

Abstract
Objective
This study aims to examine temporal trends and the association between falls and self-rated oral health (SROH) status in community-dwelling older Korean adults.
Design
Secondary analysis of a serial cross-sectional study.
Methods
We analysed biennial data from 314 846 older adults in South Korea from 2011 to 2019 using data from the Korea Community Health Survey. Self-reported fall experience data came from the injury questionnaire question, ‘Have you fallen in the past year (slipping, tripping, stumbling and falling)?’. For SROH, the participants were asked, ‘How do you feel about your oral health, such as teeth and gums, in your own opinion?’. The association between SROH and falls was examined using a weighted multivariable logistic regression model adjusted for sociodemographic characteristics, health status and behaviours, and psychological factors.
Results
Those who reported poor SROH had a lower declining slope than the other groups, although all groups showed a significantly decreasing trend in both men and women from 2011 to 2019 (p for trend<0.001). Older adults who reported having poor SROH had a more significant history of fall accidents than the good SROH groups, controlling for potential confounding variables (adjusted OR 1.16 (95% CI 1.10 to 1.21) in men; adjusted OR 1.17 (95% CI 1.13 to 1.21) in women).
Conclusions
Older adults with poor SROH, especially women, had more fall accidents, making them a priority target for fall prevention strategies. This study suggests considering SROH status when identifying fall risk factors in community-dwelling older adults.
Keywords: aged, epidemiology, oral medicine, public health
STRENGTHS AND LIMITATIONS OF THIS STUDY.
This serial cross-sectional study aimed to identify the association between self-rated oral health status and falls in community-dwelling older Korean adults using community-based nationwide survey data.
Data are serial cross-sectional; therefore, we conducted an analysis of the temporal trend of the fall experience rate according to self-rated oral health status.
This study used self-rated oral health status as an independent variable and lacked available data for additional potential confounders, which can be susceptible to measurement errors and confounding biases.
Introduction
Falls in older adults are a major public health concern worldwide,1 2 and wide-ranging public health actions have highlighted the need to improve the oral health of older persons.3 Oral health status affects general health and well-being.4 Life expectancy rates are increasing, along with an increasing number of older adults with multiple comorbidities who have difficulty maintaining optimal oral health.5 Previous studies have demonstrated that poor oral health is associated with falls. A systematic review of the relationship between oral health and frailty reported that poor oral health affects nutrition, food intake and food choice; poor oral health causes malnutrition and is a risk factor for frailty in older persons.6 7 Moreover, in a prospective cohort study in Japan (the JAGES Project), poor oral health and functional status significantly increased the risk of falls in older adults.8 It has been suggested that poor oral health is associated with fall-related events mediating nutritional status, a prominent risk factor for falls.9
Ageing, changes in physical function, chronic diseases and polypharmacy increase the risk of falls.10 In a previous systematic review of the prevalence of falls in older adults, the prevalence of falls among those living in the community was reported to be 6.7%–44.0%.11 In the South Korean context, fall experiences within a given year were reported by approximately one-third of older adult community residents (13%–42%).12 Adults aged 65 years or older are more susceptible to fatal falls and other serious consequences such as hospitalisation, loss of independence and mortality.13 Risk factors for falls in community-dwelling older adults have been extensively identified and include advanced age, female gender, impaired balance and mobility, visual impairment, depression, frailty or prefrailty, polypharmacy, fear of falling, and comorbidities.14 15 However, the epidemiological literature has addressed fall risk factors in community-dwelling older adults without considering socioeconomic and psychological characteristics, comorbidities, lifestyle, and oral health status. Moreover, no study has analysed the temporal trend of the fall experience rate according to the self-rated oral health (SROH) status of community-dwelling older adults. Although data were gathered biennially from community-dwelling older adults nationwide, there is limited knowledge about the change in fall prevalence over time and the association between SROH and fall experience in the Korean context. Given the previous work on the increasing fall risk in older people with poor oral health,16 exploring the association between SROH status and fall experience in community-dwelling older adults to tackle the rapid ageing of South Korean society is crucial.
Research questions
This study examined the temporal trends and association between subjective oral health status and fall experience in community-dwelling older adults using biennial data from the Korean Community Health Survey (CHS) conducted in South Korea from 2011 to 2019.
