

Abstract
Introduction:
Head and neck cancer is common in several parts of the world. It is sixth most prevalent neoplasms in the world. Approximately 900 000 cases diagnosed worldwide per year. It has good prognosis when timely diagnosed and treated appropriately.
Methods:
This was a retrospective study carried out in the Department of ENT-HNS of Shree Birendra Hospital, Chhauni, Kathmandu from May 2022 to April 2023. All histopathologically proven malignant cases of head and neck region were included in the study. Data were entered in Microsoft excel and managed in SPSS version 22. Analysis was done in the form of percentage and proportion and represented as table where necessary. The study has been registerd in clinical trials and has been reported in line with the STROCSS criteria.
Results:
Total 76 patients were analyzed. Age ranged from 17 to 84 years and the most common age group presenting with head and neck cancer was 61–80 years. The most common malignancy was laryngeal cancer (34%) followed by thyroid malignancies (29%). Squamous cell carcinoma was the commonest histological type (48%). Surgery with postoperative radiotherapy (RT)/radioactive iodine (RAI) was found to be the commonest treatment modality.
Conclusions:
Head and neck cancers are not uncommon and majority of patients present late with advanced stage cancer. Hence, public awareness, early diagnosis with cost-effective treatment and regular follow-up are needed to improve outcomes of these patients in our society.
Keywords: chemotherapy, head and neck carcinoma, radiotherapy
Introduction
Highlights
Head and neck malignancies are the sixth most prevalent neoplasms in the world.
Laryngeal malignancies were found to be the commonest malignancy (34%). Among them glottis carcinoma was found to be the commonest subsite.
Thyroid malignancies (29%) were second most common malignancies.
Squamous cell carcinoma (48%) was the commonest histological type of head and neck malignancies.
Head and neck cancer is common in several parts of the world. It is the sixth most prevalent neoplasms in the world1. Approximately 900 000 cases diagnosed worldwide per year2. It has good prognosis when timely diagnosed and treated appropriately. Head and neck cancers are the malignant neoplasms that develops in oral cavity, nasal cavities, paranasal sinuses, nasopharynx, oropharynx, hypopharynx, ear, scalp, salivary gland and neck3. Worldwide head and neck cancer accounts for nearly 900 000 cases and over 400 000 deaths annually2. Males are affected more than female with the ratio of 2:1–4:12. As per the world wise distribution, mouth and tongue cancers are more common in Indian subcontinent, nasopharyngeal carcinoma is more common in Hongkong, laryngeal carcinoma is 50% higher in African-American men4,5. Head and neck cancer affect fundamental functions including eating, drinking, speaking, respiration, hearing, vision, taste and smelling6. Prognosis has improved in past 30 years with early diagnosis and treatment1. Head and neck cancer rate are traditionally linked to public health issue. In this study we describe the clinicopathological type, staging and different treatment modalities of head and neck cancer. Thereby helps in reporting the epidemiology of head and neck cancer among Nepalese population. This study aimed to evaluate the pattern and report epidemiology of head and neck cancer in tertiary care centre of Nepal.
Materials and methods
This was a retrospective, cohort study conducted at the department of ENT-Head and Neck surgery department of tertiary hospital. Ethical clearance was obtained from Institutional Review Committee (IRC). Data were collected from the medical records of head and neck cancer (HNC) patients who underwent treatment between May 2022 and April 2023. Biopsy proven HNCs were included in the study. Patient records with incomplete data were excluded. Data considered of demographic details of age, sex, diagnosis, subsite specific HNCs, treatment modality and histopathology. The data were analyzed using SPSS version 22. Pearson’s χ2 test was applied and P value less than 0.05 was considered statistically significant.
Registration Unique Identifying number (UIN) of article is NCT06152055 https://classic.clinicaltrials.gov/ct2/show/NCT06152055.
This study has been reported in line with the STROCSS criteria7.
Results
Total of 76 patients (51 males and 25 females) were included in this study. Overall male: female ratio was 2.04:1. Head and neck malignancies were found to be common amongst males and laryngeal malignancy was the commonest (29%) whereas thyroid malignancies were female predominant (15%). The age ranged from 17 to 84 years. Highest number (n=27) of HNCs was present in the age group of 61–80 years (Tables 1 and 2).
Table 1.
