessed as well as radiographic outcomes (lateralisation, distalisation, inferior overhang, scapular notching, heterotopic bone formation, radiolucency, stress shielding, bone graft healing and viability and complications) and patient-reported outcomes (subjective shoulder value, Constant score, American Shoulder and Elbow Surgeons, activities of daily living which require internal rotation, activities of daily living which require external rotation and a visual analogue scale for pain). Outcomes were compared between the two groups.
Results
In total, 38 BIO-RSAs with a size 38 glenosphere were matched to 38 regular RSAs with a size 42 glenosphere. Of the 76 matched patients, 74 could be contacted and 70 (95%) were included. At the final follow-up, there were no differences between the two groups in ROM, patient-reported outcomes or radiographic outcomes (p > 0.485).
Conclusions
Using a larger glenosphere is a feasible alternative to BIO-RSA for lateralising RSA, providing comparable ROM, patient-reported and radiographic results, while potentially decreasing costs, operative time and complication rates.
Level of evidence III.
Supplementary Information
The online version contains supplementary material available at 10.1186/s10195-024-00764-4.
Keywords: Bony increased offset reverse shoulder arthroplasty, Patient-reported outcomes, Range of motion
Introduction
The introduction of the reverse shoulder arthroplasty (RSA) design by Grammont revolutionised surgical treatment for shoulder pathologies [1]. However, it came with several drawbacks including prosthetic instability, deficient internal and external rotation, aesthetic complaints owing to loss of shoulder contour, scapular impingement and stress fractures [2]. All of these can be attributed completely or partially to the medialisation and distalisation of the humerus and the centre of rotation.
One option to lateralise the glenoid component is bony increased offset reverse shoulder arthroplasty (BIO-RSA) [3]. Some studies report improved rotation with BIO-RSA compared to non-lateralised RSA [4, 5]. However, this procedure is promising but also more technically challenging, prone to specific compilations and costly compared with regular RSA [6].
Increasing the size of the glenoid component has also been proposed to further reduce the rate of scapular notching and improve rotational range of motion (ROM) by lateralising the humerus without changing the centre of rotation, and by increasing the inferior overhang. Previous studies have reported lower rates of scapular notching and greater rotational and elevation ROM in patients with a larger glenoid component [4–6]. However, other studies did not replicate these results [5, 7].
To our knowledge, no prior studies have been published directly comparing these two groups. To address the gaps and contradictions in the literature, this study aims to compare the ROM of BIO-RSA using a 38-mm (mm) component with regular RSA using a 42-mm glenoid component in a matched retrospective series using the Delta Xtend reverse shoulder prosthesis (DePuy Synthes, Warsaw, USA) with a 155 ° neck-shaft angle design. The secondary aims are to compare patient-reported and radiographic outcomes, such as scapular notching.
Methods
Patient selection
After approval from the institutional review board, all consecutive primary RSA procedures performed between January 2015 and December 2021 were identified. Because all consecutive patients were identified, no power calculation was performed. Inclusion and exclusion criteria are reported in Table 1.
Table 1.
Inclusion and exclusion criteria
| Inclusion | Exclusion |
|---|---|
| 1. RSA using Delta Xtend* model | 1. Deceased patients |
| 2A. Regular RSA + size 42 glenosphere or 2B. BIO-RSA + size 38 glenosphere | 2. Language barrier with regards to the researchers (speaking English, French, Italian, German, Dutch and Spanish) |
| 3. No contact information | |
| 4. Bone graft used for glenoid bone loss or glenoid defects (instead of lateralisation) | |
| 5. Augmented or lateralised prosthesis designs | |
| 6. Preoperative nerve palsies or neurological defects |
BIO-RSA bony increased offset reverse shoulder arthroplasty, RSA reverse shoulder arthroplasty
*Depuy Synthes, Warsaw, USA
All patients with a BIO-RSA and a size 38 glenosphere (BIO-RSA 38 group) were matched with patients with a regular RSA and a size 42 glenosphere (RSA 42 group) with a 1:1 ratio. Patients were matched based on sex, age, body mass index (BMI) and the indication for RSA using optimal pair matching. The mean and maximum distances in propensity score between the pairs were reported. The matched patients were contacted for a follow-up visit. In cases where patients were unable to visit the hospital, questionnaires were completed via telephone. The minimum follow-up for inclusion was set at 1 year, on the basis of a previous study that reported no change in ROM and patient reported outcome measures (PROMs) between the 1- and 2-year follow-up periods [8].
Variables
A revision was defined as any unplanned surgical procedure to the ipsilateral glenohumeral joint related to the arthroplasty. A complication was defined as any unforeseen medical problem caused by the RSA procedure which negatively influences the outcome temporarily or permanently [9].
The following questionnaires were completed: subjective shoulder value (SSV) [10], Constant score [11], American Shoulder and Elbow Surgeons (ASES) [12], activities of daily living which require internal rotation (ADLIR) [13, 14], activities of daily living which require external rotation (ADLER) [15] and a visual analogue scale (VAS) for pain.
Radiographic outcomes
On the most recent radiographic imaging lateralisation, distalisation, inferior overhang, scapular notching, heterotopic bone formation, radiolucency, stress shielding, bone graft healing and viability and potential other complications were independently assessed by two authors in a standardised fashion described in Additional file 1: Table S1 [3, 16–24]. All assessments were then discussed with the senior author to reach a consensus between the three assessors. For the angle and distance measurements, three authors including the senior author independently performed the measurements, and the mean result was calculated.
