

Abstract
Background
This article presents a comprehensive review of data on the impact of facial palsy during the coronavirus disease 2019 (COVID-19) pandemic. The possible causes and pathophysiological mechanisms of changes in the epidemiology of facial palsy during the COVID-19 pandemic are also discussed.
Methods
This multicenter retrospective cohort study included 943 patients diagnosed with Bell’s palsy or Ramsay Hunt syndrome. This study compared patient demographics, comorbidities, symptoms, and treatments before the COVID-19 pandemic (from 2017 to 2019) and during the COVID-19 pandemic, from 2020 to 2022).
Results
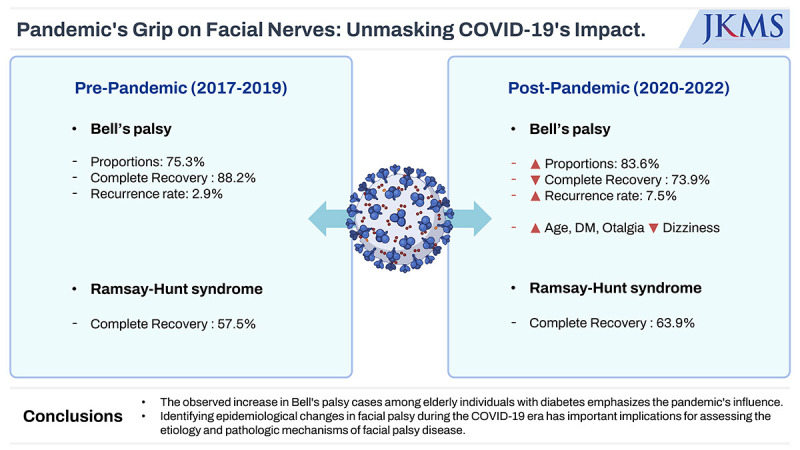
Following the COVID-19 outbreak, there has been a significant increase in the number of cases of Bell’s palsy, particularly among elderly individuals with diabetes. Bell’s palsy increased after the COVID-19 outbreak, rising from 75.3% in the pre-COVID-19 era to 83.6% after the COVID-19 outbreak. The complete recovery rate decreased from 88.2% to 73.9%, and the rate of recurrence increased from 2.9% to 7.5% in patients with Bell’s palsy. Ramsay Hunt syndrome showed fewer changes in clinical outcomes.
Conclusion
This study highlights the impact of the COVID-19 pandemic on the presentation and management of facial palsy, and suggests potential associations with COVID-19. Notably, the observed increase in Bell’s palsy cases among elderly individuals with diabetes emphasizes the impact of the pandemic. Identifying the epidemiological changes in facial palsy during the COVID-19 pandemic has important implications for assessing its etiology and pathological mechanisms of facial palsy disease.
Keywords: Bell’s Palsy, Ramsay Hunt Syndrome, COVID-19, Facial Palsy
Graphical Abstract
INTRODUCTION
The coronavirus disease 2019 (COVID-19) crisis has brought tremendous changes and unprecedented challenges to the global healthcare community. The novel coronavirus has a rapid transmission rate and causes highly contagious infections, leading to pandemics. As of 1st October 2023, the World Health Organization (WHO) has reported over 767 million COVID-19 cases and 6.9 million deaths all over the world1. Furthermore, researchers have found that COVID-19 can affect organs in the body other than the respiratory system. There have been various concerns regarding COVID-19, including its correlation with other acute or chronic diseases and underlying health conditions.
Bell’s palsy is characterized by idiopathic facial nerve dysfunction. Although the exact cause of Bell’s palsy is unknown, inflammation and ischemic compression following viral infections with herpes simplex virus-1 (HSV-1), varicella-zoster virus (VZV), Epstein-Barr virus (EBV), cytomegalovirus (CMV), and human immunodeficiency virus (HIV) have been suggested as potential mechanisms of Bell’s palsy. Facial palsy has also been documented as a neurological manifestation in COVID-19 patients, often as the first and sole presentation of COVID-19.2 In addition, the current research has reported an increased number of Bell’s palsy diagnoses following the COVID-19 outbreak. These developments underscore the need to investigate the shifting landscape in facial palsy. This study is essential because it provides both healthcare providers and patients with insights into the evolution of knowledge on facial palsy before and after the onset of COVID-19. This study aimed to provide an overview of Bell’s palsy and Ramsay Hunt syndrome manifestations during the COVID-19 pandemic to understand the association between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and facial palsy.
METHODS
This retrospective multicenter cohort study was conducted in five hospitals located in Seoul, Daejeon, Bucheon, and Hwaseong, South Korea. It included individual data from patients diagnosed with idiopathic facial palsy (Bell’s palsy) or Ramsay Hunt syndrome, facial palsy with vesicular lesions in the external auditory canal or around the ear, and/or accompanying audiovestibular symptoms, such as hearing loss or dizziness. The data comprised cases before the COVID-19 outbreak between January 2017 and December 2019 and those with facial palsy during the COVID-19 pandemic between January 2020 and December 2022. The exclusion criteria were as follows: 1) presence of bacterial infection or inflammatory disease (cholesteatoma or chronic otitis media) in the middle ear, 2) history of otologic surgery or head trauma, 3) history of head and neck cancer, 4) facial palsy associated with central nervous system lesions, and 5) autoimmune diseases.
