

Abstract
Intervention fidelity is an ongoing concern for rigorous research, from the initial stages of planning and study design to the maintenance of internal validity. An added concern is the balance between fidelity and design accommodation to better suit varied populations and individuals. In this article we describe our process for monitoring intervention fidelity during an individualized, yet standardized, strengths-based intervention with homeless youths in which we include periodic training of our professional intervention facilitators. In our ongoing study, which is based on a Solomon four-group design with repeated measures, monitoring and training are essential to ensure intervention fidelity. Despite a rich literature about intervention fidelity, little guidance is available to help researchers and practitioners implement fidelity strategies in the real world with vulnerable populations. This paper addresses this gap.
In 2000, Seligman and Csikszentmihalyi formally introduced positive psychology, with the intent of changing “the focus of psychology from preoccupation only with repairing the worst things in life to also building positive qualities” (p. 5). They added that this approach included subjective experiences of “well-being, contentment, and satisfaction (in the past); hope and optimism (for the future); and flow and happiness (in the present” (p. 5). Another similar strengths-based approach, positive youth development, represents an attempt to provide all youth, regardless of the challenges they face, with the resources, opportunities, and relationships they need to thrive during adolescence and to grow in to healthy, prosocial, competent adults (Bernat & Resnick, 2006). These moves away from a traditional deficit-focused approach to reduce health-risk behaviors view youth as a “resource to be developed, not problems to be solved,” (Resnick, 2008, p. 144) working to cultivate internal and external resources such as competence, character, confidence, caring, and connection (Lerner, Almerigi, Theokas, & Lerner, 2005; McLaughlin, Irby, & Langman, 1994). Thus positive psychology and positive youth development have been applied to help youths who use substances (Bonell et al., 2016) and young men who have sex with men who engage in risky sexual behaviors (Martin, Benotsch, Cejka, & Luckman, 2014). In addition, studies based on principles and strategies of positive psychology and positive youth development provide evidence that supportive relationships, resources, and opportunities help to reduce health-risk behaviors in youths, including youths in populations traditionally characterized by risk, such as the homeless (Dang, 2014; Dang & Miller, 2013).
Our team recently developed an intervention study of a brief group intervention focused on optimism, hope, resilience, and social connectedness as predictors of self-efficacy for safe sex and alcohol refusal in homeless young women, in which we found promising results (Rew, Powell, Brown, Becker, & Slesnick, 2017). Those who received the intervention showed significant improvements in hope (p = .017), resilience (p = .005), self-efficacy to refuse alcohol (p = .004), social connectedness (p = .003), and reduced alcohol use (p = .038) four weeks after the intervention. Moreover, participants were very satisfied with the positive strengths-based focus of the intervention. Armed with these results and a further refined intervention, we then began a four-year multi-site, longitudinal intervention study of both male and female homeless youths based on principles of positive psychology, positive youth development, and motivational interviewing (Miller & Rollnick, 2013). Motivational interviewing was included in the intervention as a third strengths-based approach because it provides a way to talk positively with youths about the possibility of change while affirming each individual’s worth rather than focusing on his or her problems or deficits. The revised intervention, described in greater detail below, consists of six 30-minute modules delivered on a one-to-one basis.
Purpose
For the successful implementation and analysis of such intervention research, maintaining and evaluating intervention fidelity is crucial. The National Institutes of Health’s Behavior Change Consortium (BCC) has identified five components that contribute to intervention fidelity: (1) study design, (2) provider or facilitator training, (3) treatment or intervention delivery, (4) treatment or intervention receipt, and (5) enactment of treatment or intervention skills (Bellg et al., 2004, p. 445). But unique challenges to intervention fidelity occur when one works with vulnerable populations such as homeless youths. In our study with homeless youths, aged 18–23 years, the training of the intervention facilitators and the fidelity of the facilitators’ delivery of the intervention have been especially important. In this article, we illustrate all five components of intervention fidelity, but with a primary focus on the training of our professional intervention facilitators and on the facilitators’ adherence to the content of the intervention as they deliver it to individual homeless youths. Establishing procedures to ensure treatment fidelity is essential for increasing the internal validity of efficacy studies and for guiding implementation of the intervention developed in the laboratory to the practice field (Naleppa & Cagle, 2010). That is, clearly established protocols can assist in the training and supervision processes of practitioners to ensure that evidence-based treatments are delivered as intended.
Fidelity is an essential concept that enables researchers to measure the reliability and validity of behavioral interventions (Bellg et al., 2004). The terms treatment fidelity (Bellg et al., 2004; O’Shea, McCormick, Bradley, & O’Neill, 2016), implementation fidelity, (Masterston-Algar, Burton, Rycroft-Malone, Sackley, & Walker, 2014; Pérez, Van der Stuyft, Zabala, Castro, & Lefèvre, 2016), and intervention fidelity (Dyas, Togher, & Siriwardena, 2014; Faulkner, 2012) have been used interchangeably to address one or more critical components of intervention studies. In this paper, we use intervention fidelity-- “the extent to which an intervention’s core components have been implemented (and differentiated from control conditions) as planned” (Nelson, Cordray, Hulleman, Darrow, & Sommer, 2012, p. 377).
Methods
Study Design
An intervention’s efficacy and effectiveness depend on its fidelity, and examination of an intervention’s fidelity begins with its design. The design must be guided by one or more behavior change theories (Beck et al., 2015). Therefore, in preparation for our intervention, we reviewed and synthesized literature on the positive psychology paradigm (Seligman & Csikszentmihalyi, 2000; Shogren, Lopez, Wehmeyer, Little, & Pressgrove, 2006), positive youth development (Benson & Saito, 2001), psychological capital (Avey, Luthans, Smith, & Palmer, 2010; Luthans, Avolio, Avey, & Norman, 2007), the possible selves model (Markus & Nurius, 1986), and principles of motivational interviewing (Miller & Rollnick, 2013) in addition to intervention literature pertaining to homeless youths (e.g., Tucker et al., 2012). This review and synthesis indicated how concepts from these theories and approaches could guide the development of specific interventions to address the health-risk behaviors that place homeless youths at greatest risk for adverse health outcomes. Figure 1 depicts the resulting conceptual and research model that provided the framework for our study.
