

This randomized clinical trial evaluates the efficacy and safety of xanomeline-trospium chloride vs placebo in adults with schizophrenia.
Key Points
Question
Is xanomeline-trospium chloride efficacious and well tolerated in people with schizophrenia experiencing acute psychosis?
Findings
In this phase 3, double-blind, randomized, placebo-controlled trial in 256 people with schizophrenia, xanomeline-trospium was associated with a statistically significant and clinically meaningful reduction in Positive and Negative Syndrome Scale total score compared with placebo. Xanomeline-trospium was generally well tolerated; the most common adverse events were primarily gastrointestinal effects, which were mild or moderate in intensity and generally transient in nature.
Meaning
EMERGENT-3 confirms previously reported clinical trials (EMERGENT-1 and EMERGENT-2) demonstrating that xanomeline-trospium is efficacious and well tolerated in people with schizophrenia experiencing acute psychosis.
Abstract
Importance
A significant need exists for new antipsychotic medications with different mechanisms of action, greater efficacy, and better tolerability than existing agents. Xanomeline is a dual M1/M4 preferring muscarinic receptor agonist with no direct D2 dopamine receptor blocking activity. KarXT combines xanomeline with the peripheral muscarinic receptor antagonist trospium chloride with the goal of reducing adverse events due to xanomeline-related peripheral muscarinic receptor activation. In prior trials, xanomeline-trospium chloride was effective in reducing symptoms of psychosis and generally well tolerated in people with schizophrenia.
Objective
To evaluate the efficacy and safety of xanomeline-trospium vs placebo in adults with schizophrenia.
Design, Setting, and Participants
EMERGENT-3 (NCT04738123) was a phase 3, multicenter, randomized, double-blind, placebo-controlled, 5-week trial of xanomeline-trospium in people with schizophrenia experiencing acute psychosis, conducted between April 1, 2021, and December 7, 2022, at 30 inpatient sites in the US and Ukraine. Data were analyzed from February to June 2023.
Interventions
Participants were randomized 1:1 to receive xanomeline-trospium chloride (maximum dose xanomeline 125 mg/trospium 30 mg) or placebo for 5 weeks.
Main Outcomes and Measures
The prespecified primary end point was change from baseline to week 5 in Positive and Negative Syndrome Scale (PANSS) total score. Secondary outcome measures were change from baseline to week 5 in PANSS positive subscale score, PANSS negative subscale score, PANSS Marder negative factor score, Clinical Global Impression–Severity score, and proportion of participants with at least a 30% reduction in PANSS total score. Safety and tolerability were also evaluated.
Results
A total of 256 participants (mean [SD] age, 43.1 [11.8] years; 191 men [74.6%]; 156 of 256 participants [60.9%] were Black or African American, 98 [38.3%] were White, and 1 [0.4%] was Asian) were randomized (125 in xanomeline-trospium group and 131 in placebo group). At week 5, xanomeline-trospium significantly reduced PANSS total score compared with placebo (xanomeline-trospium , −20.6; placebo, −12.2; least squares mean difference, −8.4; 95% CI, −12.4 to −4.3; P < .001; Cohen d effect size, 0.60). Discontinuation rates due to treatment-emergent adverse events (TEAEs) were similar between the xanomeline-trospium (8 participants [6.4%]) and placebo (7 participants [5.5%]) groups. The most common TEAEs in the xanomeline-trospium vs placebo group were nausea (24 participants [19.2%] vs 2 participants [1.6%]), dyspepsia (20 participants [16.0%] vs 2 participants [1.6%]), vomiting (20 participants [16.0%] vs 1 participant [0.8%]), and constipation (16 participants [12.8%] vs 5 participants [3.9%]). Measures of extrapyramidal symptoms, weight gain, and somnolence were similar between treatment groups.
Conclusions and Relevance
Xanomeline-trospium was efficacious and well tolerated in people with schizophrenia experiencing acute psychosis. These findings, together with the previously reported and consistent results from the EMERGENT-1 and EMERGENT-2 trials, support the potential of xanomeline-trospium to be the first in a putative new class of antipsychotic medications without D2 dopamine receptor blocking activity.
Trial Registration
ClinicalTrials.gov Identifier: NCT04738123
Introduction
Currently approved antipsychotic medications act primarily by blocking D2 dopamine receptors either as antagonists or partial agonists.1 Although these medications have demonstrated measurable efficacy for treating the positive symptoms of schizophrenia, they have limited efficacy for negative and cognitive symptoms. Moreover, positive symptoms are refractory or resistant to treatment in 20% to 30% of patients2,3,4 and adverse effects such as extrapyramidal motor symptoms, risk for developing tardive dyskinesia (TD), weight gain, and somnolence contribute to poor tolerability and adherence.5,6 There is a significant need for antipsychotics with different mechanisms of action, improved efficacy, and better safety and tolerability than current treatments.