Age distribution of HNC patients (n=76)
| Age group(Y) | Number of patients (Percentage), n (%) |
|---|---|
| <20 | 1 (1) |
| 20–40 | 20 (26) |
| 41–60 | 20 (26) |
| 61–80 | 27 (36) |
| >80 | 8 (11) |
| Total | 76 (100) |
HNC, head and neck cancer.
Table 2.
Distribution of HNCs according to subsite (n=76)
| Subsite | Number (Percentage), n (%) | P |
|---|---|---|
| Larynx | 26 (34) | |
| Thyroid | 22 (29) | |
| Parotid | 6 (8) | |
| Oral cavity | 8 (10) | 0.015 |
| Pharynx | 8 (10) | |
| Sinonasal | 2 (3) | |
| Lymphoma | 3 (4) | |
| External auditory canal | 1 (2) | |
| Total | 76 (100) |
HNC, head and neck cancer.
Laryngeal malignancies were found to be the commonest malignancy (34%). Among them glottis carcinoma was found to be the commonest subsite (Fig. 1).
Figure 1.
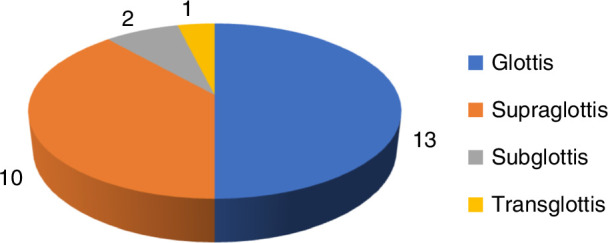
Sitewise distribution of laryngeal malignancy.
Thyroid malignancies (29%) were second most common malignancies. Among them (21%) were papillary, (5%) follicular and (1%) medullary and (1%) anaplastic. In our study squamous cell carcinoma (48%) was found to be the commonest histological type of head and neck malignancies (Table 3).
Table 3.
Histopathology of HNCs (n=76)
| Type | Number (n=76) (Percentage), n (%) |
|---|---|
| SCC | 36 (48) |
| Papillary CA | 16 (21) |
| Follicular | 4 (5) |
| Mucoepidermoid | 5 (7) |
| Non-Hodgkin’s | 3 (4) |
| Non-keratinizing (undifferentiated type) | 3 (4) |
| Adeno carcinoma | 2 (3) |
| Verrucous | 2 (3) |
| Carcinoma in situ | 1 (1) |
| Medullary | 1 (1) |
| Sebacious CA carcinoma | 1 (1) |
| Milanoma (spindle cell variant) | 1 (1) |
| Anaplastic | 1 (1) |
| Total | 76 (100) |
CA, Carcinoma; HNC, head and neck cancer; SCC, Squamous Cell Carcinoma.
TNM staging was done in all patients prior to definite treatment. Among 76 patients, stage III (32) being the commonest presentation. The overall staging of these patients is shown in (Fig. 2).
Figure 2.
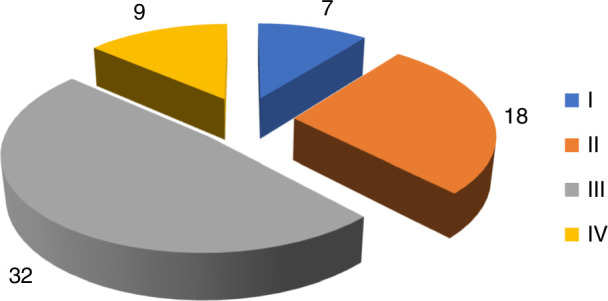
Overall staging of head and neck cancer (HNC) malignancies.
Following staging, all patients were advised for definitive or palliative treatment. The overall treatment modalities of these patients are shown in (Table 4).
Table 4.
Treatment provided to HNC patients (n=76)
| Treatment modality | Number (Percentage), n (%) |
|---|---|
| Surgery | 12 (16) |
| Surgery+RT/RAI | 26 (34) |
| Surgery+CTRT | 16 (21) |
| CTRT | 6 (8) |
| Palliative chemotherapy | 7 (9) |
| Refuse treatment | 9 (12) |
| Total | 76 (100) |
CTRT, chemoradiotherapy; HNC, head and neck cancer; RAI, radioactive iodine; RT, radiotherapy.
Twenty-six (34%) patients required surgery with postoperative radiotherapy (RT) or radioactive iodine (RAI) ablation for thyroid cancers was found to be the commonest treatment modality for the management of HNCs. Sixteen (21%) required surgery with postoperative chemoradiotherapy (CTRT). Twelve (16%) patients underwent surgery as a single treatment modality. Among surgery thyroidectomy was the commonest surgery. Six (8%) patients received upfront chemo radiation and 7 (9%) received palliative chemotherapy. Nine (12%) patients refused treatment.
