

Abstract
Background:
Based on evidences, there has been no study conducted on the effects of emotional freedom techniques on Iranian medical students. Therefore, the present study aims to investigate the impact of emotional freedom techniques on examination anxiety in Iranian nursing and allied students.
Methods:
This randomized controlled clinical trial study was conducted in 2021. The sample included students from the School of Nursing and Midwifery and the School of Paramedical Sciences enroled from the second to eighth semesters. Based on inclusion criteria, 30 students were assigned to each group. The test anxiety questionnaire was utilized to assess the test anxiety of students. The educational sessions in the intervention group were structured according to the Church’s educational package and were delivered in six non-face-to-face (online) sessions, each lasting 45 min, once a week. In the control group, no intervention was implemented. All statistical analyses were performed using IBM SPSS Statistics software version 24 (IBM SPSS Statistics).
Results:
The mean age of students in the intervention and control groups were 25.22±1.85 and 22.80±1.80 years, respectively. After the intervention, the mean examination anxiety in the experimental group (50.88) significantly decreased to within the moderate range (25–75), compared to the mean examination anxiety in the control group (65.36) within the same range (P<0.001). Furthermore, the ANCOVA analysis indicated that the group and examination anxiety before the intervention were statistically significant.
Conclusion:
This positive impact on test anxiety is particularly promising for medical sciences students, who often endure heightened stress levels due to the rigorous nature of their studies and the demands of their profession.
Keywords: anxiety, Iran, students, test anxiety
Introduction
Highlights
No study has been conducted on the effects of emotional freedom techniques (EFT) on the test anxiety of students in Iran.
The mean examination anxiety after the intervention in the experiment group was statistically significantly lower within the moderate range.
Anxiety is a crucial term for describing human behaviours. It refers to a state in which several physiological reactions occur, accompanied by emotions such as distress, worry, and depression in various scenarios. It is a situation in which an individual feels threatened1.
Examination anxiety is a form of situational anxiety, and it is a significant biopsychological factor that impacts the health and academic performance of students throughout their educational journey. While moderate levels of anxiety can potentially boost creativity among students, excessive anxiety levels can hinder concentration, attention, and learning. This may result in difficulties with verbal activities and a decline in academic performance2.
Examination anxiety consists of two main dimensions: the emotional and cognitive elements3. Research in the field has indicated that the cognitive aspect of examination anxiety significantly influences examination outcomes4, impacting both regular classroom examinations5 and even less consequential laboratory examinations6. Individuals experience examination anxiety throughout all stages of the examination process, including examination preparation7, examination performance8, and self-assessment of the examination9.
Drawing from the Social Cognitive Theory by Bandura, which posits that behaviour, cognition, and environmental factors interact reciprocally to influence learning and behaviour, we recognize that test anxiety can be affected by various contextual factors within educational settings. Nursing, Midwifery, and Paramedical Sciences students share similar academic environments and stressors, making them pertinent subjects for investigating interventions such as emotional freedom techniques (EFT) in managing test anxiety10. Secondly, considering the Transactional Model of Stress and Coping by Lazarus and Folkman, which emphasizes the dynamic interplay between individuals and their environment in appraising and coping with stressors, our study acknowledges that test anxiety is a multifaceted phenomenon influenced by personal, situational, and contextual factors11.
The nursing curriculum includes challenging courses, difficult examinations, and sustained pressure to achieve higher grades in a competitive environment12. Nursing students encounter stressful situations (particularly during clinical rotations) throughout their academic journey. Clinical education is one of the initial steps toward acquiring professional skills, but it often induces significant stress in students. Stressors reported by nursing students include monitoring the patient’s condition, receiving critiques from instructors, and fearing making mistakes during patient care13.
The Clinical Skills Center, designed to prepare students for clinical practice, provides a secure care environment to bridge the gap between theory and clinical application. Nowadays, almost all universities utilize structured clinical examinations to assess the professional competence learned in clinical skills centres14. The nature of anxiety provoked by structured clinical examinations is still a subject of debate15. Examination anxiety may arise from insufficient preparation, dissatisfaction with examination conditions despite adequate knowledge of the subject matter, or misunderstanding of the skills required for examination performance16.