Imbalances between muscarinic acetylcholine and dopamine neurotransmitter systems have been implicated in the pathophysiology of schizophrenia.7 Targeting muscarinic receptors may present a novel treatment option for people with schizophrenia.7 Xanomeline-trospium chloride (KarXT) combines the dual M1/M4 preferring muscarinic receptor agonist xanomeline with the peripherally restricted muscarinic receptor antagonist trospium chloride. In the phase 2 EMERGENT-1 trial (NCT03697252)8 and phase 3 EMERGENT-2 trial (NCT04659161)9 in people with schizophrenia experiencing acute psychosis, xanomeline-trospium significantly improved positive and negative symptoms compared with placebo and was well tolerated without many of the problematic adverse effects associated with currently approved antipsychotic medications (eg, extrapyramidal motor symptoms, weight gain, somnolence, and hyperprolactinemia). Here, we report results from the phase 3 EMERGENT-3 trial, which was designed to assess the efficacy, safety, and tolerability of xanomeline-trospium in people with schizophrenia experiencing acute psychosis.
Methods
Trial Design and Oversight
EMERGENT-3 (NCT04738123) was a phase 3, multicenter, randomized, double-blind, placebo-controlled trial conducted at 18 inpatient sites in the US and 12 inpatient sites in Ukraine between April 1, 2021, and December 7, 2022. The design of EMERGENT-3 was identical to EMERGENT-29 and very similar to EMERGENT-1.8 Ukraine was closed to further enrollment after the start of the Russia-Ukraine conflict in February 2022. The trial was conducted in accordance with the principles of the Declaration of Helsinki, the International Council of Harmonization guidelines for Good Clinical Practice, and the relevant regulations in the countries in which the research was conducted. The protocol and written informed consent were approved by a centralized institutional review board (WCG, Princeton, New Jersey). This trial followed Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Participants
EMERGENT-3 enrolled adults aged 18 to 65 years with a diagnosis of schizophrenia established by comprehensive psychiatric evaluation based on criteria in the DSM-V,10 and confirmed by Mini International Neuropsychiatric Interview for Schizophrenia and Psychotic Disorders version 7.0.2.11 A baseline Positive and Negative Syndrome Scale (PANSS)12 total score of 80 to 120 was required, with a score of 4 or higher (ie, reflective of symptoms that are moderate or worse in severity) on at least 2 of the following positive scale items: P1, delusions; P2, conceptual disorganization; P3, hallucinatory behavior; and P6, suspiciousness/persecution. A Clinical Global Improvement–Severity (CGI-S)13 score of at least 4 at screening and baseline was also required. People with a primary disorder other than schizophrenia within the 12 months preceding screening or a history of treatment resistance to antipsychotic medication were excluded. Participants with at least 20% improvement in PANSS total score between screening and baseline were also excluded. Per the US Food and Drug Administration directive on diversity in clinical trials, it is important to have representation proportional to the disease burden found in the general public; race was self-reported and entered by study staff in electronic data capture (Medidata RAVE, Medidata). There were no a priori indications that there would/will be racial differences in response or tolerability.Inclusion and exclusion criteria are provided in the eAppendix in Supplement 1.
Randomization and Interventions
Eligible participants were randomized (1:1 ratio; stratified by site) to receive twice-daily oral xanomeline-trospium or placebo using a computer-generated participant identification number and randomization schedule created by Veristat version 9.4 (SAS). Treatment group assignments were concealed from participants, trial and laboratory personnel, investigators, statisticians, and the sponsor.
Xanomeline-trospium and placebo were supplied as identical, matching capsules. Trial medication was started on day 1 of the 5-week treatment period. Xanomeline-trospium was dosed beginning with twice-daily 50-mg xanomeline and 20-mg trospium for the first 2 days and then twice-daily 100-mg xanomeline and 20-mg trospium for days 3 through 7. Beginning on day 8, there was flexible dosing with an optional dose increase to a maximum of twice-daily 125-mg xanomeline and 30-mg trospium based on tolerability as assessed by the investigator, with the option to return to 100-mg xanomeline and 20-mg trospium based on tolerability. No dose changes were allowed during the last 2 weeks of the trial. The dosing regimen was identical to that used in the EMERGENT-18 and EMERGENT-29 trials.
Procedures
CGI-S and PANSS scores were assessed at screening and baseline, and then weekly throughout the 5-week treatment period, beginning at week 1 for CGI-S and week 2 for PANSS. Spontaneous adverse events (AEs) were recorded at each visit. Orthostatic vital signs were measured supine and standing (after 2 minutes) at screening and on days 1, 3, 7, 8, 14, 21, 28, 32, and 35. Vital signs were recorded 2 hours after the morning dose at each postbaseline visit to correspond to maximum concentration. The Simpson-Angus Scale, Barnes Akathisia Rating Scale, and Abnormal Involuntary Movement Scale (AIMS) were assessed at baseline and weekly during the trial. A safety follow-up visit was performed at week 6 for participants not enrolling in the long-term, open-label, follow-up trial (EMERGENT-4).
