

Abstract
Objective
The Digital Healthcare Act introduced the prescription of digital health applications under specific circumstances in 2019 in Germany. They are funded through the social security system. In market access of prescribed digital health applications, Germany is pioneering the market. There remains a gap in understanding the views of medical professionals on the incentives of using these applications. As prescription of digital health applications starts emerging in other European countries, we sought to generate an overview of incentives and barriers that affect the caregivers in their decision of promoting and prescribing them in Germany.
Methods
A Rapid Review of the Web of Science database for the years 2017–2023 was performed using sensitive search strings. Two reviewers conducted a three-phase selection via title, abstract and full-text independently from each other. The quality of studies was assessed systematically by both reviewers. Both quantitative and qualitative studies with primary data were included, and study quality was assessed using a standardised form.
Results
Out of 1643 initial results, 12 studies with information from 9302 physicians and psychotherapists were identified. Eight quantitative and four qualitative studies were included in the analysis. Key findings suggest that while between 40% and 60% of caregivers see relevant incentives mainly based on patients’ benefits, 20–40% see relevant barriers. For the physicians’ daily work, there were slightly more barriers than incentives identified in the quantitative synthesis. The qualitative studies revealed no relevant incentives that were not attributed to patients.
Conclusion
While digital health solutions offer promising avenues for enhancing patient care, their acceptance among healthcare professionals hinges on addressing prevailing concerns. Continuous research and dialogues with the medical community are pivotal to harness the full potential of digital health applications in healthcare.
Keywords: Digital Health, e-Health, digital health applications, incentives, physicians
Introduction
In recent years, digital healthcare has become an important area in medicine, with its uptake accelerated by the pandemic. 1 Digital health applications (DHA) have been offering innovative solutions to improve medical care and provide patients with new treatment options. In 2019, the digital healthcare act (DVG) altered § 33a SGB V to include a right of prescription by physicians and psychotherapists of DHA for patients under regulated circumstances. Digitale Gesundheitsanwendung (DiGA) have to undergo a specific procedure at a federal national agency (BfArM) that is strictly regulated in order to be eligible for reimbursement. Germany is the first country to implement such a regulated process for collective reimbursement. 2
These applications, called DiGA, belong to a special group of DHAs that are funded through the social security system. They were thus included in the benefits catalogue for prescription in 2020. 3
An equivalent to DiGAs, called Prise en charge anticipée numérique des dispositifs médicaux (PECAN), was introduced to the French healthcare system in 2023.4,5 Other European countries, such as Austria, have announced their intention to follow suit. 6
Physicians and psychotherapists are the professionals who are supposed to prescribe or recommend DHAs in Germany. For this reason, the incentive profile for physicians and psychotherapists is a relevant issue for the success of DHAs. A DHA should help patients to detect, monitor or directly treat diseases by complementing the medical care structure. 7
While patient engagement on using DiGA has been analysed in a recent review, 8 there is no review of the medical professionals’ view yet.
Objective
This article aims to provide a comprehensive overview of the incentive profile of DHA for physicians and psychotherapists. The results of this analysis will contribute to the further discussion on the integration of DHAs into medical practice and sheds a light on to what extent physicians and therapists include DHA in their care practice. Understanding the incentive profile for the physicians and therapists will lead to a better possibility of addressing those beforehand in the process of the development and the market access.
The following research questions shall be answered with this analysis:
What incentives does the use of DHAs offer to the practising physician or psychotherapist?
What are potential barriers that keep them from prescribing or recommending DHAs?
Derived from this question we aim to examine what the most present incentives are to use or to not use DHAs in the medical practice.
With this Rapid Review, we will highlight various aspects that have been examined in the literature so far and look at the studies, their quality and the DHAs examined.
Methods
The form of a rapid review was chosen to carry out the literature analysis for a quick summary and critical evaluation of the situation. To implement this method, the procedure was divided into seven steps, following Randolph, whereby the first step, formulation of the research question, was already described in objectives. 9
The determination of the search terms and the establishment of the search profile are shown in the following section. As database the multiple database was searched, which is entered into several databases via Ebsco Discovery Service and Ebsco Host containing for example Medline. 1 Additionally, a hand search for grey literature in search engines on the internet was performed.
