

Abstract
Introduction
The International Federation for Surgery for Obesity and Metabolic Disorders (IFSO) Global Registry aims to provide descriptive data about the caseload and penetrance of surgery for metabolic disease and obesity in member countries. The data presented in this report represent the key findings of the eighth report of the IFSO Global Registry.
Methods
All existing Metabolic and Bariatric Surgery (MBS) registries known to IFSO were invited to contribute to the eighth report. Aggregated data was provided by each MBS registry to the team at the Australia and New Zealand Bariatric Surgery Registry (ANZBSR) and was securely stored on a Redcap™ database housed at Monash University, Melbourne, Australia. Data was checked for completeness and analyzed by the IFSO Global Registry Committee. Prior to the finalization of the report, all graphs were circulated to contributors and to the global registry committee of IFSO to ensure data accuracy.
Results
Data was received from 24 national and 2 regional registries, providing information on 502,150 procedures. The most performed primary MBS procedure was sleeve gastrectomy, whereas the most performed revisional MBS procedure was Roux-en-Y gastric bypass. Asian countries reported people with lower BMI undergoing MBS along with higher rates of diabetes. Mortality was a rare event.
Conclusion
Registries enable meaningful comparisons between countries on the demographics, characteristics, operation types and approaches, and trends in MBS procedures. Reported outcomes can be seen as flags of potential issues or relationships that could be studied in more detail in specific research studies.
Keywords: Registry, Demographics, Metabolic bariatric surgery, International trends
Introduction
Multiple randomized controlled trials (RCT), cohort studies, and case series from expert centers have demonstrated that metabolic bariatric surgery (MBS) is an effective treatment option for obesity, safely inducing not only weight loss but remission from important obesity-related diseases, including diabetes, hypertension, and cardiovascular disease [1–3]. How these positive results translate in the “real-world” setting remains largely unknown. There is also limited knowledge comparing the uptake and practice of MBS worldwide.
Registries use observational study methods to systematically collect uniform data, which are used to evaluate specified outcomes for a defined population [4]. In the field of MBS, these registries can be used to record the characteristics of the population undergoing MBS, document the types of procedures being performed, capture the safety of surgery through the prospective recording of quality indicators, and track the weight loss, health, and patient-reported outcomes of MBS. There are thirty known national and two complete regional MBS registries, each with an emerging dataset, with some having been shown already to improve outcomes for patients [5].
The International Federation for Surgery for Obesity and Metabolic Disorders (IFSO) has sought to drive collaborations between existing registries so that the positive outcomes achieved by individual registries may be translated globally. IFSO has also sought to help establish registries in other member countries that do not currently have a local registry. The Executive Board of IFSO established the IFSO Global Registry to facilitate these dual goals.
The IFSO Global Registry's mission is to provide the most credible and transparent information on MBS. To achieve this mission, the IFSO Global Registry aims to provide descriptive data about caseload and penetrance of surgery for metabolic disease and obesity in member countries and aspire to provide real-world surveillance of procedures and devices.
The first IFSO Global Registry report was produced in 2014. In that report, information was included from 18 countries coming from 5 continents that contributed 100,092 operation records, with 53,197 between the calendar years 2011–2013. The number of operations contributed ranged from one individual center that had entered 24 operation records to over 34,000 each from two countries with established national registries (Sweden and the United Kingdom).
Over time, contributions to the IFSO Global Registry have grown, and by the sixth report, there were 507,298 operations submitted by 50 contributor countries, 10 of whom were national or regional registries. However, including individual-level data from each contributing site created significant challenges for IFSO, particularly with the rigorous standards of data protection required by the General Data Protection Regulations (GDPR).
In 2022, the IFSO Global Registry Committee proposed to the Executive Board of IFSO that future reports include only aggregated data from established national or regional registries using a data dictionary focusing on demographic and descriptive data only. Outcome data was not included as it was inconsistently collected by registries worldwide, making comparisons difficult.
“Aggregated data” means that the data given to the IFSO Global Registry is already analyzed and provided as a mean or a median, meaning individuals cannot be identified. As no individual-level data transfer is required, there is no risk of a GDPR privacy breach. By only including data from national or complete regional registries, selection bias is reduced, making it more likely that the IFSO Global Report accurately represents the activity of an included country or region.
This is a summary of the key findings of the eighth report of the IFSO global registry and the second to contain only aggregated data from established national and regional registries [6].
Methods
Selected data items were chosen to describe the demographics of people with obesity who undergo MBS, the types of procedures being undertaken, and indicators of perioperative safety. A common data dictionary was developed through a consensus process and included the data items identified as the core for MBS registries through a previous collaboration with Bristol University [7].
All existing MBS registries known to IFSO were invited to contribute to the eighth report. Aggregated data was provided by each MBS registry to the team at the Australia and New Zealand Bariatric Surgery Registry (ANZBSR) and was securely stored on a Redcap™ database housed at Monash University, Melbourne, Australia.
Data was checked for completeness by the ANZBSR team and was then analyzed by the IFSO Global Registry Committee. Prior to the finalization of the report, all graphs were circulated to contributors and to the global registry committee of IFSO to ensure data accuracy (Fig. 1).
Fig. 1.

Process for data collection and collation
Statistical Methods
Aggregated data from each country or region is being compared, meaning that statistical comparisons are impossible as it is not possible to compare data that has already been analyzed and described as medians or means.
Caveats
Given that all contributing registries are well established and already collect data according to their definitions, it was not possible to completely align the data-set against the common data dictionary.
Not all countries or regions collected all of the data items that were chosen for the global report. Where an item is not collected, the country or region is not included in the reported information.
Results
Participants
Data were contributed by 24 countries and 2 complete regional registries (81.3% of all known registries), including information on 502,150 completed MBS in either 2021 (United Kingdom) or 2022 (rest of the world) (Fig. 2).
Fig. 2.