Discussion
In this study head and neck malignancies were more common among male (67%) leading overall male and female ratio 2.04:1. Among them laryngeal malignancies were found as male predominant (29%) whereas thyroid malignancies were female predominate (15%) This findings were similar with a study conducted by Warkinson et al.8, Shaheen et al.9 and Baskota et al.10
Most of the patients in our study were in the age group of 61–80years which is similar to the study by Thakur et al.11 and Lasrado et al.12. In contrast most patients were between 41 and 60 years in the study by Baskota et al.9, Mahaseth et al.13 and Funk et al.14.
In our study laryngeal malignancies were found to be the commonest malignancies (34%) in HNC. Among laryngeal malignancies, glottis carcinoma was found to be the commonest followed by supraglottic cancer. These findings are similar to the findings in a study done by Baskota el10. This is in contrast to a study done by Thakur et al.11 where thyroid carcinoma was the commonest. Similarly a study done by Mahaseth et al.13 and Dixit et al.15 oral cavity carcinoma was the commonest.
The second most commonest malignancies in our study was thyroid malignancies(29%) which was similar to the study done by Mahaseth et al.13 and Dixit et al.15. In contrast to our study, Baskota et al.10 study concluded pharyngeal malignancies as the second commonest malignancies. Whereas our study was similar with a study done by Baskota et al.10 which showed ear malignancies as the least common.
Diverse histological types of tumours are found in the head and neck region. More than 90% of head and neck cancers are of epithelial origin, of which squamous cell carcinoma constitutes the greatest majority. Other histological types include lymphomas, blastomas, sarcomas and neuroendocrine tumours3.
In our study, the commonest histopathological type squamous cell carcinoma was presented in (48%) malignancies which are lesser than in the study by Dixit et al.15 and Thapa et al.16. The second common histopathological type in our study was papillary variant of thyroid carcinoma presented in (21%) followed by follicular variant which was similar to a study done by Mahaseth et al.13, Baskota et al.10 and Dixit et al.15. In contrast to this follicular variant was the commonest in the study by Thapa et al.16.
Among 76 patients’ stage III was the commonest presentation in our study. This finding is similar to the other studies done in underdeveloped and developed countries as the patients seek medical help in advanced stage. In developed countries this finding varies as patients seek medical help as early as possible17.
In our study surgery with adjuvant postoperative radiotherapy/RAI was received by 26 (34%) patients followed by surgery with CTRT in 16 (21%) patients. None of the patient received RT as the primary treatment. Multimodality treatment was due to advanced stage presentation which contradicts with that of developed countries where radiotherapy was the commonest treatment modality due to early detection of the disease18.
Conclusions
Head and neck cancers are not uncommon. The prognosis depends on clinical stage at the time of presentation. Hence, identification of high-risk populations, precancerous lesions and early diagnosis leads to better treatment outcomes.
Ethical approval
Ethical clearance was obtained from Institutional Review Committee (IRC), Nepalese Army Imstitute of Health Sciences.
Consent
Written informed consent was obtained from the patients and patient’s parents/legal guardian for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Sources of funding
The study didn’t receive any grant from funding agencies in the public, commercial or not-for-profit sectors.
Author contribution
R.K.: conceptualization; methodology; writing—original draft; writing—review and editing. A.M.: data collection, analysis, discussion, revising and editing manuscript. R.K.M.: data collection, methodology, revising and editing manuscript. R.B.: data curation, methodology, revising and editing manuscript. S.R.D.: data curation and visualization and editing manuscript. Y.A.: data curation and visualization and editing manuscript. All authors were involved in manuscript drafting and revising and approved the final version.
Conflicts of interest disclosure
The author declares no conflicts of interest.
Research registration unique identifying number (UIN)
Registry: Clinicaltrials.gov.
Unique Identifying number: NCT06152055.
Hyperlink to the registration. https://clinicaltrials.gov/study/NCT06152055.
Guarantor
Anupama Marasini.
Data availability statement
Data those included are publicly available.
Provenance and review
Not Commissioned, externally peer-reviewed.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article
Published online 6 March 2024
Contributor Information
Reeba Karki, Email: karkireeba@gmail.com.
Anupama Marasini, Email: marasinianupama@gmail.com.
