

Abstract
Background:
Aligning cost of mental health care with expected clinical and functional benefits of that care would incentivize the delivery of high value treatments and services. In turn, ineffective or untested care could still be offered but at costs high enough to offset the delivery of high value care.
Aims:
The authors comment on Benson and Fendrick’s paper on Value-Based Insurance Design (VBID) for mental health in the September 2023 special issue of this journal. The authors also present a preliminary framework of key ingredients needed to consider VBID for mental health treatments and services.
Methods:
The authors briefly review current and past efforts to contain costs and improve quality of mental health care, which include (for example) use of carve-out and carve-in programs, evaluation of cost sharing models, impact of accountable care organizations, and studying other benefit designs and impact of federal and state policies.
Results:
Using PTSD as an example, key ingredients of VBID for mental health services were identified and include the following: tools for case identification and monitoring progress over time at the population level; specific treatments and services with evidence of clinical effectiveness, cost-effectiveness, and health equity; and an approach to document the specific treatment or service was delivered (versus another treatment or service that may lack evidence).
Discussion:
The inability to afford mental health care is a top barrier to treatment seeking. People who do elect to spend time and money on mental health care are further disadvantaged by accessing care that is not well regulated and the quality at best is questionable. VBID could be an important lever for increasing access to and use of high value mental health care. Partnerships among the research, practice, and policy communities can help ensure research solutions meet needs of these two communities.
Background
Aligning cost of mental health care with expected clinical and functional benefits of that care would incentivize the delivery of high value treatments and services. In turn, ineffective, untested, or undertested treatments and services could still be offered, for example, in a case where a patient or provider has a particular preference for a type of treatment, but at costs high enough to offset costs for high value care. This is the vision that Benson and Fendrick1 and the Center for Value-Based Insurance Design2 highlighted in the September 2023 special issue in the Journal of Mental Health Policy and Economics. Benson and Fendrick’s article1 is based on their plenary presentation at the January 2023 National Institute of Mental Health (NIMH)-National Institute on Drug Abuse (NIDA) Health Economics conference.3
Benson and Fendrick’s1 vision is a partial reality for medical care. Early successes show that reducing or eliminating co-payments for several classes of medications used to treat hypertension and diabetes was associated with no cost increases and even some cost savings from the employer and employee perspective.4 Other research consistently shows improvement in quality of care but with mixed results in terms of cost savings or cost neutrality.5 While practices that cap or increase copayments that don’t differentiate among treatments and services may reduce expenditures for insurers, these approaches may also reduce the use of essential treatments that are important in treating chronic, including symptomatic, conditions. Consequently, these practices could actually increase the use of healthcare services.6
An example law that seeks to improve the delivery of evidence-based services comes from the Affordable Care Act (ACA). The ACA stipulates that A- and B-level recommendations from the United States Preventive Services Task Force (USPSTF) must be offered with no cost sharing in Medicare,7 commercial, and individual or family plans.8 (However, this provision may be subject to change due to litigation9.) In a subsequent review of the impact of this ACA mandate on many clinical services (the review did not include mental health services), Norris et al.10 concluded that the impacts “of cost-sharing elimination varied depending on clinical service, with a majority of findings showing increases in use. Studies that included socioeconomic status reported that those who were financially vulnerable incurred substantial increases in utilization.” That is, when cost-sharing was eliminated, use of services increased particularly in low-income populations. Despite the evidence available for general medical care, less is known about the impact that eliminating or reducing cost-sharing has in the use of mental health care.
Cost Containment Strategies and Impact on Quality of Mental Health Services
Although little is known about the impact of cost-sharing models on mental health care, there have been efforts to make mental health care more affordable for decades. Research in the 1970s and 1980s found that providing more limited benefits or imposing higher cost sharing requirements was justifiable for mental health and substance use services, owing to concerns that long-term service use would drive up costs.11 However, in the 1990s, researchers found that managed care’s supply-side mechanisms for cost containment, such as utilization review, effectively managed costs without the need for higher cost-sharing from patients.11 This finding led to the passage of the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act (MHPAEA) in October 2008, which prevents insurers from providing less favorable benefits for mental health and addiction services than those provided for general medical care.11,12 However, even within the context of managed care cost containment measures, there is still a need to refine these approaches to encourage the use of high-value services and reduce the use of low-value services.
As summarized in Ettner et al.,13 carve out programs gained popularity and separately administered benefits for behavioral healthcare from medical benefits. These programs generally involve greater direct care management for each illness type (physical health by the primary insurer and behavioral health by the carve out). In contrast, carve-in plans combine mental and behavioral health benefits, where all health care services are managed under one umbrella insurance plan. While carve out plans reduced costs and increased penetration (that is the probability of any treatment), Ettner et al. reported that evidence is mixed about carve-outs’ impact on quality. Indeed, the findings were also limited by to the lack of care quality and clinical outcome data, which is a noted gap area when using claims, electronic health record, and many other administrative data sources, and where more research is needed to fill this gap and better integrate data on quality with data on cost.14,15 Interestingly, and as a consequence of MHPAEA, there are administrative incentives for employers and plans to move back to carve-in programs, and in doing so, Ettner et al.13 found an increase in inpatient costs and utilization for carve-in programs.
There are other methods that payers, providers, and patients use to attempt to control costs. For example, payers can negotiate directly with drug companies on price, using a tool that the Centers for Medicare & Medicaid Services (CMS) was recently given as part of the Inflation Reduction Act.16 Employers using self-insured plans can also influence price of services directly, though in an analysis comparing price of services between self- and fully insured plans, price of the services analyzed was generally higher in self-insured plans.17 Other efforts, like the development of Accountable Care Organizations (ACOs), empower providers, healthcare systems, and others involved in healthcare delivery to collectively work together and “share in the overall savings which are linked, in full or in part, to achieving population-based performance standards on quality measures and to reporting reductions in per member, per month costs.18” Wilson et al.’s18 review suggests these models are cost saving, but evidence of improved quality is mixed.