Epidemiological and demographic data and clinical records of the patients were analyzed. The collected data included age, sex, and presence of comorbidities, such as diabetes mellitus and hypertension. The time from the onset of palsy to treatment initiation, the degree of facial nerve palsy assessed using the House-Brackmann grading system, associated symptoms (otalgia, dizziness, tinnitus, and hyperacusis), treatment modalities such as the types of steroids and antivirals used, and facial function results after treatment were also evaluated.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Macintosh, version 29.0 (IBM Corp., Armonk, NY, USA), with P values < 0.05 considered statistically significant. Descriptive statistics such as means, percentages, and standard deviations were used to summarize the characteristics of the enrolled patients. Categorical variables, including diagnosis, laterality, accompanying symptoms, and diseases, are summarized as counts and percentages. For oral and intratympanic steroids (ITS), the χ2 test or Fisher’s exact test was used to determine whether there was a statistically significant difference in their usage before and after the COVID-19 outbreak. Normally distributed continuous variables, such as House-Brackmann grades, were analyzed using Student’s t-test to assess whether there were significant differences before and after the outbreak. Categorical variables, including diagnosis, accompanying symptoms, complete recovery, and recurrence rates, were assessed for significant changes pre-COVID-19 and after COVID-19 using the χ2 or Fisher’s exact tests.
Ethics statement
This retrospective cohort study was reviewed and approved by Institutional Review Board of Ewha Womans University Mokdong Hospital (IRB number: 2023-10-034). The requirement for written informed consent was waived owing to the retrospective nature of the study.
RESULTS
Patient characteristics
Nine hundred forty-three patients, comprising 450 males (47.7%) and 493 females (52.3%) with a mean age of 50 years (range: 1–89 years), were enrolled in this study. The average duration from the disease onset to treatment initiation was 2.52 ± 3.28 days, ranging from 0 to 73 days. The mean House-Brackmann grading at the initial visit was 3.36 ± 1.06, ranging from 2 to 6. Of the 943 patients, 748 (79.3%) were diagnosed with Bell's palsy, and the remaining 195 (20.7%) were diagnosed with Ramsay Hunt syndrome. Facial palsy laterality was documented in 802 patients (85.0%), of whom 366 (45.6%) had right-sided facial palsy, 435 (54.2%) had left-sided facial palsy, and one (0.1%) presented with bilateral facial palsy. The most common accompanying symptom was otalgia, which was observed in 42.4% of patients (n = 400), followed by tinnitus (16.8%, n = 140/835), dizziness (16.1%, n = 152/943), and hyperacusis (7.3%, n = 61/835). Hypertension was present in 29.9% of the patients (n = 282/942) and diabetes mellitus in 14.5% (n = 137/942). Regarding recurrence, 4.2% of the patients (n = 38/906) had a previous history of facial palsy.
Changes in clinical manifestations after the COVID-19 outbreak
Table 1 compares the total number of patients with facial palsy before and after the COVID-19 pandemic. Notably, the proportion of Bell’s palsy cases increased after the COVID-19 outbreak, rising from 75.3% in the pre-COVID-19 era to 83.6% after the COVID-19 outbreak, and this difference was statistically significant (P = 0.002). The time to treatment initiation after the COVID-19 outbreak was 2.65 ± 4.23 days, which was not significantly different from the pre-COVID-19 era (2.41 ± 2.25 days) (P > 0.05).
Table 1. Comparison of total patients with facial palsy between pre-COVID-19 and COVID-19 pandemic.
| Variables | Pre-COVID 19 2017–2019 (n = 497) | COVID-19 pandemic 2020–2022 (n = 446) | P value | ||
|---|---|---|---|---|---|
| Total facial palsy | 0.002** | ||||
| Bell’s palsy | 75.5 (375/497) | 83.6 (373/446) | |||
| Ramsay Hunt syndrome | 24.5 (122/497) | 16.4 (73/446) | |||
| Age, yr | 47.88 ± 16.78 | 53.22 ± 17.31 | < 0.001*** | ||
| Sex | 0.500 | ||||
| Male | 46.7 (232/497) | 48.9 (218/446) | |||
| Female | 53.3 (265/497) | 51.1 (228/446) | |||
| Laterality | 0.093a | ||||
| Right | 43.1 (192/445) | 48.7 (174/357) | |||
| Left | 56.9 (253/445) | 51.0 (182/357) | |||
| Bilateral | 0.0 (0/445) | 0.3 (1/357) | |||
| Onset to treatment (days) | 2.41 ± 2.25 | 2.65 ± 4.23 | 0.312 | ||
| Associated symptoms | |||||
| Otalgia | 59.2 (294/497) | 55.8 (249/446) | 0.302 | ||
| Dizziness | 21.5 (107/497) | 10.1 (45/446) | < 0.001*** | ||
| Tinnitus | 19.3 (75/389) | 14.6 (65/446) | 0.069 | ||
| Hyperacusis | 8.7 (34/389) | 6.1 (27/446) | 0.137 | ||
| Underlying comorbidities | |||||
| HTN | 29.0 (144/497) | 31.0 (138/445) | 0.495 | ||
| Diabetes | 8.5 (42/497) | 21.3 (95/445) | < 0.001*** | ||
| Association with COVID-19 vaccine or recent infection (< 15d) | - | 18/446 (4.0) | - | ||
| Treatment modality | < 0.001*** | ||||
| Systemic steroid | 89.3 (444/497) | 78.2 (348/446) | < 0.001*** | ||
| ITS injection | 10.1 (45/445) | 1.1 (4/357) | |||
| Anti-viral agent | < 0.001a, *** | ||||
| Valaciclovir | 25.7 (108/421) | 0.3 (1/316) | |||
| Famciclovir | 70.8 (298/421) | 96.8 (306/316) | |||
| Acyclovir | 3.6 (15/421) | 2.8 (9/316) | |||
| Initial HB grade | 3.42 ± 1.03 | 3.30 ± 1.10 | 0.082 | ||
| Grade I | 0 (0/497) | 0 (0/446) | - | ||
| Grade II–VI | 100 (497/497) | 100 (446/446) | - | ||
| Final HB grade | 1.33 ± 0.83 | 1.41 ± 0.80 | 0.150 | ||
| Grade I | 19.0 (86/453) | 27.6 (110/398) | |||
| Grade II–VI | 81.0 (365/453) | 72.4 (288/398) | |||
| Recurrence of facial palsy | 2.2 (10/461) | 6.3 (28/446) | 0.002** | ||
Data are presented as % (number) or mean ± standard deviation.