Statistics
The improvement from pre- to postoperative measurements was compared using paired Wilcoxon signed-rank tests. For the comparisons between the two groups (BIO-RSA 38 versus RSA 42), unpaired tests were used. This was chosen over paired tests owing to the potential differences in response rate between the groups leading to unequal group sizes, the overall small cohort and limited population to draw from for patient matching leading to minimal dependence between matched cases [25, 26]. Chi-squared or Fisher exact tests were used for binary categorical variables and T-tests or Mann–Whitney U tests were used for continues variables.
For the radiological assessment, reliability between the first two authors analysing the radiographs was assessed using the interclass correlation (ICC) for the angle measurements and Cohen’s kappa (k) for the grades. An ICC of less than 0.50 was considered poor reliability, between 0.5 and 0.75 moderate reliability, between 0.75 and 0.9 good reliability and greater than 0.9 was considered excellent reliability. A Cohen’s kappa of less than 0.20 was considered a slight agreement, between 0.21 and 0.40 fair, between 0.41 and 0.60 moderate, between 0.61 and 0.80 substantial and between 0.81 and 1.00 was considered almost perfect agreement [27].
To correct for multiple testing, p-values were adjusted using a Benjamini–Hochberg procedure. An adjusted p-value lower than 0.05 was considered statistically significant. A post-hoc power calculation was performed for the primary outcomes (rotational range of motion) using 0.05 as the significance level, a resulting power of > 0.80 was considered sufficient. Statistical analysis was performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Surgical technique
In all cases a Delta Xtend prosthesis was used (DePuy Synthes, Raynham, USA) with a high-mobility polyethylene insert size 3. A deltopectoral approach was used for all BIO-RSA cases and an anterosuperior approach for all RSA cases. For BIO-RSA cases, a bone graft of approximately 1 cm in width was used, harvested from the resected humeral head when possible. In cases of BIO-RSA the glenoid baseplate construct was angled 10 ° inferior, in RSA cases an inclination angle of 0 ° was aimed for. The subscapularis tendon was either absent or detached in all cases without subsequent repair.
Results
After inclusion (Fig. 1) 38 BIO-RSAs with a glenosphere size 38 were matched to 38 regular RSAs with a glenosphere size 42. The median distance in propensity scores between the matched pairs was 0.27 and the maximum distance was 0.58. Of the 76 matched patients, 74 could be contacted and 70 were included (response rate: 95%). In total, five patients had a bilateral prosthesis but both shoulders were not included in any cases. The post-hoc power calculation resulted in a statistical power of > 0.99 for the primary outcomes (rotational range of motion).
Fig. 1.
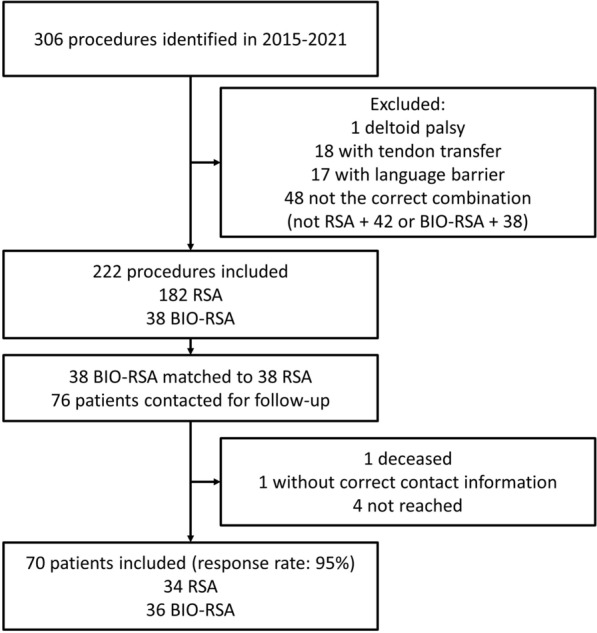
Inclusion flowchart
Study cohort
The mean age at the time of primary surgery in the cohort was 72 (SD 8) years and the majority of patients were female (44/70, 63%). The follow-up was longer in the RSA 42 group [3.7 years; interquartile range (IQR): 2.2–5.4 versus 2.3 years; IQR 2.1–2.5, p = 0.0126). The other patient characteristics did not differ between the groups after correction of the p-values (Table 2).
Table 2.