Rajeev Kumar Mahaseth, Email: drajeevmahaseth@gmail.com.
Ranishma Bista, Email: ranishmab@gmail.com.
Yuvraj Adhikari, Email: yuvraj.adhikari06@gmail.com.
References
- 1.Chin D, Boyle GM, Porceddu S, et al. Head and neck cancer: past, present and future. Expert Rev Anticancer Ther 2006;6:1111–1118. [DOI] [PubMed] [Google Scholar]
- 2.Stenson KM, Brockstein BE, Ross ME. Epidemiology and risk factors for head and neck cancer. UpToDate. 2014. https://medilib.ir/uptodate/show/3390
- 3.Gilyoma JM, Rambau PF, Masalu N, et al. Head and neck cancers: a clinico-pathological profile and management challenges in a resource-limited setting. BMC Res Notes 2015;8:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bray F, Ren JS, Masuyer E, et al. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer 2013;132:1133–1145. [DOI] [PubMed] [Google Scholar]
- 5.Lambert R, Sauvaget C, de Camargo Cancela M, et al. Epidemiology of cancer from the oral cavity and oropharynx. Eur J Gastroenterol Hepatol 2011;23:633–641. [DOI] [PubMed] [Google Scholar]
- 6.Nwawolo CC, Ajekigbe AT, Oyeneyin JO, et al. Pattern of head and neck cancers among Nigerians in Lagos. West Afr J Med 2001;20:111–116. [PubMed] [Google Scholar]
- 7.Mathew G, Agha R, for the STROCSS Group . STROCSS 2021: Strengthening the Reporting of cohort, cross-sectional and case-control studies in Surgery. Int J Surg 2021;96:10616. [DOI] [PubMed] [Google Scholar]
- 8.Warkinson JC. Stell and Maran’s Head and Neck Surgery, 4th ed. Butterworth Heinemann; 2000. [Google Scholar]
- 9.Shaheen OH. Scott Brown’s Otolaryngology (Laryngology and Head and Neck Surgery). Butterworths Heinemann; 1997;4. [Google Scholar]
- 10.Baskota DK, Agrawal R, Prasad R, et al. Distribution of malignancies in head and neck regions and their management. J Nepal Med Assoc 2005;44:68–72. [PubMed] [Google Scholar]
- 11.Thakur SK, Ghimire N, Acharya R, et al. The intraoperative pathological findings in cases of chronic suppurative otitis media with central perforation of tympanic membrane at a tertiary care centre in Eastern Nepal. Asian J Med Sci 2017;8:42–47. [Google Scholar]
- 12.Lasrado S, Prabhu P, Kakria A, et al. Clinicopathological profile of head and neck cancers in the Western development region, Nepal: a 4-year snapshot. Asian Pac J Cancer Prev 2012;13:6059–6062. [DOI] [PubMed] [Google Scholar]
- 13.Mahaseth RK, Kc S, Dutta VB, et al. Clinicohistopathological Profile of Head and Neck Cancers During COVID-19 Pandemic in a Tertiary Care Hospital. JMEC; 2021. [Google Scholar]
- 14.Funk GF, Karnell LH, Robinson RA, et al. Presentation, treatment, and outcome of oral cavity cancer: A national cancer data base report. Head Neck 2002;24:165–180. [DOI] [PubMed] [Google Scholar]
- 15.Dixit S, Upadhyaya C, Humagain M, et al. Clinico-histopathological survey of head and neck cancer at tertiary health care centre-Dhulikhel Hospital. Kathmandu Univ Med J 2016;14:167–171. [PubMed] [Google Scholar]
- 16.Thapa N, Jha AK, Rijal JP, et al. Study on head and neck tumours presented in ENT OPD of Nepal Medical College Teaching Hospital. Nepal Med Coll J NMCJ 2003;5:79–81. [PubMed] [Google Scholar]
- 17.Hong WK, Lippman SM, Wolf GT. Recent advances in head and neck cancer—larynx preservation and cancer chemoprevention: the Seventeenth Annual Richard and Hinda Rosenthal Foundation Award Lecture. Cancer Res 1993;53:5113–5120. [PubMed] [Google Scholar]
- 18.Garden AS, Morrison WH, Ang KK, et al. Hyperfractionated radiation in the treatment of squamous cell carcinomas of the head and neck: a comparison of two fractionation schedules. Int J Radiat Oncol Biol Phys 1995;31:493–502. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data those included are publicly available.