Number of metabolic bariatric surgical procedures per country or region. NB: X-axis is a logscale. Twenty-four countries and 2 regional registries contributed 502,150 procedures, with 449,815 (89.5%) primary procedures and 52,335 (10.5%) revisional procedures. Michigan is a state in the United States of America, and 39 of its 41 sites also contribute to the MBSAQIP (USA) Registry, meaning 10,437 procedures are potentially represented twice in this graph. The UK data is from 2021
Most procedures were primary MBS procedures (n = 449,815 (89.6%)), meaning they were the first MBS procedure a participant had undertaken. Revisional procedures (n = 52,335 (10.4%)) included those procedures undertaken to convert one MBS procedure to another or to correct a side effect of the procedure. The highest rates of revisional MBS were seen in Australia (Table 1).
Table 1.
Number of primary and revisional procedures by country or region
| Country or region | Primary (n) |
Revisional (n) |
Primary % |
Revisional % |
|---|---|---|---|---|
| United States of America | 204,324 | 52,335 | 88.6% | 11.4% |
| Brazil | 63,442 | 7,048 | 90.0% | 10.0% |
| France | 32,490 | 6,400 | 83.5% | 16.5% |
| China | 29,823 | 248 | 99.2% | 0.8% |
| Chile | 16,855 | 749 | 95.7% | 4.3% |
| Australia | 16,308 | 3,914 | 80.6% | 19.4% |
| Italy | 14,391 | 1,499 | 90.6% | 9.4% |
| Netherlands | 12,327 | 1,052 | 92.1% | 7.9% |
| USA—Michigan | 9,319 | 1,201 | 88.6% | 11.4% |
| Russia | 7,345 | 415 | 94.7% | 5.3% |
| Mexico | 6,649 | 409 | 94.2% | 5.8% |
| Iran | 6,631 | 141 | 97.9% | 2.1% |
| United Kingdom | 6,118 | 616 | 90.9% | 9.1% |
| Israel | 5,556 | 1,063 | 83.9% | 16.1% |
| Sweden | 4,677 | 223 | 95.4% | 4.6% |
| Canada—Ontario | 2,064 | 100 | 95.4% | 4.6% |
| New Zealand | 2,014 | 94 | 95.5% | 4.5% |
| Austria | 1,817 | 285 | 86.4% | 13.6% |
| Norway | 1,575 | 76 | 95.4% | 4.6% |
| South Korea | 1,406 | 60 | 95.9% | 4.1% |
| Venezuela | 1,351 | 132 | 91.1% | 8.9% |
| Azerbaijan | 1,191 | 32 | 97.4% | 2.6% |
| Kuwait | 934 | 187 | 83.3% | 16.7% |
| Uzbekistan | 614 | 5 | 99.2% | 0.8% |
| South Africa | 394 | 2 | 99.5% | 0.5% |
| Malaysia | 200 | 1 | 99.5% | 0.5% |
Data Completeness
Sweden, Michigan (USA), Netherlands, Ontario (Canada), France, and Israel reported complete, or near-complete, case ascertainment—meaning their local Registry captured every person who underwent a metabolic bariatric procedure. MBSAQIP (USA) reported 82.4%, Norway 89%, and Australia 82.2% case ascertainment. Other countries did not report case ascertainment.
Demographics and Setting
Twenty-five registries provided data on sex, being recorded as male or female. The majority of participants were female (81.1%). Females predominated in all contributing registries (Fig. 3).
Fig. 3.

Proportion of participants in registries recorded as female or male. Differences in overall numbers in each registry recording sex may reflect people identifying as a sex other than male or female or the field being incompletely recorded
Twenty-one registries provided the median age on the day of surgery. The median age day of surgery ranged from 31 years (IQR 25–37 years) in China to 44.7 years (IQR 35.8–53.5 years) in the United Kingdom (Table 2). Participants undergoing primary MBS were younger than those undergoing revisional MBS (Table 3). Males tended to be older than females, apart from in China, Kuwait, South Korea, Iran, Italy, and Malaysia, where they were younger (Table 3).
Table 2.
Median age on the day of surgery by country or region. Age day of surgery for all procedures by country or region
| Country | Median | Lower IQR | Upper IQR |
|---|---|---|---|
| Australia | 42.4 | 33.9 | 51.5 |
| Austria | 41 | 39.8 | 48 |
| Canada—Ontario | 43.8 | 36.1 | 51.8 |
| China | 31 | 25 | 37 |
| France | 41 | 32 | 51.1 |
| Iran | 38 | 31 | 45 |
| Israel | 37.2 | 28.2 | 47.2 |
| Italy | 45 | 35 | 52 |
| Kuwait | 34 | 25 | 42 |
| Malaysia | 41 | 35.5 | 47.5 |
| Netherlands | 45 | 34 | 54 |
| New Zealand | 43.6 | 35.2 | 51.9 |
| Norway | 42 | 32.5 | 51.2 |
| Russia | 40.8 | 34.4 | 48.8 |
| South Africa | 43 | 37 | 50 |
| South Korea | 35 | 29 | 42 |
| Sweden | 41 | 32 | 50 |
| United Kingdom | 44.7 | 35.8 | 53.5 |
| United States of America | 43 | 35 | 52 |
| USA- Michigan | 43 | 35 | 52 |
| Uzbekistan | 41 | 34 | 45 |
Table 3.