Outcomes
The prespecified primary end point was change from baseline to week 5 in PANSS total score. Prespecified secondary end points were change from baseline to week 5 in PANSS positive subscale score, PANSS negative subscale score,12 PANSS Marder negative factor score,14 and CGI-S score,13 as well as the proportion of participants with at least a 30% reduction from baseline to week 5 in PANSS total score. The trial included pharmacokinetic and exploratory end points not reported here.
Safety Assessments
Safety was assessed by monitoring for spontaneous AEs after administration of the first dose of trial medication on day 1 until the time of discharge on day 35. The Simpson-Angus Scale was used to measure drug-related extrapyramidal motor symptoms (range, 0 to 40; higher scores indicate greater drug-induced parkinsonian symptoms)15; the Barnes Akathisia Rating Scale was used to assess akathisia (range, 0 to 14; higher scores indicate greater symptoms of akathisia)16; and the AIMS was used to assess risk of TD (range, 0 to 28; rating of 2 or higher on the global severity item indicates evidence of TD).17 Body weight, vital signs, and clinical laboratory values were also assessed.
Sample Size
Assuming a between-treatment group mean (SD) difference in change from baseline to week 5 in PANSS total score of 8 (16) points based on results from EMERGENT-1 and other similar antipsychotic registration trials, it was estimated that a sample size of approximately 172 participants (86 per group) would achieve 90.3% power for a 2-sided test at α of .05. With an anticipated attrition rate of 30%, enrollment of 246 participants was planned.
Statistical Analysis
Baseline demographics were reported descriptively using the intent-to-treat (ITT) population. All efficacy analyses were performed using the modified ITT (mITT) population, defined as all randomized participants who received at least 1 dose of the trial drug and had 1 baseline PANSS assessment and at least 1 postbaseline PANSS assessment. The difference in change from baseline to week 5 in PANSS total score was estimated using a mixed model for repeated measures (MMRM; SAS version 9.4 [SAS Institute]) with likelihood-based modeling to handle incomplete data. The model included terms for treatment group (xanomeline-trospium or placebo), visit (weeks 2, 3, 4 and 5), treatment by visit interaction, site, age, sex, and baseline PANSS score. Least squares (LS) mean change from baseline, SE, and LS mean difference between the xanomeline-trospium and placebo groups at week 5 along with the 95% CI and a 2-sided P value were calculated for the primary end point. A 2-sided P value of ≤.05 was considered statistically significant. Continuous secondary end points were analyzed in the same manner as the primary efficacy analysis. Cohen d effect size was calculated using the absolute value of the difference in LS mean change in score from baseline at week 5 between the xanomeline-trospium and placebo groups divided by the pooled SD estimated from the MMRM.
A supportive analysis was conducted with the MMRM approach used for the primary analysis, using the completer population, defined as all mITT participants who had a valid PANSS total score at week 5. Missing data assumptions used in the primary analysis were also evaluated with sensitivity analyses using multiple imputation approaches. Finally, a post hoc sensitivity analysis was performed in the intent-to-treat (ITT) population, defined as all participants who were randomized to treatment.
For the PANSS responder analysis, PANSS items were rescaled from a range of 1 through 7 to 0 through 6 or, equivalently, PANSS total scores were floor-adjusted by subtracting 30 points from baseline and postbaseline scores. This floor adjustment was prespecified in the statistical analysis plan. The percentage of PANSS responders at each week was calculated and summarized by treatment group. The percentage of PANSS responders at week 5 was compared between treatment groups (xanomeline-trospium and placebo) using the Cochran-Mantel-Haenszel test stratified by site.
To account for multiplicity, a fixed sequence testing procedure was used for all efficacy variables, which was also used in the EMERGENT-1 and EMERGENT-2 trials. The primary end point was tested first, followed by secondary efficacy outcomes measures in the following order: change from baseline to week 5 for xanomeline-trospium vs placebo in PANSS positive subscale score, PANSS negative subscale score, and PANSS Marder negative factor score, followed by CGI-S score and then the proportion of participants with at least a 30% reduction in PANSS total score (responders).
Safety analyses were performed in all randomized participants receiving at least 1 dose of xanomeline-trospium or placebo (safety population). Safety and tolerability data were summarized descriptively by treatment group and time point as appropriate. The number and percentage of participants with any treatment-emergent AEs (TEAEs), any serious TEAE, any severe TEAE, and any TEAE leading to trial drug discontinuation were summarized by treatment group. Mean change (SD) from baseline was calculated for measures of body weight and vital signs, as well as the Simpson-Angus Rating Scale, Barnes Akathisia Rating Scale, and AIMS scores, and summarized by treatment group. Data were analyzed from February to June 2023.
Results
Participants
A total of 431 individuals were screened, and 256 participants were randomized to receive xanomeline-trospium (125 participants) or placebo (131 participants) (Figure 1). The safety population included 253 participants (xanomeline-trospium, 125 participants; placebo, 128 participants), and the mITT population included 234 participants (xanomeline-trospium, 114 participants; placebo, 120 participants). A total of 46 participants (36.8%) in the xanomeline-trospium group and 38 participants (29.0%) in the placebo group discontinued the trial early, with the most common reasons being withdrawal of consent followed by AEs.