Figure 1.
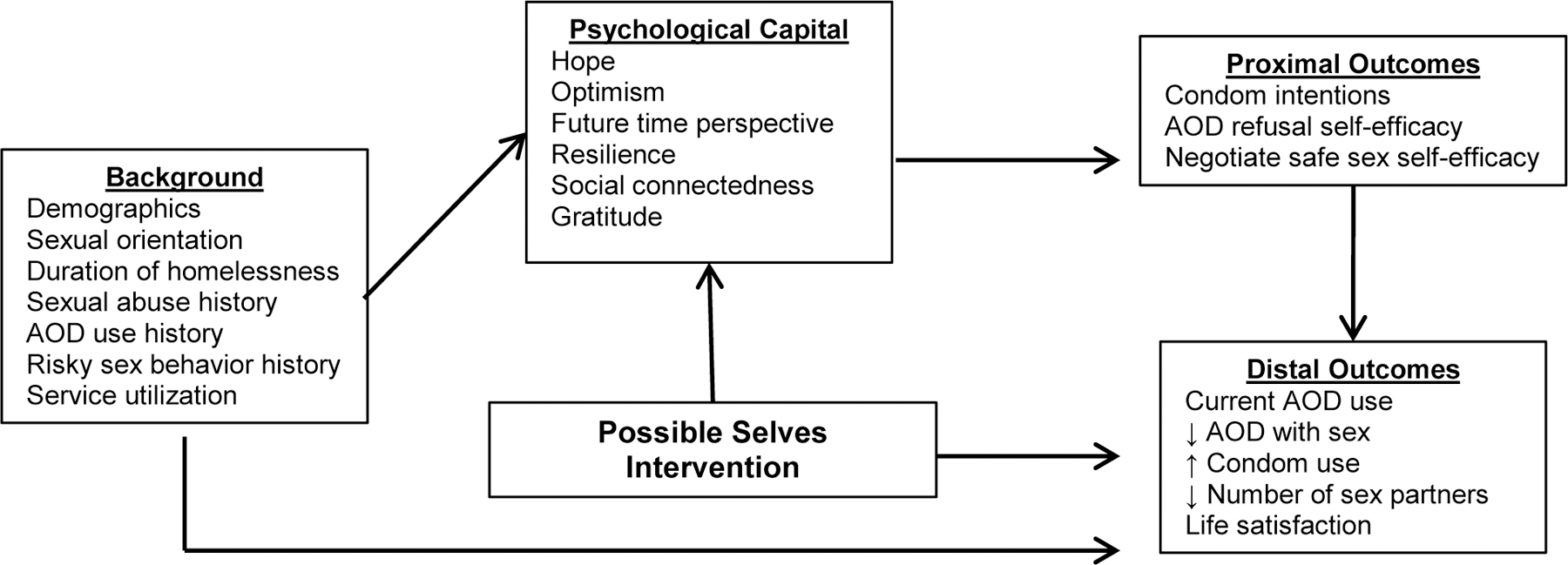
Conceptual and Research Model for Possible Selves Intervention for Homeless Youths
Legend: OD = alcohol and other drug use
The conceptual and research model in Figure 1 presents specific variables that positive psychology suggests motivate behavior: the variables of hope, optimism, future time perspective, resilience, social connectedness, and gratitude constitute psychological capital (Luthans et al., 2007). These concepts or variables guide the content of our intervention and the protocol of our research design. The background variables (e.g., demographics, sexual orientation, duration of homelessness, etc.) provide the context and culture of the population that we are seeking to serve and the organizations in which we are delivering the intervention. The proximal and distal outcomes, as depicted in the model, are important aspects of the intervention because alcohol use, drug use, and risky sexual behaviors are quintessential characteristics of homeless youths and are costly to society. Engagement in these health-risk behaviors robs youths of unmet potential and substantially increases their need for health care and social services (Hwang, Weaver, Aubry, & Hoch, 2011; Turnbull, Muckle, & Masters, 2007).
Despite having a clearly depicted conceptual and research model to guide an intervention study, one must recognize and control a number of extraneous variables that can threaten the fidelity of such a study. Among those extraneous variables are such things as how compatible the intervention is with a provider’s beliefs about behavior change, how well the intervention provider buys into the aims and approaches of the intervention, how the intervention providers are trained, and whether or not they are monitored and supported on a daily basis (Anyon, Nicotera, & Veeh, 2016). At the onset of an intervention study, the investigators must have a clear idea of what competencies are needed in an intervention facilitator and must be committed to hiring those individuals who have such competencies and who will buy into the study’s conceptual or theoretical foundation of the study (Borrelli et al., 2005). In our study, for example, one essential competency is that an intervention facilitator must be able to demonstrate to a youth how to correctly apply and remove both male and female condoms. Thus our protocol, might best be addressed by graduate students in health professions such as nursing, psychology, or social work. Other critical competencies are that facilitators must not be judgmental and must be able to listen carefully to verbal and non-verbal communication from the homeless youth participants.
Overview of the Intervention
Our intervention study is a tailored, motivational and educational series of six one-on-one, face-to-face meetings designed to strengthen homeless youths’ psychological capital and reinforce skills to resist alcohol and drug misuse and risky or unsafe sexual behaviors. The intervention manual consists of a detailed description of the homeless youth population for whom the intervention is designed as well as a description of the information to be shared with the participant and the materials needed to enhance this presentation. Because this intervention was developed specifically for a vulnerable population of youths, it is essential that those providing the intervention closely follow the principles of motivational interviewing [MI] (i.e., that such an intervention is person-centered, that it is done with a participant and not on or to them), the GRA intends to build a partnership with the homeless youth, supporting his or her autonomy and evoking what is within the youth (Miller & Rollnick, 2013).