Patient characteristics
| BIO-RSA 38 (n = 36) | RSA 42 (n = 34) | p-value | Adjusted p-value | |
|---|---|---|---|---|
| Female, n (%) | 22 (61) | 22 (65) | A0.756 | 1.000 |
| Age, mean years (SD) | 70 (8) | 73 (7) | B0.0424 | 0.806 |
| BMI, mean kg/m2 (SD) | 26 (4) | 26 (4) | B0.990 | 1.000 |
| Diagnosis, n (%) | C0.912 | 1.000 | ||
| Osteoarthritis | 13 (36) | 14 (41) | ||
| Cuff tear arthropathy | 12 (33) | 9 (26) | ||
| Irreparable cuff tear | 10 (28) | 10 (29) | ||
| Acute fracture | 1 (3) | 1 (3) | ||
| ASA classification, n (%) | A0.938 | 1.000 | ||
| I | 8 (24) | 15 (42) | ||
| II | 21 (62) | 15 (42) | ||
| III | 5 (15) | 6 (17) | ||
| Comorbidities, n (%) | ||||
| Diabetes | 3 (8) | 2 (6) | C1.000 | 1.000 |
| Cardiological | 20 (56) | 18 (53) | A0.826 | 1.000 |
| Thyroid disease | 5 (14) | 4 (12) | C1.000 | 1.000 |
| Gastroenterological | 4 (11) | 4 (12) | C1.000 | 1.000 |
| Respiratory | 0 (0) | 3 (9) | C0.109 | 1.000 |
| Urological | 4 (11) | 3 (9) | C1.000 | 1.000 |
| Neurological | 1 (3) | 5 (14) | C0.199 | 1.000 |
| Psychological | 2 (6) | 1 (3) | C0.609 | 1.000 |
| Oncological | 0 (0) | 1 (3) | C0.486 | 1.000 |
| Smoking, n (%) | 5 (14) | 3 (9) | C0.711 | 1.000 |
| Dominant side operated, n (%) | 12 (52) | 7 (32) | A0.167 | 1.000 |
| Previous surgery, n (%) | 12 (33) | 6 (18) | A0.133 | 1.000 |
| Rotator cuff | 11 (31) | 3 (9) | A0.0231 | 0.462 |
| Latarjet | 1 (3) | 2 (6) | C0.609 | 1.000 |
| Other | 1 (3) | 1 (3) | C1.000 | 1.000 |
| Follow-up time, median years (IQR) | 2.3 (2.1–2.5) | 3.7 (2.2–5.4) | D0.0006 | 0.0126 |
BMI body mass index, BIO-RSA bony increased offset reverse shoulder arthroplasty, RSA reverse shoulder arthroplasty, SD standard deviation
Achi-square
Bt-test
CFisher exact test
DMann–Whitney U test
Acromioplasty was more commonly performed in the RSA 42 group (32/34, 94% versus 25/36, 69%, p = 0.0399). The other treatment characteristics did not differ between the two groups (Table 3).
Table 3.
Treatment characteristics
| BIO-RSA 38 (n = 36) | RSA 42 (n= 34) | p-value | Adjusted p-value | |
|---|---|---|---|---|
| Acromioplasty, n (%) | 25 (69) | 32 (94) | A0.00798 | 0.0399 |
| Humerus size, median (IQR) | 10 (10–11) | 10 (10–11) | D0.707 | 0.707 |
| Cemented humerus, n (%) | 0 (0) | 3 (9) | C0.109 | 0.327 |
| Retroversion, median ° (IQR) | 30 (30–30) | 30 (30–30) | D0.588 | 0.707 |
| Locking screws, n (%) | A0.069 | 0.276 | ||
| 2/4 | 0 (0) | 17 (50) | ||
| 0/4 | 36 (100) | 17 (50) | ||
| Graft donor, n (%) | ||||
| Humeral head | 34 (94) | |||
| Iliac crest | 1 (3) | |||
| Allograft | 1 (3) |
BIO-RSA bony increased offset reverse shoulder arthroplasty, IQR interquartile range, RSA reverse shoulder arthroplasty
Achi-square
Bt-test
CFisher exact test
DMann–Whitney U test
Information on preoperative assessments was available in 67 patients (96%). There was no difference between the groups in preoperative PROMs and ROM (p > 0.260; Table 4).
Table 4.
Preoperative measurements
| Median (IQR) | BIO-RSA 38 (n = 36) | RSA 42 (n = 34) | p-value | Adjusted p-value |
|---|---|---|---|---|
| Subjective Shoulder Value (0–100) | 30 (30–50) | 40 (30–48) | 0.554 | 0.554 |
| VAS pain (0–10) | 6 (5–7) | 7 (5–7) | 0.348 | 0.554 |
| Anterior elevation, ° | 90 (70–130) | 105 (80–137) | 0.547 | 0.554 |
| External rotation, ° | 10 (−4 to 30) | 20 (10–44) | 0.065 | 0.260 |
| Internal rotation, level reached | buttock (hip-L3) | L3 (buttock-T12) | 0.059 | 0.260 |
BIO-RSA bony increased offset reverse shoulder arthroplasty, IQR interquartile range, RSA reverse shoulder arthroplasty, VAS visual analogue scale
Patient-reported outcomes
PROM results at final follow-up were available in 67 patients (96%). The SSV and pain score at final follow-up improved significantly compared with the preoperative measurements (p < 0.001), the other PROMs were not recorded preoperatively. There were no differences between the two groups in PROMs at the final follow-up or the amount of improvement between preoperative measurements and the final follow-up (p = 0.961, Table 5).
Table 5.