Methods
Study design
We conducted a secondary analysis of consecutive cross-sectional survey data collected biennially from 2011 to 2019. The CHS is a nationwide population-based survey among community-dwelling adults aged 19 years and older to assess community health promotions conducted by the Korea Disease Control and Prevention Agency (KDCA) since 2008. The survey uses a complex, multistage, stratified sampling design to collect information related to health status, health behaviours, healthcare utilisation and health determinants to ensure the representativeness of the Korean census.17
Sample
The eligibility criteria for our study included being older adults (age ≥65 years) and living in South Korea. Older adults without complete data on oral health status, fall experience or any other covariates were excluded from the sample. The same questionnaire was used to assess SROH status and fall experience during this period.
Variables
Fall experience
Self-reported fall experience was the dependent variable in this study. The CHS assesses fall experience based on a single question: ‘Have you fallen in the past year (slipping, tripping, stumbling, and falling)?’. The answers were dichotomous, with either a yes or no response.
Self-rated oral health
In the CHS, for SROH, participants were asked, ‘How do you feel about your oral health, such as teeth and gums, in your own opinion?’ The responses were as follows: excellent, very good, good, fair and poor. SROH was classified into binary variables: good for the responses ‘very good’ or ‘good’ or ‘fair’ and poor for the responses ‘bad’ or ‘very bad’.18
Covariates
Based on previous literature on the factors influencing falls in older adults, we included covariates for sociodemographic characteristics, health status and behaviours, and psychological factors.1 19 20 Sociodemographic variables included age (65–74 years, 75–84 years and 85 years or older), sex and education (less than high school, high school or college and above). Average monthly household income (in US dollars (USD)): <US$846, US$846–US$2536, US$2537–US$4226 and ≥US$4227).21 In the present study, body mass index (BMI) was grouped according to the Asia-Pacific BMI classification (<18.5, 18.5–22.9, 23–24.9 and ≥25 kg/m2).21 Comorbidities and health behaviours included hypertension (yes vs no), diabetes (yes vs no), smoking (current, former, never),22 alcohol consumption (yes vs no)22 and regularly recommended walking activity (yes vs no).23 Psychological factors included self-rated health status and depression (yes vs no).
Statistical analysis
Survey analysis procedures were used to account for sample weights, and a complex sampling design was used to ensure nationally representative estimates.24 Using cross-sectional weights proposed by the KDCA, data from four cross-sectional surveys were collected every 2 years from 2011 to 2019, and a single data file was created to explore secular trends. Estimates of the crude weighted prevalence and 95% CIs of falls were calculated by cycle, sex and age. Crude linear trends in the prevalence of falls according to SROH were evaluated using linear regression models across survey cycles to estimate regression coefficients (β) and 95% CIs for every 2 year change. The p values for the trends were estimated using the survey cycle as a continuous variable.
A weighted multivariable logistic regression analysis was used to model the odds of experiencing a fall, depending on SROH, adjusted for related covariates. In addition, logistic regression analyses for secular trends during the entire period were conducted using each year as an explanatory variable and fall experience as a dependent variable (−0.63245=2011, –0.31622=2013, 0.00000=2015, 0.31622=2017, 0.63245=2019).25 All statistical tests were two sided, and statistical significance was set at p<0.05. The p values were not adjusted for multiple tests and were interpreted as exploratory. All statistical analyses were conducted using R statistical software (V.4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of the respondents
The initial sample size for the 2011–2019 CHS biannual cycle was 1 144 045 respondents. We excluded 819 558 respondents younger than 65 years and 9641 with missing information on either oral health status or fall experience. This yielded a final sample of 314 846 respondents (men: 129 750; women: 185 096); respondents with missing covariates (2.9%) were excluded from the multivariable analyses (figure 1).
Figure 1.