Figure 1. Consolidated Standards of Reporting Trials (CONSORT) Flow Diagram for the EMERGENT-3 Trial.

aThree participants who were randomized to placebo withdrew before receiving trial drug (1 met a protocol-specified withdrawal criterion and 2 withdrew consent).
bThe safety population included all participants who received at least 1 dose of trial drug.
cThe modified intent-to-treat (mITT) population, used for all efficacy analyses, included all participants randomized who received at least 1 dose of trial drug, had a baseline Positive and Negative Syndrome Scale (PANSS) assessment, and at least 1 postbaseline PANSS assessment.
Baseline demographics and characteristics were similar between treatment groups (Table 1). The majority of participants were men (191 of 256 participants [74.6%]); 156 of 256 participants (60.9%) were Black or African American, 98 (38.3%) were White, and 1 (0.4%) was Asian; the mean (SD) age was 43.1 (11.8) years. A total of 21 of 125 participants (16.8%) in the xanomeline-trospium group compared with 27 of 131 (20.6%) in the placebo group were from Ukraine. Mean (SD) baseline PANSS total scores were 97.3 (8.9) in the xanomeline-trospium group and 96.7 (8.9) in the placebo group.
Table 1. Baseline Demographics and Characteristics (Intent-to-Treat Population).
| Characteristic | Participants, No. (%) | ||
|---|---|---|---|
| Xanomeline-trospium chloride (n = 125) | Placebo (n = 131) | Overall (N = 256) | |
| Age, mean (SD), y | 43.6 (11.4) | 42.6 (12.2) | 43.1 (11.8) |
| Sex | |||
| Female | 38 (30.4) | 27 (20.6) | 65 (25.4) |
| Male | 87 (69.6) | 104 (79.4) | 191 (74.6) |
| Race | |||
| Asian | 1 (0.8) | 0 | 1 (0.4) |
| Black or African American | 79 (63.2) | 77 (58.8) | 156 (60.9) |
| White | 45 (36.0) | 53 (40.5) | 98 (38.3) |
| Not reported | 0 | 1 (0.8) | 1 (0.4) |
| Body mass index, mean (SD)a | 28.8 (5.6) | 28.0 (5.2) | 28.38 (5.4) |
| Baseline PANSS score, mean (SD) | |||
| Total | 97.3 (8.9) | 96.7 (8.9) | 97.0 (8.9) |
| Positive subscale score | 26.9 (3.7) | 26.4 (3.3) | 26.7 (3.5) |
| Negative subscale score | 22.6 (3.2) | 22.0 (3.7) | 22.3 (3.5) |
| Marder negative factor score | 22.0 (3.7) | 21.8 (4.2) | 21.9 (3.9) |
| Baseline CGI-S score, mean (SD) | 5.1 (0.6) | 5.0 (0.6) | 5.1 (0.6) |
Abbreviations: CGI-S, Clinical Global Improvement–Severity; PANSS, Positive and Negative Syndrome Scale.
Body mass index is calculated as weight in kilograms divided by height in meters squared.
Primary Efficacy End Point
For the primary end point, xanomeline-trospium was associated with a statistically significant 8.4-point greater reduction from baseline to week 5 in PANSS total score compared with placebo; the LS mean (SE) change from baseline to week 5 in PANSS total score was −20.6 (1.6) in the xanomeline-trospium group compared with −12.2 (1.6) in the placebo group (LS mean difference, −8.4; 95% CI, −12.4 to −4.3; P < .001; Cohen d effect size, 0.60) (Figure 2A; eTable 1 in Supplement 1). Among participants receiving xanomeline-trospium, a statistically significant improvement in PANSS total score vs placebo was evident starting at week 2 (first postbaseline rating) and was enhanced through the end of the trial (week 5). A supportive analysis of change from baseline to week 5 in PANSS total score for completers, a sensitivity analysis using placebo-based multiple imputation, and an exploratory post hoc analysis in the ITT population supported the primary analysis (eTable 2 in Supplement 1).
Figure 2. Positive and Negative Syndrome Scale (PANSS) and Clinical Global Improvement-Severity (CGI-S) End Points (Modified Intent-To-Treat [mITT] Population).