Median age on the day of surgery by country or region. Age day of surgery by sex for primary and revisional procedures by country or region
| Primary metabolic bariatric procedures | Revisional Metabolic Bariatric Procedures | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | All | Female | Male | All | |||||||||||||
| Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | |
| Australia | 39.9 | 32.2 | 49.4 | 42.6 | 34.8 | 51 | 40.5 | 32.7 | 49.8 | 49.5 | 41 | 57 | 51.2 | 42.6 | 58.6 | 49.9 | 41.2 | 57.4 |
| Austria | 39 | 40.4 | 48 | 43.2 | 41 | 50.5 | 40 | 40.7 | 48.7 | 48 | 27.5 | 40.9 | 54 | 29.4 | 44.6 | 49 | 27.6 | 41.7 |
| Canada—Ontario | 43.2 | 35.6 | 51.4 | 46.7 | 39.5 | 54.1 | 43.7 | 37.2 | 53.9 | 44.8 | 37.7 | 51.3 | 48.3 | 40.4 | 52.9 | 45.5 | 37.8 | 51.8 |
| China | 31 | 25 | 37 | 30 | 23 | 36 | 30 | 24.4 | 37 | 43.7 | 32.8 | 49.4 | 45.3 | 34.6 | 48.9 | 44.7 | 34.7 | 46.9 |
| Iran | 38 | 31 | 46 | 36 | 30 | 42 | 38 | 31 | 45 | 40 | 34 | 48 | 39 | 35 | 48 | 40 | 34 | 48 |
| Israel | 34.9 | 26.7 | 44.6 | 36.9 | 27.4 | 46.8 | 35.3 | 26.8 | 45.2 | 46.2 | 37.18 | 54.2 | 48.7 | 38.2 | 55.3 | 46.8 | 37.4 | 54.4 |
| Italy | 44 | 34 | 52 | 36 | 45 | 52 | 44 | 34 | 52 | 45 | 32 | 57 | 48 | 39 | 57 | 45 | 32 | 57 |
| Kuwait | 33 | 24 | 41 | 31 | 22 | 39 | 32 | 23 | 42 | 40 | 32 | 47 | 42 | 34 | 48 | 41 | 32 | 47 |
| Malaysia | 41 | 36 | 49 | 40 | 35 | 45.8 | 41 | 36 | 49 | 49 | 0 | 0 | 0 | 0 | 0 | 49 | 0 | 0 |
| Netherlands | 43 | 33 | 52 | 48 | 37 | 55 | 44 | 34 | 53 | 50 | 41 | 56 | 52 | 47 | 59 | 50 | 42 | 57 |
| New Zealand | 42.7 | 34.7 | 51.5 | 46.3 | 37.4 | 53.7 | 43.3 | 35.1 | 51.8 | 47.5 | 39.6 | 56.2 | 51.4 | 44.3 | 58.3 | 48.2 | 40.1 | 57 |
| Norway | 40.7 | 32 | 50.3 | 45.5 | 35 | 52.5 | 41.9 | 32.4 | 51 | 46.3 | 35.2 | 54.2 | 45.9 | 36.4 | 56.6 | 46.3 | 35.8 | 55.4 |
| Russia | 40.5 | 25.3 | 48.6 | 41.4 | 34.6 | 49.2 | 40.6 | 34.2 | 48.6 | 44.7 | 39.5 | 51.7 | 46 | 39.7 | 52.9 | 44.9 | 39.6 | 52 |
| South Africa | 41 | 36 | 49 | 46 | 38 | 54 | 43 | 37 | 50 | 50 | 50 | 50 | 48 | 48 | 48 | 49 | 48 | 50 |
| South Korea | 36 | 29 | 43 | 33 | 29 | 40 | 35 | 29 | 42 | 38.5 | 34 | 43.3 | 41 | 30.8 | 48 | 39 | 33.8 | 43.3 |
| Sweden | 40 | 32 | 49 | 44 | 35 | 52 | 40 | 34 | 50 | 46 | 37 | 54 | 48 | 39.5 | 52 | 46 | 37.5 | 54 |
| United Kingdom | 43.3 | 34.7 | 52.5 | 47.6 | 38.5 | 55.4 | 43.9 | 35.2 | 53 | 49.7 | 42.2 | 56.5 | 52.3 | 47.3 | 58.8 | 50.3 | 42.6 | 56.9 |
| United States of America | 42 | 34 | 51 | 45 | 37 | 54 | 43 | 34 | 52 | 49 | 42 | 57 | 52 | 44 | 59 | 50 | 42 | 57 |
| USA-Michigan | 42 | 34 | 51 | 45 | 38 | 54 | 42 | 34 | 51 | 48 | 40 | 55 | 52 | 43.5 | 61 | 48 | 41 | 56 |
| Uzbekistan | 36 | 28 | 43 | 44 | 30 | 49 | 40 | 29 | 46 | 38 | 36 | 40 | 46 | 44 | 48 | 42 | 40 | 44 |
The median BMI on the day of a primary MBS was collected by 21 registries and ranged from 36.1 kg/m2 for women in China to 47.7 kg/m2 for males in South Africa (Table 4).
Table 4.