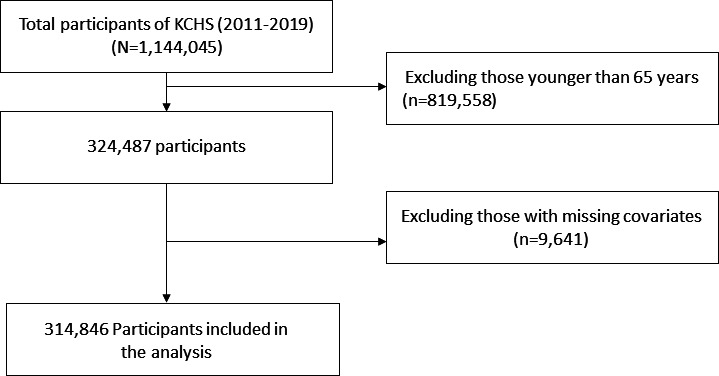
Flow chart of the study samples and participants excluded from the study. KCHS, Korea community health survey.
The unweighted and weighted sample sizes in the 2011–2019 cycle by sex, according to sociodemographic characteristics, health status and behaviours, and psychological factors, are presented in table 1. Within the study sample, more respondents were older adults aged 65–74 years (64.1% men and 58.2% women) than those aged 75 years and older. More than half the participants had an educational level of middle school or below. The prevalence of falls in the study sample was 15.0% in men and 23.7% in women. More than half of the respondents reported that both men and women had poor oral health (table 1).
Table 1.
General characteristics of the study population, using 2011–2019 Korea community health survey data
| Variable | Weighted men (N (%)) |
Weighted women (N (%)) |
| Year | ||
| 2011 | 2 153 288 (15.0) | 2 935 595 (15.8) |
| 2013 | 2 542 206 (17.7) | 3 365 349 (18.1) |
| 2015 | 2 889 175 (20.1) | 3 791 815 (20.4) |
| 2017 | 3 238 425 (22.5) | 4 128 931 (22.2) |
| 2019 | 3 550 167 (24.7) | 4 396 952 (23.6) |
| Fall experience | ||
| No | 12 213 830 (85.0) | 14 212 769 (76.4) |
| Yes | 2 159 431 (15.0) | 4 405 873 (23.7) |
| Self-rated oral health | ||
| Good | 6 380 547 (44.4) | 7 676 231 (41.2) |
| Poor | 7 992 714 (55.6) | 10 942 410 (58.8) |
| Sociodemographic factors | ||
| Age, years | ||
| 65–74 | 9 218 396 (64.1) | 10 842 801 (58.2) |
| 75–84 | 4 550 581 (31.7) | 6 498 438 (34.9) |
| 85– | 604 284 (4.2) | 1 277 402 (6.9) |
| Education | ||
| College or over | 2 656 892 (18.5) | 844 777 (4.5) |
| High school | 3 878 954 (27.0) | 2 124 657 (11.4) |
| Middle school or below | 7 818 662 (54.5) | 15 625 757 (84.0) |
| Body mass index | ||
| Underweight (<18.5) | 1 106 346 (7.7) | 2 896 611 (15.6) |
| Normal (18.5–22.9) | 5 476 436 (38.1) | 6 404 979 (34.4) |
| Overweight (23.0–24.9) | 4 216 652 (29.3) | 4 251 511 (22.8) |
| Obese (>24.9) | 3 573 826 (24.9) | 5 065 540 (27.2) |
| Household income level (US$/month) | ||
| ≥US$4227 | 6 426 925 (44.7) | 6 594 085 (35.4) |
| US$2537–US$4227 | 2 163 382 (15.1) | 2 444 782 (13.1) |
| US$846–US$2536 | 1 242 175 (8.6) | 1 617 728 (8.7) |
| <US$846 | 4 540 779 (31.6) | 7 962 047 (42.8) |
| Health status and behaviours, and psychological factors | ||
| Hypertension | ||
| No | 7 167 805 (49.9) | 8 166 783 (43.9) |
| Yes | 7 201 841 (50.1) | 10 443 521 (56.1) |
| Diabetes | ||
| No | 11 178 952 (77.8) | 14 676 643 (78.9) |
| Yes | 3 190 830 (22.2) | 3 935 213 (21.1) |
| Smoking | ||
| Current | 2 885 967 (20.1) | 451 473 (2.4) |
| Former | 8 320 260 (57.9) | 517 958 (2.8) |
| Never | 3 167 034 (22.03) | 17 649 210 (94.79) |
| Alcohol consumption | ||
| No | 1 773 185 (12.3) | 8 813 808 (47.3) |
| Yes | 12 600 075 (87.7) | 9 804 834 (52.7) |
| Walking activity | ||