Patient-reported and clinical outcomes
| BIO-RSA 38 (n = 36) | RSA 42 (n = 34) | p-value | Adjusted p-value | |
|---|---|---|---|---|
| At final follow-up | ||||
| Subjective shoulder value (0–100), median (IQR) | 80 (70–91) | 80 (60–90) | D0.488 | 0.961 |
| VAS pain (0–10)), median (IQR) | 1 (0–2) | 1 (0–3) | D0.615 | 0.961 |
| Constant score, mean (SD) | 62 (17) | 65 (23) | B0.699 | 0.961 |
| ASES score, median (IQR) | 82 (75–90) | 82 (67–92) | D0.790 | 0.961 |
| ADLIR score, median (IQR) | 84 (78–88) | 86 (77–95) | D0.370 | 0.961 |
| ADLER score, median (IQR) | 29 (28–30) | 29 (21–30) | D0.290 | 0.961 |
| Anterior elevation, median ° (IQR) | 160 (134–170) | 150 (115–160) | D0.365 | 0.961 |
| Abduction, median ° (IQR) | 150 (115–170) | 140 (88–160) | D0.564 | 0.961 |
| External rotation, median ° (IQR) | 40 (20–49) | 30 (20–45) | D0.676 | 0.961 |
| External rotation in abduction, median ° (IQR) | 75 (60–80) | 70 (45–90) | D0.961 | 0.961 |
| Internal rotation, median level reached (IQR) | L1 (L5-T12) | L4 (buttock-T12) | D0.380 | 0.961 |
| Improvement from preoperative to final follow-up | ||||
| Subjective shoulder value (0–100), mean Δ (SD) | 44.6 (24.8) | 31.0 (29.0) | B0.197 | 0.961 |
| VAS pain (0–10), mean Δ (SD) | − 4.7 (3.2) | − 4.2 (2.2) | B0.607 | 0.961 |
| Anterior elevation, mean Δ ° (SD) | 38.4 (55.9) | 29.0 (52.4) | B0.578 | 0.961 |
| External rotation, mean Δ ° (SD) | 21.1 (32.1) | 2.9 (27.6) | B0.070 | 0.961 |
| Internal rotation, mean Δ* (SD) | 4.7 (5.3) | − 1.4 (5.3) | B0.00220 | 0.0352 |
BIO-RSA bony increased offset reverse shoulder arthroplasty, IQR interquartile range, RSA reverse shoulder arthroplasty, SD standard deviation, VAS visual analogue scale
*Improvement measured in number of anatomic landmarks (such as one vertebra) surpassed superiorly compared with the preoperative level reached
Bt-test
DMann–Whitney U test
Clinical outcomes
Information on clinical outcomes was available in 52 patients (74%). Postoperatively, there were no cases with an external rotation lag sign or Hornblower sign. All ROM measurements in the total cohort improved significantly compared with preoperative measurements (p < 0.0132), except for internal rotation (p = 0.052). There were no differences between the two groups in ROM at final follow-up (p = 1.000). The level reached in internal rotation improved by more anatomical landmarks in the BIO-RSA 38 group (Δ4.7, SD Δ5.3 versus Δ−1.4, SD Δ5.3, p = 0.0352, Table 5).
Radiographic outcomes
Radiographs were available in 45 patients (59%). The interobserver reliability between the first to assessors was good for the lateralisation shoulder angle [LSA; ICC: 0.851, 95% confidence interval (CI): 0.457, 0.942] and for the inferior overhang (ICC: 0.769, 95%CI: 0.600, 0.873), and was excellent for the distalisation shoulder angle (DSA; ICC: 0.911, 95%CI: 0.842, 0.951). The reliability was poor for the radiological grading of scapular notching (k = 0.425), glenoid lucencies (k= 0.161) humeral lucencies (k = 0.474), ossification (k = 0.353) and for the assessment of graft healing (k = 0.068). The reliability was moderate for the assessment of graft viability (k = 0.644), zones of humeral lucencies (k = 0.581) and stress shielding (k = 0.536).
None of the components were considered at risk of loosening (notching grade IV, radiolucencies grade III or IV, or radiolucencies in more than three zones). Of the 25 patients with a BIO-RSA and available radiographs, the graft was considered viable in 21 cases (84%) and healed in 23 cases (92%). The inferior overhang was greater in the RSA 42 group (4.91 mm; SD 1.84 versus 2.96 mm; SD 1.80, p = 0.02186). The other radiographic measurements and outcomes did not significantly differ between the two groups (p > 0.485, Table 6).
Table 6.
Radiographic measurements and outcomes
| BIO-RSA 38 (n = 25) | RSA 42 (n = 20) | p-value | Adjusted p-value | |
|---|---|---|---|---|
| Lateralisation angle, mean ° (SD) | 82.7 (8.2) | 82.8 (8.0) | B0.738 | 1.000 |
| Distalisation angle, mean ° (SD) | 52.1 (8.1) | 57.6 (9.4) | B0.04846 | 0.436 |
| Lateralisation/distalisation, median (IQR) | 1.62 (1.40–1.71) | 1.42 (1.21–1.77) | D0.178 | 1.000 |
| Inferior overhang, mean mm (SD) | 2.96 (1.80) | 4.91 (1.84) | B0.002186 | 0.02186 |
| Notching, n (%) | C0.853 | 1.000 | ||
| None | 18 (75) | 16 (80) | ||
| Grade I | 5 (21) | 3 (15) | ||
| Grade II | 1 (5) | 1 (4) | ||
| Glenoid: lucency grade, n (%) | C0.708 | 1.000 | ||
| None | 23 (96) | 19 (95) | ||
| Grade I | 0 (0) | 1 (5) | ||
| Grade II | 1 (4) | 0 (0) | ||
| Humerus: lucencies, median n of zones (IQR) | 0 (0–1) | 0 (0–0) | D0.155 | 1.000 |
| Humerus: highest grade of lucencies, n (%) | C0.233 | 1.000 | ||
| None | 18 (72) | 18 (90) | ||
| Grade I | 4 (16) | 0 (0) | ||
| Grade II | 2 (8) | 2 (10) | ||
| Grade III | 1 (4) | 0 (0) | ||
| Ossification grade, n (%) | C0.492 | 1.000 | ||
| None | 18 (72) | 16 (80) | ||
| Grade I | 5 (20) | 3 (15) | ||
| Grade II | 2 (8) | 0 (0) | ||
| Grade III | 0 (0) | 1 (5) | ||
| Stress shielding, n (%) | 3 (12) | 2 (10) | C1.000 | 1.000 |
| Graft healed, n (%) | 23 (92) | |||
| Graft viable, n (%) | 21 (84) |
BIO-RSA bony increased offset reverse shoulder arthroplasty, mm millimetres, RSA reverse shoulder arthroplasty
Achi-square
Bt-test
CFisher exact test
DMann–Whitney U test
Complications
Three unfavourable events occurred: one patient in the BIO-RSA 38 group suffered a periprosthetic fracture of the humeral diaphysis which healed successfully with conservative treatment. One patient in the RSA 42 group underwent a single-stage revision replacing all components 6 months after the primary RSA owing to a periprosthetic joint infection. One patient in the BIO-RSA 38 group underwent a revision owing to aseptic loosening of the glenoid 3 years after the primary RSA, in which the glenoid components were replaced and the glenoid was reconstructed with a bone graft from the iliac crest.