The search strategy was prepared using the PEO scheme including search terms in German and English. 10 The research question was prepared as follows:
What incentives (O) does the use of DHAs (E) offer to the practising physician or psychotherapist (P)?
The attributions to the PEO Scheme and the derived search terms entered for title and Abstract search are shown in Table 1:
Table 1.
PEO scheme for the Rapid Review.
| Description | Search parameters | Exclusion criteria | |
|---|---|---|---|
| Population | Physicians and psychotherapists in outpatient setting | (‘*Arzt’ OR ‘*Ärzte’ OR ‘Doktor’ OR ‘Mediziner’ OR ‘doctor’ OR ‘physician’ OR ‘Psychotherapeut*’ OR ‘Therapeut*’ OR ‘Psychologe’ OR ‘psychotherapist’ OR ‘therapist’ OR ‘psychologist’) | Non-practising physicians, Patients and other groups |
| Exposure | Assessment concerning the use of DHA | (‘Befragung’ OR ‘Umfrage’ OR ‘Erhebung*’ OR ‘Fragebogen’ OR ‘Interview’ OR ‘Dialog*’ OR ‘Gespräch*’ OR ‘survey’ OR ‘questionnaire’ OR ‘interview’ OR ‘conversation’) AND (‘DiGA’ OR ‘Digitale Gesundheitsanwendung*’ OR ‘Gesundheits-App’ OR ‘digital health application’ OR ‘health app’) |
Assessment investigating the use of digital applications in hospitals or other institutions. No primary Assessment of data from physicians or psychotherapists. |
| Outcome | Incentives in the use of DHAs | (‘Anreize’ OR ‘Incentive’ OR ‘Motivation’) | Findings without reference to the incentives to the use of digital applications |
Source: Own representation based on: G_NIUS. 4
The literature selection was based on time, language, type of publication and data and content. Two authors (CCJK and FK, researchers and health economists) independently reviewed the literature and performed the exclusion. Disagreements on exclusion or inclusion were resolved amicably in discussion. There were no relevant discrepancies in the selection.
A time restriction was chosen from 2017 in order to include pre-investigations of DiGA, if necessary, due to the procedure for admission before the 2020 roll-out.
Inclusion Criteria were qualitative, quantitative and mixed-methods design studies with a reporting of primary data. Also, only articles that reported primary data on a comprehensive level where selected and this mostly excluded conference contributions, dissertations and books.
Articles were excluded if they did not address Germany, contained no primary data, did not address caregivers, did address digital applications in inpatient care or were not related to DHA. Also excluded were findings without references to the incentives or barriers for caregivers. Furthermore, studies not addressing Germany and written in languages that were not German or English were excluded.
Furthermore, an assessment of the study quality was conducted. All studies were evaluated using a standardised form from Appendices C and D by Hawker et al. with nine different categories. 11 By the means of this uniform, systematic evaluation form, studies with different research designs could be critically evaluated. This is particularly important since both qualitative and quantitative surveys were included. Both reviewers independently rated the included studies with the scores between 1 and 4 (1 = very poor, 2 = poor, 3 = fair, 4 = good) for each category. A high quality was assumed when at least 75% (27–36 points) were reached. For the scores for the methodology of the studies, the mean between the scoring of both reviewers was calculated if they were not more than 3 points apart from each other.
Lastly, the results were summarised in tables and structured using the PRISMA scheme. 12 Incentives and barriers were then identified in the quantitative synthesis also indicating the power due to the amount of participants agreeing to this topic. The numbers of participants agreeing to certain barriers or incentives were calculated backwards from given percentages and number of participants in the corresponding question and rounded to a whole person. The power was then calculated based on all participants assigned to quantitative settings. Furthermore, the findings of the qualitative Studies were summarised in a qualitative synthesis.