| Walking for 30 min/day and ≥5 days a week | 7 090 013 (49.4) | 7 383 545 (39.7) |
| The others | 7 273 763 (50.6) | 11 221 368 (60.3) |
| Self-rated health status | ||
| Good | 9 697 984 (67.5) | 9 577 551 (51.4) |
| Poor | 4 674 962 (32.5) | 9 039 606 (48.6) |
| Depression | ||
| No | 13 580 883 (94.5) | 16 856 182 (90.5) |
| Yes | 792 377 (5.5) | 1 762 459 (9.5) |
Trends in prevalence of fall experience according to SROH
The fall experience among men with good SROH from 2011 to 2019 ranged from 15.8% (95% CI 14.69% to 16.86%) to 10.9% (95% CI 10.17% to 11.61%) and from 17.5% (95% CI 16.70% to 18.27%) to 23.4% (95% CI 22.31% to 24.49%) in female older adults. The prevalence of fall experience with poor SROH was from 15.1 (95% CI 14.25 to 15.88) to 20.0 (95% CI 19.05 to 21.02) among men and from 23.4 (95% CI 22.63 to 24.23) to 30.0 (95% CI 29.07 to 30.94) in women (figure 2). Despite all groups showing a significantly decreasing trend (p for trend<0.001) in both males and females, older adults who reported poor SROH had a lower declining slope than the good SROH group (β coefficient=−0.34 for good SROH vs −0.28 for poor SH in men, β coefficient=−0.29 for good SROH vs −0.25 for poor SROH in women). Notably, the number of falls in the poor SROH group was consistently higher than that in the good SROH group from 2011 to 2019 (Appendix Table 1).
Figure 2.
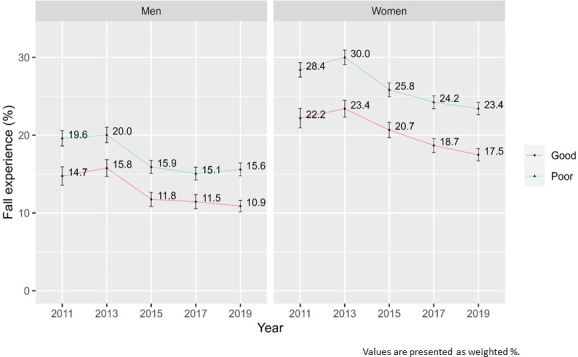
Trends in fall experience rate according to self-rated oral health, Korea community health survey 2011–2019.
bmjopen-2023-081549supp001.pdf (111.8KB, pdf)
Association between fall experience and SROH
The results of the hierarchical logistic regression analyses examining the relationship between fall experience and SROH among the respondents are shown in table 2. In male older adults, the logistic regression analysis (model 1) showed that the OR of having a fall experience was significantly higher in the poor group than in the good group (OR 1.44 (95% CI 1.37 to 1.51)). This OR was still significantly high after controlling for sociodemographic factors (adjusted OR 1.31 (95% CI 1.25 to 1.38) in model 2) and other confounders, including health status and behaviours and psychological factors (adjusted OR 1.16 (95% CI 1.10 to 1.21) in model 3) (table 2).
Table 2.
Association between fall experience and self-rated oral health by hierarchical logistic regression analysis
| Self-rated oral health | Men, OR (95% CI) | Women, OR (95% CI) | |
| Model 1* | Good | 1.00 (ref) | 1.00 (ref) |
| Poor | 1.44 (1.37 to 1.51) | 1.42 (1.38 to 1.47) | |
| Model 2† | Good | 1.00 (ref) | 1.00 (ref) |
| Poor | 1.31 (1.25 to 1.38) | 1.34 (1.29 to 1.38) | |
| Model 3‡ | Good | 1.00 (ref) | 1.00 (ref) |
| Poor | 1.16 (1.10 to 1.21) | 1.17 (1.13 to 1.21) |
*Model 1: Unadjusted. OR, 95% CI.
†Model 2: Adjusted for sociodemographic factors.
‡Model 3: Adjusted for sociodemographic factors, health status and behaviours, and psychological factors.