Discussion
The current study aimed to compare the outcomes of RSA using a larger (size 42) glenosphere with BIO-RSA with a regular glenosphere (size 38), using a Delta Xtend prosthesis for both groups, designed as an inlay prosthesis with a 155 ° neck-shaft angle. At the final follow-up, there was no difference in postoperative ROM and PROMs between the groups. The level reached in internal rotation increased by a greater amount in the BIO-RSA 38 group (p = 0.0352). However, although not statistically significant, internal rotation trended towards lower preoperative values in the BIO-RSA 38 group. Furthermore, the clinical relevance of this difference is questionable. Similarly, external rotation improved markedly in the BIO-RSA group but was inferior preoperatively in this group. Both differences were not statistically significant. Apart from a greater inferior overhang in the RSA 42 group, there were no differences in radiographic measurements or outcomes. These results suggest that using a larger glenosphere size is a feasible alternative for lateralising RSA.
Range of motion
Previous studies have found glenoid lateralisation to be associated with postoperative range of motion, alongside preoperative shoulder function, preoperative status of the rotator cuff, surgical approach and implant design [28–30]. To our knowledge, there are no previous studies directly comparing BIO-RSA with a regular glenosphere size to RSA using a larger glenosphere size. The literature comparing BIO-RSA with regular RSA, regardless of glenosphere size, is contradictory. Only a few studies report improved rotational ROM, which did not seem to translate to superior PROM results [31–33]. Similarly, literature comparing ROM between glenosphere sizes is sparse and contradictory. Some studies report superior ROM, which does not translate to superior PROM results [5–7, 34]. Our results suggest that the benefit in terms or rotational ROM when using a BIO-RSA instead of a regular RSA is matched by the benefit of using a larger glenosphere.
The increase in lateralisation when using a size 42 glenosphere, which is currently the largest commercially available glenosphere for this implant model, instead of a size 38 is minimal (2 mm) compared with the increase in lateralisation when opting for BIO-RSA (1 cm). In the current study, the poly-ethylene insert was the same size for both groups. The increased lateralisation in BIO-RSA leads to greater muscle tension, which is beneficial for movement. Despite the minimal lateralisation, using a larger glenosphere also leads to increased wrapping of the surrounding muscles around the prosthesis which also increases muscle tension. In contrast to BIO-RSA, the larger glenosphere also does not change the centre of rotation, thereby maintaining the positive effect on the deltoid moment arm that is inherent to the medialised centre of rotation in RSA. Nevertheless, increasing the size of the glenosphere also increases the dynamic anteroposterior span of the prosthesis, leading to an increased rotational arc of the humerus. This results in a more anterior position of the humerus in internal rotation, which may cause an anterior conflict between the greater tuberosity and the conjoined tendon-coracoid complex, potentially limiting internal rotation. Using BIO-RSA with a standard glenosphere does not increase the diameter of the rotational arc, potentially avoiding an anterior conflict. Further biomechanical studies are required to confirm the dynamic changes caused by increasing the glenosphere size.
Previous studies focus on objective ROM measured in clinic. However, for daily activities requiring rotational motion, more complex movements are necessary than internal or external rotation alone, such as adequate abduction and extension [35]. A previous study confirmed this discordance between objective and patient-reported range of motion [36]. To assess functional internal and external rotation in tasks of daily living the ADLIR and ADLER questionnaires were used in this study. Satisfactory results were achieved in our cohort of patients undergoing RSA and BIO-RSA (median ADLIR > 84/100 and median ADLER 29/30) and no difference was observed between the two groups.
Radiographic parameters
Implant positioning was assessed on radiographs using the LSA, DSA, and inferior overhang. Interestingly, the angles did not differ significantly between the groups, despite inherent differences in implant positioning. A possible explanation may be the inaccuracy of these measurements on plain radiographs: the angle is highly dependent on the angle in which the radiograph is taken and the position of the arm. Furthermore, the inferior overhang was significantly lower in the BIO-RSA 38 group (p = 0.02186). However, the overhang is measured using lines drawn parallel to the central peg of the glenoid. In contrast to regular RSA, the glenoid component is placed in about 10 ° inferior inclination when using a BIO-RSA technique as described by Boileau et al.[37]. This results in a lower measurement than the true inferior overhang.
In the current cohort, the rate of scapular notching did not differ between the two groups (p = 1.000). To our knowledge, there are no previous studies comparing radiographic outcomes between BIO-RSA and regular RSA using a larger glenosphere. However, two previous studies comparing BIO-RSA with regular RSA regardless of glenosphere size found a higher rate of notching in the RSA group (75% versus 40% and 68% versus 33%, p < 0.028) [33, 38]. When a larger glenoid component is placed in the same position, more inferior overhang is created, potentially decreasing the rate of notching. One previous randomised study found a significant reduction in scapular notching rate using a larger glenoid component; 49% in patients receiving a 38-mm component, and 12% with a 42-mm component [4].
Costs
BIO-RSA using an autograft from the humeral head is more economical compared with other lateralisation techniques, such as using an allograft or an augmented baseplate [39]. However, the added operative time and specific operative tools required for this procedure still lead to increased costs compared with regular RSA, while opting for a larger glenosphere does not increase the time or costs of the procedure. We hypothesize that regular RSA using a larger glenosphere is more cost-effective than BIO-RSA.