Results
Figure 1 gives an overview over the rapid review process. The search yielded 1643 results. One additional document from grey literature was identified by hand search. Excluding duplicates, 992 unique contributions remained for screening for inclusion based on their title. Subsequently, 48 papers were identified for abstract screening. Of these, 34 were excluded based on the specified exclusion criteria; 14 articles were identified as potentially eligible and subjected to full text screening; two additional papers were excluded during full text screening. Neither of these papers had conducted a primary data collection.
Figure 1.
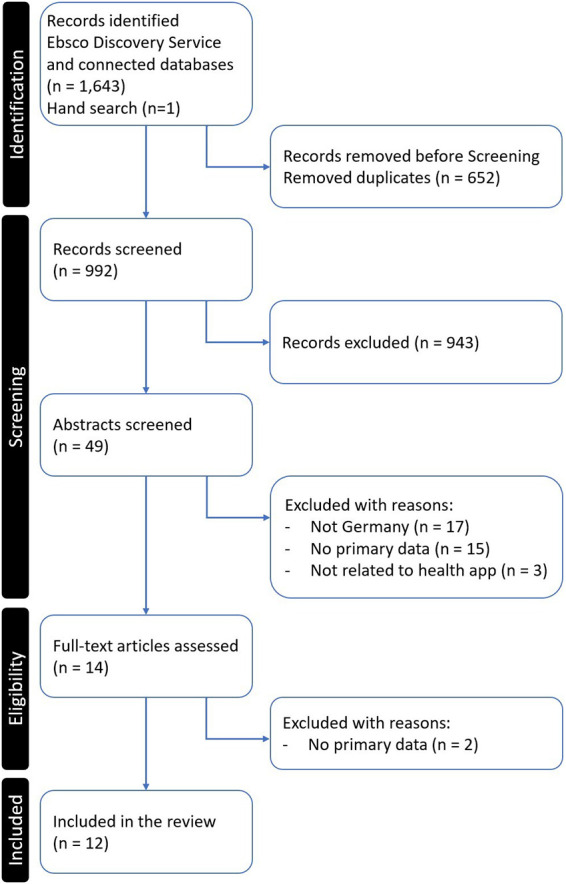
PRISMA flow diagram, own depiction.
A total of 12 sources were included in the analysis. Results were scanned for similar studies in the references. There were no relevant cross references identified within the chosen time span.
Table 2 provides an overview of the studies identified in this literature search. In particular, the methodology, the acceptance measurement as well as if it explicitly analyses DiGA and the disease field are listed here. In the last column, the score based on the independent quality evaluation is displayed.
Table 2.
Publications overview.
| Publication | Year | Methodology* (Num. Participants) | Acceptance measurements** | German DiGA specific | Targeted Illness | Score (%/ points) |
|---|---|---|---|---|---|---|
| Breil et al. 13 | 2022 | Quantitative: Online Survey (46) | UTAUT 14 (2) | No | Hypertension | (96,53%/34,57) |
| Götzl et al. 15 | 2022 | Qualitative: Semi-standardised interviews (2) | No standardised Indicator | No | Mental Health | (84,72%/30,5) |
| Hafner et al. 16 | 2022 | Quantitative: Online Survey (112) | UTAUT | No | Depression | (86,11%/31) |
| Hafner et al. 17 | 2022 | Qualitative: Guideline-based Interviews (6) | UTAUT | No | Depression | (77,78%/28) |
| Löbner et al. 18 | 2022 | Quantitative: Postal questionnaire (68) | Normalisation process theory (NPT 19 ) | No | Depression | (96,53%/34,57) |
| Schinle et al. 20 | 2022 | Quantitative: Online Survey (301) | Digital Health Compliance Questionnaire (DHCQ) | No | Dementia | (98,61%/35,5) |
| Wangler and Jansky 21 | 2020 | Qualitative: Guideline-based Interviews (35) | No standardised Indicator | No | Not specified (prevention) | (95,83%/34,5) |
| Wangler and Jansky 22 | 2021 | Quantitative: Postal questionnaire (2138) | No standardised Indicator | No | Not specified | (97,22%/35) |
| Wangler and Jansky 23 | 2022 | Qualitative: Semi-standardised interviews (38) | No standardised Indicator | Yes | Not specified | (100,00%/36) |
| Wangler and Jansky 24 | 2022 | Quantitative: Postal questionnaire (3829) | No standardised Indicator | Yes | Not specified | (100,00%/36) |
| Wangler and Jansky 25 | 2023 | Quantitative: Postal questionnaire (88) | No standardised Indicator | No | Diabetes | (90,28%/32,5) |
| Stiftung Gesundheit 26 | 2022 | Quantitative: Online Survey (2639) | No standardised Indicator | Yes | Not specified | (62,50%/22,5) |
Methodology and participants are assigned only for the addressed target group of service providers, other methodologies on patients may be included in the article.