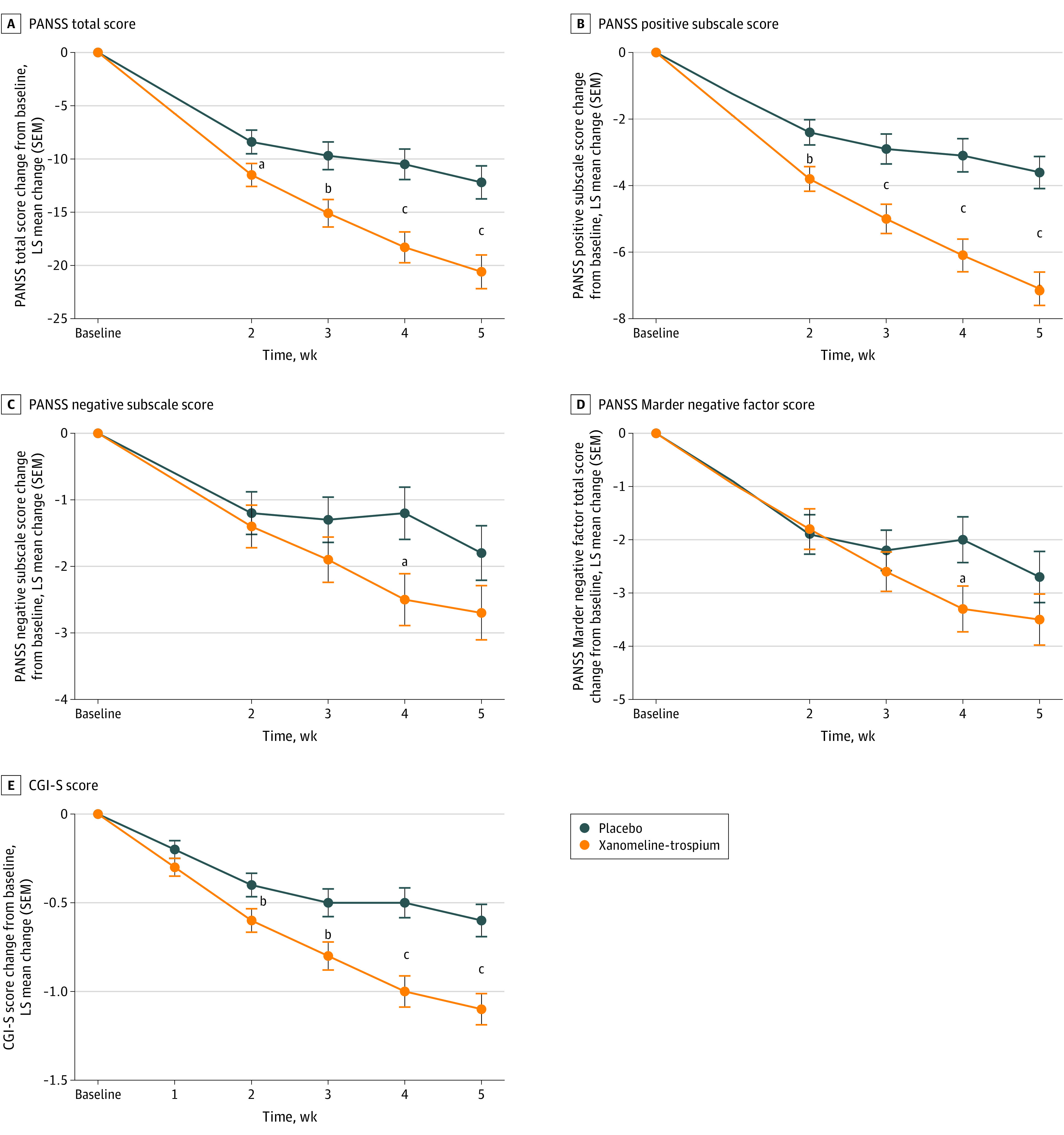
All efficacy analyses were performed using the mITT analysis set, defined as all randomized participants who received at least 1 dose of trial medication at baseline and at least 1 postbaseline PANSS assessment (xanomeline-trospium chloride n = 114, placebo n = 120). LS indicates least squares.
aP < .05.
bP < .01.
cP < .001.
Secondary Efficacy Outcomes Measures
The LS mean (SE) change from baseline to week 5 in the PANSS positive subscale score was −7.1 (0.5) in the xanomeline-trospium group compared with −3.6 (0.5) in the placebo group (LS mean difference, −3.5; 95% CI, −4.7 to −2.2; P < .001) (Figure 2B; eTable 1 in Supplement 1). The prespecified PANSS negative subscale score did not meet statistical significance at week 5, although the LS mean change from baseline in PANSS negative subscale score and PANSS Marder negative factor score achieved statistical significance at week 4 (Figure 2C and D; eTable 1 in Supplement 1). Although the prespecified secondary end point of CGI-S was not formally tested given the prespecified hierarchical testing procedure, the LS mean (SE) change from baseline to week 5 in CGI-S score was −1.1 (0.1) in the xanomeline-trospium group compared with −0.6 (0.1) in the placebo group (LS mean difference, −0.5; 95% CI, −0.8 to −0.3; nominal P < .001) (Figure 2E; eTable 1 in Supplement 1). Finally, the percentage of PANSS responders (at least 30% improvement from baseline in floor-adjusted PANSS total scores) at week 5 was 50.6% in the xanomeline-trospium group, compared with 25.3% in the placebo group (rate difference, 25.4%; 95% CI, 10.8% to 38.5%; nominal P < .01) (Figure 3; eTable 1 in Supplement 1).