The findings from a systematic review indicate that examination anxiety affects around 30% of nursing students, significantly impacting their academic performance and overall well-being. This study reported significant effects of various treatments, such as hypnotherapy and aromatherapy for relaxation, in reducing examination stress. Furthermore, the results indicated that examination anxiety has multiple effects on the success of nursing students and is a determinant factor in their success within this population17.
In recent years, numerous clinical trials on EFT as a treatment for emotional distress have been conducted17,18. EFT, or emotional freedom techniques, is an evidence-based technique that blends elements of cognitive therapy with tapping on specific acupressure and acupuncture points using fingertips. The integration of these components has demonstrated effectiveness in alleviating psychological conditions such as stress, anxiety, fear, depression, post-traumatic stress disorder (PTSD), as well as reducing physical symptoms like pain, fibromyalgia, and traumatic brain injury19.
Moreover, this technique has been examined across diverse university student populations as a means of stress reduction. The findings suggest that EFT is an effective method for diminishing examination anxiety and enhancing academic performance19,20.
Based on the literature review, no study has been conducted on the effects of EFT on test anxiety among students in Iran. Test anxiety among medical sciences students, particularly in the Iranian context, presents a significant impediment to academic performance and overall well-being. Despite the prevalence of this issue, there is a shortage of research exploring effective interventions tailored to this specific demographic. Our study seeks to bridge this gap by investigating the potential efficacy of EFT as a viable intervention for alleviating test anxiety in Iranian medical sciences students. By elucidating this gap and articulating our objective to provide an evidence-based solution to mitigate test anxiety, we aim to contribute meaningfully to student mental health and academic performance enhancement. Hence, the current research seeks to explore the effects of EFT on test anxiety among Iranian students studying nursing and allied health disciplines.
Materials and methods
This randomized controlled clinical trial (RCT) study was conducted to investigate the impact of EFT on examination anxiety among nursing and paramedical students at Kerman University of Medical Sciences in 2021. The study population included students from the School of Nursing and Midwifery and the School of Paramedical Sciences (Radiology, Operating Room, Laboratory Sciences, Anesthesia, Physiotherapy) enroled from the second to eighth semesters.
Sample size and criteria
The required sample size, with a confidence level of 95% and a test power of 80%, was calculated using Dawson Church’s formula21, resulting in 28 individuals in each group. Considering a 10% potential dropout rate, the final sample size was determined to be 30 individuals per group. Inclusion criteria for the study included being a student enroled from the second to eighth semesters, not having previously received this intervention, and obtaining a score higher than the average on the state and trait anxiety questionnaire. Exclusion criteria involved concurrent use of tranquilizers or anti-anxiety medications during the intervention, self-reported heart or respiratory diseases, absenteeism of more than two sessions in the intervention sessions, and participation in psychotherapeutic interventions simultaneous with the current study.
Students meeting the inclusion criteria were enroled using an available sampling method. Subsequently, a stratified random allocation method was employed to divide them into two groups: intervention and control. The samples were categorized into two groups based on gender and age (±2 years). In other words, the first sample was randomly assigned (using drawing lots) to either the intervention or control group. Subsequently, samples were allocated to each group based on matching variables while adhering to random assignment conditions.
Scales
The test anxiety questionnaire (TAI), designed and validated by Aboighasemi et al.22 comprises 25 items, and respondents provide answers based on a 5-point Likert scale. The spectrum used in the questionnaire includes never, rarely, sometimes, often, and always. Scores ranging from 1 to 25 indicate poor levels of the variable in the population, while scores from 26 to 75 suggest moderate levels, and scores of 76 and above represent excellent levels. The reliability of this instrument, calculated on the students in this study, was determined using the Cronbach’s alpha method (α=0.89).