The results were based on the Student’s t-test or χ2 test, unless otherwise noted.
COVID-19 = coronavirus disease 2019, HTN = hypertension, ITS = intratympanic steroid, HB = House-Brackmann.
aThe Fisher’s exact test was used.
Statistical significance (*P < 0.05, **P < 0.01, ***P < 0.001) is indicated in bold.
Bell’s palsy
For Bell’s palsy (Table 2), the age increased significantly from 47 years (with a mean of 47.49 ± 17.07) to 53 years (with a mean of 53.16 ± 17.26) following the outbreak of COVID-19 (P < 0.001). Furthermore, diabetes as a comorbidity also showed a significant increase from 8.5% (n = 32/375) to 24.2% (n = 90/372) after the COVID-19 outbreak (P < 0.001). Sex and the affected side, however, exhibited no statistically significant differences (P > 0.05).
Table 2. Comparison of patients with Bell’s palsy between pre-COVID 19 and COVID-19 pandemic.
| Variables | Pre-COVID 19 2017–2019 (n = 375) | COVID-19 pandemic 2020–2022 (n = 373) | P value | |
|---|---|---|---|---|
| Age, yr | 47.49 ± 17.07 | 53.16 ± 17.26 | < 0.001*** | |
| < 60 | 72.8 (273/375) | 56.6 (211/373) | < 0.001*** | |
| ≥ 60 | 27.9 (102/375) | 43.4 (162/373) | ||
| Sex | 0.343 | |||
| Male | 46.4 (174/375) | 49.9 (186/373) | ||
| Female | 53.6 (201/375) | 50.1 (187/373) | ||
| Associated symptoms | ||||
| Otalgia | 30.1 (113/375) | 37.5 (140/373) | 0.037* | |
| Dizziness | 18.7 (70/375) | 5.1 (19/373) | < 0.001** | |
| Tinnitus | 11.9 (35/293) | 11.5 (43/373) | 0.868 | |
| Hyperacusis | 8.2 (24/293) | 5.9 (22/373) | 0.247 | |
| Underlying comorbidities | ||||
| HTN | 33.6 (126/375) | 33.3 (124/372) | 0.938 | |
| Diabetes | 8.5 (32/375) | 24.2 (90/372) | < 0.001*** | |
| Initial HB grade | 3.41 ± 1.04 | 3.20 ± 1.08 | 0.004** | |
| Grade I | 0 (0/375) | 0 (0/375) | - | |
| Grade II–VI | 100 (375/375) | 100 (373/375) | ||
| Final HB grade | 1.20 ± 0.68 | 1.38 ± 0.77 | 0.001** | |
| Grade I | 88.2 (306/347) | 73.9 (249/337) | < 0.001*** | |
| Grade II–VI | 11.8 (41/347) | 26.1 (88/337) | ||
| Recurrence of facial palsy | 2.9 (10/349) | 7.5 (28/373) | 0.005** | |
Data are presented as mean ± standard deviation or % (number).
The results were based on the Student’s t-test or χ2 test, unless otherwise noted.
COVID-19 = coronavirus disease 2019, HTN = hypertension, HB = House-Brackmann.
Statistical significance (*P < 0.05, **P < 0.01, ***P < 0.001) is indicated in bold.
Among the accompanying symptoms, otalgia significantly increased following the COVID-19 outbreak from 30.1% (n = 113/375) to 37.5% (n = 140/373) (P = 0.037). Conversely, the number of dizziness episodes significantly decreased from 18.7% (n = 70/375) before the COVID-19 pandemic to 5.1% (n = 19/373) during COVID-19 pandimic outbreak (P < 0.001). Tinnitus and hyperacusis, on the other hand, remained unchanged (P > 0.05).