The Possible Selves Intervention (PSI) is grounded in accepting and supporting the participant while evoking the motivation to generate images of one’s best possible self (Markus & Nurius, 1986). The PSI includes opportunities for self-reflection and focuses on ambivalence within the participant about reaching personal goals while living in an environment where alcohol and drug (AOD) use and risky sex present daily challenges. The focus of the intervention is not on external events but on creative thinking about oneself and one’s identity (a critical developmental task throughout adolescence). The six modules of the PSI are filled with colorful and provocative images that were selected to evoke self-reflection. These modules encourage the participant to build skills in (a) communication (i.e., using assertive messages, negotiating for safer sex, and resisting AOD use/abuse), (b) correct application, removal, and disposal of male and female condoms, and (c) goal-setting for reduced AOD use, and practicing safer sex. Assessments are also made with the participant throughout the six sessions of their personal structural and behavioral barriers to setting goals of reducing or avoiding AOD use and practicing safer sex. Such barriers might include external triggers for AOD use such as associating with others who are engaging in health-risk behaviors and internal triggers for risky sexual behavior such as feeling angry or lonely. Each participant is given a small notebook in which to take notes to keep as reminders of their self-determined goals and strategies for meeting them.
To test the effectiveness of this intervention with homeless youths who are aged 18 – 23 years, we are using a rigorous modification of the standard Solomon four-group design (Campbell & Stanley, 1963; McGahee & Tinge, 2009) with repeated measures. After the initial posttest for each group, subsequent posttests occur at 3 and 6 months (12 and 24 weeks) after the intervention. With this design, we can test the main effects of the intervention plus main effects of pre-testing. Figure 2 presents the four-group design and testing pattern. Hypotheses to be tested include (O2 > O1), (O2 > O6), (O10 > O7), and (O10 > O13). As can be seen in Figure 2, to measure both proximal and distal outcomes associated with the intervention, participants will complete follow-up measures at 3 and 6 months following the last session of the intervention. The distal outcomes for Group 4 (see figure) are also measured 3 and 6 months after the first measurement (O13 O14).
Figure 2.
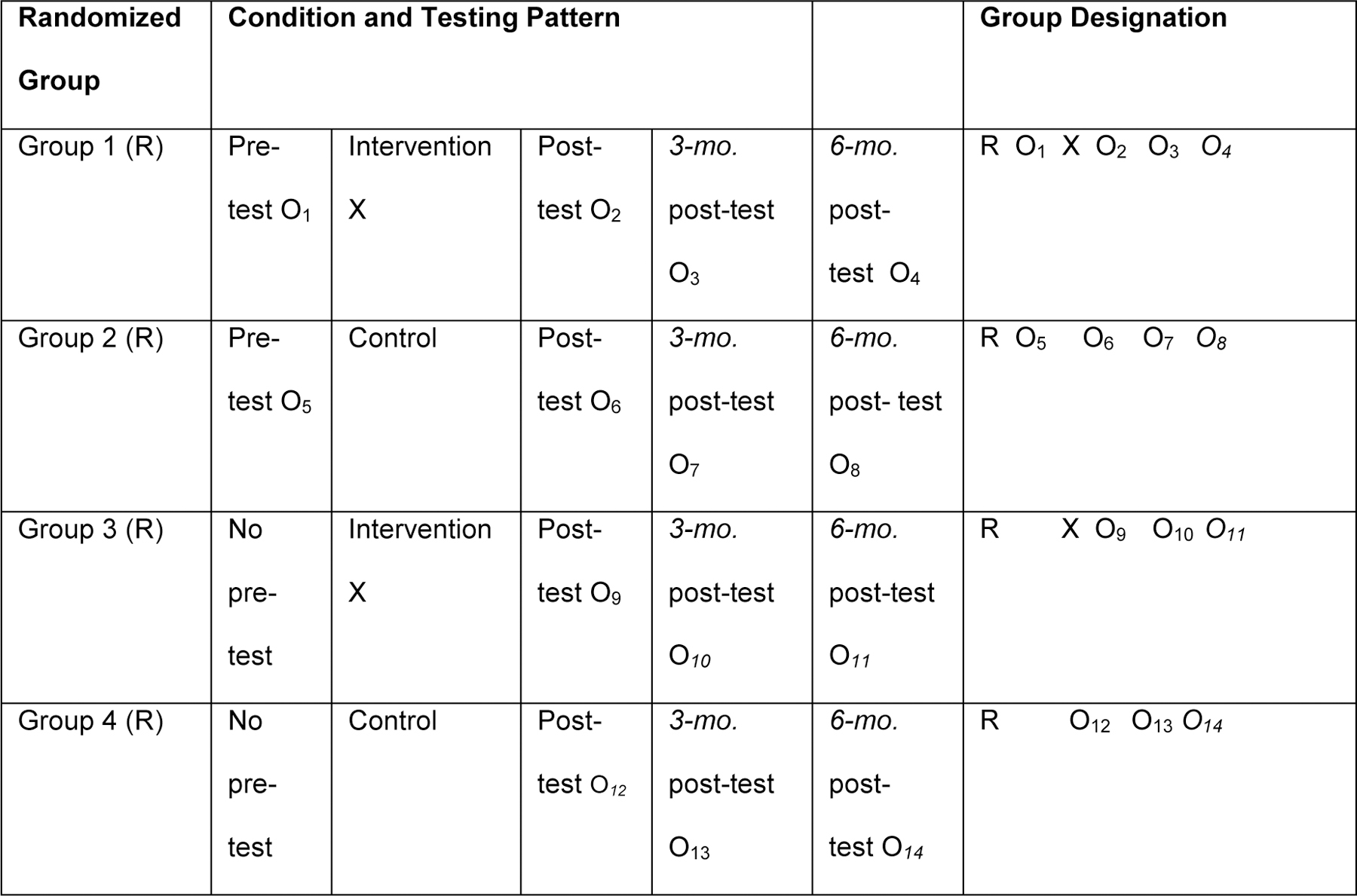
Solomon Four-Group Design for Possible Selves Intervention for Homeless Youths
R = randomized; X = intervention condition; O = observation; measurement of variables
Settings for this intervention study are two drop-in centers, 1,000 miles apart, where homeless youths can obtain health and social services including food, clothing, respite from inclement weather, and information about community-based services available in the respective cities of Austin, Texas and Columbus, Ohio. The two sites have similar purposes and provide many of the same services, but they also have distinct differences, which include the number of hours of operation. The Texas site is open only a few hours each day, 3 days each week; the Ohio site is open 24 hours per day, 7 days per week. Thus, variables inherent in these different environments could influence the outcomes and they must be carefully controlled in data analysis.