Study procedure
To conduct the study, after obtaining ethical approval from the Ethics Committee of Kerman University of Medical Sciences and a clinical trial registration code from the Iranian Registry of Clinical Trials, the researcher visited the research environment. Eligible students were provided with information about the nature of the study, the number of sessions, and the training process, emphasizing that their information would remain confidential and anonymous. After obtaining the necessary permissions and obtaining written informed consent from the students, each participant initially completed a demographic and background information questionnaire.
Subsequently, based on the entry conditions and samples, participants were randomly assigned to either the intervention or control group through a randomized drawing. The examination anxiety questionnaire was then completed by both groups. The intervention group received EFT intervention once a week on a fixed day. The questionnaire was administered once more by both groups during the final session and then repeated for follow-up 2 months later.
Stages of the study
The educational sessions in the intervention group were based on the Church’s educational package21 and were delivered in 6 non-face-to-face (online) sessions, each lasting 45 min, once a week. In the control group, no intervention was conducted. The sessions were organized as follows:
Session 1: During the first session, the therapist established a therapeutic relationship with the student and provided necessary information about the number and duration of sessions. Symptoms and signs of anxiety were described. Therapy using emotional release techniques was introduced, and participants were asked, “Do you understand how these unpleasant feelings resulting from anxiety-provoking events arise?”
Participants were instructed to imagine crumpling a piece of paper in their hands; if they paid attention, they would see that all the compressed tissues of the paper and its original shape were lost. It was explained that this is exactly what we do with our nervous system and muscles, transferring a lot of contraction and expansion to our muscles and blood vessels during the neural pressures experienced throughout the day.
Session 2: In this session, the physical anxiety factors were defined and explained. It was explained that when your nervous system is overwhelmed by tension, chemicals are released in the body, preparing you for fight or flight. This stress response can be beneficial in emergency situations where rapid action is required.
The calm response acts as a brake that stops stress and brings the body and mind back to a balanced state. After identifying your problem, you should assess its intensity on a scale from 0 (no discomfort) to 10 (maximum discomfort). Evaluate any physical or emotional discomfort related to a specific problem. By doing this, you can assess your progress after completing the entire emotional release technique. Following this, a participant was asked to grade the intensity of their discomfort on a scale of 0–10 as one of the assignments, using their example to demonstrate how to classify the intensity of discomfort.
Session 3: In this session, suppressed emotions resulting from stress were addressed, emphasizing that negative feelings about oneself are found due to judgments. It was mentioned that before starting the tapping, the participant should create an empathetic sentence that describes their problem. While creating this sentence, which should be expressed during tapping, they should consider the following points: (a) Acknowledge their problem and (b) Accept themselves despite any problem or fear they have. This sentence is the most common one used in the emotional release technique, and the problem expressed in this part can be about anything without limitations. The participant’s attention was drawn to several examples, such as “Although I am afraid of speaking in public, I deeply and completely accept myself” and “Despite having a headache, I deeply and completely accept myself.” Then, they were asked to write down their own sentence creation based on the issues discussed during the week on the sentence formation worksheet.
Session 4: Continuing from the third session, this session also focused on examining and coping with negative emotions. The student was informed that if they harbour permanent and unchangeable negative emotions about themselves, they might have arrived at the conclusion mentioned in the previous session. At this stage, essential techniques were introduced by tapping on 16 key points of the body (refer to Fig. 1). Then, using a grading scale, the sense of discomfort and problems in the body were examined. The student was asked to rate the intensity of their discomfort on a scale from 6 (no discomfort) to 16 (maximum severity). As homework, based on the emotional feelings triggered by thoughts, they were instructed to tap on key points of the body according to what they had learned about tapping on these points.
Figure 1.