Limitations
First, patients were identified retrospectively, which may lead to a selection bias owing to the factors influencing the decision to perform RSA or BIO-RSA. To address this shortcoming, patients were matched to create more comparable groups. Despite including age as a matching parameter, the age differed significantly between the groups, this may indicate that the RSA cohort was too small to achieve optimal matching. There was also a significant difference in follow-up time between the groups. This reflects current practice as BIO-RSA is becoming increasingly popular in recent years. We intentionally selected a large time window to include a large cohort, which benefits the matching accuracy. The difference in follow-up time may be a source of bias, however, a previous study found no significant changes in results after 1 year, which was the minimum follow-up in this study [8]. Furthermore, the approach differed between the groups (the anterosuperior approach was used for regular RSA and the deltopectoral approach for BIO-RSA); however, the approach did not influence outcomes in previous studies [40, 41]. Second, bone graft healing and viability, and implant positioning is best assessed on computed tomography (CT) scans instead of radiographs. However, CT scans were not available in all patients. To maintain methodological consistency, we opted to assess these factors on radiographs in all patients. Last, the current cohort is too small to compare rare complications and revisions between the two groups.
Conclusions
At a minimum of 1 year follow-up, there was no difference in range of motion when comparing BIO-RSA with a size 38 glenosphere to RSA with a size 42 glenosphere. Similarly, no differences were found in patient-reported and radiographic results, apart from a smaller inferior overhang in the BIO-RSA group. However, prospective, randomised studies are required to confirm the findings, as well as including different prosthesis designs. Besides the similar clinical results found in this study, increasing the glenosphere size is less technically demanding and time consuming compared with BIO-RSA, less costly, and does not have technique-specific complications, such as graft non-union and resorption. These findings suggest that using a larger glenosphere size is a feasible and simple alternative to BIO-RSA for lateralising RSA. The conclusions of this study may also add perspective for manufacturers to pursue development and research towards larger (i.e. 44–46 mm) glenospheres.
Supplementary Information
Additional file 1: Table S1. Radiographic analysis methods.
Acknowledgements
None.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Biographies
Arno A. Macken
is an MD and a PhD candidate in Orthopaedics.
Geert Alexander Buijze
is a fellowship-trained shoulder surgeon, an assistant-professor, and has obtained a PhD in orthopaedics.
Michael Kimmeyer
is a fellowship-trained shoulder surgeon.
Tilman Hees
is a fellowship-trained shoulder surgeon.
Denise Eygendaal
is a fellowship-trained upper extremity surgeon, has obtained a PhD in orthopaedics, is a professor in orthopaedics, and is the head of the department of orthopaedics and sports medicine.
Michel van den Bekerom
is a fellowship-trained upper extremity surgeon, has obtained a PhD in orthopaedics, is a professor in orthopaedics and traumatology.
Laurent Lafosse
is a fellowship-trained shoulder and brachial plexus surgeon.
Thibault Lafosse
is a fellowship-trained shoulder and brachial plexus surgeon.
Author contributions
AAM performed study conceptualisation, data curation, formal analysis, investigation, methodology, project administration, resource acquisition, software, supervision, validation, visualisation, writing—original draft and writing—review & editing; GAB performed study conceptualisation, methodology, project administration, resource acquisition, supervision, validation and writing—review & editing; MK performed data curation, formal analysis, investigation, methodology, project administration, visualisation and writing—original draft; TL performed data curation and writing—review & editing; DE contributed to the methodology, resources, supervision and writing—review & editing; MvdB contributed to the methodology, resources, supervision and writing—review & editing; LL performed study conceptualisation, resource acquisition and writing—review & editing; TL performed study conceptualisation, methodology, project administration, resource acquisition, supervision, validation and writing—review & editing.
Data availability
Data will be made available upon reasonable request with the authors.
Declarations
Ethics approval and consent to participate
Ethical approval was provided by the National Commission on Informatics and Liberty (Commission nationale de l’informatique et des libertés) 3 Place de Fontenoy—TSA 80715—75334 Paris cedex under the IRB number: 2229030.
Consent for publication
Not applicable.