BMI on the day of primary MBS by country and sex
| Female | Male | All | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | Median | Lower IQR | Upper IQR | |
| China | 36.1 | 32.1 | 41 | 40.4 | 35.9 | 46.1 | 37.4 | 33.1 | 42.9 |
| South Korea | 37.3 | 34.3 | 41.2 | 41.0 | 36.5 | 46.4 | 38.1 | 35.0 | 42.6 |
| Sweden | 40.2 | 36.7 | 44.3 | 42.3 | 38.7 | 46.7 | 40.6 | 37.2 | 44.8 |
| Israel | 41 | 38.5 | 44 | 42 | 39.1 | 45.7 | 41 | 38.7 | 44.5 |
| Norway | 40.6 | 37.4 | 44.6 | 42.9 | 39.3 | 47.5 | 41.1 | 37.7 | 45.2 |
| Netherlands | 41.6 | 39.3 | 45 | 41.9 | 39 | 45.7 | 41.7 | 39.2 | 45.1 |
| Malaysia | 43.5 | 35.3 | 45.9 | 44 | 38.2 | 50.5 | 42 | 36 | 46 |
| Kuwait | 41.5 | 38.8 | 46.1 | 43.1 | 40.1 | 49.8 | 42 | 39.2 | 47.1 |
| Iran | 41 | 38 | 45 | 43 | 40 | 47 | 42 | 39 | 45 |
| Italy | 41 | 38 | 45 | 43 | 39 | 48 | 42 | 38 | 46 |
| Australia | 41.8 | 37.7 | 47.1 | 43.3 | 39.2 | 48.9 | 42.1 | 38 | 47.5 |
| Russia | 41.5 | 37.1 | 47.3 | 45.3 | 41.0 | 51.1 | 42.2 | 37.4 | 47.8 |
| Uzbekistan | 42 | 38 | 44 | 44 | 40 | 46 | 43 | 39 | 45 |
| New Zealand | 43.0 | 38.9 | 48.5 | 44.6 | 40.2 | 51.6 | 43.3 | 39.1 | 48.8 |
| United States of America | 43 | 40 | 49 | 45 | 40 | 51 | 44 | 40 | 50 |
| Austria | 43.7 | 40.4 | 48 | 45.1 | 41 | 50.5 | 44 | 40.7 | 48.7 |
| USA-Michigan | 44.1 | 40.3 | 49.3 | 45.8 | 41.2 | 51.6 | 44.3 | 40.4 | 49.7 |
| United Kingdom | 45 | 40.6 | 50.4 | 46.5 | 41.5 | 52.3 | 45.1 | 40.8 | 50.7 |
| Canada—Ontario | 45.5 | 41.8 | 51.2 | 47.5 | 42.4 | 53.2 | 45.6 | 41.8 | 51.4 |
| South Africa | 45.2 | 41.3 | 52.2 | 47.7 | 42 | 55.2 | 45.8 | 41.6 | 53 |
*France collects BMI information differently from other registries. Their data is included for completeness below:
Procedure Types
The most commonly performed primary procedure worldwide was sleeve gastrectomy (SG) (Fig. 4a), and the most commonly performed revisional procedure was Roux-en-Y gastric bypass (RYGB) (Fig. 4b) with the caveat that the MSBAQIP (USA) has an additional category being “revisional/conversion” surgery that does not specify the subsequent procedure type.
Fig. 4.

MBS procedure type. *Potential for procedures to be represented twice due to possible overlaps with the datasets of the USA and Michigan. a Primary MBS procedures (n = 449,815). b Revisional procedures (n = 31,278; excluded 21,057 cases labelled revision/conversion cases from United States of America that did not have a procedure type specified)
However, there are differences between countries when considering primary MBS. While the United States of America (USA) reported 140,339 primary SG (68.8%), RYGB was the most commonly reported primary MBS in Brazil, Venezuela, Netherlands, Norway, Ontario (Canada), Austria, and Sweden, with one-anastomosis gastric bypass (OAGB) being the most common procedure in Israel and “other” procedures predominating in South Africa (Fig. 5a).
Fig. 5.
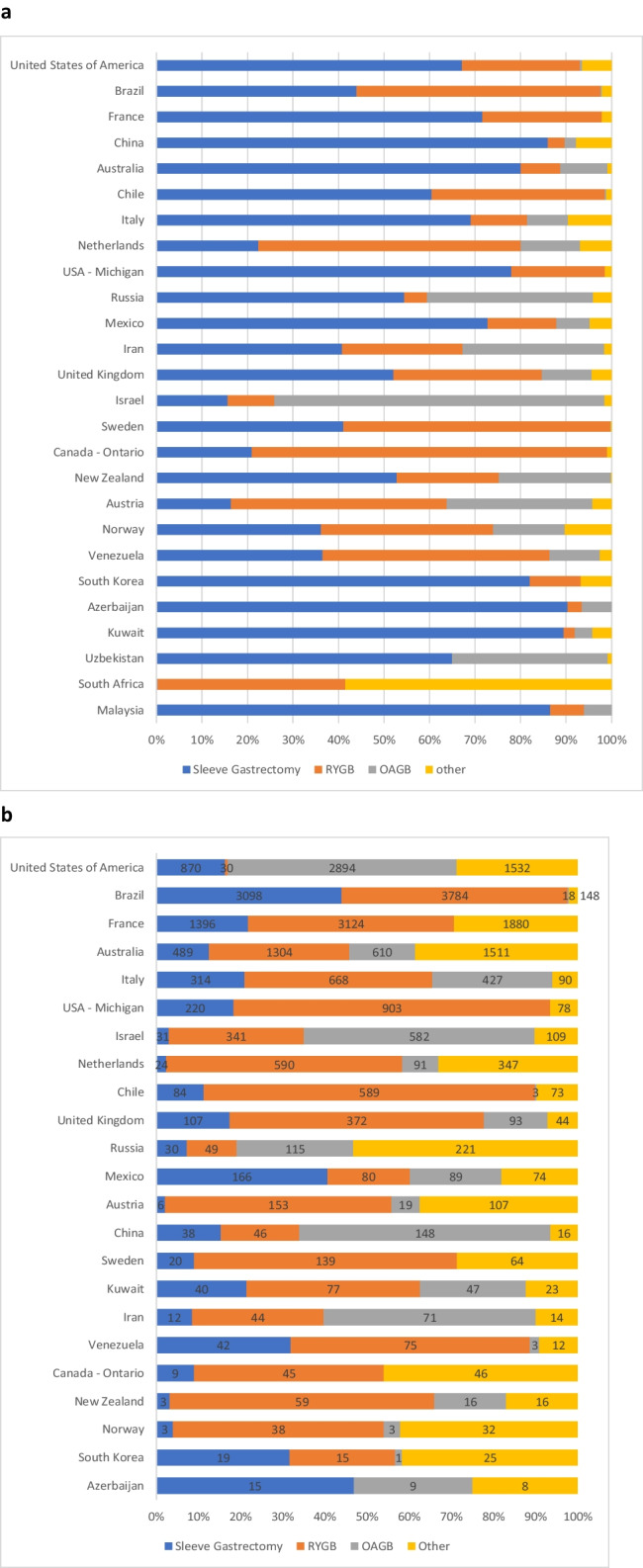
a Primary MBS types by country or region (n = 449,815). b Revisional MBS types by country or region (n = 52,335). Malaysia (n = 1), Uzbekistan (n = 5), and South Africa (n = 3) cannot be graphically displayed. The United States of America reported an additional 21,057 revisional cases labelled “revision/conversion” that are not able to be displayed graphically. This means the breakdown of procedures displayed in this graph may not be representative
Most procedures were completed laparoscopically, with the proportion of robotic cases being higher in the revisional setting (Table 5). The two USA-based registries reported the overall highest use of robotic systems.