Intervention Facilitator Training
Intervention fidelity depends not only on intervention design, but on how intervention facilitators are trained, monitored, and supported. Borrelli et al. (2005) note that the training component of fidelity showed the lowest adherence (22%) across public health studies (N = 292). Specificity of training methods is needed for study replication and increases confidence that study results are due to the intervention and not to provider skills and drift over time. At both sites, the intervention is delivered by graduate research assistants (GRAs) with a background in nursing, psychology, or social work. According to Beck et al. (2015), the training of intervention providers should be standardized. The GRAs are trained by the research team to deliver the intervention, but they are also instrumental in recruiting participants and collecting research data at both sites. The initial groups of GRAs were trained at their respective sites by one of the two multiple principal investigators (MPI) over a 3-day period. This training consisted of issuing a training manual to the GRAs, discussing the philosophical and conceptual bases of the intervention, viewing video-tapes of the intervention being delivered, and role-playing to practice each of the modules. As GRAs are students who graduate from the university and move on, new GRAs are hired and trained with a combination of the original methods and close apprenticeship in the field with an experienced interventionist. It is imperative that the GRAs follow the study protocols, as outlined in the intervention manual, to ensure fidelity on a daily basis. GRAs work in pairs when recruiting new study participants so that one can recruit and administer a pre-test, if indicated, and the other can deliver the intervention. Potential participants must be randomized to one of the four groups of the Solomon 4-Group design. A computer program randomly assigns participants in chronological order at each site as they enroll in the study; the chart in Figure 3, which enables strict adherence to the protocol, illustrates this process. Using the chart, GRAs record their initials and the date of each intervention module as it is delivered and they track all pre- and posttesting in the same way.
Figure 3.
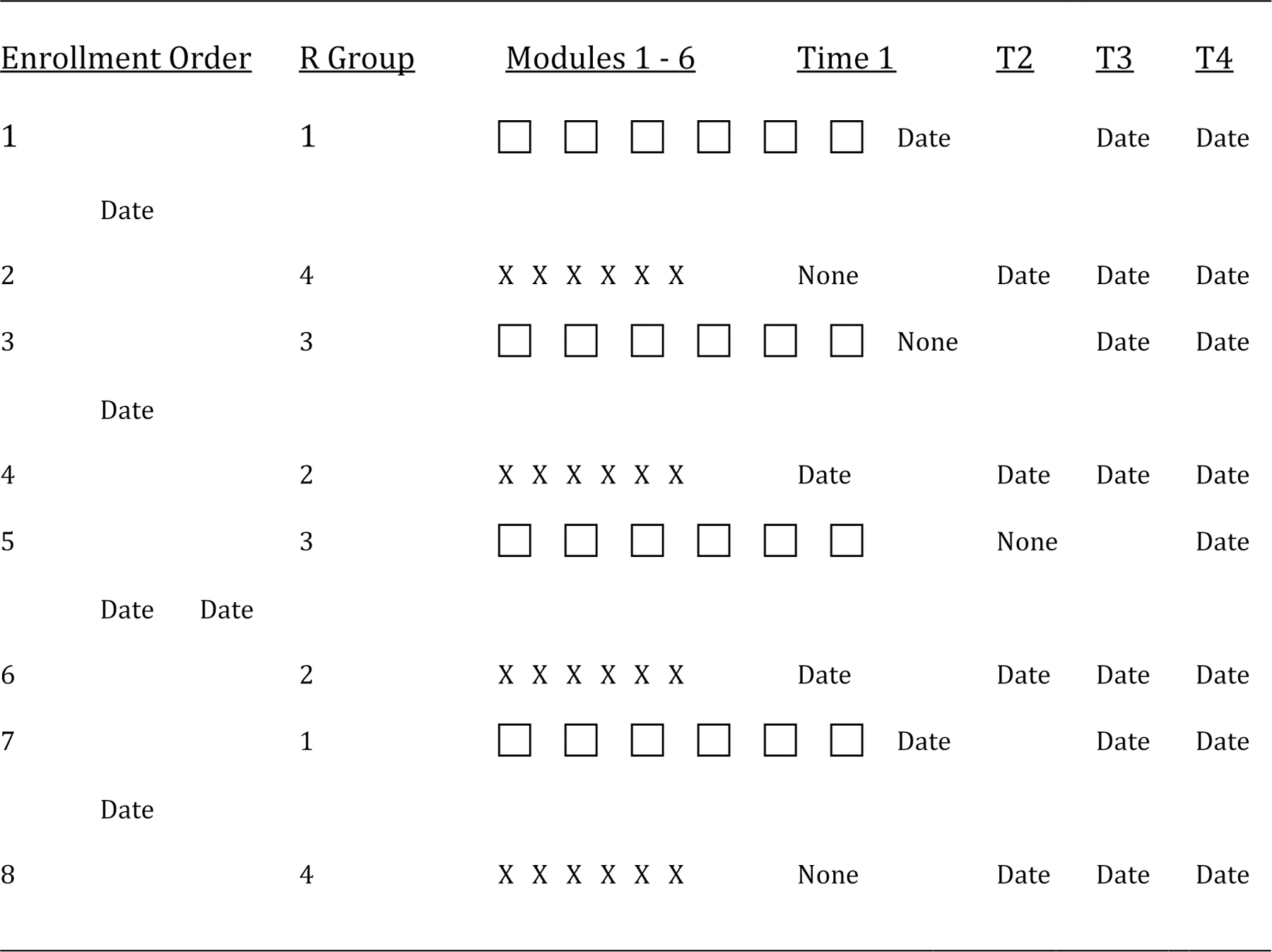
Randomization of Participants to Solomon Four-Groups in Possible Selves Intervention for Homeless Youths
Note: R Group = randomized groups (Groups 1 + 2 complete pretest; 3 + 4 do not complete pretest; 1 + 3 receive intervention; 2 + 4 receive services as usual); □ = received intervention sessions; X = received services as usual). Time 1 = pre-test; T2 = first post-test; T3 = 3-month post-test; T4 = 96-month post-test.