After the COVID-19 outbreak, the initial House-Brackmann grade for facial palsy decreased from 3.41 ± 1.04 to 3.20 ± 1.08 (P = 0.004), and the final grade decreased from 1.20 ± 0.68 to 1.38 ± 0.77 (P < 0.001). Subsequently, the complete recovery rate based on House-Brackmann grade I significantly decreased from the pre-COVID-19 era (88.2%, 306/346) to 73.9% (n = 249/337) (P < 0.001) COVID-19 pandemic outbreak. There was also a significant increase in the incidence of recurrent facial palsy from 2.9% (n = 10/349) before the COVID-19 outbreak to 7.5% (n = 28/373) (P = 0.005) after the COVID-19 pandemic. In essence, Bell's palsy increased in elderly patients with diabetes after the COVID-19 outbreak, accompanied by a decrease in the cure rate.
Ramsay Hunt syndrome
Regarding Ramsay Hunt syndrome, age, sex, affected side, diabetes, and hypertension showed no significant differences before and after COVID-19. The initial House-Brackmann grade worsened, shifting from 3.45 ± 0.99 to 3.79 ± 1.07 (P = 0.024, Table 3). However, no significant differences were observed in the results of the final treatment. The accompanying symptoms showed no significant differences before and after the COVID-19 outbreak (P > 0.05). The complete recovery rate of Ramsay Hunt syndrome increased from 57.5% (n = 61/106) to 63.9% (n = 39/61); however, this change was not statistically significant (P > 0.05). In summary, Ramsay Hunt syndrome showed no significant changes after the onset of COVID-19.
Table 3. Comparison of patients with Ramsay Hunt syndrome between pre-COVID-19 and COVID-19 pandemic periods.
| Variables | Pre-COVID 19 2017–2019 (n = 122) | COVID-19 pandemic 2020–2022 (n = 73) | P value | |
|---|---|---|---|---|
| Age, yr | 49.03 ± 15.92 | 53.55 ± 17.69 | 0.067 | |
| < 60 | 73.8 (90/122) | 61.6 (45/73) | 0.076 | |
| ≥ 60 | 26.2 (32/122) | 38.4 (28/73) | ||
| Sex | 0.615 | |||
| Male | 47.5 (58/122) | 43.8 (32/73) | ||
| Female | 52.5 (64/122) | 56.2 (41/73) | ||
| Associated symptoms | ||||
| Otalgia | 73.8 (90/122) | 78.1 (57/73) | 0.499 | |
| Dizziness | 30.3 (37/122) | 35.6 (26/73) | 0.445 | |
| Tinnitus | 41.7 (40/96) | 30.1 (22/73) | 0.123 | |
| Hyperacusis | 10.4 (10/96) | 6.8 (5/73) | 0.419 | |
| Underlying comorbidities | ||||
| HTN | 14.8 (18/122) | 19.2 (14/73) | 0.420 | |
| Diabetes | 8.2 (10/122) | 6.8 (5/73) | 0.733 | |
| Initial HB grade | 3.45 ± 0.99 | 3.79 ± 1.07 | 0.024* | |
| Grade I | 0 (0) | 0 (0) | - | |
| Grade II–VI | 100 (122) | 100 (73) | ||
| Final HB grade | 1.74 ± 1.11 | 1.59 ± 1.00 | 0.394 | |
| Grade I | 62/107 (57.9) | 39/61 (63.9) | 0.513 | |
| Grade II–VI | 45/107 (42.1) | 22/61 (36.1) | ||
| Recurrence of facial palsy | 0 (0/111) | 0 (0/73) | - | |
Data are presented as mean ± standard deviation or % (number).
The results were based on the Student’s t-test or χ2 test, unless otherwise noted.
COVID-19 = coronavirus disease 2019, HTN = hypertension, HB = House-Brackmann.
Statistical significance (*P < 0.05, **P < 0.01, ***P < 0.001) is indicated in bold.
Changes in applied treatment
The use of oral steroids showed significant differences before and after the COVID-19 outbreak, demonstrating a decreasing trend from 89.3% to 79.2% (P < 0.001; Table 1). Similarly, the application frequency of ITS declined during the COVID-19 pandemic, with rates of 10.1% (n = 45/445) in the pre-COVID-19 period and 1.1% (n = 4/357) after the outbreak. This difference was statistically significant (P < 0.001).
DISCUSSION
The COVID-19 outbreak has emerged as a global concern, causing profound changes in various aspects of life, including medical care. Significant shifts have been observed in the field of otolaryngology. Analysis of surgical healthcare during the pandemic revealed a marked decrease in otolaryngological surgical cases after the COVID-19 emergency declaration.3
Consistent with our findings, recent studies on facial palsy have indicated that an increasing number of Bell’s palsy diagnoses are associated with COVID-19. Cohort and case series data from Spain and the United Kingdom demonstrated a higher risk, with a standardized incidence ratio of 1.33.4 A retrospective case-control study also suggested a link between facial palsy and COVID-19, as the symptoms aligned with SARS-CoV-2 infection.5 Furthermore, a longitudinal cohort study spanning 41 healthcare organizations reported an increased incidence of Bell’s palsy in patients with COVID-19 patients.6 A study conducted in the United Kingdom also noted a statistically significant increase in Bell's palsy cases in 2020 (3.5%) compared to 2019 (1.3%).7 These findings not only underscore the rising incidence of Bell’s palsy, but also suggest that facial palsy can manifest as the sole symptom or initial sign of COVID-19, further substantiating SARS-CoV-2 as a potential viral cause of Bell’s palsy.8,9
Contrary to these observations, studies from Turkey reported that the number of patients with facial palsy detected during the COVID-19 pandemic was similar to previous years.10,11 Another study explored the Bell’s palsy cluster around the “peaks” of the COVID-19 pandemic in the Spanish population, and did not find an increase in the incidence of Bell’s palsy cases in relation to the increase the incidence of SARS-CoV-2 infections.12
Notably, we observed that the age at which Bell’s palsy was diagnosed increased after COVID-19 from 47 to 53 years. This age trend is consistent with the findings of a large-scale Korean retrospective study.13 Aging, with its associated weakened immune system (immunosenescence), may contribute to a higher risk of Bell’s palsy during the pandemic.14,15 In addition to this dynamic process describing the changes occurring in the innate and adaptive immune systems with age, other possible factors include a combination of comorbidities in the elderly population and prioritized COVID-19 vaccination.