Table 5.
Operative approach by country or region
| Primary MBS | Revisional MBS | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Laparoscopic | Open | Endoscopic | Robotic | Unspecified | Laparoscopic rate | Robotic rate | Laparoscopic | Open | Endoscopic | Robotic | Unspecified | Laparoscopic rate | Robotic rate | |
| Australia | 16,151 | 2 | 1 | 117 | 37 | 99.0% | 0.7% | 3769 | 21 | 78 | 35 | 11 | 96.3% | 0.9% |
| Austria | 1738 | 4 | 1 | 42 | 32 | 95.7% | 2.3% | 271 | 10 | 0 | 1 | 3 | 95.1% | 0.4% |
| Canada—Ontario | 2050 | 13 | 0 | 0 | 1 | 99.3% | 0.0% | 98 | 2 | 0 | 0 | 0 | 98.0% | 0.0% |
| France | 32,408 | 82 | 0 | 0 | 0 | 99.7% | 0.0% | 6,261 | 139 | 0 | 0 | 0 | 97.8% | 0.0% |
| Iran | 6624 | 7 | 0 | 0 | 0 | 99.9% | 0.0% | 141 | 0 | 0 | 0 | 0 | 100.0% | 0.0% |
| Israel | 5548 | 6 | 0 | 0 | 2 | 99.9% | 0.0% | 1057 | 6 | 0 | 0 | 0 | 99.4% | 0.0% |
| Italy | 12,926 | 5 | 0 | 88 | 1372 | 89.8% | 0.6% | 884 | 14 | 4 | 2 | 595 | 59.0% | 0.1% |
| Kuwait | 900 | 0 | 32 | 2 | 0 | 96.4% | 0.2% | 178 | 2 | 0 | 7 | 0 | 95.2% | 3.7% |
| Mexico | 6526 | 13 | 112 | 11 | 1 | 97.9% | 0.2% | 375 | 0 | 20 | 0 | 0 | 94.9% | 0.0% |
| Netherlands | 12,306 | 9 | 12 | 0 | 0 | 99.8% | 0.0% | 1039 | 10 | 3 | 0 | 0 | 98.8% | 0.0% |
| New Zealand | 2014 | 0 | 0 | 0 | 0 | 100.0% | 0.0% | 93 | 0 | 0 | 0 | 1 | 98.9% | 0.0% |
| Norway | 1576 | 0 | 0 | 0 | 0 | 100.0% | 0.0% | 74 | 2 | 0 | 0 | 0 | 97.4% | 0.0% |
| Russia | 7249 | 73 | 3 | 0 | 0 | 99.0% | 0.0% | 294 | 18 | 1 | 0 | 0 | 93.9% | 0.0% |
| South Africa | 393 | 1 | 0 | 0 | 0 | 99.7% | 0.0% | |||||||
| Sweden | 4665 | 7 | 0 | 0 | 5 | 99.7% | 0.0% | 218 | 4 | 0 | 0 | 1 | 97.8% | 0.0% |
| United Kingdom | 6012 | 13 | 18 | 75 | 0 | 98.3% | 1.2% | 597 | 7 | 2 | 9 | 1 | 96.9% | 1.5% |
| USA—Michigan | 6369 | 3 | 0 | 2,947 | 0 | 68.3% | 31.6% | 828 | 17 | 0 | 356 | 0 | 68.9% | 29.6% |
| United States of America | 203,060 | 90 | 1174 | 61,425 | 0 | 76.4% | 23.1% | 4152 | 132 | 1,042 | 991 | 0 | 65.7% | 15.7% |
| Uzbekistan | 614 | 0 | 0 | 0 | 0 | 100.0% | 0% | 5 | 0 | 0 | 0 | 0 | 100% | 0% |
| Venezuela | 1484 | 0 | 0 | 0 | 0 | 100.0% | 0% | |||||||
Diseases Associated with Obesity—Diabetes
The definition of diabetes varied between registries (Table 6) and included information on the number of people undergoing MBS and concurrent diabetes from 22 registries. The proportion of people undergoing MBS who also have diabetes ranges from 47.4% for Azerbaijan to 7.7% for France and 11% for the Norwegian and Australian Registries. Men are overrepresented in the proportion of people with diabetes undergoing MBS (Table 7).
Table 6.
Definition of diabetes by registry
| Country | Definition used |
|---|---|
| Australia | Diabetes Status at the Baseline is determined by the patient identifying themselves as having diabetes at the operation and having treatment for their diabetes |
| Canada—Ontario | Diabetes status at baseline is determined by the patient’s primary care physician at baseline |
| China | T2DM was defined as fasting blood glucose > 7.0 mmol/L, or/and random blood glucose > 11.1 mmol/L, or/and 2-h blood glucose after a 75-g oral glucose tolerance test > 11.1 mmol/L, or/and the use of antihyperglycemic drugs |
| Iran | Diabetes status at baseline is determined by the history of the previous diabetes diagnosis, receiving diabetes treatment or diagnosis based on lab tests (FBS > 126 or HbA1C > 6.5) at the time of operation |
| Israel | Self-reported by the patient before surgery |
| Italy | Diabetes status is determined according to ADA (American Diabetes Association) Diabetes Care 2014; 37(S 1): S81-90 |
| Kuwait | Patients with type 2 diabetes |
| Netherlands | > 42 mmol HbA1c/ mol HbA |
| New Zealand | Diabetes Status at the Baseline is determined by the patient identifying themselves as having diabetes at the operation and having treatment for their diabetes |
| Norway | Treated with medication |
| Russia | Diabetes status at baseline is determined by the patient self-reporting as having diabetes at the operation or having diabetes treatment |
| South Africa | ADA criteria for DM/pre-diabetes and gestational DM |
| South Korea | Diabetes status at baseline is determined by the patient identifying themselves as having diabetes at the time of the operation and having diabetes treatment |
| Sweden | Patients with type 2 diabetes and with medication f |
| United Kingdom | Patients with type 2 diabetes at surgery who are treated with diabetes medication |
| USA—Michigan | Type I or Type II diabetes: (Disease marked by high levels of sugar in the blood that occurs because the body does not respond correctly to insulin, a hormone released by the pancreas) non-insulin-dependent diabetes mellitus (NIDDM), adult-onset diabetes mellitus treated with (please check all that apply): Diet, Oral Medications, Insulin-dependent, Non-Insulin Injectables |
| Uzbekistan | Established type 2 diabetes mellitus before surgery, who are treated with diabetes medications |
Table 7.