NIMH supports research projects that aim to improve quality of mental health services (e.g.,19,20). For example, Geissler21 examines the role of insurance networks in facilitating guideline-concordant care. McConnell22 studies the impact of Medicaid 1115 waivers, which were implemented to improve care for children and adults with serious mental illnesses, on healthcare utilization and suicide-related behaviors. Goff and Geissler23 examine the effects of Medicaid Accountable Care Organizations (ACOs) on behavioral health care quality and outcomes for children. Johnston24 examines how the Medicare Quality Payment Program can incentivize the provision of evidence-based depression and anxiety treatment by primary care providers. However, more research is needed that makes better determinations about quality and that better nuances how high- and low-quality mental health care is financed.
Other approaches to cost containment raise deductibles via high deductible plans in efforts to protect against the need for catastrophic and expensive services. In doing so, high deductible plans create demand-side incentives to utilize services more efficiently because of greater cost sharing for patients.25 While high-deductible plans are associated with overall reduction of costs, there is some evidence these plans can disproportionately reduce low value spending relative to overall spending for medical services.25
Raising deductibles is a blunt instrument,26 however, and not only reduce low value services but also high value services, except perhaps in all but the most urgent of circumstances. Indeed, Schilling et al.27 found that high deductible plans were associated with a disproportionate reduction of spending for mental health services (compared to medical services), and despite the overall reduction in spending, there was an increase in spending on emergency department visits.
A Path to VBID for Mental Health Care
Key Ingredients and Research Gaps
In efforts to reduce costs associated with the delivery of high value mental health care and increase costs associated with the delivery of low value mental health services, we propose a framework to identify the key ingredient needed to more precisely adjust cost while ensuring use of necessary and high-quality mental health care. The first ingredient is an operational definition of high and low value mental health care. The VBID center28 characterizes low value care as that which provides little or no benefit to patients, has the potential to cause harm, incur unnecessary cost to patients, or waste limited healthcare resources. Conversely, “[h]igh-value care means providing the best care possible, efficiently using resources, and achieving optimal results for each patient”.29 Within this definition is the need for specific evidence-based treatments and services for an indicated condition that are also associated with an efficient use of resources versus an alternative (e.g., are cost-effective, cost-beneficial). The second ingredient is a tool for case identification (e.g., screening) and tool to monitor progress over time for the target population (e.g., as in measurement-based care or use of a quality measure). The third ingredient is an approach to document the delivery of that high value treatment or service versus another treatment or service. These ingredients loosely map onto the framework to categorize measures to assess the impact of low value care.30
While necessary, these ingredients are not sufficient. Value-based care cannot be undertaken without addressing health equity. For example, measuring patient outcomes without considering the baseline risk level of patients can promote “perverse incentives” that lead to unintended consequences, for example, incentivizing providers to serve healthier patients.31,32 Models where providers or health care systems are reimbursed for certain quality improvement activities may favor those who have healthier patients and/or the resources to devote to documenting their activities.33 Thus, any strategy to identify high and low value care should define for whom, and in what circumstances, is this care high vs low value. The strategy should also evaluate the impact on disparity reduction and ensure the strategy does not exacerbate disparities, as even many people with commercial or public insurance do not have access to high value care. For example, some quality improvement initiatives require the collection of demographic data to track impact on health equity and ensure that more complex cases have equal access to care.34
Table 1 presents a preliminary framework for how VBID could be considered for mental health treatment and services using the ingredients describe above. We select PTSD as a diagnostic example because it is a common and potentially debilitating mental illness. As reported by NIMH,55 PTSD affects 3.6% of US adults in the past year. Approximately 1/3 of adults with PTSD experience serious impairment, 1/3 experience moderate impairment, and 1/3 experience mild impairment. Evidence-based treatments and services exist that can be delivered in both primary care and specialty settings.40 There is also evidence that treatment is cost-effective (e.g.,51), and there are examples of alternative interventions that lack clinical trial level evidence of effectiveness but are being delivered in practice despite the lack of evidence.46
Table 1.
Ingredients for VBID Readiness of Mental Health Services for PTSD.
| VBID Ingredients | VBID Readiness for PTSD Treatments and Services |
|---|---|
|
| |
| Valid approaches to identify patients | Yes. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5)35 and The PTSD Checklist for DSM-5 (PCL-5)36 |
|
| |
| Valid measures of improvement that can be used as part of measurement-based care | Yes. PCL-537 |
|
| |
| Outcome-focused quality measures that take the form of assessing the fraction of a given group of patients whose outcomes meet or exceed certain specified clinical objectives | Partially. Quality measures developed for use in the military health system, though not routinely used.38,39 |
|
| |
| Evidence-based interventions that can be delivered in practice settings | Yes for individual treatments. Individual treatments like Written Exposure Therapy (WET), Prolonged Exposure, and Cognitive Processing Therapy are examples well supported by clinical trials and recommended in clinical practice guidelines.40,41 |
| Yes for delivery models. Service delivery models like The Collaborative Care Model (CoCM), a specific and evidence-based service delivery model for primary care associated with improved outcomes, improved organization of care, and reduction disparity reduction, is well supported by clinical trials evidence and is recommended in a clinical practice guideline.40–44 | |
|
| |
| Intervention alternatives (either individual treatments or service delivery models) that are being delivered in practice, lack evidence of effectiveness (because they are ineffective or have not been rigorously tested), but could be offered with increased cost sharing | Yes for individual treatments. Individual treatment examples that lack robust evidence include Emotional Freedom Techniques (EFT), Prolonged Exposure in Primary Care (PE-PC), and Seeking Safety (SS)41,45 Yes for service delivery models. Service delivery models with insufficient evidence include Primary Care Behavioral Health (PCBH)46 |
|
| |
| Evidence of cost-effectiveness | Yes for individual treatments. There is evidence that many evidence based treatments are cost effective and/or can be delivered efficiently.47–49 |
| Yes for service delivery models. CoCM in general is cost-effective and, in some cases, cost savings.50 Evidence that CoCM for PTSD is cost-effective is positive but lest robust.51–53. | |
|
| |
| Systematic documentation that the evidence-based intervention was delivered (versus another intervention) | No for individual psychotherapies. There is no standard way to document that one specific psychotherapy was delivered versus another (e.g., WET, which is effective, versus EFT that has insufficient evidence). Billing codes (e.g., CPT codes) can document the delivery of psychotherapy in general but are not psychotherapy specific and are not designed to encourage an indicated dose of psychotherapy. |
| Partially for service delivery models. CoCM can specifically be documented via billing code (versus generic care integration codes) in those plans that reimburse for CoCM. However, billing codes may not be a good indicator of intervention fidelity. | |
|
| |
| Evidence that the interventions promote health equity and/or are associated with reductions of health disparities | Service delivery interventions like CoCM are associated with reductions of health disparities.44 Evidence suggests WET is effective in diverse (to include Spanish speaking) populations.54 |
Shared Responsibility among the Research, Practice, and Policy Communities
For VBID for MH to be realized, there should be thoughtful partnerships among the research, practice, and policy communities to (i) ensure high value mental health treatments and services can be identified, (ii) determine what structures are needed to affordably deliver evidence-based treatments, and (iii) employ approaches to monitor outcomes at a population level to help minimize common intervention drift that happens moving interventions from research to practice. Figure 1 articulates the primary responsibility for each community and identifies areas of overlap that necessitate strong partnerships.