Figure 3. Percentage of Participants With at Least 30% Reduction From Baseline in Floor-Adjusted Positive and Negative Syndrome Scale (PANSS) Total Score by Trial Week (Modified Intent-to-Treat Population).

Safety
Treatment-emergent AEs (TEAEs) were reported in 88 participants (70.4%) in the xanomeline-trospium group compared with 64 (50.0%) in the placebo group (Table 2). The most common TEAEs occurring in at least 5% of participants receiving xanomeline-trospium and at a rate at least twice that observed in the placebo group were nausea (24 participants [19.2%] vs 2 participants [1.6%]), dyspepsia (20 participants [16.0%] vs 2 participants [1.6%]), vomiting (20 participants [16.0%] vs 1 participant [0.8%]), constipation (16 participants [12.8%] vs 5 participants [3.9%]), hypertension (8 participants [6.4%] vs 2 participants [1.6%]), and diarrhea (7 participants [5.6%] vs 1 participants [0.8%]) (Table 2). Commonly reported cholinergic TEAEs were all mild to moderate in intensity, generally began within the first 2 weeks of treatment, and were transient in nature. The percentages of participants who discontinued treatment due to a TEAE were similar between the xanomeline-trospium group (8 participants [6.4%]) and placebo group (7 participants [5.5%]) (eTable 3 in Supplement 1). One serious TEAE (gastroesophageal reflux disease) was reported in the xanomeline-trospium group compared with none in the placebo group.
Table 2. Safety and Tolerability During the 5-Week Treatment Period (Safety Population).
| Variable | Participants, No. (%) | |
|---|---|---|
| Xanomeline-trospium chloride (n = 125) | Placebo (n = 128) | |
| Any TEAE | 88 (70.4) | 64 (50.0) |
| Serious TEAEa | 1 (0.8) | 0 |
| TEAE leading to discontinuation | 8 (6.4) | 7 (5.5) |
| TEAE occurring in ≥5% of participants in the xanomeline-trospium chloride group | ||
| Nausea | 24 (19.2) | 2 (1.6) |
| Dyspepsia | 20 (16.0) | 2 (1.6) |
| Vomiting | 20 (16.0) | 1 (0.8) |
| Constipation | 16 (12.8) | 5 (3.9) |
| Headache | 14 (11.2) | 15 (11.7) |
| Hypertensionb | 8 (6.4) | 2 (1.6) |
| Insomnia | 7 (5.6) | 10 (7.8) |
| Diarrhea | 7 (5.6) | 1 (0.8) |
| Mean (SD) change from baseline in body weight at week 5, kg | 1.4 (3.37) | 2.0 (3.08) |
| ≥7% Increase in body weight from baseline to week 5, No./total No. (%) | 5/78 (6.4) | 12/92 (13.0) |
| Mean (SD) change from baseline to week 5 in Simpson-Angus Scale score | −0.1 (0.56) | −0.1 (0.36) |
| Mean (SD) change from baseline to week 5 in Barnes Akathisia Rating Scale score | −0.1 (0.75) | −0.1 (0.88) |
| Mean (SD) change from baseline to week 5 in Abnormal Involuntary Movement Scale score | 0.0 (0.45) | 0.0 (0.15) |
Abbreviation: TEAE, treatment-emergent adverse event.
One serious TEAE of gastroesophageal reflux disease was reported.
Hypertension is the Medical Dictionary for Regulatory Activities preferred term and is not necessarily reflective of clinical hypertension.
No clinically meaningful changes from baseline to week 5 on any of the extrapyramidal motor symptom scales were detected between the xanomeline-trospium and placebo groups; across scales, participants had low mean scores at baseline and minimal change from baseline to the end of the trial. The mean (SD) change from baseline to week 5 in scores for the Barnes Rating Scale was −0.1 (0.75) points for xanomeline-trospium vs −0.1 (0.88) points for placebo, and the mean (SD) change in Simpson-Angus Scale score for extrapyramidal motor symptoms was −0.1 (0.56) points vs −0.1 (0.36) points, respectively (Table 2). No cases of TD were reported in either treatment group; mean (SD) change from baseline to week 5 in AIMS score was 0.0 (0.45) in the xanomeline-trospium group and 0.0 (0.15) in the placebo group (Table 2). Symptoms of akathisia were reported by 4 participants (3.2%) in the xanomeline-trospium group and 2 participants (1.6%) in the placebo group; all cases of akathisia were reported at the same trial center and none were deemed related to the trial drug in the opinion of the investigator. Three TEAEs of akathisia (2 in the placebo group, 1 in the xanomeline-trospium group) were ongoing at the end of treatment.
Xanomeline-trospium was not associated with weight gain or somnolence compared with placebo. The mean (SD) change in body weight from baseline to week 5 was 1.4 (3.4) kg in the xanomeline-trospium group and 2.0 (3.1) kg in the placebo group (Table 2). Five (4.0%) participants receiving xanomeline-trospium and 3 (2.3%) receiving placebo had an increase in body weight reported as a TEAE. The number of participants who experienced at least 7% increase in body weight from baseline to week 5 was 5 (6.4%) in the xanomeline-trospium group and 12 (13.0%) in the placebo group. The incidence of somnolence was 1.6% and 0% in participants receiving xanomeline-trospium and placebo, respectively.