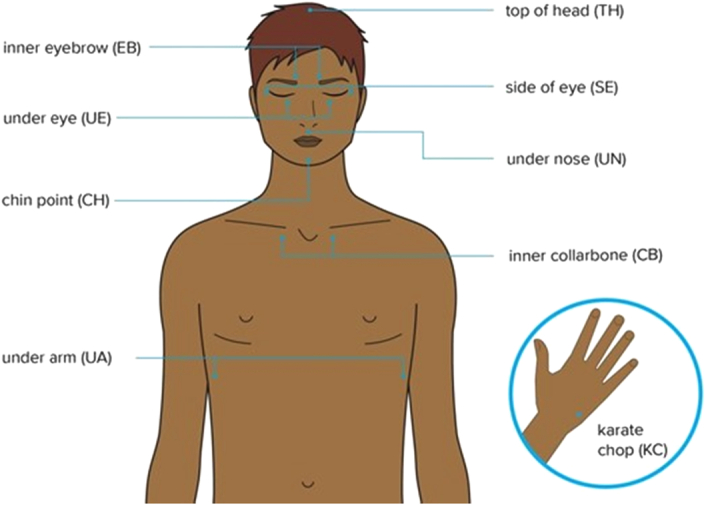
Emotional freedom techniques tapping points.
Session 5: In this session, along with focusing on the participant’s problem and anxiety-inducing distress, tapping on key points of the body and visualization were practiced. Again, the intensity of the problem was evaluated using a grading scale from 0 to 10. If the intensity was still high, the tapping process was repeated as follows: the participant was taught to tap from the top of the head to under the arm, and after tapping under the arm, the tapping sequence was completed by tapping again on the top of the head. As they tapped on each point, they were instructed to repeat the reminder phrase, which was a shortened version of the empathetic sentence from the previous step. As homework, the participant was asked to review the 10-tap exercise during the week, evaluate the intensity of the problem, and record it in the event log sheet.
Session 6: In this session, once again, emphasis was placed on the grading scale, and participants were asked to reevaluate the intensity of their problem on a scale of 0–10. If the participant still experienced significant anxiety, they were instructed to say, “Even though I still have some problems, I deeply and completely accept myself.” In the end, the content of the previous sessions was summarized, and a post-assessment was conducted.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics software version 24 (IBM SPSS Statistics). The normality of variables was assessed using the Shapiro–Wilk test. A χ2 test and one-way ANOVA were applied to compare the categorical data between treatment groups in the control. Paired sample t-test or Wilcoxon signed-rank test was applied to compare group data. ANOVA and Kruskal–Wallis test were applied to compare parametric continuous and nonparametric data between the groups, respectively. Anxiety score after intervention was assessed with ANCOVA. In all levels of analysis, P less than 0.05 was considered statistically significant.
Ethical considerations
The study protocol adhered to the principles of the Helsinki Declaration. Informed consent was obtained from all participants, and written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal upon request. The Ethics Committee of Kerman University of Medical Sciences approved this study (code: IR.KMU.REC.1401.369). Additionally, this clinical trial was registered at http://www.ClincalTrials.gov (Code: IRCT20221207056739N1).
Results
The mean age of students in the intervention and control groups was 25.22±1.85 and 22.80±1.80 years, respectively. There was no significant age difference between the two groups (P=0.59). According to Table 1, the two groups showed no differences based on demographic data before the study.
Table 1.
Demographic profile of the two groups of students.
| Variables | Experiment, n (%) | Control, n (%) | P |
|---|---|---|---|
| Sex | |||
| Female | 17 (63) | 20 (66.7) | 0.77 |
| Male | 10 (37) | 10 (33.3) | |
| Place of living | |||
| House | 18 (66.7) | 21 (70) | 0.78 |
| Dormitory | 8 (33.3) | 9 (30) | |
| Semester | |||
| 2 | 6 (22.2) | 7 (23.3) | 0.62 |
| 3 | 2 (7.4) | 3 (10) | |
| 4 | 10 (37) | 14 (46.7) | |
| 5 | 4 (14.8) | 1 (3.3) | |
| 6 | 5 (18.5) | 5 (15.7) | |
Based on Table 2, the average examination anxiety scores in the intervention and control groups followed a normal distribution. Therefore, parametric tests were employed to compare the examination anxiety scores within and between the groups.
Table 2.