Figure 1.
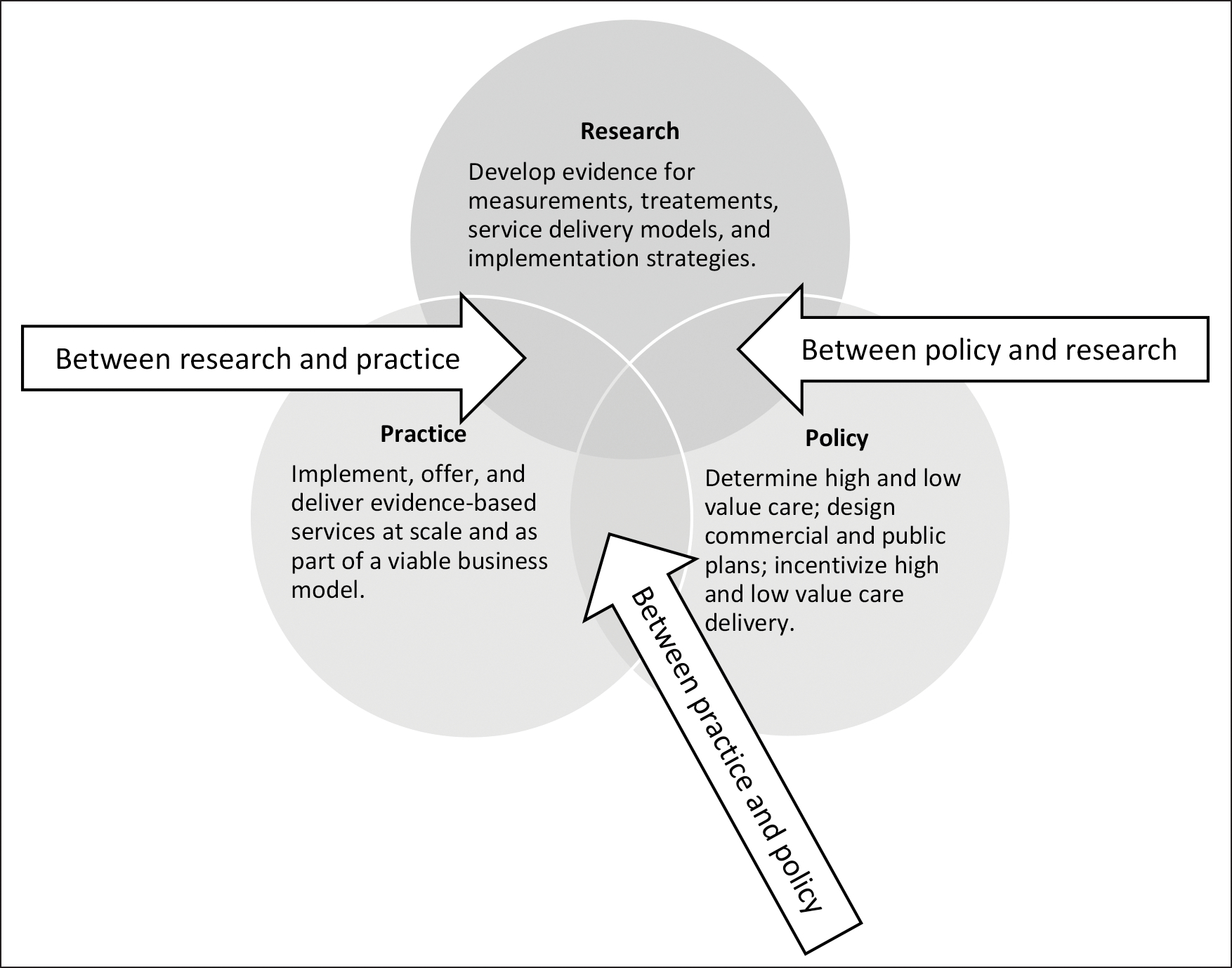
Primary Responsibilities of the Research, Practice, and Policy Communities and Areas Necessitating Partnerships.
The concept of practice-policy-research partnerships is important to define. It is critical that scientists who develop interventions consider contexts in which they will be delivered. Intervention developers should, at a minimum, collect information about the costs of services and the structures needed to facilitate implementation so that those tasked with making decisions about the value of an intervention and the return on investment can make informed decisions. Relatedly, practice and policy partners may be added to a study advisory board but may not be as truly involved as they should be in the actual science.56,57 An example of a research-practice partnership that led to eventual changes in practice and policy is the IMPACT Collaborative Care study.58 Before the study was launched, the design of the service intervention was co-developed with administrators, experts in service integration and other key informants to develop a model that would be easily adopted into practice. Data on the structures needed to successfully support the model was captured throughout the study. These data were important in informing the current financing of the model that support collaborative care in practice. A similar set of partnerships occurred within the military health system, which had implemented the collaborative care model for service members with PTSD and depression in 2007 and then tested enhancements to the model in a subsequent multi-site trial.42,59
Relatedly, policy makers are often in the position to quickly implement novel financing and service models before scientists have a chance to evaluate the potential impact. This can lead to funds being used to address important problems, without knowing what the impact of the model will be on access to mental health care. Early coordination with researchers to test the impact of these models on population health will identify which models are most effective and which would benefit from redesign. Natural experiments like this were funded by NIMH in the mid to late 1990’s, for instance the Colorado state alternative capitation systems study, where interrupted time series designs were applied to Colorado’s reorganization of the mental health system in real time.60–62 NIMH’s contemporary investments support projects that not only engage policy makers but also seeks to better understand the needs of policy makers and factors associated their decision making.63 More studies of this nature are needed.20,64,65
As the lead federal agency for research on mental health, NIMH shares responsibility with the practice and policy communities to ensure high value treatments and services are developed, tested in relevant settings, and ultimately delivered to people with mental illnesses. Examples below illustrate some ways in which research, policy, and practice partners/constituents can work together to promote the principles of high-value care.