Proportion of people undergoing primary MBS who also have diabetes
| Country or region | Female | Male | All | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Diabetes (n) | Total (n) | % with diabetes | Diabetes (n) | Total (n) | % with diabetes | Diabetes (n) | Total (n) | % with diabetes | |
| France | NA | NA | 6.5% | NA | NA | 13.1% | NA | NA | 7.7% |
| Norway | 96 | 1180 | 8.1% | 77 | 396 | 19.4% | 173 | 1576 | 11.0% |
| Australia | 1213 | 12,341 | 9.8% | 513 | 3149 | 16.3% | 1726 | 15,490 | 11.1% |
| Iran | 597 | 5245 | 11.4% | 174 | 1386 | 12.6% | 771 | 6631 | 11.6% |
| Netherlands | 988 | 9815 | 10.1% | 502 | 2485 | 20.2% | 1490 | 12,302 | 12.1% |
| Sweden | 394 | 3665 | 10.8% | 177 | 962 | 18.4% | 571 | 4627 | 12.3% |
| Russia | 643 | 5944 | 10.8% | 273 | 1384 | 19.7% | 916 | 7328 | 12.5% |
| New Zealand | 205 | 1727 | 11.9% | 63 | 279 | 22.6% | 268 | 1995 | 13.4% |
| Israel | 520 | 4247 | 12.2% | 236 | 1309 | 18.0% | 756 | 5556 | 13.6% |
| Kuwait | 82 | 602 | 13.6% | 52 | 305 | 17.0% | 134 | 907 | 14.8% |
| Malaysia | 24 | 160 | 15.0% | 7 | 40 | 17.5% | 31 | 200 | 15.5% |
| United Kingdom | 690 | 5054 | 13.7% | 261 | 914 | 28.6% | 951 | 5969 | 15.9% |
| Canada—Ontario | 260 | 1764 | 14.7% | 69 | 284 | 24.3% | 329 | 2048 | 16.1% |
| Austria | 67 | 399 | 16.8% | 57 | 150 | 38.0% | 124 | 549 | 22.6% |
| Italy | 1700 | 9236 | 18.4% | 1400 | 3094 | 45.2% | 3100 | 12,330 | 25.1% |
| USA-Michigan | 2091 | 7711 | 76.5% | 641 | 1608 | 23.5% | 2732 | 9319 | 29.3% |
| United States of America | 36,896 | 131,228 | 28.1% | 11,022 | 25,101 | 43.9% | 47,918 | 156,329 | 30.7% |
| South Africa | 66 | 258 | 25.6% | 47 | 93 | 50.5% | 113 | 351 | 32.2% |
| Uzbekistan | 166 | 525 | 31.6% | 49 | 89 | 55.1% | 215 | 614 | 35.0% |
| South Korea | 315 | 947 | 33.3% | 141 | 329 | 42.9% | 456 | 1303 | 35.0% |
| China | NA | NA | NA | NA | NA | NA | 11,571 | 29,823 | 38.8% |
| Azerbaijan | 507 | 1104 | 45.9% | 57 | 87 | 65.5% | 564 | 1191 | 47.4% |
*NA, not available
Mortality Following MBS
The mortality rate following MBS is low in all 19 registries that report this variable. Mortality rates are lower for primary than revisional procedures (Table 8).
Table 8.
Mortality following MBS
| Country or region | Primary | Revisional | ||||||
|---|---|---|---|---|---|---|---|---|
| Deaths (n) | Total* (n) | Mortality rate | Known cases | Deaths (n) | Total* (n) | Mortality rate | Known cases | |
| Australia | 6 | 15,044 | 0.04% | 92.2% | 2 | 3703 | 0.05% | 94.6% |
| Austria | 0 | 1023 | 0.00% | 56.3% | 0 | 197 | 0.00% | 69.4% |
| Canada—Ontario | 0 | 2064 | 0.00% | 100.0% | 0 | 100 | 0.00% | 100.0% |
| China | 3 | NS | NS | NS | 3 | NS | NS | NS |
| France | 22 | 32,490 | 0.10% | 100.0% | 16 | 6400 | 0.30% | 100.0% |
| Iran | 9 | 6631 | 0.14% | 100.0% | 2 | 141 | 1.42% | 100.0% |
| Israel | 1 | 5556 | 0.02% | 100.0% | 2 | 1063 | 0.19% | 100.0% |
| Italy | 2 | 14,391 | 0.01% | 100.0% | 3 | 1499 | 0.20% | 100.0% |
| Malaysia | 0 | 200 | 0.00% | 100.0% | 0 | 1 | 0.00% | 100.0% |
| Netherlands | 4 | 12,327 | 0.03% | 100.0% | 3 | 1052 | 0.29% | 100.0% |
| New Zealand | 0 | 1881 | 0.00% | 93.4% | 0 | 88 | 0.00% | 93.6% |
| Norway | 0 | 1576 | 0.00% | 100.0% | 0 | 76 | 0.00% | 100.0% |
| Russia | 2 | 7345 | 0.03% | 100.0% | 1 | 315 | 0.32% | 100.0% |
| South Africa | 1 | 394 | 0.25% | 100.0% | 0 | 2 | 0.00% | 100.0% |
| South Korea | 0 | 1303 | 0.00% | 91.8% | 0 | 38 | 0.00% | 63.3% |
| Sweden | 0 | 4677 | 0.00% | 100.0% | 0 | 223 | 0.00% | 100.0% |
| United Kingdom | 2 | 2747 | 0.07% | 44.9% | 1 | 224 | 0.45% | 36.4% |
| United States of America | 149 | 204,175 | 0.07% | 99.9% | 59 | 5267 | 1.12% | 98.9% |
| USA Michigan | 2 | 9319 | 0.02% | 100.0% | 3 | 1201 | 0.25% | 100.0% |
total number of procedures with known death status
Mortality rate percentage of patients readmitted out of all procedures where death status is known
Known cases percentage of procedures where death status is known out of the total number of procedures. Excludes unknown/missing values
NS not stated
Discussion
These data are from the eighth report of the IFSO Global Registry [6]. All IFSO chapters are represented in this report, and 81.3% of known registries have included their data. As the data provided by each registry is already analyzed (aggregated), it is impossible to compare data between contributors statistically; however, trends are easily seen.