UTAUT (2) (Unified Theory of Acceptance and Use of Technology): A theoretical framework that integrates various models to explain individuals’ intentions to use an information system and their subsequent usage behaviour with its extension UTAUT 2.
Normalisation Process Theory (NPT): A theoretical framework that helps to explain the processes through which new technologies or practices become routinely embedded in everyday work in healthcare settings. Digital Health Compliance Questionnaire (DHCQ): DHCQ is not a widely recognised standard questionnaire; it might be a tool or a method developed by the authors himself.
Eight quantitative and four qualitative studies were identified. Three of the studies assessed the acceptance of DHA with UTAUT and also three especially addressed DiGA.
Quantitative studies
Breil et al. 13
Breil et al. include 46 physicians. They were asked to report their attitudes towards a hypertension app. The intention to use the application was moderate for physicians (measured with UTAUT, mean 3.4, SD 0.9). This research pinpointed performance expectancy as the primary factor influencing the acceptance of mHealth apps for hypertension self-management by physicians. E-Health literacy was also identified as having a positive influence on physicians.
Hafner et al. 16
The study of Hafner et al. incorporates a heterogenous group of healthcare service providers including social workers and other non-medical professionals; 112 of those were physicians or psychotherapists. The results of this group were not reported separately. Therefore, the answers could not be attributed to physicians or psychotherapist directly, and, for this reason, this study was not included in the following quantitative synthesis.
Löbner et al. 18
The survey of Löbner et al. concentrates on DHA with a focus on depression; 68 physicians and psychotherapists were included in the study. Partially had they worked with the application in an intervention group and partially not. In the study, nearly half (48.5%) of the General Practitioners (GPs) either continued to recommend (for the intervention group) or began suggesting (for the control group) the e-mental health intervention after the trial ended. Benefits such as simple integration and enhancing patient involvement in disease control were noted. The study suggests simplifying the usage of DHAs and the integration in daily practice.
Schinle et al. 20
Schinle et al. have a sample size of 301 physicians and psychotherapists surveyed, based on the use of a dementia application. However, there is only a summary of the results of their study and hardly any information about the frequency of responses. For this reason, only one dimension (monitoring disease progression) could be included in the quantitative summary.
Wangler and Jansky 22
This study, which targets any DHAs, includes 2138 physicians and provides one of the biggest cohorts found by this review. Questions were limited to a given set. Free-text answers were not reported; 36% of the physicians who held favourable views highlighted patient motivation and compliance as benefits. Conversely, 44% of respondents who were skeptical raised concerns about data privacy, reliability, potential legal complications and the added workload resulting from app usage.
Wangler and Jansky 24
This study by the same authors again has the biggest cohort with 3829 physicians. It addressed specifically any type of DiGA. In this study, free-text entries were clustered and reported and thus included in the quantitative synthesis. Wangler and Jansky highlight that there is a significant need to enhance the understanding of GPs regarding the fundamentals of the DVG. Addressing their concerns directly is vital. Providing in-depth training sessions that detail the conditions and benefits of utilising DiGA is essential.