Between Research and Practice
NIMH and other federal agencies encourage and support work that helps translate research findings into meaningful change in clinical practice, to improve patients’ access to high-quality services.
To provide specific high-quality care, the research and practice communities must have tools to define and measure specific high-quality care. Measures for quality of care are developed in the field and then endorsed by governing bodies, such as National Committee for Quality Assurance (NCQA), National Quality Forum (NQF), Battelle, and CMS’s Measures Under Consideration process. The endorsing process provides credibility to the measures and can help facilitate use of the measures by insurers and health care systems. Reviewing data from such measures can help patients, providers, and payers to identify high-quality services. While NIMH has existing funding announcements to bolter research in this space [20], quality measures are limited in supply and rarely used in mental health care. To help catalyze research in this area, NIMH also issued a specific funding announcement for investigators to develop outcome-focused mental health quality measures that can be submitted for endorsement to regulatory bodies with the ultimate goal of promoting the development and use of such measures to guide mental health treatment decisions.19
NIMH partners directly with other agencies to facilitate the translation of research to practice. For example, NIMH partnered with the Health Resources and Services Administration to provide implementation support, as part of HRSA’s efforts to implement the collaborative care model in nurse lead health clinics.66 NIMH and the National Institute on Drug Abuse (NIDA) partner with the Substance Abuse and Mental Health Services Administration (SAMHSA) to help facilitate research in Certified Community Behavioral Health Clinics (CCBHCs)67,68 and has even developed a database to help connect researchers with CCBHC practice partner.69 NIMH also requires researchers have practice partners such that research informs practice and in turn, practice informs research such as in the first70 and subsequent generations of the Early Psychosis Intervention Network (EPINET).71
Between Policy and Research
Translating research into clinical practice often goes together with translating research into policy. NIMH supports research that seeks to examine the impact of policies on patient- and provider-level outcomes. NIMH frequently work with other federal agencies to identify how research can be put into policy. For example, AHRQ and the USPSTF considers input from NIMH to inform the relevant key question in the USPSTF’s evidence review used for their recommendations. NIMH also provided technical assistance to CMS regarding billing codes for CoCM.72 NIMH supports research that directly addresses priorities outlined by groups like the USPSTF and the American College of Surgeons Committee on Trauma whose recommendations are supported by policy or practice mandates that incentivize the delivery of recommended services.73–75 Additionally, NIMH encourages researchers to co-design projects with policy makers and funders. Here, for example, Smelson et al.76 worked with third payers a priori to design a study testing components of their intervention, MISSION. Supported by evidence from multiple clinical trials, MISSION in its full form is highly effective for people with co-occurring mental health and substance use disorders but is unaffordable. Thus, Smelson and payers agreed on informal willingness to pay thresholds, knowing that components of MISSION would be less effective (than MISSION full) but affordable to deliver in routine practice.
Between Policy and Practice
NIMH has less of a direct role in policy-practice partnerships. However, there are examples as to how such partnerships can help to advance access to effective mental health care and where research can help. The USPSTF’s longstanding recommendation to screen for depression in primary care77 and newer recommendation for anxiety disorders78 helps encourage providers to identify new patients with these mental disorders so they can be connected to evidence based care. A- or B-level recommendations from the USPSTF alone may be insufficient to change practice, however. Rhee et al.79 examined the impact of the 2009 USPSTF depression screening recommendation and noted limited improvements in depression screening, diagnosis, and provision of subsequent depression care. Rhee et al’s findings suggest that despite a policy-empowered USPSTF recommendation,8 more solutions are needed to improve screening practices and connection to quality depression care.
In another example, Kahn et al.,80 examined value-based program penalty results for hospitals in the Hospital Readmissions Reduction Program, the Hospital Value-Based Purchasing Program, and the Hospital-Acquired Condition Reduction. The authors assessed the impact of health equity risk factors at the patient and community levels on hospital penalties. They found that hospitals are being penalized for risk factors out of the hospital’s control and may be worse for hospitals in underserved communities, which could further exacerbate health inequities. As Kahn et al argues, there is a need for value-based programs to account not only for hospitals’ risk-adjusted performance but also for patient and community health equity risk factors – largely beyond hospitals’ control – that influence patient outcomes. Though mental health care was not explicitly discussed in Kahn et al., people with mental illness are historically underserved and disproportionately and adversely affected by disparities in healthcare.81 And thus, research to better understand and intervene on those modifiable risk factors could better inform how case mix adjustments are made for mental health care.
Despite a limited role in practice-policy partnerships, NIMH certainly supports policy-focused research that has direct practice relevance on topics not directly thought of as healthcare. Specifically, a recent Notice of Special Interest (NOSI) solicits research examining the impact of policy interventions aimed at addressing social determinants of health to improve functioning and well-being for people with serious mental illnesses.65
Discussion
Access to and use of high value mental health services continue to be major challenges in the United States.15,82,83 Decades of research to understand the limitations to our system of care, to develop novel implementation, system and financing models have been support by NIMH, yet, with a few exceptions, many models are not supported or used by policy and practice. This science to services drop-off has resulted in significant quality of care challenges, and these disparities are felt deeply in communities with restricted financial resources and are faced with the decision to pay for mental health care or eat. This gap is widening.84 Not only is there a significant economic burden associated with unmet mental health needs, but the inability to afford mental health care is a top reason for not seeking services.85 People who do elect to spend time and money on mental health care are further disadvantaged by accessing care that is not well regulated and the quality at best is questionable. Value-Based Care Models that include support for evidence-based practices, measurement-based care and minimizes cost-sharing could be an important lever for increasing access and use of mental health care.
We acknowledge that financing is only part of a larger picture in mental health care. Barriers like access to providers trained in evidence-based treatment with availability to provide a therapeutic dose of care to a target population remain (e.g.,86,87). However, these issues need not first be resolved to consider VBID for mental health, as high value services (e.g., CoCM) exist and have already been demonstrated to improve the organization of care,88 perhaps freeing up resources and “stopping the flood” of unnecessary services89 to increase the capacity for high value care delivery.