More women than men seek MBS in every contributing registry. In most countries, women undergoing MBS are younger than their male counterparts, with the exception of China, Kuwait, South Korea, Iran, Italy, and Malaysia. Women are also more likely to have a lower BMI than men.
While women are more likely to undergo MBS than men, men who undergo MBS are more likely to have diabetes. These data may suggest that the main driver for men seeking MBS is health concerns rather than weight loss alone. These sex-based differences are important considerations when designing patient-focused educational material and guidelines for MBS.
China (37.5 kg/m2) and South Korea (38.1 kg/m2) reported the lowest median BMI on the day of primary MBS. These countries also reported high rates of diabetes in their participants undergoing primary MBS, at 38% and 35%, respectively. Other countries that reported high rates of diabetes in their participants also reported higher BMI on the day of surgery (South Africa, Uzbekistan, USA, Michigan, and Ontario). This difference most likely reflects the increased risk of metabolic diseases in Asian populations at lower BMI [8].
Similar to previous IFSO Surveys [9], SG is the most popular primary MBS globally; however, these data are possibly skewed by the high proportion of primary participants from the USA. Of note, there are nine registries where RYGB, OAGB, or other procedures are reported more often as MBS primary procedures than SG. This is a change from previous reports [9] and is a trend away from SG as the preferred primary procedure that should be monitored.
Revisional surgery rates were the highest in Australia, France, and Israel. This may reflect the higher proportion of primary gastric bands and SG previously performed in these countries [9]. As the rates of primary gastric band procedures continue to fall globally, it will be interesting to see if the need for revisional surgery changes in these countries It will also be important to monitor if the rate of revisional is impacted by the introduction of effective pharmacotherapies [10].
Mortality following MBS was a rare event in all registries that measured this important metric, with rates ranging from 0 to 0.25% in the primary setting and 0–1.42% in the revisional setting, highlighting the safety of MBS.
The strength of this study was the number of included registries, the use of aggregated data that had already been cleaned and checked by contributing registries, and the representation of all IFSO Chapters. The limitations include the lack of clarity about case acquisition rates from most registries, inconsistencies in data definition, and missing data items from some registries.
Conclusions
This report highlights the opportunities that registries offer to make meaningful comparisons between countries on the demographics, characteristics, operation types and approaches, and trends in MBS procedure types. Reported outcomes can be seen as flags of potential issues or relationships that could be studied in more detail in specific research studies.
Acknowledgements
The IFSO Global Registry Committee would like to acknowledge all the contributors to the IFSO Global Registry, along with all their contributing patients who have gifted their data to their local registry to improve MBS. We also acknowledge the important work of Manuela Mozzarella, who helped contact all IFSO societies and encouraged participation in the Global Registry. Thanks also to the ANZ Bariatric Surgery Registry team, who collated the data from around the world, and Meaghan Thompson, who created the graphics for the eighth annual report.
IFSO Global Registry Collaboration
IFSO Global Registry Collaboration
| Country | Contributors |
| Australia | Angus Campbell, Jennifer Holland, Jenifer Cottrell, Robin Thompson, Dianne Brown, Wendy Brown, Ian Caterson |
| Austria | Felix Langer, Philipp Beckerhinn, Gehard Prager |
| Azerbaijan | Taryel Omerov |
| Brazil | Karina Otani, Ricardo Cohen |
| Canada—Ontario | Karen Barlow, Mehran Anvari |
| Chile | Camilo Boza, Amalia Villaseca |
| China | Cunchuan Wang, Wah Yang |
| France | Andrea Lazzati, David Lechaux, Valerie Leborgne, Francois Pattou |
| Iran | Mohammad Kermansaravi |
| Israel | Inbal Globus, Nasser Sakran |
| Italy | Mario Musella, Vincenzo Schiavone, Antonio Franzese |
| Korea | Sang Kuon Lee |
| Kuwait | Salman Al-Sabah |
| Malaysia | Nik Ritza Kosai Nik Mahmood, Guhan Muthkumaran, Ismail Ahmed Ali, Teh Shunxing, Nursuhadah Mohamed Yusof |
| Mexico | José G. Rodríguez Villarreal |
| Netherlands | Floris Bruinsma, Ronald Liem, Simon Nienhuijs, and Jan Willem Greve |
| Aotearoa New Zealand | Angus Campbell, Jennifer Holland, Jenifer Cottrell, Robin Thompson, Dianne Brown, Andrew MacCormick, Ian Caterson |
| Norway | Hannu Lyyjynen, Villy Vage |
| Russia | Bekkhan Khatsiev |
| South Africa | Eugene van Zyl, Tess van der Merwe |
| Sweden | Johan Ottoson |
| United Kingdom | Andrew Curry |
| United States of America | Benjamin Clapp, John Morton, Scott Shikora |
| USA- Michigan | Aaron J. Bonham, Amanda Stricklen, Rachel Ross, Amir Ghaferi |
| Uzbekistan | Nozim Jumaev |
| Venezuela | Pedro Monsalve, Luis Level |
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Declarations
Conflict of Interest
Wendy A. Brown reports Grants from Johnson and Johnson, Medtronic, GORE, Applied Medical, Novo Nordisk, NHMRC, and the Australian Commonwealth Government. Personal fees from Johnson and Johnson, GORE, Novo Nordisk, Pfizer, Medtronic, Lily, and Merck Sharpe and Dohme for lectures and advisory boards. Ricardo Cohen reports Research grant paid to their Institution from Johnson and Johnson and Medtronic; Advisory board for Morphic Medical, Baritek, and Medtronic; Speaker for Johnson and Johnson, Medtronic, and NovoNordisk. Francois Pattou reports a speaker honorarium from Medtronic, Ethicon, Lexington, Novo-Nordisk, and Lilly. Benjamin Clapp reports being a consultant for Medtronic; a travel stipend from Moon Surgical; food from Ethicon. Gerhard Prager reports speaker fees and educational grants from Metronic; educational grants from Novo Nordisk and Johnson and Johnson. Scott Shikora reports being the Editor in Chief of Obesity Surgery. All other authors declare no competing interests.
