

Dear Editors,
In this Journal, Weide et al. [1] reported unexpected favorable survival rates after intratumoral treatment with interleukin-2 (IL-2) in patients with cutaneous and soft tissue metastases of malignant melanoma (MM) without lymph node or visceral involvement. This study also showed a complete response in 66.70 % of the patients treated, with 25 % remaining free of any recurrence after intratumoral IL-2 [1].
A 77-year-old woman with a past history of a T4b primary MM on the right foot (Breslow thickness 4.30 mm) and groin dissection performed 3 years previously (N2b stage) presented at our melanoma unit with a biopsy-proven in-transit metastasis on the distal third of the left leg (Fig. 1a). Gadolinium MRI images of the leg demonstrated a 53 × 52 × 50 mm subcutaneous tumor involving the calf muscle and a second 40 × 48 × 56 mm transit infiltrating the posterior tibial neurovascular bundle (Fig. 1b). A PET-CT scan failed to show visceral metastatic involvement. The lesion was considered unresectable, and the comorbidities of the patient, primarily morbid obesity with prominent groin folder, precluded isolated limb perfusion. Radiation therapy provided no clinical or radiological response.
Fig. 1.
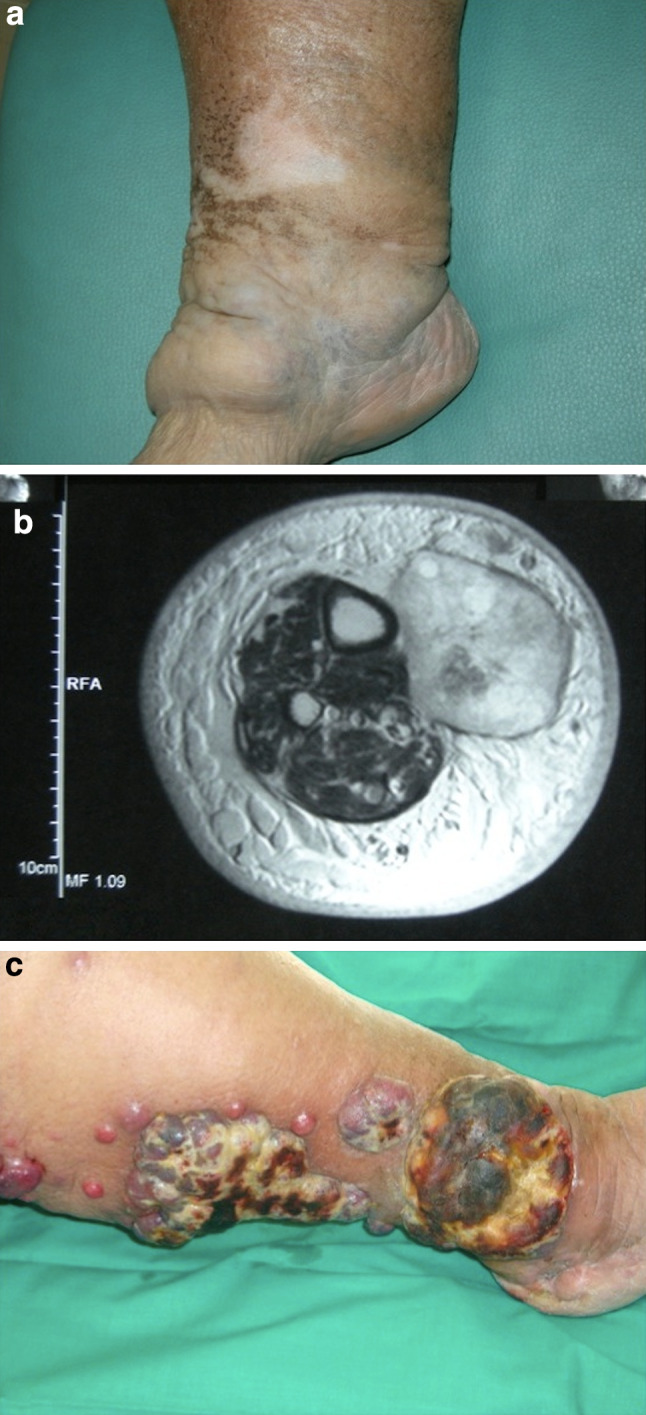
In-transit metastasis of malignant melanoma on the lower leg. a On physical examination, the distal third of the left leg presented 2 deep, firm, and painless tumoral nodules. b Gadolinium MRI image of the upper in-transit lesion infiltrating the calf muscle. c Progression of the nodules after the treatment with intralesional interleukin-2
The patient had reported local pain resistant to conventional therapies, which prevented her from walking. The patient was then offered intralesional treatment with interleukin-2. Total daily doses of 6-10 MIU of recombinant human IL-2 (Proleukin®) were divided between both subcutaneous lesions, using sonography to guide the injections. This dose was administered twice a week during the first 4 weeks.
After this initial treatment, the tumors became inflamed and ulcerated and entered a fast-growing phase with an outbreak of new in-transit lesions along the leg and thigh (Fig. 1c). Continuous bleeding and intractable pain led the patient to accept amputation. However, this surgical option was ultimately not performed because the patient died 2 weeks later due to severe symptomatic hyponatremia (serum sodium 118.2 mEq/L) that was unresponsive to supportive therapy.
In addition to the Weide et al. [1–3] study, several recent studies have stressed the advantages of local therapy for in-transit melanoma with intralesional interleukin-2. However, no study describes an association between tumor size and potential local toxicity. The mechanism of action of intralesional interleukin-2 is unknown. However, it is hypothesized that it works through a combination of tumor cytolysis by activated killer cells and apoptosis with an intense dermal intratumoral and peritumoral inflammatory response [1, 3]. Thus, the dramatic clinical changes observed might be explained as a consequence of tumoral necrosis and inflammation. Nevertheless, new in-transit lesions developed simultaneously despite the stability of the in-transit lesions prior to the treatment. This evolution might support the hypothesis of paradoxical tumor growth after the intralesional injection of IL-2 in a bulky tumor.
Although acceptable results have been demonstrated using intralesional interleukin-2 for this difficult clinical condition, this option should be offered cautiously to patients with bulky in-transit MM metastases.
Acknowledgments
Conflict of interest
None declared.
References
- 1.Weide B, Eigentler TK, Pflugfelder A, Leiter U, Meier F, Bauer J, et al. Survival after intratumoral interleukin-2 treatment of 72 melanoma patients and response upon the first chemotherapy during follow-up. Cancer Immunol Immunother. 2011;60:487–493. doi: 10.1007/s00262-010-0957-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weide B, Derhovanessian E, Pflugfelder A, Eigentler TK, Radny P, Zelba H, et al. High response rate after intratumoral treatment with interleukin-2. Cancer. 2010;116:4139–4146. doi: 10.1002/cncr.25156. [DOI] [PubMed] [Google Scholar]
- 3.Dehesa LA, Vilar-Alejo J, Valeron-Almazan P, Carretero G. Experience in the treatment of cutaneous in transit melanoma metastases and satellitosis with intralesional interleukin-2. Actas Dermosifiliogr. 2009;100:571–585. doi: 10.1016/S0001-7310(09)71905-2. [DOI] [PubMed] [Google Scholar]