Elderly individuals are at greater risk due to the presence of common comorbidities such as heart disease, hypertension, diabetes, cerebrovascular disease, and respiratory issues. HSV may become reactivated in immunocompromised elderly individuals with COVID-19, potentially causing facial palsy.16 However, it is important to note that further evidence is needed to confirm these hypotheses.
However, the association between COVID-19 vaccines and Bell’s palsy remains debatable. To date, more than 5.55 billion people worldwide, accounting for roughly 72.3 percent of the global population, have received a COVID-19 vaccine.17 A French study suggested that COVID-19 vaccines could potentially contribute to Bell's palsy owing to a type 1 interferon response.18 They explained that the adverse reactions, characterized by a profound type 1 interferon response triggered by mRNA COVID-19 vaccines, resembled the response observed in patients receiving type I interferon therapy. This similarity suggests that the type I interferon response induced by vaccines could be a potential mechanism linking COVID-19 vaccines to Bell's palsy. With the surge in the COVID-19 pandemic, the elderly and high-risk individuals are strongly advised to receive COVID-19 vaccinations and booster shots.19 Some researchers have also raised concerns about the potential correlation between the increased occurrence of Bell’s palsy and COVID-19 vaccines. In our study, we did not specifically analyze vaccination status. However, our findings provide indirect evidence suggesting a potential association between the elderly patients who received the vaccine and the occurrence of facial palsy.
Additionally, we observed an increase in recurrent Bell's palsy cases following the COVID-19 outbreak, from 2.9% before the outbreak to 7.5%. Researchers have proposed a potential link between recurrent Bell's and mRNA-based vaccines.20,21 A retrospective cohort study indicated a strong association between mRNA COVID-19 vaccines and recurrent Bell’s palsy after a second vaccine dose.22
Another notable finding in our study was the reduced complete recovery rate during the COVID-19 outbreak, which decreased from 88.2% before pre-COVID-19 to 73.9% during the pandemic period. This decline coincides with a decreasing trend in steroid use during the COVID-19 pandemic. In addition, the response to steroid therapy, facial palsy grade, and six-month recovery were significantly different between the COVID-19-positive and COVID-19-negative subgroups.23 As SARS-CoV-2 has spread worldwide, hospital visits and admissions have declined steeply.24 Deferred care of this disease may lead to increased morbidity and mortality in many communities. However, it is interesting to note that the time from the onset of facial palsy to hospital arrival during COVID-19 remained at two days, which was the same as the pre-COVID-19 period in this study (P = 0.620).
The potential direct influence of SARS-CoV-2 on facial paralysis cannot be overlooked. Facial palsy has been reported as the first or sole symptom in patients with COVID-19.9,25,26 The proposed mechanisms of facial palsy related to SARS-CoV-2 include decreased blood circulation and vascular changes, leading to ischemic neuropathy and acute inflammation-induced demyelination of the facial nerve.27 Direct viral toxicity or immune-mediated mechanisms may play a role in facial nerve damage.
There is a growing body of evidence suggesting that viruses other than SARS-CoV-2 might compound this issue. Recent studies have identified a surge in HSV-1 and VZV occurrences among COVID-19 patients, emphasizing that the reactivation of these viruses in immunocompromised COVID-19 patients could further compound the risks.28,29 Determining whether SARS-CoV-2 acts as the primary instigator of Bell’s palsy or whether coinfections account for the diminished recovery rate during the pandemic remains a vital research question.
During the COVID pandemic era, there has been a noticeable increase in otalgia among patients, a symptom linked to worse prognosis and higher severity in Bell’s palsy cases.30,31,32 Zoster sine herpes (ZSH), caused by VZV, is a clinical manifestation of neuropathic pain in the absence of a rash. The suggested etiology of ZSH is that viral reactivation occurs only in the enteric nervous system, which does not project to the skin, and the severity and duration of pain worse.33 VZV reactivation without a cutaneous vesicle displays various symptoms of peripheral invasion other than into the skin, and facial palsy has been reported in 8–28% of ZSH cases.34,35 ZSH-related Bell’s palsy could explain the surge in otalgia, and analyzing the viral presence in future Bell’s palsy cases during COVID-19 may shed light on this issue. Conversely, the incidence of vertigo in patients with Bell’s palsy declined sharply during the pandemic from 18.7% to 5.1%. In a study by Choi et al.’s 2023 study13 during the COVID-19 pandemic, the occurrence of dizziness as a concomitant symptom among patients with facial palsy was reported to be 1.6%, which is lower than the 24% reported in the pre-COVID-19 period, although the difference was not statistically significant. There is a lack of reports on the clinical characteristics of facial palsy in the COVID-19 era, making it challenging to draw conclusions regarding the pathophysiological causes of increasing dizziness in the COVID-19 era. Further research is crucial to understand this shift.