Normality distribution of anxiety scores.
| Experiment | Control | |||
|---|---|---|---|---|
| Variables | Shapirov | P | Shapirov | P |
| Before intervention | 0.72 | 0.08 | 0.93 | 0.06 |
| After intervention | 0.95 | 0.19 | 0.92 | 0.06 |
In the intervention group (Table 3), the mean examination anxiety was 62.40 before and 50.88 after the intervention. Considering that a lower score on the examination anxiety questionnaire is better, it is evident that examination anxiety improved during the study in the intervention group, and this difference was statistically significant (P=0.001).
Table 3.
Differences of anxiety scores between two groups.
| Variables | Experiment | Control | t | P |
|---|---|---|---|---|
| Before intervention | 62.40 (SD=11.62) | 69.20 (SD=16.28) | −1.79 | 0.07 |
| After intervention | 50.88 (SD=8.84) | 65.36 (SD=15.23) | −4.32 | <0.001 |
| t | 3.78 | 1.77 | ||
| P | 0.001 | 0.08 |
In the control group, the mean examination anxiety was 69.2 before the intervention and 65.36 after the intervention. These changes were not statistically significant based on the mean difference (P=0.08). The independent t-test revealed that the mean examination anxiety before the intervention in the intervention group (62.4) and the control group (69.2) was within the moderate range (25–75). This difference was not statistically significant (P=0.07).
The mean examination anxiety after the intervention in the intervention group (50.88) was statistically significantly lower within the moderate range (25–75) compared to the mean examination anxiety in the control group (65.36) within the same range (P<0.001). Furthermore, according to the ANCOVA analysis, both the group and examination anxiety levels before the intervention reached statistical significance (Table 4).
Table 4.
ANCOVA results of anxiety score after education.
| Type III sum of squares | df | Mean squares | F | P | |
|---|---|---|---|---|---|
| Intercept | 2310.77 | 1 | 2310.77 | 18.36 | <0.001 |
| Anxiety before intervention | 1969.51 | 1 | 1969.51 | 15.64 | <0.001 |
| Group | 1816.12 | 1 | 1816.12 | 14.43 | <0.001 |
| Error | 6796.12 | 54 | 125.85 |
Discussion
Based on the results, EFT education had a significant effect on reducing test anxiety in medical students. The observed reduction in test anxiety among medical students after EFT education aligns with previous research indicating the technique’s effectiveness in managing stress and anxiety. Some studies, including those involving Turkish nursing students23, adolescents in the USA24, Iranians25, and American students26, concluded that EFT education has an essential effect on reducing anxiety. EFT education has the potential to decrease test anxiety in medical students due to various factors, including psychological, physiological, and educational elements.
EFT involves tapping on specific acupressure points while focusing on emotional concerns. This process is believed to stimulate the body’s energy meridians, promoting a relaxation response. By integrating EFT into their routine through education, medical students can cultivate a self-help tool for regulating stress, which assists in managing the physiological arousal linked with test anxiety20.
EFT incorporates cognitive restructuring by encouraging individuals to verbalize and acknowledge their fears and concerns while tapping. This dual focus on the cognitive and emotional aspects of anxiety may facilitate emotional processing, allowing medical students to confront and reframe their negative thoughts about examinations. This shift in cognitive perspective may contribute to reduced anxiety levels27. EFT education empowers individuals to take an active role in managing their emotional well-being. By teaching medical students a practical technique they can use independently, the intervention fosters a sense of self-efficacy. Feeling in control of one’s emotional responses to stressors can contribute to increase confidence and a more positive mindset when facing examinations28.
The mind-body connection is a central concept in EFT. By acknowledging the interplay between emotional and physical experiences, medical students may develop a heightened awareness of how their thoughts and emotions manifest physically. This awareness can be instrumental in recognizing and addressing early signs of anxiety, enabling proactive intervention before it escalates29. EFT is a positive coping mechanism that students can integrate into their daily lives. Unlike some traditional stress management methods, EFT is portable, discreet, and can be practiced without special equipment. Students can apply the technique before examinations, during study breaks, or in any situation where anxiety arises, fostering resilience and adaptability in the face of stressors30.