VBID for mental health care is highly appealing because it reduces friction between providers and patients by making high value services free or low cost, while increasing the cost of delivering low value services. While we use PTSD care as an illustration, there are others (e.g., other mental illnesses and effective service delivery models to treat those illnesses) that are ripe for integration into VBID. Further, while evidence gaps remain (e.g., lack of quality measures; documentation of a specific EBP versus another, ensuring health equity) they can be filled in concurrent with pursing VBID for mental health services. To move the field forward, it is imperative to promote a strategic agenda that involves the research, policy, and practice partnerships to make that happen. NIMH has and will continue to support and enhance these partnerships between scientists, policy makers, and practice communities through future funding announcements and strategic partnerships with other federal agencies.
Implications for Health Care:
VBID holds promise to make high value mental health care more affordable while discouraging low value treatments and services.
Implications for Health Policies:
While evidence gaps remain, these gaps can be filled concurrently with pursuit of VBID for mental health services.
Implications for Future Research:
This paper identifies important research opportunities to help make VBID a reality for mental health care.
Footnotes
Disclaimer: The views expressed herein are those of the authors and not necessarily those of the National Institute of Mental Health, National Institutes of Health, or any other government agency or organization.
References
- 1.B enson NM and Fendrick AM, Value-Based Insurance Design: Clinically Nuanced Consumer Cost-Sharing for Mental Health Services. J Ment Health Policy Econ 2023; 26(3): 101–108. [PubMed] [Google Scholar]
- 2.Center for Value-Based Insurance Design. 2/15/2024]; Available from: https://vbidcenter.org/
- 3.N IMH. Health Economics at NIMH and NIDA – Domestic and International. 2023; Available from: https://www.nimh.nih.gov/news/events/2023/health-economics-at-nimh-and-nida-domestic-and-international
- 4.C hernew ME, Juster IA, Shah M, Wegh A, Rosenberg S, Rosen AB, Sokol MC, Yu-Isenberg K, Fendrick AM. Evidence that value-based insurance can be effective. Health Aff 2010; 29(3): 530–536. [DOI] [PubMed] [Google Scholar]
- 5.L ee JL, Maciejewski M, Raju S, Shrank WH, Choudhry NK. Value-based insurance design: quality improvement but no cost savings. Health Aff 2013; 32(7): 1251–1257. [DOI] [PubMed] [Google Scholar]
- 6.L uiza VL, Chaves LA, Silva RM, Emmerick IC, Chaves GC, Fonseca de Araújo SC, Moraes EL, Oxman AD. Pharmaceutical policies: effects of cap and co-payment on rational use of medicines. Cochrane Database Syst Rev 2015. May 8 2015(5): CD007017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.T olbert J The coverage provisions in the Affordable Care Act: An update. Kaiser Family Foundation. 2015. [Google Scholar]
- 8.S iu AL, Bibbins-Domingo K, and D. Grossman D. Evidence-Based Clinical Prevention in the Era of the Patient Protection and Affordable Care Act: The Role of the US Preventive Services Task Force. JAMA 2015; 314(19): 2021–2022. [DOI] [PubMed] [Google Scholar]
- 9.C hopra Z and Fendrick AM. Clinical Implications Of The Braidwood Ruling: Use Of Pre-ACA Task Force Recommendations. Health Affairs Forefront. May 2023. [Google Scholar]
- 10.Norris HC, Richardson HM, Benoit MC, Shrosbree B, Smith JE, Fendrick AM. Utilization Impact of Cost-Sharing Elimination for Preventive Care Services: A Rapid Review. Med Care Res Rev 2022; 79(2): 175–197. [DOI] [PubMed] [Google Scholar]
- 11.Barry CL, Huskamp HA, and Goldman HH. A political history of federal mental health and addiction insurance parity. Milbank Q 2010; 88(3): 404–433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Humensky JL, Duffy SQ, Cubillos L, Freed MC, Rupp A. Health Economic Interests at NIMH and NIDA to Improve Delivery of Behavioral Health Services. J Ment Health Policy Econ 2024; 27(1): 33–39. [PMC free article] [PubMed] [Google Scholar]
- 13.Ettner SL, Xu H, and F. Azocar F. What Happens When Employers Switch from a “Carve-Out” to a “Carve-In” Model of Managed Behavioral Health? J Ment Health Policy Econ 2019; 22(3): 85–94. [PubMed] [Google Scholar]
- 14.Rupp A, Freed MC, and Juliano-Bult D. Insurance markets, labor markets, and the mental health services delivery system. J Ment Health Policy Econ 2019; 22(4): 151–154. [PubMed] [Google Scholar]
- 15.Freed MC. A Mental Health Services Research Agenda in the Era of COVID-19: Steadfast Commitment to Addressing Evolving Challenges. J Ment Health Policy Econ 2021; 24(4): 137–142. [PubMed] [Google Scholar]
- 16.CMS. Medicare Drug Price Negotiation. 2024. [cited 2024 2/16/2024]; Available from: https://www.cms.gov/inflation-reduction-act-and-medicare/medicare-drug-price-negotiation
- 17.Sen AP, Chang JY, and Hargraves J. Health Care Service Price Comparison Suggests That Employers Lack Leverage To Negotiate Lower Prices. Health Aff 2023. 42(9): 1241–1249. [DOI] [PubMed] [Google Scholar]
- 18.Wilson M, Guta A, Waddell K, Lavis J, Reid R, Evans C. The impacts of accountable care organizations on patient experience, health outcomes and costs: a rapid review. J Health Serv Res Policy 2020; 25(2): 130–138. [DOI] [PubMed] [Google Scholar]
- 19.NIMH. Developing Measures to Advance Quality in Mental Health Care Services (R01 Clinical Trial Not Allowed). 2023. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/rfa-files/RFA-MH-23-265.html
- 20.NIMH. Innovative Mental Health Services Research Not Involving Clinical Trials (R01 Clinical Trials Not Allowed). 2023. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/pa-files/PAR-23-095.html
- 21.Geissler KLH. The Role of Insurance Networks and Organizational Factors in Guideline-Concordant Care for Serious Mental Illness. 2021. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/y7z3Hfssx0O3BfqKxrPIgg/project-details/10306958
- 22.McConnell KJ. The Effects of Medicaid Section 1115 Serious Mental Illness Waivers on Healthcare Utilization and Suicide-Related Behaviors. 2023. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/TlKE2bm-i06_gECRLhgwnA/project-details/10775350
- 23.Goff S and Geissler KLH. Effect of Medicaid Accountable Care Organizations on Behavioral Health Care Quality and Outcomes for Children. 2023. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/WFkhM1ZffUyBQCy6W9GIyw/project-details/10729117
- 24.Johnston KJ. Can the Medicare Quality Payment Program Incentivize Evidence-Based Treatment of Depression and Anxiety Disorders by Primary Care Providers? 2021. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/eB0f6IsUMEqgP-0aI_bZhw/project-details/10631718
- 25.Rabideau B, Eisenberg MD, Reid R, Sood N. Effects of employer-offered high-deductible plans on low-value spending in the privately insured population. J Health Econ 2021; Mar;76:102424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fendrick AM and Soonavala R. Expanding the “safe harbor” in high-deductible health plans: better coverage and lower healthcare costs. Am J Manag Care 2017; 23(12): 724–725. [PubMed] [Google Scholar]
- 27.Schilling CJ, Eisenberg MD, Kennedy-Hendricks A, Busch AB, Huskamp HA, Stuart EA, Meiselbach MK, Barry CL. Effects of High-Deductible Health Plans on Enrollees With Mental Health Conditions With and Without Substance Use Disorders. Psychiatr Serv 2022; 73(5): 518–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Center for Value-Based Insurance Design. [cited 2024 2/15/2024]; Available from: https://vbidcenter.org/.