Footnotes
Key Points
• The most commonly performed primary metabolic bariatric procedure worldwide is sleeve gastrectomy.
• Roux-en-Y gastric bypass is the most commonly performed revisional metabolic bariatric surgical procedure.
• Asian countries report patient cohorts that have a lower BMI but higher rates of diabetes.
• Mortality is rare after metabolic bariatric surgery in all contributing countries.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Wendy A. Brown, Email: Wendy.Brown@monash.edu
on behalf of the IFSO Global Registry Collaboration:
Angus Campbell, Jennifer Holland, Jenifer Cottrell, Robin Thompson, Dianne Brown, Wendy Brown, Ian Caterson, Felix Langer, Philipp Beckerhinn, Gehard Prager, Taryel Omerov, Karina Otani, Ricardo Cohen, Karen Barlow, Mehran Anvari, Camilo Boza, Amalia Villaseca, Cunchuan Wang, Wah Yang, Andrea Lazzati, David Lechaux, Valerie Leborgne, Francois Pattou, Mohammad Kermansaravi, Inbal Globus, Nasser Sakran, Mario Musella, Vincenzo Schiavone, Antonio Franzese, Sang Kuon Lee, Salman Al-Sabah, Nik Ritza Kosai Nik Mahmood, Guhan Muthkumaran, Ismail Ahmed Ali, Teh Shunxing, Nursuhadah Mohamed Yusof, José G. Rodríguez Villarreal, Floris Bruinsma, Ronald Liem, Simon Nienhuijs, Jan Willem Greve, Angus Campbell, Jennifer Holland, Jenifer Cottrell, Robin Thompson, Dianne Brown, Andrew MacCormick, Ian Caterson, Hannu Lyyjynen, Villy Vage, Bekkhan Khatsiev, Eugene van Zyl, Tess van der Merwe, Johan Ottoson, Andrew Curry, Benjamin Clapp, John Morton, Aaron J. Bonham, Amanda Stricklen, Rachel Ross, Amir Ghaferi, Nozim Jumaev, Pedro Monsalve, and Luis Level
References
- 1.Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. 2020;324(9):879–887. doi: 10.1001/jama.2020.12567. [DOI] [PubMed] [Google Scholar]
- 2.Carlsson LMS, Sjöholm K, Jacobson P, et al. Life expectancy after bariatric surgery in the swedish obese subjects study. N Engl J Med. 2020;383(16):1535–1543. doi: 10.1056/NEJMoa2002449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sjostrom L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA. 2014;311(22):2297–2304. doi: 10.1001/jama.2014.5988. [DOI] [PubMed] [Google Scholar]
- 4.Gliklich RE, Dreyer NA, Leavy MB, editors. Registries for evaluating patient outcomes: a user's guide. 3rd ed. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014. [PubMed]
- 5.Brown WA, MacCormick AD, McNeil JJ, Caterson ID. Bariatric surgery registries: can they contribute to improved outcomes? Curr Obes Rep. 2017;6(4):414–419. doi: 10.1007/s13679-017-0286-3. [DOI] [PubMed] [Google Scholar]
- 6.IFSO Global Registry Eighth report. 2023. https://www.ifso.com/pdf/8th-ifso-registry-report-2023.pdf.
- 7.Coulman KD, Chalmers K, Blazeby J, et al. Development of a bariatric surgery core data set for an international registry. Obes Surg. 2023;33(5):1463–1475. doi: 10.1007/s11695-023-06545-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bansal M, Misra A. Cardiovascular disease and diabetes in South Asians: the twin epidemic. Curr Diabetes Rev. 2021;17(9):e122820189512. doi: 10.2174/1573399817666201228121145. [DOI] [PubMed] [Google Scholar]
- 9.Angrisani L, Santonicola A, Iovino P, Ramos A, Shikora S, Kow L. Bariatric surgery survey 2018: similarities and disparities among the 5 IFSO chapters. Obes Surg. 2021;31(5):1937–1948. doi: 10.1007/s11695-020-05207-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mok J, Adeleke MO, Brown A, Magee CG, Firman C, Makahamadze C, Jassil FC, Marvasti P, Carnemolla A, Devalia K, Fakih N, Elkalaawy M, Pucci A, Jenkinson A, Adamo M, Omar RZ, Batterham RL, Makaronidis J. Safety and efficacy of liraglutide, 3.0 mg, once daily vs placebo in patients with poor weight loss following metabolic surgery: The BARI-OPTIMISE randomized clinical trial. JAMA Surg. 2023;158(10):1003–11. 10.1001/jamasurg.2023.2930. [DOI] [PMC free article] [PubMed]