During the pre- and COVID-19 pandemic phases, we observed a decline in the use of systemic steroids, intratympanic steroid injections, and antiviral medications for facial palsy treatment. This reduction likely stems from restricted hospital access and postponement of treatments during the pandemic. For example, individuals with conditions, such as diabetes, severe hypertension, gastric ulcers, or glaucoma, may receive steroids only during hospitalization or when their comorbidities are being monitored. Factors such as limitations in hospital visits and admissions due to the pandemic may encourage a more conservative approach rather than active treatment, such as the use of high-dose steroids. Additionally, concerns surrounding the use of high-dose corticosteroids, especially in the context of potential complications of COVID-19 or vaccinations, may have influenced treatment choices.
Ramsay Hunt syndrome, which is linked to VZV infection, is another area of concern. A possible connection between SARS-CoV-2 infection or COVID-19 vaccination and Ramsay Hunt syndrome has been suggested in several case reports36,37,38,39 Ramsay Hunt syndrome, accompanied by VZV meningitis following COVID-19 vaccination or post-SARS-CoV-2 infection was reported, which is extremely rare in immunocompetent individuals, and the authors suggested that viral activation of the facial nerve during the convalescent phase of COVID-19 or vaccination status might cause perturbations in immunity. While our data did not show significant Ramsay Hunt syndrome changes pre- and after the COVID-19 pandemic, understanding this relationship requires extensive epidemiological research.
This study had some limitations. First, we did not conduct viral antigen tests for HSV-1, VZV, or SARS-CoV-2 in patients with facial palsy, which may have offered more profound insight into the viral origin of facial palsy in the context of COVID-19. Second, our analysis primarily identified associations and trends, but did not conclusively establish causal relationships between COVID-19 and facial palsy. Large controlled epidemiological studies are essential for further investigation of causation. Third, although we mentioned anecdotally reported cases of facial palsy associated with the adverse effects of COVID-19 vaccines, we did not provide comprehensive data on the vaccination status and characteristics of these cases. Fourth, we did not investigate the incidence rate, that is, the number of cases of the disease in the entire population, but rather the number of diagnoses made at the same hospital during the same period in the past and present. Therefore, verifying the accurate incidence rate by considering the total number of patients would provide a clearer insight into the relationship between COVID-19 and facial palsy.
This could have added depth to our analysis. Further studies are needed to comprehensively assess the relationship between vaccination and facial palsy. Furthermore, potential selection or reporting biases in our data collection and analysis were not addressed, which may have affected the generalizability of our findings. It is important to consider these biases when interpreting results. Finally, the absence of laboratory findings for recent viral infections and imaging studies of the temporal bone limit our ability to comprehensively understand the underlying facial nerve pathologies during the COVID-19 pandemic. We also did not investigate the specifics of vaccination status, such as vaccine type or booster dose, in patients with facial palsy. A detailed assessment of vaccination status could provide relevant evidence regarding the relationship between viral activation in facial palsy and vaccination.
In conclusion, our analysis of 943 acute peripheral facial palsy patients with APFP revealed marked changes in the clinical manifestations and treatment of the COVID-19 outbreak. We noted an uptick in the incidence of Bell’s palsy, especially in elderly patients with diabetes, and observed a decline in full recovery rates along with an increase in recurrent cases. In contrast, patients with Ramsay Hunt syndrome displayed minimal variation in clinical outcomes. Collectively, these observations highlighted the potential influence of the COVID-19 pandemic on facial palsy presentation and management.
ACKNOWLEDGMENTS
The authors thank all the members of the Korean Facial Nerve Disorder Subcommittee for their help and support.
Footnotes
Funding: This study was supported by the Soonchunhyang University Research Fund for J. D. L. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1F1A1072918 for S. H. K.). This work was supported by the Industrial Strategic Technology Development Program (2023, P0023215, the Commercialization of Soricle, and tinnitus treatment platform based on non-invasive VNS and CBT for solving unmet medical needs of H.Y.L.).
Disclosure: The authors have no potential conflicts of interest to disclose.
- Data curation: Lee SA, Jeong J, Chung JH, Kim J, Jun BC, Yeo SG, Kim SH, Lee JD.
- Formal analysis: Kwak MY, Lee HY, Kim J, Jun BC, Yeo SG, Lee JD.
- Funding acquisition: Lee HY.
- Methodology: Kwak MY, Lee HY, Lee SA, Jeong J, Kim J, Jun BC, Kim SH, Lee JD.
- Resources: Kwak MY, Lee SA, Jeong J, Chung JH, Jun BC.
- Software: Lee HY, Chung JH.
- Supervision: Jun BC, Yeo SG, Kim SH, Lee JD.
- Validation: Lee HY, Kim J.
- Visualization: Lee HY.
- Writing - original draft: Kwak MY, Lee HY.
- Writing - review & editing: Kwak MY, Lee HY, Kim SH, Lee JD.