Similarly, these associations were consistently observed in female older adults. In the unadjusted logistic regression model 1, the ORs were significantly higher for the poor group than for the good SROH group (OR 1.42 (95% CI 1.38 to 1.47)). In model 2, which was adjusted for sociodemographic factors, poor SROH respondents were significantly more likely to report fall experiences than respondents in other groups (adjusted OR 1.34 (95% CI 1.29 to 1.38)). Fall experience was also significantly associated with poor SROH after controlling for sociodemographic factors, health status and behaviours, and psychological factors (adjusted OR 1.17 (95% CI 1.13 to 1.21)) (table 2).
Discussion
This study examined the prevalence of falls and the relationship between SROH and fall experience among adults aged 65 years and older using 2011–2019 CHS data. Our study findings, using national-level population big data, show that the fall experience rate decreased significantly in both men and women.
The estimated fall experience showed a statistically significant decline across older adults in all the SROH groups. The present findings could be explained by increased public awareness of health education and the initiative for a comprehensive community care system for older adults in Korea, which has led to a reduction in the prevalence of fall experiences.26 These findings were consistent with previous research that showed that fall prevalence declined from 2011 to 2013 in Chinese older adults aged ≥60 years, although the difference was not significant (2011:19.64%; 2013:19.28%; p=0.60).27 Non-fatal falls among American older adults increased from 2012 to 2016, and the contemporary incidence of falls decreased from 2016 to 2018.28
However, female older adults consistently reported a fall experience rate more than twice that of male older adults over the 9-year study period. In addition, compared with older adults reporting good SROH, poor SROH was significantly associated with fall experiences in community-dwelling older adults in Korea. These results were in line with those of previous studies showing that female older adults had a significantly higher likelihood of falling among Chinese than male older adults (OR 1.44, 95% CI 1.28 to 1.61).27 In Swedish community-dwelling men and women aged 70 years, the adjusted OR for falling in women was 1.49 (95% CI 1.02 to 2.19) compared with men older adults.29 Moreover, female older adults were also more prone to experience fall incidents than male older adults using data from the Survey of Living Conditions and Welfare Needs of Korean Older Persons (OR 1.90 (95% CI 1.61 to 2.24)) for older women versus older men (OR 1.59 (95% CI 1.26 to 1.99)). The biological plausibility linking sex and falling may be related to sex-based differences in psychosocial aspects and bone and muscle balance due to ageing, as well as hormonal changes associated with menopause.30
In all adjusted models, poor SROH was significantly associated with higher odds of falling. This result is in line with that of a previous study using self-reported questionnaires in which poor oral function, such as difficulty eating tough foods, dry mouth and fewer teeth, were predictors of incident falls in community-dwelling older people.8 In addition, poor oral health status, as measured by a clinical dental examination and oral health questionnaire, has been reported as a risk factor for fall-related fractures. More specifically, compared with those with 20 teeth or more, the HRs (95% CIs) of fall-related fractures in individuals with 1–9 teeth and edentulous individuals were 2.67 (1.24 to 5.75) and 2.31 (1.01 to 5.28), respectively.9 Our study findings support the prior explanation that poor oral function is associated with increased malnutrition due to difficulty in eating31 and a decline in muscle strength and physical function, resulting in an increased risk of falls in both cross-sectional and prospective cohort studies.32 33
This time trend is critical because it provides dynamic information about fall prevalence to enable better preventive projects, help design care policies for older adults and allocate health resources for fall prevention. Nonetheless, few studies have examined the temporal trends of fall experiences by SROH. In this study, those who reported poor SROH had a lower slope of decline than those in the good SROH group, despite all groups showing a significantly decreasing trend for both men and women. The declining trend in fall experiences among all groups could be explained by the efforts of health authorities in Korea to develop and implement evidence-based guidelines for fall prevention,12 provide fall prevention interventions34 and conduct National Injury Surveillance and Prevention to minimise damage and social losses resulting from injury and falls.35
In particular, female older adults with poor SROH should be regarded as a priority target population in oral health promotion and fall prevention campaigns, such as the 8020 campaign launched in Japan to preserve at least 20 teeth at the target age of 80 years.36 In addition to a public oral health campaign, to deal with oral health problems in this vulnerable population, public health professionals who deal with female older adults in the community should assess their oral health and handle any issues appropriately, such as educating them on effective methods for preventing tooth decay with fluoride, proper cleaning against periodontal disease, regular dental checkups and timely dental care to prevent tooth loss and maintain optimal oral health.