Test anxiety often manifests as performance anxiety, impacting concentration and memory recall during examinations. EFT education may assist in reducing this performance-related stress by addressing the underlying emotional factors. As medical students become proficient in using EFT, they may experience a more focused and centred mindset, enhancing their cognitive performance during tests31. EFT education offers the potential for long-term emotional resilience. By equipping medical students with a practical tool for managing stress, the intervention may contribute to developing adaptive coping strategies that extend beyond their academic journey32. This aspect is precious in the demanding field of medical sciences, where ongoing stressors are prevalent.
Limitations and strength
Sampling bias occurs when the participants selected for the study are not representative of the broader population from which they are drawn. In this case, if the study recruits participants from a specific subset of Iranian medical sciences students, such as those from a particular university or region, the findings may not be generalizable to all Iranian medical sciences students. For instance, if the sample disproportionately includes students from higher socioeconomic backgrounds or those with particular personality traits, it could skew the results. To mitigate this, researchers should aim for a diverse and representative sample that reflects the demographics of Iranian medical sciences students.
Response bias arises when participants provide inaccurate or misleading responses, consciously or unconsciously. Relying on self-reported measures for test anxiety can introduce response bias, as participants may feel inclined to present themselves in a favourable light or may overestimate the effectiveness of the intervention. In the case of this study, participants might feel pressured to report reductions in test anxiety after undergoing EFT, either due to social desirability bias or the placebo effect. To minimize response bias, researchers could employ objective measures of test anxiety, such as physiological indicators or behavioural observations, in addition to self-report measures.
Investigating only the short-term effects of EFT on test anxiety may not provide a comprehensive understanding of its efficacy. Test anxiety can be a chronic and recurrent issue for many students, and its management often requires long-term interventions. By focusing solely on short-term outcomes, the study may overlook the sustainability of the intervention’s effects. Longitudinal studies with extended follow-up periods would be necessary to assess whether any reductions in test anxiety persist over time or if additional booster sessions of EFT are needed to maintain its benefits.
The study focuses on Iranian Medical Sciences students, providing valuable insights into a specific cultural context. This can enhance the applicability of the findings to this particular population. Depending on the study’s design and sample size, the findings may have the potential for generalizability to other medical sciences students or even students in different cultural contexts who experience test anxiety.
Implications
The study’s positive outcomes, underscore the potential significance of incorporating EFT into the repertoire of interventions to address test anxiety. Such findings would contribute to the existing literature by providing evidence for the efficacy of EFT in a context where stress levels are exceptionally high, such as medical sciences education in Iran. This could have broader implications for educational institutions globally, suggesting that alternative therapeutic approaches like EFT could be beneficial in diverse academic settings.
A robust discussion should explore the potential mechanisms through which EFT may have impacted test anxiety. The tapping technique in EFT is believed to influence the body’s energy system, promoting a sense of relaxation and emotional balance. Examining the psychological and physiological changes associated with EFT in the context of test anxiety elucidates its potential as a self-help tool that students can integrate into their coping strategies.
Consideration should be given to the potential integration of EFT into educational programs aimed at reducing test anxiety. If EFT proves effective, educators and academic institutions may need to explore ways to incorporate this technique into existing support services. Providing students with tools like EFT as part of their academic toolkit can contribute to their overall resilience and well-being.
Conclusion
The findings suggest that EFT may be an effective and accessible approach to reducing anxiety levels among medical sciences students facing the pressures of tests. The results of the study indicate a statistically significant decrease in test anxiety scores among participants who underwent EFT sessions, highlighting the potential of this technique as a viable tool for managing and mitigating anxiety associated with academic assessments. This positive impact on test anxiety is particularly promising for medical sciences students, who often experience heightened stress levels due to the rigorous nature of their studies and the demands of their profession. Overall, the findings pave the way for further investigations into innovative approaches to promoting mental well-being among students facing the challenges of academic stress.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Source of funding
Not applicable.
Author contribution
All of the authors contributed equally in any stage of the study. All of the authors approved the final version of the manuscript.