Wangler and Jansky 25
This study focuses on 88 diabetology physicians who were surveyed by mail about the use of a DHAs in type 2 diabetic patients; 49% of the physicians deemed DHAs a positive instrument in the health service provision. While health apps offer beneficial impacts on prevention and treatment, numerous diabetology specialists express concerns about the apps’ usability, clarity and security.
Stiftung Gesundheit 26
This study is a yearly online assessment by the German ‘Public Health Foundation’ with changing topics. This is a special issue on DiGA; 2639 physicians answered the online questionnaire on the use of DiGA and the representativeness is validated in comparison to the population. The areas where the use of DiGA is deemed effective were analysed over three years consecutively, and the agreement to possible areas of usage rose with each year. Due to the type of publication, this report loses points in Hawkers quality assessment for features such as missing an abstract and not following best publication practices falling below 75% quality although there is a representative database of good quality.
Quantitative synthesis
Five of the eight quantitative studies reported physicians or therapists seeing obstacles or being sceptical overall towards DHAs/DiGAs.18,22,24–26 In total, 3027 physicians out of 7.921 participants in these studies reported scepticism. This attributes to 38% of all physicians in these studies seeing obstacles in the use of DHAs/DiGAs. There is a difference in perception between DHAs with 42.6% scepticism and DiGAs with 36.4%.
Detailed reasons that were mentioned for or against the usage of DHAs in the quantitative analysis were divided into incentives (18) and barriers (23) In Table 3, these are listed in descending order of the highest to the lowest power (Number of service providers expressing the incentive or barrier) according to caregivers mentioning them in the studies.
Table 3.
Incentives/Barriers.
| Reasons for or against the use of DHA | DHA | Power | Share* | Sources |
|---|---|---|---|---|
| Incentives | ||||
| Raising motivation in Patients | Both | 3836 | 63.35% | 22,24,25 |
| Improve Patient compliance | Both | 2830 | 47.43% | 22,24 |
| Easy to understand | DiGA | 2058 | 53.75% | 24 |
| Better informed patients through DHA | DHA | 1926 | 31.46% | 18,22,24,25 |
| Protecting personal Data | DiGA | 1833 | 47.87% | 24 |
| Offer Individualisation | DiGA | 1737 | 45.36% | 24 |
| Doctor's appointment planning more effective | Both | 1526 | 25.57% | 22,24 |
| Reliable sources of information on the programme | DiGA | 1479 | 38.63% | 24 |
| Empowerment of Patients on terms of their illness | DiGA | 1340 | 35.00% | 24 |
| Faster diagnosis and risk assessment | Both | 1315 | 21.72% | 22,24,25 |
| Relieve for recording health data and measurements | Both | 1125 | 18.85% | 22,24 |
| Communication between patient and physician made easier | Both | 902 | 14.90% | 22,24,25 |
| Listing in the DiGA Directory | DiGA | 900 | 23.50% | 24 |
| Additional Information through DHA helps physicians treat more efficiently and personally | Both | 801 | 13.23% | 22,24,25 |
| Through DiGA physicians can reach new patient groups | DiGA | 728 | 19.01% | 24 |
| Monitoring of disease progression | DHA | 259 | 86.05% | 20 |
| Easy integration as additional treatment option | DHA | 30 | 44.12% | 18 |
| Strengthening personal responsibility of patients | DHA | 30 | 44.12% | 18 |
| Barriers | ||||
| Data Security/ Privacy concerns | Both | 3562 | 40.44% | 13,18,22,24–26 |
| Too complicated for Patients | Both | 2450 | 40.46% | 22,24,25 |
| More Work for Physicians | Both | 1980 | 32.70% | 22,24,25 |
| Reduces doctor–patient relationship | Both | 1752 | 28.93% | 22,24,25 |
| Generate to much data hindering fast and effective patient treatment | Both | 1459 | 24.45% | 22,24 |
| Too time-consuming to use | Both | 1085 | 18.18% | 22,24 |
| Doubts about effectiveness | Both | 847 | 31.29% | 18,26 |
| Doubts about usage/Acceptance by users | Both | 741 | 26.92% | 18,26 |
| Costs | DiGA | 712 | 26.98% | 26 |
| Encourage patients to self-diagnose and self-treat | Both | 692 | 11.60% | 22,24 |