References
- 1.World Health Organization. COVID-19 Weekly Epidemiological Update. Edition 150. Geneva, Switzerland: World Health Organization; 2023. [Google Scholar]
- 2.Egilmez OK, Gündoğan ME, Yılmaz MS, Güven M. Can COVID-19 cause peripheral facial nerve palsy? SN Compr Clin Med. 2021;3(8):1707–1713. doi: 10.1007/s42399-021-00967-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Okuno T, Takada D, Shin JH, Morishita T, Itoshima H, Kunisawa S, et al. Surgical volume reduction and the announcement of triage during the 1st wave of the COVID-19 pandemic in Japan: a cohort study using an interrupted time series analysis. Surg Today. 2021;51(11):1843–1850. doi: 10.1007/s00595-021-02286-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Li X, Raventós B, Roel E, Pistillo A, Martinez-Hernandez E, Delmestri A, et al. Association between covid-19 vaccination, SARS-CoV-2 infection, and risk of immune mediated neurological events: population based cohort and self-controlled case series analysis. BMJ. 2022;376:e068373. doi: 10.1136/bmj-2021-068373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Codeluppi L, Venturelli F, Rossi J, Fasano A, Toschi G, Pacillo F, et al. Facial palsy during the COVID-19 pandemic. Brain Behav. 2021;11(1):e01939. doi: 10.1002/brb3.1939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tamaki A, Cabrera CI, Li S, Rabbani C, Thuener JE, Rezaee RP, et al. Incidence of Bell Palsy in patients with COVID-19. JAMA Otolaryngol Head Neck Surg. 2021;147(8):767–768. doi: 10.1001/jamaoto.2021.1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zammit M, Markey A, Webb C. A rise in facial nerve palsies during the coronavirus disease 2019 pandemic. J Laryngol Otol. 2020;134(10):1–4. doi: 10.1017/S0022215120002121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sevil E, Değer Kulaksiz B, Islamoglu A. Association between the inflammatory parameters and prognosis of Bell’s Palsy. NORTHWESTERN MEDICAL JOURNAL. 2021;1(2):35–41. [Google Scholar]
- 9.Gupta KK, Balai E, Tang HT, Ahmed AA, Doshi JR. Comparing the use of high-dose to standard-dose corticosteroids for the treatment of Bell’s Palsy in adults-a systematic review and meta-analysis. Otol Neurotol. 2023;44(4):310–316. doi: 10.1097/MAO.0000000000003823. [DOI] [PubMed] [Google Scholar]
- 10.Mutlu A, Kalcioglu MT, Gunduz AY, Bakici B, Yilmaz U, Cag Y. Does the SARS-CoV-2 pandemic really increase the frequency of peripheral facial palsy? Am J Otolaryngol. 2021;42(5):103032. doi: 10.1016/j.amjoto.2021.103032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aslan M, Çiçek MT. Can isolated sudden sensorineural hearing loss (SSNHL) and idiopathic acute facial paralysis (Bell’s Palsy) be symptoms of COVID-19? Am J Otolaryngol. 2021;42(5):103129. doi: 10.1016/j.amjoto.2021.103129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Martin-Villares C, Alba JR, Gonzalez-Gimeno MJ. Data from 235 cases of Bell’s Palsy during COVID-19 pandemic: were there clusters of facial palsy? Neuroepidemiology. 2021;55(6):495–496. doi: 10.1159/000518671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Choi GW, Yon DK, Choi YS, Lee J, Park KH, Lee YJ, et al. Comparing the clinical manifestations of Bell’s Palsy between pre-COVID-19 pandemic and COVID-19 pandemic periods. J Clin Med. 2023;12(4):1700. doi: 10.3390/jcm12041700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nikolich-Žugich J. The twilight of immunity: emerging concepts in aging of the immune system. Nat Immunol. 2018;19(1):10–19. doi: 10.1038/s41590-017-0006-x. [DOI] [PubMed] [Google Scholar]
- 15.Aviv-Sharon E, Aharoni A. Generalized logistic growth modeling of the COVID-19 pandemic in Asia. Infect Dis Model. 2020;5:502–509. doi: 10.1016/j.idm.2020.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shanshal M, Ahmed HS. COVID-19 and herpes simplex virus infection: a cross-sectional study. Cureus. 2021;13(9):e18022. doi: 10.7759/cureus.18022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bayani F, Hashkavaei NS, Arjmand S, Rezaei S, Uskoković V, Alijanianzadeh M, et al. An overview of the vaccine platforms to combat COVID-19 with a focus on the subunit vaccines. Prog Biophys Mol Biol. 2023;178:32–49. doi: 10.1016/j.pbiomolbio.2023.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Soeiro T, Salvo F, Pariente A, Grandvuillemin A, Jonville-Béra AP, Micallef J. Type I interferons as the potential mechanism linking mRNA COVID-19 vaccines to Bell’s Palsy. Therapie. 2021;76(4):365–367. doi: 10.1016/j.therap.2021.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nham E, Song JY, Noh JY, Cheong HJ, Kim WJ. COVID-19 vaccination in Korea: past, present, and the way forward. J Korean Med Sci. 2022;37(47):e351. doi: 10.3346/jkms.2022.37.e351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhang H, Sanchez Gomez D, Repajic M, Liu AK. Another case of Bell’s Palsy recurrence after Pfizer-BioNTech COVID-19 vaccination. Cureus. 