This study has several limitations. SROH was measured by subjective oral health rather than objective oral health, as measured by clinical dental examination and medical records, including dental prostheses and number of teeth.37 Nevertheless, SROH research has been widely conducted in epidemiological studies,38 and SROH used in the CHS was considered an acceptable oral health outcome measure. However, significant predictors of the risk of falls, such as the number of teeth, need to include data on annual oral health status in the CHS. Second, although the associated covariates related to falls were included, other potentially important factors such as cognitive ability, various types of comorbidities and activity limitations were not. Therefore, future research should include variables related to fall risk, such as psychological, physical, cognitive and residential environmental factors. Third, fall experiences in this study were confirmed through self-reports during the past year; therefore, self-reports might be vulnerable to recall bias. Finally, as this was a serial cross-sectional study, the relationship between poor SROH and fall experience may not be causal. Owing to the limitations of the study design, well-designed longitudinal studies are required to confirm these findings. Fourth, to elucidate the causal relationship between oral health and fall experience, further data related to nutrition and food intake behaviour as mediators or moderators indicated that malnutrition data needs to be collected in this population.39
Despite these limitations, this is the first study to identify trends and the association between SROH and fall experience in community-dwelling older adults nationwide. In addition, the results of our study provide a comprehensive understanding of the association between SROH and fall experience, which is valuable for devising oral health promotion strategies to help manage fall accidents at a national level.
Conclusion
Poor oral health is considered as a risk factor for falls in community-dwelling older adults. However, there has been limited research on this topic in the context of South Korea’s ageing population. The findings of this study indicated that those who reported poor SROH had a lower slope of decline than those who reported good SROH, despite all groups showing a significantly decreasing fall experience trend in both male and female older adults. Moreover, after adjusting for potential confounding variables, older adults who reported poor SROH had a greater history of falls than those with good SROH. Notably, older females with poor SROH posed a substantial concern that cannot be ignored in fall experience trends related to SROH. Therefore, primary healthcare professionals, including dentists, physicians and public health nurses, need to pay attention to SROH status to prevent falls in female older adults. Objective clinical oral assessments, oral health management and referral of dental care resources are required to address oral health problems in this target population.
Supplementary Material
Footnotes
H-JS and S-KA contributed equally.
Contributors: Guarantor, Conceptualisation: H-JS, S-KA and M-JC. Data curation, Formal analysis: S-KA. Funding acquisition: H-JS. Methodology, Project administration, Visualisation: H-JS and S-KA. Writing–original draft and revision: H-JS, S-KA and M-JC. Writing–review and editing: H-JS and M-JC.
Funding: This research was supported by the Research Grant of Chungnam National University Hospital in 2022 by Hyun-Ju Seo.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available on reasonable request. Publicly available datasets were analysed in this study. This data can be found here: (https://chs.kdca.go.kr/chs/rawDta/rawDtaProvdMain.do) (assessed on 18 August 2023). The original data presented in the study are included in the article and online supplemental material, further inquiries can be directed to the corresponding author.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
The Institutional Review Board of the KDCA approved the CHS. Raw CHS data were downloaded from the CHS website after applying for and receiving permission from the website administrator (April 2022). This study was approved by the Institutional Review Board of Chungnam National University (202204-SB-046-01).