| No familiarity/lacking possibilities to test | Both | 680 | 25.12% | 18,26 |
| High effort for prescription | DiGA | 561 | 21.26% | 26 |
| Complex/ bureaucratic activation | DiGA | 480 | 18.19% | 26 |
| Not enough information for Patients | Both | 467 | 17.25% | 18,26 |
| Technical problems prescribing | DiGA | 375 | 14.21% | 26 |
| Organisational barriers | DiGA | 296 | 11.22% | 26 |
| Rejection by health insurers | DiGA | 127 | 4.81% | 26 |
| Doubts about trustworthiness of content | DHA | 23 | 50.00% | 13 |
| Technical reliability of software | DHA | 20 | 43.48% | 13 |
| No time during consultation | DHA | 12 | 17.65% | 18 |
| Problems in access for the patients | DHA | 4 | 8.70% | 13 |
| Concerns about reimbursement | DHA | 3 | 6.52% | 13 |
| Threat of misdiagnosis | DiGA | 30 | 34.09% | 25 |
Share is the proportion of the answers given to all subjects in the corresponding studies with the possibility to name incentives or barriers within the cited studies.
Incentives for the use of DHA and DiGA revealed several benefits attributed to both patients and physicians. Notably, caregivers found value in DHA and DiGA for raising motivation in patients (3836 caregivers), improving patient compliance (2830), and on the physicians’ side making doctor's appointment planning more effective (1526).
When specific to DiGA, they found it easy to understand (2058), appreciated the protection of personal data (1833), and saw benefits in individualisation (1737). Furthermore, DiGA were seen as a reliable source of information (1479) and an empowerment of patients in terms of their illness (1340). Digitale Gesundheitsanwendung had the benefit of being listed in the DiGA Directory (900) and the possibility for physicians to reach new patient groups (728).
On the other hand, benefits associated only with DHA included better-informed patients (1926), monitoring of disease progression (259), easy integration as additional treatment option (30) and strengthening personal responsibility of patients (30).
Major concerns raised for both DHA and DiGA were data security and privacy (3562), the complexity for patients (2450), increased workload for physicians (1980) and potential negative influences on the doctor–patient relationship (1752). Further barriers were the assumption that they generate too much data that would hinder fast and effective treatment (1459), it would be too time consuming to use (1085) and there were doubts about their effectiveness (847) and usage in general (741). Encouraging patients to self-diagnose and self-treat (692) was a threat mentioned aside of lacking familiarity and possibility to test (680). Missing information for patients was also a concern (467).
For DiGA-specific concerns, physicians/caregivers pointed out issues such as costs (712), high effort for prescription (561) and bureaucratic activation processes (480). Further problems attributed to the system as technical problems when prescribing DiGA (375), organisational barriers (296) and rejection by health insurers (127). A smaller proportion also saw a threat of misdiagnoses (30).
Meanwhile, issues specific to DHA included doubts about the trustworthiness of content (23), technical reliability of the software (20), no time during consultation (12), problems in access for the patients (4) and concerns about reimbursement (3).
When summing up the identified incentives and barriers, 29.28% of the corresponding study participants see Incentives in both Application forms, 37.59% in DiGA and 34.22% in DHAs, respectively. 28.64% of the respondents see different Types of barriers, 16.21% in DiGAs and 24.60% in DHAs.
With 22.20% seeing incentives for their work as caregivers, 46.50% mentioning incentives on the patient side and 18.27% who report advantages for both sides, many of the advantages seen by caregivers seem to be attributed to patients’ benefits; 23.59% see barriers for themselves, 33.60% see barriers on the patient side and 19.59% for both groups. Possible disadvantages are therefore mainly seen as impacting the patients. Still barriers for caregivers seem to be higher than the incentives.