There were small increases in mean systolic and diastolic blood pressure as measured at peak plasma concentration (Cmax; 2 hours post dose) in the xanomeline-trospium group compared with placebo, which peaked after 1 week (2 to 3 mm Hg) and partially attenuated by the end of the trial (eFigure 1 in Supplement 1). Hypertension was reported as a TEAE more frequently in the xanomeline-trospium group than the placebo group (8 participants [6.4%] vs 2 participants [1.6%], respectively). TEAEs of hypertension were largely transient elevations of blood pressure (higher than 140 mm Hg systolic or higher than 90 mm Hg diastolic) and most resolved during the trial. In participants with a TEAE of hypertension, mean blood pressure at the end of the trial was similar to baseline and did not lead to trial discontinuation. No increases in QTc interval were observed with xanomeline-trospium . Xanomeline-trospium treatment was associated with an increase from baseline in supine heart rate compared with placebo that peaked at day 8 (mean [SD], 13.0 [15.30] bpm vs 4.4 [14.02] bpm) and decreased through the end of the trial (mean [SD], 11.2 [14.99] bpm vs 5.9 [13.70] bpm).
Discussion
In the phase 3 EMERGENT-3 trial in people with schizophrenia experiencing acute psychosis, xanomeline-trospium was associated with a statistically significant and clinically meaningful 8.4-point greater reduction in PANSS total score compared with placebo at week 5. Statistically significant improvements in PANSS total score were observed with xanomeline-trospium starting at week 2 (first postbaseline measure) and enhanced through the end of the trial (week 5). The treatment effect sizes observed for the primary end point in this trial (0.60), the EMERGENT-1 trial (0.75),8 and the EMERGENT-2 trial (0.61)9 were robust; the median treatment effect size reported across 105 trials of antipsychotics in the treatment of acute psychosis in people with schizophrenia was 0.42.6 Treatment with xanomeline-trospium also resulted in a significantly greater reduction from baseline to week 5 in positive symptoms than placebo as measured by the PANSS positive subscale.
Xanomeline-trospium was well tolerated with an adverse effect profile substantially consistent with the previously reported EMERGENT-18 and EMERGENT-29 trials. The overall percentage of participants discontinuing treatment was similar between the xanomeline-trospium (36.8%) and placebo groups (29.0%), as was the percentage of people discontinuing due to TEAEs (6.4% vs 5.5%, respectively). The most common TEAEs in the xanomeline-trospium group were primarily gastrointestinal in nature; these TEAEs were all mild or moderate in intensity and improved in the first 2 to 3 weeks of the trial.
TEAS of hypertension were more common with xanomeline-trospium (8 participants [6.4%]) than placebo (2 participants [1.6%]). However, mean changes in systolic and diastolic blood pressure assessed at 2 hours postdose (ie, the approximate Cmax) were similar between the xanomeline-trospium and placebo treatment groups and remained relatively flat over the course of the 5-week trial; hypertension TEAEs were mostly mild, transient elevations of blood pressure in a small number of participants. The effect of xanomeline-trospium treatment on blood pressure is being evaluated in an ongoing ambulatory blood pressure monitoring trial in people with schizophrenia. As in prior trials, there was an increase in heart rate in the xanomeline-trospium group compared with the placebo group that decreased in magnitude by the end of the trial.
Limitations
The EMERGENT-3 trial had limitations typical of registration trials in acute psychosis. First, the duration of the trial was 5 weeks; schizophrenia is a lifelong illness and longer trials are needed to assess the durability of the effect and long-term safety and tolerability of xanomeline-trospium. Xanomeline-trospium was associated with rapid improvement in psychotic symptoms starting at week 2 and it continued to separate from placebo at week 5, suggesting additional improvement may occur at later time points. Two 52-week, open-label trials (EMERGENT-4 and EMERGENT-5) are currently under way to assess the longer-term effects of xanomeline-trospium in an outpatient setting. Second, the EMERGENT-3 trial did not include an active comparator group and, thus, only cross-trial comparisons can be made as opposed to direct comparisons of xanomeline-trospium with other currently available antipsychotic medications. Additionally, recruitment of participants from the US and Ukraine was planned. The Russia-Ukraine conflict commenced after recruitment started, and Ukraine was closed to further enrollment.