References
- 1. Matsuyama Y, Aida J, Watt RG, et al. Dental status and compression of life expectancy with disability. J Dent Res 2017;96:1006–13. 10.1177/0022034517713166 [DOI] [PubMed] [Google Scholar]
- 2. World Health Organization . Falls, WHO fact sheets. 2021. Available: https://www.who.int/news-room/fact-sheets/detail/falls
- 3. Petersen PE, Ogawa H. Promoting oral health and quality of life of older people - the need for public health action. Oral Health Prev Dent 2018;16:113–24. 10.3290/j.ohpd.a40309 [DOI] [PubMed] [Google Scholar]
- 4. Raphael C. Oral health and aging. Am J Public Health 2017;107:S44–5. 10.2105/AJPH.2017.303835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Porter J, Ntouva A, Read A, et al. The impact of oral health on the quality of life of nursing home residents. Health Qual Life Outcomes 2015;13:102. 10.1186/s12955-015-0300-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hakeem FF, Bernabé E, Sabbah W. Association between oral health and frailty: A systematic review of longitudinal studies. Gerodontology 2019;36:205–15. 10.1111/ger.12406 [DOI] [PubMed] [Google Scholar]
- 7. Rapp L, Sourdet S, Lacoste-Ferré MH. Oral health and Undernutrition in the frail elderly persons. J Nutr Health Aging 2021;25:484–91. 10.1007/s12603-020-1546-6 [DOI] [PubMed] [Google Scholar]
- 8. Mochida Y, Yamamoto T, Fuchida S, et al. Does poor oral health status increase the risk of falls?: the JAGES project longitudinal study. PLoS One 2018;13:e0192251. 10.1371/journal.pone.0192251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ito W, Komiyama T, Ohi T, et al. Relationship between oral health and fractures in community-dwelling older Japanese adults. J Am Med Dir Assoc 2021;22:1184–9. 10.1016/j.jamda.2021.01.058 [DOI] [PubMed] [Google Scholar]
- 10. Neziraj M, Hellman P, Kumlien C, et al. Prevalence of risk for pressure ulcers, malnutrition, poor oral health and falls - a register study among older persons receiving municipal health care in southern Sweden. BMC Geriatr 2021;21:265. 10.1186/s12877-021-02205-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Fhon JRS, Rodrigues RAP, Neira WF, et al. Fall and its association with the frailty syndrome in the elderly: systematic review with meta-analysis. Rev Esc Enferm USP 2016;50:1005–13. 10.1590/s0080-623420160000700018 [DOI] [PubMed] [Google Scholar]
- 12. Kim K-I, Jung H-K, Kim CO, et al. Evidence-based guidelines for fall prevention in Korea. Korean J Intern Med 2017;32:199–210. 10.3904/kjim.2016.218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Vieira ER, Palmer RC, Chaves PHM. Prevention of falls in older people living in the community. BMJ 2016;353:i1419. 10.1136/bmj.i1419 [DOI] [PubMed] [Google Scholar]
- 14. Zhao Y (Lucy), Alderden J, Lind BK, et al. A comprehensive assessment of risk factors for falls in community-dwelling older adults. J Gerontol Nurs 2018;44:40–8. 10.3928/00989134-20180913-04 [DOI] [PubMed] [Google Scholar]
- 15. Almada M, Brochado P, Portela D, et al. Prevalence of falls and associated factors among community-dwelling older adults: A cross-sectional study. J Frailty Aging 2021;10:10–6. 10.14283/jfa.2020.44 [DOI] [PubMed] [Google Scholar]
- 16. Badewy R, Singh H, Quiñonez C, et al. Impact of poor oral health on community-dwelling seniors: A Scoping review. Health Serv Insights 2021;14:1178632921989734. 10.1177/1178632921989734 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Seo HJ, Choi MJ, Ahn SK. Secular trends and related factors in leisure-time sedentary behavior among Koreans: an analysis of data from the 2011-2017 Korea community health survey. Epidemiol Health 2022;44:e2022023. 10.4178/epih.e2022023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Kotronia E, Brown H, Papacosta AO, et al. Poor oral health and the association with diet quality and intake in older people in two studies in the UK and USA. Br J Nutr 2021;126:118–30. 10.1017/S0007114521000180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hakeem FF, Bernabé E, Sabbah W. Self-rated oral health and frailty index among older Americans. Gerodontology 2021;38:185–90. 10.1111/ger.12513 [DOI] [PubMed] [Google Scholar]
- 20. Han A, Shin M, Yang J ho, et al. Body mass index and self-rated oral health in Korean adults in 2017. Gerodontology 2023;40:183–91. 10.1111/ger.12624 [DOI] [PubMed] [Google Scholar]
- 21. Lim JU, Lee JH, Kim JS, et al. Comparison of world health organization and Asia-Pacific body mass index classifications in COPD patients [DOI] [PMC free article] [PubMed]