Routine fidelity checks must be made throughout the study, not just at the outset (Dumas, Lynch, Laughlin, Smith, & Prinz, 2001; Faulkner, 2012; Horner, Rew, & Torres, 2006). Such ongoing assessment is especially important for behavioral interventions because, unlike a static instrument, the human element of administration during the study can introduce a host of confounders. Facilitators can differ in skill, experience, motivation, and consistency, and fluctuations can result from staff turnover during the ongoing study (Faulkner, 2012; Horner et al., 2006). Because the GRAs are hired from two distinctly different pools of graduate students in different geographic locations, such potential confounding variables may be particularly evident and must be recognized, and controlled during data analysis.
With the study participants’ permission, all interventionists audio-taped their intervention sessions, which they then reviewed using an intervention fidelity checklist. This checklist was developed by one of the investigators for use in two previous intervention studies and adapted for this study. The checklist follows the content of each intervention session in detail and may also be used as an outline when delivering the content of each session. This checklist was particularly useful when a facilitator was just beginning to work on the project and could benefit from feedback, as well as when new GRAs subsequently joined the project and were trained. The checklist showed the content to be covered in each of the six sessions and included a space for indicating the amount of time the facilitator spent on each component of the specific session. Along with the tape-recording of each session, the checklist provided useful feedback about addressing the content and managing the time allowed for the session. Figure 4 presents a checklist from the second session, or Module 2, which was used to train the facilitators and to monitor their intervention delivery.
Figure 4.
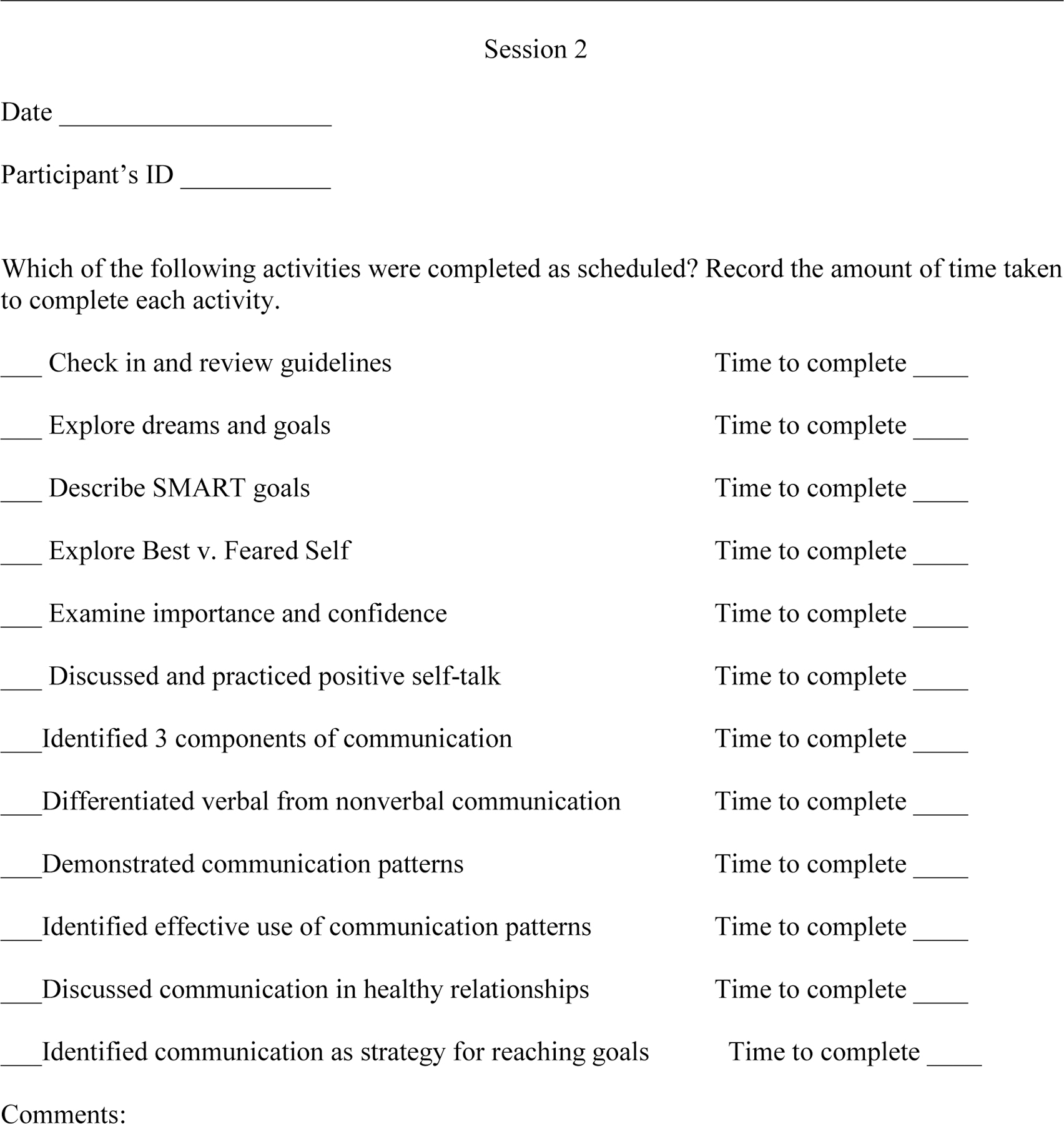
Sample Checklist for Intervention Fidelity in Possible Selves Intervention for Homeless Youths
These session checklists are reviewed by one of the MPIs and/or the site project coordinator at regular intervals to ascertain that the content and process of the intervention are followed closely. These reviews also are useful in identifying when a GRA may be deviating from the intervention protocol. When such deviation occurs, the MPI then schedules additional training with the GRA to ensure fidelity of the intervention. For example, on one occasion, a GRA did not follow the protocol as outlined on the checklist because she was in a hurry to finish the session and attend to some personal business. This was captured in the audio-tape and the documentation of amount of time spent on each component of that particular session. The GRA was then counseled and reminded of the importance of providing the full amount of time needed on each component of the intervention. The GRA then completed a role-playing session with the MPI and committed to following the protocol exactly, putting her personal agenda aside.