- 29.Razmaria AA. JAMA PATIENT PAGE. High-Value Care. JAMA 2015; Dec 8; 314(22): 2462. [DOI] [PubMed] [Google Scholar]
- 30.Maratt JK, Kerr EA, Klamerus ML, Lohman SE, Froehlich W, Bhatia RS, Saini SD. Measures Used to Assess the Impact of Interventions to Reduce Low-Value Care: a Systematic Review. J Gen Intern Med 2019; 34(9): 1857–1864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Brown GS, Burlingame GM, Lambert MJ, Jones E, Vaccaro J. Pushing the quality envelope: a new outcomes management system. Psychiatr Serv 2001; 52(7): 925–34. [DOI] [PubMed] [Google Scholar]
- 32.Groenewegen PP, Spreeuwenberg P, Leyland AH, de Boer D, Boerma W. Case-mix adjustments for patient reported experience and outcome measures in primary care: an empirical approach to identify patient characteristics as case-mix adjusters based on a secondary analysis of an international survey among patients and their general practitioners in 34 countries. J Patient Rep Outcomes 2023; Dec 4; 7(1): 127.33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Rosenthal MB, Frank RG, Li Z, Epstein AM. Early experience with pay-for-performance: from concept to practice. JAMA 2005; 294(14): 1788–1793. [DOI] [PubMed] [Google Scholar]
- 34.Lewis C, Horstam C., Blumenthal D, Abrams MK. “Value-Based Care: What It Is, and Why It’s Needed” (explainer). 2023, Commonwealth Fund. [Google Scholar]
- 35.Bovin MJ, Kimerling R, Weathers FW, Prins A, Marx BP, Post EP, Schnurr PP. Diagnostic Accuracy and Acceptability of the Primary Care Posttraumatic Stress Disorder Screen for the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) Among US Veterans. JAMA Netw Open 2021. Feb 1; 4(2): e2036733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL.The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J Trauma Stress 2015; 28(6): 489–498. [DOI] [PubMed] [Google Scholar]
- 37.Wortmann JH, Jordan AH, Weathers FW, Resick PA, Dondanville KA, Hall-Clark B, Foa EB, Young-McCaughan S, Yarvis JS, Hembree EA, Mintz J, Peterson AL, Litz BT. Psychometric analysis of the PTSD Checklist-5 (PCL-5) among treatment-seeking military service members. Psychol Assess 2016; 28(11): 1392–1403. [DOI] [PubMed] [Google Scholar]
- 38.Hepner KA et al. Quality of Care for PTSD and Depression in the Military Health System Phase I Report. 2016, RAND. [PMC free article] [PubMed] [Google Scholar]
- 39.Hepner KA, Roth CP, Sloss EM, Paddock SM, Iyiewuare PO, Timmer MJ, and Pincus HA. Quality of Care for PTSD and Depression in the Military Health System: Final Report. 2017, RAND Corporation: Santa Monica, CA. [PMC free article] [PubMed] [Google Scholar]
- 40.The Management of Posttraumatic Stress Disorder Work Group. VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder Version 3.0. 2017, Department of Veterans Affairs and Department of Defense. [Google Scholar]
- 41.Management of Posttraumatic Stress Disorder and Acute Stress Disorder Work Group. VA/DoD Clinical Practice Guideline for Management of Posttraumatic Stress Disorder and Acute Stress Disorder D.o.V.A.a.D.o. Defense, Editor. 2023, Government Printing Office: Washington, DC. [Google Scholar]
- 42.Engel CC, Bray RM, Jaycox LH, Freed MC, Zatzick D, Lane ME, Brambilla D, Rae Olmsted K, Vandermaas-Peeler R, Litz B, Tanielian T, Belsher BE, Evatt DP, Novak LA, Unützer J, Katon WJ. Implementing collaborative primary care for depression and posttraumatic stress disorder: design and sample for a randomized trial in the U.S. military health system. Contemp Clin Trials 2014; 39(2): 310–319. [DOI] [PubMed] [Google Scholar]
- 43.Fortney JC, Pyne JM, Kimbrell TA, Hudson TJ, Robinson DE, Schneider R, Moore WM, Custer PJ, Grubbs KM, Schnurr PP. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry 2015; 72(1): 58–67. [DOI] [PubMed] [Google Scholar]
- 44.Jackson-Triche ME, Unutzer J, and Wells KB. Achieving Mental Health Equity: Collaborative Care. Psychiatr Clin North Am 2020; 43(3): 501–510. [DOI] [PubMed] [Google Scholar]
- 45.Norman S, Hamblen J, and Schnurr PP. Overview of Psychotherapy for PTSD. [cited 2024 2/16/2024]; Available from: https://www.ptsd.va.gov/professional/treat/txessentials/overview_therapy.asp#one
- 46.Possemato K, Johnson EM, Beehler GP, Shepardson RL, King P, Vair CL, Funderburk JS, Maisto SA, Wray LO. Patient outcomes associated with primary care behavioral health services: A systematic review. Gen Hosp Psychiatry; 2018. 53: 1–11. [DOI] [PubMed] [Google Scholar]
- 47.Le QA, Doctor JN, Zoellner LA, Feeny NC. Cost-effectiveness of prolonged exposure therapy versus pharmacotherapy and treatment choice in posttraumatic stress disorder (the Optimizing PTSD Treatment Trial): a doubly randomized preference trial. J Clin Psychiatry 2014; 75(3): 222–30. [DOI] [PubMed] [Google Scholar]