Competing interests
AAM declares no competing interests; GAB provided consultancy services for Stryker; MK declares no competing interests; TL declares no competing interests; DE declares no competing interests; MvdB declares no competing interests; LL received royalties from Depuy and provided consultancy services for Stryker and Smith and Nephew; TL provided consultancy for Depuy, Stryker and Smith and Nephew. This study received no funding or other forms of support.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Boileau P, Watkinson DJ, Hatzidakis AM, Balg F. Grammont reverse prosthesis: design, rationale, and biomechanics. J Shoulder Elb Surg. 2005;14:S147–S161. doi: 10.1016/j.jse.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 2.Umar M, Hughes M, Barrington-Ford LM, Pearson K, Waseem M. Comparison of bony increased offset-reverse shoulder arthroplasty and standard reverse shoulder arthroplasty outcomes. J Orthop. 2020;18:58–62. doi: 10.1016/j.jor.2019.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony increased-offset reversed shoulder arthroplasty minimizing scapular impingement while maximizing glenoid fixation. Clin Orthop Relat Res. 2011;469:2558–2567. doi: 10.1007/s11999-011-1775-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Torrens C, Guirro P, Miquel J, Santana F. Influence of glenosphere size on the development of scapular notching: a prospective randomized study. J Shoulder Elb Surg. 2016;25:1735–1741. doi: 10.1016/j.jse.2016.07.006. [DOI] [PubMed] [Google Scholar]
- 5.Müller AM, Born M, Jung C, Flury M, Kolling C, Schwyzer HK, Audigé L. Glenosphere size in reverse shoulder arthroplasty: is larger better for external rotation and abduction strength? J Shoulder Elb Surg. 2018;27:44–52. doi: 10.1016/j.jse.2017.06.002. [DOI] [PubMed] [Google Scholar]
- 6.Mollon B, Mahure SA, Roche CP, Zuckerman JD. Impact of glenosphere size on clinical outcomes after reverse total shoulder arthroplasty: an analysis of 297 shoulders. J Shoulder Elb Surg. 2016;25:763–771. doi: 10.1016/j.jse.2015.10.027. [DOI] [PubMed] [Google Scholar]
- 7.Al Yaseen M, Smart YW, Seyed-Safi P, Abdelmonem AH, Makki D, Morgan B, Sandher D. Effect of implant size, version and rotator cuff tendon preservation on the outcome of reverse shoulder arthroplasty. Cureus. 2022 doi: 10.7759/CUREUS.25741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mahendraraj KA, Carducci MP, Galvin JW, Golenbock SW, Grubhofer F, Jawa A. Reassessing the minimum two-year follow-up standard after total shoulder arthroplasty-is one year sufficient? Shoulder Elb. 2021;13:527–533. doi: 10.1177/1758573220922845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Audigé L, Schwyzer HK, Äärimaa V, et al. Core set of unfavorable events of shoulder arthroplasty: an international Delphi consensus process. J Shoulder Elb Surg. 2019;28:2061–2071. doi: 10.1016/j.jse.2019.07.021. [DOI] [PubMed] [Google Scholar]
- 10.Gilbart MK, Gerber C. Comparison of the subjective shoulder value and the constant score. J Shoulder Elb Surg. 2007;16:717–721. doi: 10.1016/j.jse.2007.02.123. [DOI] [PubMed] [Google Scholar]
- 11.Constant CR, Gerber C, Emery RJH, Søjbjerg JO, Gohlke F, Boileau P. A review of the constant score: modifications and guidelines for its use. J Shoulder Elb Surg. 2008;17:355–361. doi: 10.1016/j.jse.2007.06.022. [DOI] [PubMed] [Google Scholar]
- 12.Kocher MS, Horan MP, Briggs KK, Richardson TR, O’Holleran J, Hawkins RJ. Reliability, validity, and responsiveness of the American shoulder and elbow surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Jt Surg. 2005;87:2006–2011. doi: 10.2106/00004623-200509000-00014. [DOI] [PubMed] [Google Scholar]
- 13.Beckers JJ, Lafosse L, Caruso G, Kopel L, Commeil P, Mariaux S, Lafosse T. A pilot-study focusing on internal rotation after reverse total shoulder arthroplasty using the activities of daily living which require internal rotation (ADLIR) score. Shoulder Elb. 2021 doi: 10.1177/17585732211053273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Werthel JD, Wagner ER, Elhassan BT. Long-term results of latissimus dorsi transfer for internal rotation contracture of the shoulder in patients with obstetric brachial plexus injury. JSES Open Access. 2018;2:159. doi: 10.1016/j.jses.2018.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Boileau P, Chuinard C, Roussanne Y, Neyton L, Trojani C. Modified latissimus dorsi and teres major transfer through a single delto-pectoral approach for external rotation deficit of the shoulder: as an isolated procedure or with a reverse arthroplasty. J Shoulder Elb Surg. 2007;16:671–682. doi: 10.1016/j.jse.2007.02.127. [DOI] [PubMed] [Google Scholar]
- 16.Boutsiadis A, Lenoir H, Denard PJ, Panisset JC, Brossard P, Delsol P, Guichard F, Barth J. The lateralization and distalization shoulder angles are important determinants of clinical outcomes in reverse shoulder arthroplasty. J Shoulder Elb Surg. 2018;27:1226–1234. doi: 10.1016/j.jse.2018.02.036. [DOI] [PubMed] [Google Scholar]
- 17.Duethman NC, Aibinder WR, Nguyen NTV, Sanchez-Sotelo J. The influence of glenoid component position on scapular notching: a detailed radiographic analysis at midterm follow-up. JSES Int. 2020;4:144–150. doi: 10.1016/j.jses.2019.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Jt Surg—Ser B. 2004 doi: 10.1302/0301-620X.86B3.14024. [DOI] [PubMed] [Google Scholar]
- 19.Spiry C, Berhouet J, Agout C, Bacle G, Favard L. Long-term impact of scapular notching after reverse shoulder arthroplasty. Int Orthop. 2021;45:1559–1566. doi: 10.1007/s00264-021-04998-3. [DOI] [PubMed] [Google Scholar]