Conclusions
In EMERGENT-3, in adults with schizophrenia experiencing acute psychosis, xanomeline-trospium was associated with statistically significant and clinically meaningful improvement in schizophrenia symptoms and was generally well tolerated. The efficacy, safety, and tolerability of xanomeline-trospium in EMERGENT-3 were substantially consistent with the results reported for the EMERGENT-1 and EMERGENT-2 trials. Together, these results demonstrate that xanomeline-trospium has the potential to be the first in a new class of antipsychotic medications targeting muscarinic receptors and an alternative to D2 dopamine receptor antagonists not associated with the adverse effects of EPS, weight gain, or somnolence.
eAppendix. Inclusion and Exclusion Criteria
eTable 1. Efficacy Measures at Week 5 (mITT Population)
eTable 2. Primary and Supportive Analyses for Primary End Point: Change From Baseline at Week 5 in PANSS Total Score
eTable 3. Treatment-Emergent Adverse Events Leading to Trial Discontinuation
eFigure. Mean Systolic and Diastolic Blood Pressure Measures Recorded at 2 Hours Post Dose (Cmax)
Trial Protocol
Data Sharing Statement
References
- 1.Lieberman JA, First MB. Psychotic disorders. N Engl J Med. 2018;379(3):270-280. doi: 10.1056/NEJMra1801490 [DOI] [PubMed] [Google Scholar]
- 2.Conley RR, Kelly DL. Management of treatment resistance in schizophrenia. Biol Psychiatry. 2001;50(11):898-911. doi: 10.1016/S0006-3223(01)01271-9 [DOI] [PubMed] [Google Scholar]
- 3.Giordano GM, Caporusso E, Pezzella P, Galderisi S. Updated perspectives on the clinical significance of negative symptoms in patients with schizophrenia. Expert Rev Neurother. 2022;22(7):541-555. doi: 10.1080/14737175.2022.2092402 [DOI] [PubMed] [Google Scholar]
- 4.Ohi K, Muto Y, Sugiyama S, Shioiri T. Safety and efficacy in randomized controlled trials of second-generation antipsychotics versus placebo for cognitive impairments in schizophrenia: a meta-analysis. J Clin Psychopharmacol. 2022;42(2):227-229. doi: 10.1097/JCP.0000000000001232 [DOI] [PubMed] [Google Scholar]
- 5.Emsley R, Chiliza B, Asmal L, Harvey BH. The nature of relapse in schizophrenia. BMC Psychiatry. 2013;13:50. doi: 10.1186/1471-244X-13-50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939-951. doi: 10.1016/S0140-6736(19)31135-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Paul SM, Yohn SE, Popiolek M, Miller AC, Felder CC. Muscarinic acetylcholine receptor agonists as novel treatments for schizophrenia. Am J Psychiatry. 2022;179(9):611-627. doi: 10.1176/appi.ajp.21101083 [DOI] [PubMed] [Google Scholar]
- 8.Brannan SK, Sawchak S, Miller AC, Lieberman JA, Paul SM, Breier A. Muscarinic cholinergic receptor agonist and reripheral antagonist for schizophrenia. N Engl J Med. 2021;384(8):717-726. doi: 10.1056/NEJMoa2017015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kaul I, Sawchak S, Correll CU, et al. Efficacy and safety of the muscarinic receptor agonist KarXT (xanomeline-trospium) in schizophrenia (EMERGENT-2): results from a randomised, double-blind, placebo-controlled phase 3 study. Lancet. 2024;403(10422):160-170. doi: 10.1016/S0140-6736(23)02190-6 [DOI] [PubMed] [Google Scholar]
- 10.American Psychiatric Association . Schizophrenia and other psychotic disorders. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013:89-122. [Google Scholar]
- 11.Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(suppl 20):22-33. [PubMed] [Google Scholar]
- 12.Kay SR, Opler LA, Lindenmayer JP. The Positive and Negative Syndrome Scale (PANSS): rationale and standardisation. Br J Psychiatry Suppl. 1989;(7):59-67. doi: 10.1192/S0007125000291514 [DOI] [PubMed] [Google Scholar]
- 13.Haro JM, Kamath SA, Ochoa S, et al. ; SOHO Study Group . The Clinical Global Impression-Schizophrenia scale: a simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr Scand Suppl. 2003;(416):16-23. doi: 10.1034/j.1600-0447.107.s416.5.x [DOI] [PubMed] [Google Scholar]
- 14.Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry. 1997;58(12):538-546. doi: 10.4088/JCP.v58n1205 [DOI] [PubMed] [Google Scholar]
- 15.Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl. 1970;212:11-19. doi: 10.1111/j.1600-0447.1970.tb02066.x [DOI] [PubMed] [Google Scholar]
- 16.Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154:672-676. doi: 10.1192/bjp.154.5.672 [DOI] [PubMed] [Google Scholar]
- 17.Guy W. ECDEU Assessment Manual for Psychopharmacology. Revised. National Institute of Mental Health; 1976. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix. Inclusion and Exclusion Criteria
eTable 1. Efficacy Measures at Week 5 (mITT Population)
eTable 2. Primary and Supportive Analyses for Primary End Point: Change From Baseline at Week 5 in PANSS Total Score
eTable 3. Treatment-Emergent Adverse Events Leading to Trial Discontinuation
eFigure. Mean Systolic and Diastolic Blood Pressure Measures Recorded at 2 Hours Post Dose (Cmax)
Trial Protocol
Data Sharing Statement