- 48.Sloan DM, Marx BP, Lee DJ, Resick PA. A Brief Exposure-Based Treatment vs Cognitive Processing Therapy for Posttraumatic Stress Disorder: A Randomized Noninferiority Clinical Trial. JAMA Psychiatry 2018; 75(3): 233–239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mavranezouli I, Megnin-Viggars O, Grey N, Bhutani G, Leach J, Daly C, Dias S, Welton NJ, Katona C, El-Leithy S, Greenberg N, Stockton S, Pilling S. Cost-effectiveness of psychological treatments for post-traumatic stress disorder in adults. PLoS One 2020. Apr 30;15(4):e0232245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Grochtdreis T, Brettschneider C, Wegener A, Watzke B, Riedel-Heller S, Härter M, König HH. Cost-effectiveness of collaborative care for the treatment of depressive disorders in primary care: a systematic review. PLoS One 2015. May 19; 10(5): e 0123078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Lavelle TA, Kommareddi M, Jaycox LH, Belsher B, Freed MC, Engel CC. Cost-effectiveness of collaborative care for depression and PTSD in military personnel. Am J Manag Care 2018; 24(2): 91–98. [PubMed] [Google Scholar]
- 52.Painter JT, Fortney JC, Austen MA, Pyne JM. Cost-Effectiveness of Telemedicine-Based Collaborative Care for Posttraumatic Stress Disorder. Psychiatr Serv 2017; 68(11): 1157–1163. [DOI] [PubMed] [Google Scholar]
- 53.Grote NK, Simon GE, Russo J, Lohr MJ, Carson K, Katon W. Incremental Benefit-Cost of MOMCare: Collaborative Care for Perinatal Depression among Economically Disadvantaged Women. Psychiatr Serv 2017; 68(11): 1164–1171. [DOI] [PubMed] [Google Scholar]
- 54.DeJesus CR, Trendel SL, and Sloan DM. A systematic review of written exposure therapy for the treatment of posttraumatic stress symptoms. Psychol Trauma 2024. Feb 15. doi: 10.1037/tra0001659. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.NIMH. Post-Traumatic Stress Disorder (PTSD). [cited 2024 2/16/2024]; Available from: https://www.nimh.nih.gov/health/statistics/posttraumatic-stress-disorder-ptsd
- 56.Jones N, Mascayano F, Susser E, Yang LH. Forecasting the Future: Lived Experience and the Transformation of Mental Health Services Research in the United States. J Ment Health Policy Econ 2023. 26(2): 77–83. [PubMed] [Google Scholar]
- 57.Humensky JL, Freed MC, Azrin ST, Acri M, Pintello D. Economic and Policy Research Interests Highlighted in the 25th NIMH-Sponsored Mental Health Services Research Conference. J Ment Health Policy Econ 2023; 26(3): 109–114. [PMC free article] [PubMed] [Google Scholar]
- 58.Unutzer J, Katon W, Callahan CM, Williams JW Jr, Hunkeler E, Harpole L, Hoffing M, Della Penna RD, Noël PH, Lin EH, Areán PA, Hegel MT, Tang L, Belin TR, Oishi S, Langston C; IMPACT Investigators. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288(22): 2836–2845. [DOI] [PubMed] [Google Scholar]
- 59.Engel CC, Jaycox LH, Freed MC, Bray RM, Brambilla D, Zatzick D, Litz B, Tanielian T, Novak LA, Lane ME, Belsher BE, Olmsted KL, Evatt DP, Vandermaas-Peeler R, Unützer J, Katon WJ. Centrally Assisted Collaborative Telecare for Posttraumatic Stress Disorder and Depression Among Military Personnel Attending Primary Care: A Randomized Clinical Trial. JAMA Intern Med 2016; 176(7): 948–956. [DOI] [PubMed] [Google Scholar]
- 60.Bloom JR, Hu TW, Wallace N, Cuffel B, Hausman JW, Sheu ML, Scheffler R. Mental health costs and access under alternative capitation systems in Colorado. Health Serv Res 2002; 37(2): 315–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Bloom JR, Hu TW, Wallace N, Cuffel B, Hausman J, Scheffler R. Mental health costs and outcomes under alternative capitation systems in Colorado: early results. J Ment Health Policy Econ 1998. 1(1): 3–13. [DOI] [PubMed] [Google Scholar]
- 62.Catalano R, Libby A, Snowden L, Cuellar AE. The effect of capitated financing on mental health services for children and youth: the Colorado experience. Am J Public Health 2000; 90(12): 1861–1865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Hoagwood KE, McKay MM. Accelerator Strategies for States to Improve System Transformations Affecting Children, Youth and Families. 2022. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/rxeNm-keV0yjoM0fUSWS1w/project-details/10437754
- 64.Purtle J, Moucheraud C, Yang LH, Shelley D. Four very basic ways to think about policy in implementation science. Implement Sci Commun 2023. Sep 12; 4(1): 111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.NIMH. Notice of Special Interest (NOSI): Impact of Policy Interventions Aimed at Addressing Social Determinants of Health to Improve Functioning and Well-being for People with Serious Mental Illnesses. 2024. [cited 2024 2/18/2024]; Available from: https://grants.nih.gov/grants/guide/notice-files/NOT-MH-24-340.html
- 66.US Department of Health and Human Services. Training on Implementing Collaborative Care Model for Behavioral Health Conditions in Nurse-Led Safety-Net Clinics. 2017. [cited 2024 2/16/2024]; Available from: https://crs.od.nih.gov/CRSPublic/View.aspx?Id=6221&FY=2019
- 67.NIMH. Notice of Special Interest (NOSI): Research using implementation science to support the delivery of evidence-based practices in community-based mental or general medical healthcare settings. 2022. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/notice-files/NOT-MH-22-170.html
- 68.NIMH. Advancing Learning Health Care Research in Outpatient Mental Health Treatment Settings (R34 Clinical Trial Optional). 2024. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/pa-files/PAR-24-118.html