Conflicts of interest disclosure
Not applicable.
Research registration unique identifying number (UIN)
This clinical trial was registered at http://www.ClincalTrials.gov, identifier: IRCT20221207056739N1.
Guarantor
Mozhgan Taebi.
Data availability statement
Data will be available by corresponding author on the request.
Acknowledgements
The authors express their deepest gratitude to all those who contributed to completing this study. Additionally, the authors appreciate the participants who generously shared their time and insights, without whom this study would not have been achievable. Finally, the authors acknowledge the unwavering support and encouragement from their colleagues, friends, and families, whose encouragement sustained them through the challenges of this endeavour.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 3 April 2024
Contributor Information
Mansooreh Azzizadeh Forouzi, Email: forozy@gmail.com.
Mozhgan Taebi, Email: m_taeby@yahoo.com.
Atena Samarehfekri, Email: mail.mazums@gmail.com.
Niloofar Rashidipour, Email: spsmazums@gmail.com.
References
- 1.Bostani S, Rambod M, Irani PS, et al. Comparing the effect of progressive muscle relaxation exercise and support group therapy on the happiness of nursing students: a randomized clinical trial study. Int J Africa Nursing Sci 2020;13:100218. [Google Scholar]
- 2.Horwitz E, Tallon M, Luo H. Anxiety in schools: the causes, consequences, and solutions for academic anxieties. JC Cassady, Foreign Language Anxiety 2009;2:56–78. [Google Scholar]
- 3.Gu R, Ge Y, Jiang Y, et al. Anxiety and outcome evaluation: the good, the bad and the ambiguous. Biol Psychol 2010;85:200–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.DeCaro MS, Thomas RD, Albert NB, et al. Choking under pressure: multiple routes to skill failure. J Exp Psychol Gen 2011;140:390. [DOI] [PubMed] [Google Scholar]
- 5.Zeidner M.Reinhard Pekrun, Lisa Linnenbrink-Garcia. Anxiety in education. International handbook of emotions in education. Routledge; 2014:265–288. [Google Scholar]
- 6.Ajmal M, Ahmad S. Exploration of anxiety factors among students of distance learning: a case study of Allama Iqbal Open University. Bull Educ Res 2019;41:67–78. [Google Scholar]
- 7.Thomas CL, Cassady JC, Heller ML. The influence of emotional intelligence, cognitive test anxiety, and coping strategies on undergraduate academic performance. Learn Individual Diff 2017;55:40–48. [Google Scholar]
- 8.Cassady JC.Jerrell C. Cassady. Anxiety in the schools: Causes, consequences, and solutions for academic anxieties. Handbook of Stress and Academic Anxiety: Psychological Processes and Interventions with Students and Teachers. Springer; 2022:13–30. [Google Scholar]
- 9.Sommer M, Arendasy ME. Comparing different explanations of the effect of test anxiety on respondents’ test scores. Intelligence 2014;42:115–127. [Google Scholar]
- 10.Wang AH, Lee CT, Espin S. Undergraduate nursing students’ experiences of anxiety-producing situations in clinical practicums: a descriptive survey study. Nurse Educ Today 2019;76:103–108. [DOI] [PubMed] [Google Scholar]
- 11.Franco H. Testing the impact of an online mindfulness program on prelicensure nursing students stress and anxiety. Nurs Forum 2022;57:288–297. [DOI] [PubMed] [Google Scholar]
- 12.Cornine A. Reducing nursing student anxiety in the clinical setting: An integrative review. Nurs Educ Perspect 2020;41:229–234. [DOI] [PubMed] [Google Scholar]
- 13.Yildirim N, Karaca A, Ankarali H, et al. Stress experienced by Turkish nursing students and related factors. Clin Exp Health Sci 2016;6:121–128. [Google Scholar]
- 14.Stinson C, Curl ED, Hale G, et al. Mindfulness meditation and anxiety in nursing students. Nurs Educ Perspect 2020;41:244–245. [DOI] [PubMed] [Google Scholar]