2022;14(7):e27422. doi: 10.7759/cureus.27422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yu BY, Cen LS, Chen T, Yang TH. Bell’s Palsy after inactivated COVID-19 vaccination in a patient with history of recurrent Bell’s Palsy: a case report. World J Clin Cases. 2021;9(27):8274–8279. doi: 10.12998/wjcc.v9.i27.8274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Repajic M, Lai XL, Xu P, Liu A. Bell’s Palsy after second dose of Pfizer COVID-19 vaccination in a patient with history of recurrent Bell’s Palsy. Brain Behav Immun Health. 2021;13:100217. doi: 10.1016/j.bbih.2021.100217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Uysal HA, Güllüoğlu H. Comparison of facial palsy cases before and during the pandemic coronavirus disease-2019. Med J Bakirkoy. 2023;19(2):156–162. [Google Scholar]
- 24.Nourazari S, Davis SR, Granovsky R, Austin R, Straff DJ, Joseph JW, et al. Decreased hospital admissions through emergency departments during the COVID-19 pandemic. Am J Emerg Med. 2021;42:203–210. doi: 10.1016/j.ajem.2020.11.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lima MA, Silva MT, Soares CN, Coutinho R, Oliveira HS, Afonso L, et al. Peripheral facial nerve palsy associated with COVID-19. J Neurovirol. 2020;26(6):941–944. doi: 10.1007/s13365-020-00912-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Islamoglu Y, Bercin S, Aydogan S, Sener A, Tanriverdi F, Gunaydin GP, et al. Assessment of SARS-CoV-2 in the cerumen of COVID-19-positive patients. Ear Nose Throat J. 2021;100(2 Suppl):155S–157S. doi: 10.1177/0145561320966067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang J, Lu H, Zeng H, Zhang S, Du Q, Jiang T, et al. The differential psychological distress of populations affected by the COVID-19 pandemic. Brain Behav Immun. 2020;87:49–50. doi: 10.1016/j.bbi.2020.04.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Katz J, Yue S, Xue W. Herpes simplex and herpes zoster viruses in COVID-19 patients. Ir J Med Sci. 2022;191(3):1093–1097. doi: 10.1007/s11845-021-02714-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Xu R, Zhou Y, Cai L, Wang L, Han J, Yang X, et al. Co-reactivation of the human herpesvirus alpha subfamily (herpes simplex virus-1 and varicella zoster virus) in a critically ill patient with COVID-19. Br J Dermatol. 2020;183(6):1145–1147. doi: 10.1111/bjd.19484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Peitersen E. Bell’s Palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;122(549):4–30. [PubMed] [Google Scholar]
- 31.Katusic SK, Beard CM, Wiederholt WC, Bergstralh EJ, Kurland LT. Incidence, clinical features, and prognosis in Bell’s Palsy, Rochester, Minnesota, 1968–1982. Ann Neurol. 1986;20(5):622–627. doi: 10.1002/ana.410200511. [DOI] [PubMed] [Google Scholar]
- 32.Kopitović A, Katanić F, Kalember S, Simić S, Vico N, Sekulić S. Bell’s Palsy-retroauricular pain threshold. Medicina (Kaunas) 2021;57(3):263. doi: 10.3390/medicina57030263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lee HY, Kim MG, Park DC, Park MS, Byun JY, Yeo SG. Zoster sine herpete causing facial palsy. Am J Otolaryngol. 2012;33(5):565–571. doi: 10.1016/j.amjoto.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 34.Furuta Y, Ohtani F, Aizawa H, Fukuda S, Kawabata H, Bergström T. Varicella-zoster virus reactivation is an important cause of acute peripheral facial paralysis in children. Pediatr Infect Dis J. 2005;24(2):97–101. doi: 10.1097/01.inf.0000151032.16639.9c. [DOI] [PubMed] [Google Scholar]
- 35.Hato N, Sawai N, Teraoka M, Wakisaka H, Takahashi H, Hinohira Y, et al. Valacyclovir for the treatment of Bell’s Palsy. Expert Opin Pharmacother. 2008;9(14):2531–2536. doi: 10.1517/14656566.9.14.2531. [DOI] [PubMed] [Google Scholar]
- 36.Chu WK, Lin KY, Sun HY, Chen YC, Cheng A. Herpes zoster aseptic meningitis and Ramsay Hunt syndrome in an immunocompetent young adult post mild COVID-19 - a coincidence? J Microbiol Immunol Infect. 2023;56(5):1114–1115. doi: 10.1016/j.jmii.2023.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Woo CJ, Chou OH, Cheung BM. Ramsay Hunt syndrome following COVID-19 vaccination. Postgrad Med J. 2022;98(1164):738–739. doi: 10.1136/postgradmedj-2021-141022. [DOI] [PubMed] [Google Scholar]
- 38.Lakhoua G, Charfi O, Dabbeche S, Zaiem A, Kastalli S, Daghfous R, et al. An atypical Ramsey Hunt syndrome after covid 19 immunization. Therapie. 2023;78(4):442–443. doi: 10.1016/j.therap.2022.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hwang YS, Kim YS, Shin BS, Kang HG. Two cases of Ramsay-Hunt syndrome following varicella zoster viral meningitis in young immunocompetent men: case reports. BMC Neurol. 2023;23(1):43. doi: 10.1186/s12883-023-03074-0. [DOI] [PMC free article] [PubMed] [Google Scholar]