Qualitative studies
Götzl et al. 15
Götzl et al. conducted semi-standardised interviews with five experts on the usage of artificial intelligence (AI) in mental health apps. Of these experts only two (EXP 1 and EXP 5) were therapists. Only in some aspects the answers are directly contributable to these two experts or agreed by all experts. All experts agree in a positive attitude towards AI in mHealth Apps. Both therapists said the app should be connected to a health counselling facility. A barrier was seen by one expert as the possibility of enforcing digital media overuse. Other statements could not be directly connected to the therapists.
Hafner et al. 17
In the context of this study, guided individual interviews were conducted with 13 service providers, among others. Deductive elements from UTAUT were integrated into the guidelines. Of the 13 service providers, three psychologists and three physicians were interviewed. All 13 experts agree on the improvement of treatment options by digital health technologies in general. Nearly all experts (12/13) agree that it is substantial to continue the integration of personal interaction, especially in the care for depression. Other statements could not be attributed to the target group.
Wangler and Jansky 21
Their empirical investigations into DHA summarise that although there is potential to augment patient care outcomes, their guideline-based Interviews of 35 physicians indicates a limited adoption rate among GPs. Several barriers to widespread implementation have been identified. A primary concern is the absence of a comprehensive catalogue providing an overview of applications available, which impedes informed selection, especially due to the lack of standardised metrics to distinguish good applications from their suboptimal counterparts and neutral evaluations. A further realisation is that there are missing data protection standards and accreditation protocols to ensure the credibility and safety of these applications. The potential legal liability stemming from those health applications is a further reason for reservations. Moreover, the ambiguous remuneration frameworks for consultancy pertaining to these applications remain a pertinent issue warranting deliberation.
Wangler and Jansky 23
This study with semi-standardised interviews of 38 physicians on the usage and familiarity with DIGA shows several changes in the perception of DiGA over traditional DHA.
Physicians well-acquainted with DiGA underscore its higher quality, primarily due to enhanced information and guidance. They also identified a heightened trust in DiGAs, a result of rigorous legal mandates they adhere to. Furthermore, DiGAs exhibit potential in fortifying preventive healthcare measures and accelerating recovery. This is accompanied by the assurance of increased safety and reliability, a merit of the evaluation procedures instituted by the BfArM. In addition, DiGAs offer support in domains of self-monitoring, lifestyle modifications, prevention and medication management. A positive role is also observed in DiGAs’ capacity to amplify motivation, adherence, patient empowerment and health literacy. The direct networking between physicians and patients facilitated by DiGA is also identified to enhance effectiveness and efficiency.
However, the study also elucidated certain persisting challenges with DiGA. Among them are reservations regarding data security and the accuracy of the tools, which might lead to potential measurement errors and therapeutic missteps. Moreover, there is a potential to augment the uncertainty in patients who are already apprehensive about their health status.
Overall there seems to be a transition from DHA to DiGA addressing several points that hindered physicians in recommending DHA leading to a higher willingness to use these tools in daily practice.
Qualitative synthesis
This is also presented in the qualitative synthesis shown in Figure 2. The synthesis shows that the incentives are mainly attributed to the patients’ side. In the qualitative studies, there is low evidence for factors in using DHAs/DiGAs that are attractive to the caregivers. Also, there are more concerns expressed than incentives identified.
Figure 2.

Qualitative Synthesis, own depiction.
Digitale Gesundheitsanwendungs seem to reduce barriers that were previously connected to DHAs. Like the chance of promoting digital literacy, prevention, self-monitoring and motivation. At the same time, they introduce the risk of measurement errors and therapeutic missteps.
Even though there is a renumeration framework for DiGAs, this step has seemingly not moved the caregivers to see this as an incentive in contrast to DHAs.
Overall learnings
Both the qualitative and quantitative studies suggest that DiGAs have less disadvantages as their predecessor the DHAs and more advantages for caregivers.