Intervention Delivery
Several strategies can be used to ensure the fidelity of intervention delivery. Intervention facilitators may (a) use an intervention manual or script, (b) complete video- or audio-tapes of the intervention, and (c) meet regularly with principal investigators to review all aspects of the study that pertain to them. In a brief, but complex intervention, such as the one described here, it is necessary to follow a script or use an intervention manual to ensure that all participants in the intervention groups receive the same information and practice the same skills. In this study, the content is presented as a series of images and words that facilitators present to participants using PowerPoint on a laptop computer. These images are meant to evoke positive feelings and memories in the participant and, when accompanied by a discussion with an intervention facilitator, result in a personalized experience that we hope will motivate the participant to engage in behaviors that lead to positive health outcomes. As stated above, with permission from each participant, the facilitators also audio-taped each session of the intervention. These audio-tapes are then reviewed by the principal investigators and other members of the research team for continuous quality improvement.
Regular team meetings are held at both sites to review the procedures for recruiting and retaining youths in the study as well as to address other issues related to delivery of the intervention. Recruitment for the study is guided by the randomization chart shown in Figure 3. When participants are recruited, for example, if intervention facilitators are “tempted” to assign a participant volunteer to a particular condition because the individual wishes to be in the intervention rather than the control group, we remind them of the study design and reiterate the rationale that guides it. Such circumstances may arise when potential participants are friends with other youths receiving services from the same provider. When the homeless youths hear about the study, they may approach the staff in pairs or small groups and request that they be enrolled in the same arm of the study. GRAs then must explain the concept of random assignment. They emphasize that the order of enrollment is pre-determined and they are not at liberty to alter that. The importance of this approach is frequently reinforced in team meetings.
After providing the intervention for at least 6 months, we asked GRAs from both sites to respond anonymously to several open-ended questions about how well they think they have maintained intervention fidelity throughout the study. We were granted approval from our institutional review board to obtain, analyze, and report these data here. The GRAs all gave informed consent. Each of them identified the fidelity checklist as a helpful tool. In response to a question about what structural factors facilitated maintaining intervention fidelity, one of the GRAs (intervention facilitators) answered, “Having the fidelity checklist visible during the intervention when I was less experienced.” When asked to comment freely on any aspect of delivery of the intervention, another GRA wrote, “Once you are provided with the theoretical background of the techniques utilized in the modules, you are better able to understand where the individual slides fit in the grand scheme of the intervention. Therefore you are able to link information from one module to the next, which provides more continuity and natural flow to the modules.” This comment underscores the salience of having a strong conceptual framework for such an intervention study.
Intervention Receipt
Receipt of an intervention focuses on the assessment of the participant’s comprehension of the intervention and ability to perform intervention skills (Borrelli et al., 2005). In our brief intervention, facilitators engage the homeless youths in ongoing conversations throughout the six sessions. The purpose of these conversations is to determine that each youth understands the information being presented in the PowerPoint images. This also allows facilitators to ascertain that the youth receives the intervention as it is intended. For example, in the first session, the facilitator shows a slide that presents the following four simple guidelines for the interaction between facilitator and participant: (1) the conversations will be confidential, (2) the conversations will not be about people who are not there, (3) all questions are good, and (4) each session will start and stop on time. These guidelines are accompanied by the image of a stop watch. Before proceeding, the facilitator checks to make sure the participant understands and agrees to follow these guidelines. At the beginning of the second session, the facilitator checks with the participant to be sure s/he remembers these guidelines for their interactions.
Many homeless youths experience substance use and if a facilitator believes that there is evidence that a participant is “impaired” by such use at the time they are scheduled to receive one of the intervention modules, the facilitator is encouraged to reschedule the meeting. If the participant disagrees with the facilitator’s suggestion to reschedule the meeting, the GRA may continue with the session to maintain the trust of the participant. If necessary, an additional session may then be scheduled to reinforce what the participant missed because of his/her temporary impairment. This enhances this component of intervention fidelity; it might otherwise be impossible to determine whether the youth has understood the material presented.
Throughout the study, the GRAs document each time they interact with a participant. They provide the date and their initials for each data collection session and for each of the modules presented.
Enactment of Specific Skills
The final component in the evaluation of intervention fidelity is the participant’s enactment or performance of specific intervention skills. To a limited extent, this can be observed during the study, but in our example, it ultimately depends on the findings from our analysis at the conclusion of the study. Enactment can also be assessed throughout the intervention period using role-play. For example, role-play provides feedback to the intervention facilitator regarding the participant’s success in applying assertive communication skills and can be useful in identifying those skills that need more reinforcement. One example from our study can illustrate the enactment of specific intervention skills. In the fifth session, participants are shown how to apply and remove both male and female condoms using an anatomically correct plastic model. The facilitator then asks the participant to demonstrate how to apply and remove these condoms correctly, and the skill is practiced until the participant correctly enacts each step. The facilitator provides the rationale for each step and ends the session by helping the youth relate this skill to being one’s best possible self.