- 69.National Council for Mental Wellbeing. Evidence-Based Practice Implementation Science Pilot. 2022. [cited 2024 2/16/2024]; Available from: https://www.thenationalcouncil.org/program/ccbhc-e-national-training-and-technical-assistance-center/ccbhc-ebp-implementation-science-pilot/
- 70.NIMH. Early Psychosis Intervention Network (EPINET). [cited 2024 2/16/2024]; Available from: https://www.nimh.nih.gov/research/research-funded-by-nimh/research-initiatives/early-psychosis-intervention-network-epinet
- 71.NIMH. Early Psychosis Intervention Network (EPINET): Learning Health Care Research to Improve Mental Health Services and Outcomes (P01 Clinical Trial Optional). 2024. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/rfa-files/RFA-MH-24-105.html
- 72.Press MJ, Howe R, Schoenbaum M, Cavanaugh S, Marshall A, Baldwin L, Conway PH. Medicare Payment for Behavioral Health Integration. N Engl J Med 2017: 376(5): 405–407. [DOI] [PubMed] [Google Scholar]
- 73.NIH. Notice of Special Interest (NOSI): Addressing Evidence Gaps in Screening. 2022. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-22-179.html
- 74.NIH. Notice of Special Interest (NOSI): Increasing Uptake of Evidence-Based Screening in Diverse Populations Across the Lifespan. 2022. [cited 2024 2/16/2024]; Available from: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-22-178.html
- 75.Zatzick DF and Bulger EM. A Deployment Focused Pragmatic Trial of Optimal Stepped Care Intervention Targeting PTSD and Comorbidity for Acutely Hospitalized Injury Survivors Treated in US Trauma Care Systems. 2022. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/Iy6zRzRo1k24fgi-K3up0w/project-details/10506526
- 76.Smelson DA et al. Supporting Treatment Access and Recovery for Co-Occurring Opioid Use and Mental Health Disorders (STAR-COD). 2021. [cited 2024 2/16/2024]; Available from: https://reporter.nih.gov/search/Au2AYliZFkKjTRmE-WlMfQ/project-details/10373400
- 77.U.S. Preventive Services Task Force. Barry MJ, Nicholson WK, Silverstein M, Chelmow D, Coker TR, Davidson KW, Davis EM, Donahue KE, Jaén CR, Li L, Ogedegbe G, Pbert L, Rao G, Ruiz JM, Stevermer JJ, Tsevat J, Underwood SM, Wong JB. Screening for Depression and Suicide Risk in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2023; 329(23): 2057–2067. [DOI] [PubMed] [Google Scholar]
- 78.U.S. Preventive Services Task Force. Barry MJ, Nicholson WK, Silverstein M, Coker TR, Davidson KW, Davis EM, Donahue KE, Jaén CR, Li L, Ogedegbe G, Pbert L, Rao G, Ruiz JM, Stevermer J, Tsevat J, Underwood SM, Wong JB. Screening for Anxiety Disorders in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2023; 329(24): 2163–2170. [DOI] [PubMed] [Google Scholar]
- 79.Rhee TG, Capistrant BD, Schommer JC, Hadsall RS, Uden DL. Effects of the 2009 USPSTF Depression Screening Recommendation on Diagnosing and Treating Mental Health Conditions in Older Adults: A Difference-in-Differences Analysis. J Manag Care Spec Pharm 2018; 24(8): 769–776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kahn CN 3rd, Rhodes K, Pal S, McBride TJ, May D, DaVanzo JE, Dobson A. CMS Hospital Value-Based Programs: Refinements Are Needed to Reduce Health Disparities and Improve Outcomes. Health Aff 2023; 42(7): 928–936. [DOI] [PubMed] [Google Scholar]
- 81.Lieff SA, Mijanovich T, Yang L, Silver D. Impacts of the Affordable Care Act Medicaid Expansion on Mental Health Treatment Among Low-income Adults Across Racial/Ethnic Subgroups, 2010–2017. J Behav Health Serv Res 2024; 51(1): 57–73. [DOI] [PubMed] [Google Scholar]
- 82.Freed MC. Remember the denominator: improving population impact of translational behavioral research. Transl Behav Med 2020; 10(3): 667–673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.SAMHSA. Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health, S.A.a.M.H.S. Administration, Editor. 2023. [Google Scholar]
- 84.Cook BL, Trinh N-A, Li Z, Hou SS-Y, Progovac A. Trends in Racial-Ethnic Disparities in Access to Mental Health Care, 2004–2012. Psychiatr Serv 2017; 68(1): 9–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.The White House. Reducing the Economic Burden of Unmet Mental Health Needs. 2022. [cited 2024 2/16/2024]; Available from: https://www.whitehouse.gov/cea/written-materials/2022/05/31/reducing-the-economic-burden-of-unmet-mental-health-needs/.
- 86.McLean CP, et al. Policy Recommendations for Increasing the Use of Evidence-Based Psychotherapy for Posttraumatic Stress Disorder in the Military Health System. Mil Med, 2023. [DOI] [PubMed] [Google Scholar]
- 87.McLean CP, et al. , Barriers and Potential Solutions to Implementing Evidence-Based PTSD Treatment in Military Treatment Facilities. Mil Med, 2022. [DOI] [PubMed] [Google Scholar]
- 88.Belsher BE, Jaycox LH, Freed MC, Evatt DP, Liu X, Novak LA, Zatzick D, Bray RM, Engel CC. Mental Health Utilization Patterns During a Stepped, Collaborative Care Effectiveness Trial for PTSD and Depression in the Military Health System. Med Care 2016; 54(7): 706–713. [DOI] [PubMed] [Google Scholar]
- 89.Chandrashekar P, Fendrick AM, and Ganguli I. Stopping the flood: reducing harmful cascades of care. Am J Manag Care 2021; 27(5): 178–180. [DOI] [PMC free article] [PubMed] [Google Scholar]