- 20.Brooker AF, Bowerman JW, Robinson RARL. Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Jt Surg Am. 1973;55(8):1629–1632. doi: 10.2106/00004623-197355080-00006. [DOI] [PubMed] [Google Scholar]
- 21.Durchholz H, Salomonsson B, Moroder P, Lambert S, Page R, Audigé L. Core set of radiographic parameters for shoulder arthroplasty monitoring: criteria defined by an international delphi consensus process. JBJS Open Access. 2019 doi: 10.2106/JBJS.OA.19.00025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schoch BS, Barlow JD, Schleck C, Cofield RH, Sperling JW. Shoulder arthroplasty for post-traumatic osteonecrosis of the humeral head. J Shoulder Elb Surg. 2016;25:406–412. doi: 10.1016/j.jse.2015.08.041. [DOI] [PubMed] [Google Scholar]
- 23.Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components. A radiographic analysis of loosening. Clin Orthop Relat Res NO. 1979;141:17–27. [PubMed] [Google Scholar]
- 24.Melis B, DeFranco M, Lädermann A, Molé D, Favard L, Nérot C, Maynou C, Walch G. An evaluation of the radiological changes around the Grammont reverse geometry shoulder arthroplasty after eight to 12 years. J Bone Jt Surg—Ser B. 2011;93B:1240–1246. doi: 10.1302/0301-620X.93B9.25926. [DOI] [PubMed] [Google Scholar]
- 25.Pearce N. Analysis of matched case-control studies. Br Med J. 2016 doi: 10.1136/BMJ.I969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bland JM, Altman DG. Statistics notes: matching. Br Med J. 1994;309:1128. doi: 10.1136/bmj.309.6962.1128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159. doi: 10.2307/2529310. [DOI] [PubMed] [Google Scholar]
- 28.Luster TG, Dean RS, Trasolini NA, Josef K, Parada SA, Ralston RK, Waterman BR. Predictive factors influencing internal rotation following reverse total shoulder arthroplasty. J Shoulder Elb Surg. 2023 doi: 10.1016/j.jse.2023.10.006. [DOI] [PubMed] [Google Scholar]
- 29.Hao KA, Cueto RJ, Gharby C, Freeman D, King JJ, Wright TW, Almader-douglas D, Schoch BS, Werthel J. Influence of lateralized versus medialized reverse shoulder arthroplasty design on external and internal rotation : a systematic review and meta-analysis. Clin Shoulder Elb. 2023 doi: 10.5397/cise.2023.00577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ducharne L, Godenèche A, Nérot C, Aswad R, Resurg S, Garret J. Factors that affect external rotation following reverse shoulder arthroplasty : a retrospective multi-centre study on 501 shoulders. Arch Orthop Trauma Surg. 2023;143(11):6487–6496. doi: 10.1007/s00402-023-04935-6. [DOI] [PubMed] [Google Scholar]
- 31.Amorim-Barbosa T, Ribau A, Fonte H, Barros LH, Claro R. Comparative clinical and radiologic evaluation between patients undergoing standard reversed shoulder arthroplasty or bony increased offset. Clin Shoulder Elb. 2023 doi: 10.5397/CISE.2022.01270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Imai S. Restoration of external rotation following a lateral approach for glenoid bony increased-offset reverse shoulder arthroplasty. JB JS open access. 2021 doi: 10.2106/JBJS.OA.20.00136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Athwal GS, MacDermid JC, Reddy KM, Marsh JP, Faber KJ, Drosdowech D. Does bony increased-offset reverse shoulder arthroplasty decrease scapular notching? J Shoulder Elb Surg. 2015;24:468–473. doi: 10.1016/j.jse.2014.08.015. [DOI] [PubMed] [Google Scholar]
- 34.Sabesan VJ, Ackerman J, Sharma V, Baker KC, Kurdziel MD, Wiater JM. Glenohumeral mismatch affects micromotion of cemented glenoid components in total shoulder arthroplasty. J Shoulder Elb Surg. 2015;24:814–822. doi: 10.1016/j.jse.2014.10.004. [DOI] [PubMed] [Google Scholar]
- 35.Hochreiter B, Wyss S, Gerber C. Extension of the shoulder is essential for functional internal rotation after reverse total shoulder arthroplasty. J Shoulder Elb Surg. 2022;31:1166–1174. doi: 10.1016/j.jse.2021.11.006. [DOI] [PubMed] [Google Scholar]
- 36.Hao KA, Kakalecik J, Cueto RJ, Janke RL, Wright JO, Wright TW, Farmer KW, Struk AM, Schoch BS, King JJ. Discordance between patient-reported and objectively measured internal rotation after reverse shoulder arthroplasty. J Shoulder Elb Surg. 2023;32:2051–2058. doi: 10.1016/j.jse.2023.03.033. [DOI] [PubMed] [Google Scholar]
- 37.Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony increased offset-reversed shoulder arthroplasty (BIO-RSA) JBJS Essent Surg Tech. 2017;7:e37. doi: 10.2106/JBJS.ST.17.00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kirzner N, Paul E, Moaveni A. Reverse shoulder arthroplasty vs BIO-RSA clinical and radiographic outcomes at short term follow-up. J Orthop Surg Res. 2018;13:1–7. doi: 10.1186/s13018-018-0955-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Boileau P, Morin-Salvo N, Gauci MO, Seeto BL, Chalmers PN, Holzer N, Walch G. Angled BIO-RSA (bony-increased offset–reverse shoulder arthroplasty): a solution for the management of glenoid bone loss and erosion. J Shoulder Elb Surg. 2017;26:2133–2142. doi: 10.1016/j.jse.2017.05.024. [DOI] [PubMed] [Google Scholar]
- 40.Seok HG, Park JJ, Park SG. Anterosuperior approach versus deltopectoral approach for reverse total shoulder arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17:527. doi: 10.1186/s13018-022-03414-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Macken AA, Haagmans-Suman A, van Spekenbrink-Spooren A, van Noort A, van den Bekerom MPJ, Eygendaal D, Buijze GA. Anterosuperior versus deltopectoral approach for primary reverse total shoulder arthroplasty. Bone Joint J. 2023;105-B:1000–1006. doi: 10.1302/0301-620X.105B9.BJJ-2023-0238.R1. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. Radiographic analysis methods.
Data Availability Statement
Data will be made available upon reasonable request with the authors.