- 15.Adib-Hajbaghery M, Yazdani M. Effects of OSCE on learning, satisfaction and test anxiety of nursing students: a review study. Iranian J Med Educ 2018;18:70–83. [Google Scholar]
- 16.Beggs C, Shields D, Janiszewski Goodin H. Using guided reflection to reduce test anxiety in nursing students. J Holist Nurs 2011;29:140–147. [DOI] [PubMed] [Google Scholar]
- 17.Von der Embse N, Jester D, Roy D, et al. Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. J Affect Disord 2018;227:483–493. [DOI] [PubMed] [Google Scholar]
- 18.Sebastian B, Nelms J. The effectiveness of Emotional Freedom Techniques in the treatment of posttraumatic stress disorder: a meta-analysis. Explore 2017;13:16–25. [DOI] [PubMed] [Google Scholar]
- 19.Church D, Stapleton P, Vasudevan A, et al. Clinical EFT as an evidence-based practice for the treatment of psychological and physiological conditions: a systematic review. Future Psychol Approaches Enhance Ther Outcomes 2023;16648714:113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Vural PI, Körpe G, Inangil D. Emotional freedom techniques (EFT) to reduce exam anxiety in Turkish nursing students. Eur J Integr Med 2019;32:101002. [Google Scholar]
- 21.Church D. The EFT manual. Hay House, Inc; 2013. [Google Scholar]
- 22.Aboighasemi A, Asadi Moghaddam A, Najarian B, et al. Construction and validation of a test for the measurement of test anxiety among Ahwaz guidance school Students. J Educ Sci 1997;3:61–74. [Google Scholar]
- 23.İnangil D, Irmak Vural P, Doğan S, et al. Effectiveness of music therapy and emotional freedom technique on test anxiety in turkish nursing students: a randomised controlled trial. Eur J Integr Med 2020;33:101041. [Google Scholar]
- 24.Gaesser AH, Karan OC. A randomized controlled comparison of emotional freedom technique and cognitive-behavioral therapy to reduce adolescent anxiety: a pilot study. J Alternat Complement Med 2017;23:102–108. [DOI] [PubMed] [Google Scholar]
- 25.Ghasemzadeh A, Ghamari M, Hosseinian S. The impact of emotional freedom techniques on Students’ anxiety reduction and psychological wellbeing increase.. Educ Strategies Med Sci 2019;12:135–145. [Google Scholar]
- 26.Rogers R, Sears S. Emotional Freedom Techniques (EFT) for stress in students: a randomized controlled dismantling study. Energy 2015;7:27. [Google Scholar]
- 27.Pandey N. EFT as a tool to resolve anxiety: a case study approach. Int J Psycho-Soc Res (IJPSR) 2020;9:1–3. [Google Scholar]
- 28.Purwoko B, & Arianto A. The implementation of Emotional Freedom Technique (EFT) within the scope of education. 2nd International Conference on Education Innovation Springer Nature 2018 (ICEI 2018). https://www.atlantis-press.com/proceedings/icei-18/55907597
- 29.Stewart A, Boath E, Carryer A, et al. Can emotional freedom techniques (EFT) be effective in the treatment of emotional conditions? Results of a service evaluation in Sandwell. J Psychol Ther Prim Care 2013;2:71–84. [Google Scholar]
- 30.Boath E, Stewart A, Carryer A. A narrative systematic review of the effectiveness of Emotional Freedom Techniques (EFT). Staffordshire University, CPSI Monograph; 2012a. [Google Scholar]
- 31.Boath E, Stewart A, Carryer A. Tapping for PEAS: Emotional freedom technique (EFT) in reducing presentation expression anxiety syndrome (PEAS) in university students. Innovat Pract Higher Educ 2012b;1– 12. [Google Scholar]
- 32.Bach D, Groesbeck G, Stapleton P, et al. Clinical EFT (Emotional Freedom Techniques) improves multiple physiological markers of health. J Evid-Based Integr Med 2019;24:2515690X18823691. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be available by corresponding author on the request.