The final test of the fidelity of the intervention occurs at the conclusion of the study, when we analyze the 6-month follow-up data from participants and determine whether there are statistically significant differences between those who received the intervention and those who did not. This will also determine the final effectiveness of the intervention. This fidelity component can also be tested before the conclusion of the study by determining whether there is a statistically significant difference between those who completed the pretest and the first posttest on the specific health-related skills related to alcohol refusal self-efficacy and safer sex self-efficacy.
Discussion
Assurance of fidelity often predicts treatment outcomes and can increase statistical power by reducing unintended variability (Borrelli et al., 2005). Specification of procedures to enhance fidelity can increase external validity as well by easing treatment replication and training across multiple sites. This is especially important when interventions are implemented in real world settings, and with complicated interventions or study designs (Garbacz, Brown, Spee, Polo, & Budd, 2014). Unfortunately, little guidance is available to researchers and practitioners on how to implement fidelity strategies. The current study addresses this gap.
The use of various strategies to ensure fidelity is likely the result of a broadening of the concept over the past 20 years (Borrelli et al., 2005). The model employed in the current study, developed by the NIH Behavioral Change Consortium (BCC), offers a comprehensive five-part framework that includes study design, training, delivery and receipt of the intervention, as well as enactment of intervention skills. A comprehensive review of the literature by Borelli and colleagues (2005) indicated that only 6.5% of health behavior studies showed 80% adherence, calculated as the number of strategies used to ensure fidelity divided by the number of strategies applicable to the study design. Further, only 27% of studies assessed whether the intervention was delivered as intended. In this study, the application of the BCC model was presented along with our practical application of strategies to enhance fidelity. This information may be useful to others who work with homeless youths or other high-risk, vulnerable young people to increase fidelity and, therefore, the internal and external validity of study findings, including ultimate dissemination of efficacious interventions.
This paper is limited by its presentation of a detailed description of how intervention fidelity was incorporated in a single study. It is further limited by the fact that enactment of the skills addressed in the intervention have not yet been fully analyzed owing to the longitudinal nature of the ongoing study. Return demonstration and role-playing some skills serve as proxies for behaviors that we hope the recipients will enact in the real world.
Intervention fidelity demands attention from conceptualization to completion of an intervention study. With a vulnerable population and a complex randomized Solomon four-group design delivered in two distinct geographic areas, we face multiple challenges. Careful adherence to our conceptual and research model, selecting intervention facilitators with specific communication skills, following strict randomization procedures, ongoing training and monitoring of intervention facilitators, and statistical analysis of changes in skills among those who received the intervention will enhance our confidence in the reliability and validity of this intervention.
Acknowledgement:
This paper was supported by a grant awarded to the first author from the National Institute of Child Health and Human Development/National Institutes of Health [R01 HD083576]. Editorial support with manuscript development was provided by the Cain Center for Nursing Research and the Center for Transdisciplinary Collaborative Research in Self-management Science (P30 NR015335) at The University of Texas at Austin School of Nursing.
References
- Anyon Y, Nicotera N, & Veeh CA (2016). Contextual influences on the implementation of a schoolwide intervention to promote students’ social, emotional, and academic learning. Children & Schools, 38(2), 81–88. [Google Scholar]
- Avey JB, Luthans F, Smith RM, & Palmer NF (2010). Impact of positive psychological capital on employee well-being over time. Journal of Occupational Health Psychology, 15, 17–28. [DOI] [PubMed] [Google Scholar]
- Beck AK, Baker A, Britton B, Wratten C, Bauer J, … Carter G (2015). Fidelity considerations in translational research: Eating As Treatment—a stepped wedge, randomized controlled trial of a dietitian delivered behaviour change counselling intervention for head and neck cancer patients undergoing radiotherapy. Trials, 16, 465 doi: 10.1186/s13063-015-0978-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bellg AJ, Borrelli B, Resnick B, Hecht J, Minicucci DS, Ory M, … Czajkowski S (2004). Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychology, 23, 443–451. doi: 10.1037/0278-6133.23.5.443 [DOI] [PubMed] [Google Scholar]
- Benson PL, & Saito RN (2001). The scientific foundations of youth development. In Benon PL, & Pittman KJ (Eds.). Trends in youth development: Visions, realities, and challenges (pp. 135–154). Boston, MA: Kluwer Academic. [Google Scholar]
- Bernat DH, & Resnick MD (2006). Healthy youth development: Science and strategies. Journal of Public Health Management Practice, Nov(Suppl.), S10–S16. [DOI] [PubMed] [Google Scholar]
- Bonell C, Hinds K, Dickson K, Thomas J, Fletcher A, Murphy S, … Campbell R (2016). What is positive youth development and how might it reduce substance use and violence? A systematic review and synthesis of theoretical literature. BMC Public Health, 16, 135. doi: 10.1186/s12889-016-2817-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borrelli B, Sepinwall D, Ernest D, Bellg AJ, Czajkowski S, Breger R, … Orwig D (2005). A new tool to assess treatment fidelity and evaluation of treatment fidelity across 10 years of health behavior research. Journal of Consulting and Clinical Psychology, 73, 852–860. doi: 10.1037/0022-006X.73.5.852 [DOI] [PubMed] [Google Scholar]