- 22. Gu Y, Wu W, Bai J, et al. Association between the number of teeth and frailty among Chinese older adults: a nationwide cross-sectional study. BMJ Open 2019;9:e029929. 10.1136/bmjopen-2019-029929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Schutz Y, Nguyen DMT, Byrne NM, et al. Effectiveness of three different walking prescription durations on total physical activity in Normal- and overweight women. Obes Facts 2014;7:264–73. 10.1159/000365833 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Kang YW, Ko YS, Kim YJ, et al. Korea community health survey data profiles. Osong Public Health Res Perspect 2015;6:211–7. 10.1016/j.phrp.2015.05.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Bae SG, Kim JY, Kim KY, et al. Changes in dietary behavior among adolescents and their association with government nutrition policies in Korea, 2005-2009. J Prev Med Public Health 2012;45:47–59. 10.3961/jpmph.2012.45.1.47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Lee KS. Health care perspectives on community care. J Korean Med Assoc 2018;61:586. 10.5124/jkma.2018.61.10.586 [DOI] [Google Scholar]
- 27. Wu H, Ouyang P. Fall prevalence, time trend and its related risk factors among elderly people in China. Arch Gerontol Geriatr 2017;73:294–9. 10.1016/j.archger.2017.08.009 [DOI] [PubMed] [Google Scholar]
- 28. Moreland B, Kakara R, Henry A. Trends in nonfatal falls and fall-related injuries among adults aged ≥65 years - United States, 2012-2018. MMWR Morb Mortal Wkly Rep 2020;69:875–81. 10.15585/mmwr.mm6927a5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Johansson J, Nordström A, Nordström P. Greater fall risk in elderly women than in men is associated with increased gait variability during Multitasking. J Am Med Dir Assoc 2016;17:535–40. 10.1016/j.jamda.2016.02.009 [DOI] [PubMed] [Google Scholar]
- 30. Jo A-R, Park M-J, Lee B-G, et al. Association between falls and nutritional status of community-dwelling elderly people in Korea. Korean J Fam Med 2020;41:111–8. 10.4082/kjfm.18.0112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hasegawa Y, Horii N, Sakuramoto-Sadakane A, et al. Is a history of falling related to oral function? A cross-sectional survey of elderly subjects in rural Japan. Int J Environ Res Public Health 2019;16:3843. 10.3390/ijerph16203843 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Albani V, Nishio K, Ito T, et al. Associations of poor oral health with frailty and physical functioning in the oldest old: results from two studies in England and Japan. BMC Geriatr 2021;21:187. 10.1186/s12877-021-02081-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kimble R, McLellan G, Lennon LT, et al. Association between oral health markers and decline in muscle strength and physical performance in later life: longitudinal analyses of two prospective cohorts from the UK and the USA. Lancet Healthy Longev 2022;3:e777–88. 10.1016/S2666-7568(22)00222-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Lee SH, Bak WS, Shin GY, et al. Development of a fall-prevention exercise program for elderly people in community. J Muscle Joint Health 2020;27:61–70. [Google Scholar]
- 35. Lee YK, Hong SO, Park SJ, et al. Data resource profile: the Korea national hospital discharge in-depth injury survey. Epidemiol Health 2021;43:e2021052. 10.4178/epih.e2021052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Ministry of Health, Labour, and Welfare . e-Health Net, Available: https://www.e- healthnet.mhlw.go.jp/information/teeth/h-01-003.html
- 37. Maille G, Saliba-Serre B, Ferrandez AM, et al. Objective and perceived oral health status of elderly nursing home residents: a local survey in Southern France. Clin Interv Aging 2019;14:1141–51. 10.2147/CIA.S204533 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Maida CA, Xiong D, Marcus M, et al. Quantitative data collection approaches in subject-reported oral health research: a Scoping review. BMC Oral Health 2022;22:435. 10.1186/s12903-022-02399-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Akinkugbe AA, Sharma S, Ohrbach R, et al. Directed Acyclic graphs for oral disease research. J Dent Res 2016;95:853–9. 10.1177/0022034516639920 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2023-081549supp001.pdf (111.8KB, pdf)
Data Availability Statement
Data are available on reasonable request. Publicly available datasets were analysed in this study. This data can be found here: (https://chs.kdca.go.kr/chs/rawDta/rawDtaProvdMain.do) (assessed on 18 August 2023). The original data presented in the study are included in the article and online supplemental material, further inquiries can be directed to the corresponding author.