- Campbell DT, & Stanley JC (1963). Experimental and quasi-experimental designs for research. Boston, MA: Houghton Mifflin Company. [Google Scholar]
- Dang MT (2014). Social connectedness and self-esteem: Predictors of resilience in mental health among maltreated homeless youth. Issues in Mental Health Nursing, 35, 212–219. doi: 10.3109/01612840.2013.860647 [DOI] [PubMed] [Google Scholar]
- Dang MT, & Miller E (2013). Characteristics of natural mentoring relationships from the perspectives of homeless youth. Journal of Child and Adolescent Psychiatric Nursing, 26, 246–253. doi: 10.1111/jcap.12038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dumas JE, Lynch AM, Laughlin JE, Smith EP, & Prinz RJ (2001). Promoting intervention fidelity conceptual issues, methods, and preliminary results from the EARLY ALLIANCE prevention trial. American Journal of Preventive Medicine, 20, 38– 47. [DOI] [PubMed] [Google Scholar]
- Dyas JV, Togher F, & Siriwardena AN (2014). Intervention fidelity in primary care complex intervention trials: Qualitative study using telephone interviews of patients and practitioners. Quality in Primary Care, 22, 25–34. [PubMed] [Google Scholar]
- Faulkner MS (2012). Intervention fidelity: Ensuring application to practice of youth and families. Journal for Specialists in Pediatric Nursing, 17, 33–40. doi: 10.111/j.1744-6155.2011.00305.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garbacz L, Brown DM, Spee GA, Polo AJ, & Budd KS (2014). Establishing treatment fidelity in evidence-based parent training programs for externalizing disorders in children and adolescents. Clinical Child Family Psychology Review, 17, 230–247. [DOI] [PubMed] [Google Scholar]
- Horner S, Rew L, & Torres R (2006). Enhancing intervention fidelity: A means of strengthening study impact. Journal for Specialists in Pediatric Nursing, 11, 80–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hwang SW, Weaver J, Aubry T, & Hoch JS (2011). Hospital costs and length of stay among homeless patients admitted to medical, surgical, and psychiatric services. Medical Care, 49, 350–354. [DOI] [PubMed] [Google Scholar]
- Lerner RM, Almerigi JB, Theokas C, & Lerner JV (2005). Positive youth development: A view of the issues. Journal of Early Adolescence, 25(1), 10–16. doi:0.1177/0272431604273211 [Google Scholar]
- Luthans F, Avolio BJ, Avey JB, & Norman SM (2007). Positive psychological capital: Measurement and relationship with performance and satisfaction. Personnel Psychology, 60, 541–572. [Google Scholar]
- Markus H, & Nurius P (1986). Possible selves. American Psychologist, 41, 954–969. [Google Scholar]
- Masterson-Algar P, Burton CR, Rycroft-Malone J, Sackley CM, & Walker MF (2014). Towards a programme theory for fidelity in the evaluation of complex interventions. Journal of Evaluation in Clinical Practice, 20, 445–452. doi: 10.1111/jep.12174 [DOI] [PubMed] [Google Scholar]
- McGahee TW, & Tinge MS (2009). The use of the Solomon four-group design in nursing research. Southern Nursing Online Journal of Nursing Research, 9(1). Available at http://www.resourcenter.net/images/snrs/files/sojnr_articles2/Vol09Num01Art14.pdf [Google Scholar]
- McLaughlin MW, Irby MA, & Langman J (1994). Urban sanctuaries: Neighborhood organizations in the lives and futures of inner-city youth. San Francisco, CA: Wiley. [Google Scholar]
- Miller WR, & Rollnick S (2013). Motivational interviewing (3rd ed.). New York. NY: The Guilford Press. [Google Scholar]
- Naleppa MJ, & Cagle JG (2010). Treatment fidelity in social work intervention research: A review of published studies. Research on Social Work Process, 20, 674–681. [Google Scholar]
- Nelson MC, Cordray DS, Hulleman CS, Darrow CL, & Sommer EC (2012). A procedure for assessing intervention fidelity in experiments testing educational and behavioral interventions. The Journal of Behavioral Health Services & Research, 39, 374–396. doi: 10.1007/s11414-012-9295-x [DOI] [PubMed] [Google Scholar]
- O’Shea O, McCormick R, Bradley JM, & O’Neill B (2016). Fidelity review: A scoping review of the methods used to evaluate treatment fidelity in behavioural change interventions. Physical Therapy Reviews, 21, 207–214. doi: 10.1080/10833196.2016.1261237 [DOI] [Google Scholar]
- Pérez D, Van der Stuyft P, Zabala MC, Castro M, & Lefèvre P (2016). A modified theoretical framework to assess implementation fidelity of adaptive public health interventions. Implementation Science, 11, 91. doi: 10.1186/s13012-016-0457-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Resnick MD (2008). Best bets for improving the odds for optimum youth development. In Kline KK (Ed.). Authoritative Communities: The scientific case for nurturing the whole child (pp. 137–150). New York, NY: Springer. [Google Scholar]
- Rew L, Powell T, Brown A, Becker H, & Slesnick N (2017). An intervention to enhance psychological capital and health outcomes in homeless female youths. Western Journal of Nursing Research, 39, 356–373. doi: 10.1177/0193945916658861 [DOI] [PubMed] [Google Scholar]
- Seligman MEP, & Csikszentmihalyi M (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5–14. doi: 10.1037//0003-066X55.1.5 [DOI] [PubMed] [Google Scholar]
- Shogren KA, Lopez SJ, Wehmeyer ML, Little TD, & Pressgrove CL (2006). The role of positive psychology constructs in predicting life satisfaction in adolescents with and without cognitive disabilities: An exploratory study. Journal of Positive Psychology, 1(1), 37–52. [Google Scholar]
- Tucker JS, Ryan GW, Golinelli D, Ewing B, Wenzel SL, Kennedy DP, … Zhou A (2012). Substance use and other risk factors for unprotected sex: Results from an event-based study of homeless youth. AIDS Behavior, 16, 1699–4707. doi: 10.1007/s10461-011-0017-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turnbull J, Muckle W, & Masters C (2007). Homelessness and health. Canadian Medical Association Journal, 177, 1065–1066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenzel SL, Tucker JS, Golinelli D, Green HD Jr., & Zhou A (2010). Personal network correlates of alcohol, cigarette, and marijuana use among homeless youth. Drug and Alcohol Dependency, 112, 140–149. doi: 10.1016/j.drugalcdep.2010.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]