The share of caregivers seeing the strongest incentives is about 40–60%. However, the highest consent with the barriers was 20–40%. However, incentives for the physicians are not very obvious in both forms of analysis, whereas barriers are very clear in the qualitative design but only slightly higher than the incentives in quantitative designs.
Discussion
This rapid review has been more limited than a systematic review. The short time span starting from 2017 will on the one hand lead to the exclusion of papers on the incentives for service providers of DHAs that were effective before the digital healthcare act. On the other hand, this approach also shows the current perception of DHA following the new legislation, especially in terms of payment for DHAs through the German social system. For some physicians from the start of the renumeration of DiGAs, these were perceived as competitors on the funds in the healthcare system. 26
Methodological limitations
The restriction to one database, even if it is a multiple database, increases the possibility of having missed relevant sources. While this reduces the workload significantly, the Ebsco Discovery service still includes a broad biomedical index of over 9.000 journals and relevant partner databases like Medline. Additionally, in several preceding reviews, PubMed, which would have been a further relevant database, did not produce additional results.
Limitations in study designs
Although the overall quality of the studies was good, some limitations apply in terms of the usability of data. One study in particular did not allow for single attribution of information to the group of healthcare professionals. 16 And due to the different study designs, different medical conditions and subjective selection of questions in interviews and surveys may bias the results, especially as some studies focus on special DHAs that include special features and obstacles not transferable to all kinds of DHAs. Some studies incorporated service providers that already had experience with DHAs. This could have been analysed separately supposing that this changes the overall perception. Five of the 13 studies are from the same team of researchers and provide a significant part of the participants. This is a high risk of bias in this review, because of the similar study designs and questions it is likely to overrate these conclusions.
The definition of DHA is not always the same throughout the studies and there is no explanation as to what type of applications the service providers attributed to DHA in general. This could have a negative effect on the interpretation of the differences of the strictly categorised DiGA and DHAs in general.
The overall informative value of the studies is limited as several of the studies report limited experience of the caregivers with DHA or DiGA, suggesting that there is a systematic bias possible regarding the non-responding service providers.
Similar results as in our review are found in a report on diabetes in terms of digitalisation in general: This survey of 326 diabetologists reveals that obstacles are seen above all in unclear remuneration (80.0%), legal uncertainties (50.3%) and high investment costs (46.5%) as well as in risks of misuse of patient data (38.4%) and susceptibility to errors (33.%%). This shows that some detractors are attributed to digitalisation in general and might not be only DHA specific. 27
There are other articles mentioning this topic but they do not include primary data on incentives or consider the barriers highlighted by service providers.28–30
Political representatives were interviewed in another study showing a different perspective on the hurdles and incentives that does not match strongly with the direct feedback from the target groups, that identified the will to digitalise in the target group as issue. 31
Conclusion
The acceptance of DHA by caregivers is still not well researched although it is a significant market access factor that needs to be considered. A relevant share of studies focus on one specific indication only. Only three studies could be identified that focus especially on DiGA.23,24,26 The fact that the user experience by patients as well as health care professionals have been found to be significant barriers for usage seems to call for a more systematic inclusion of those stakeholders in the product development process.
Incentives and Barriers were mainly identified from the evidence of the quantitative study designs. However, the qualitative designs helped getting a deeper view into the topics although being mostly specific on certain illnesses and not easily transferable into best practice.
Furthermore, there is only limited evidence on what would make DHAs more attractive, including rewarding remuneration or better support in appointments. Interoperability and integration in the caregivers IT-infrastructure are not present in these studies. Reduced effort in diagnosis, treatment or documentation is only present in the quantitative studies and is contradictory to the barriers that identify more work for the caregivers.
The relevance of our findings is emphasised by the fact, that German policy makers are reacting to the identified top three detractors of DiGAs with the Digitalgesetz (DigiG), which is to be ratified in 2024. The concern of excess costs is mitigated by introducing a performance-based element to coverage, which will constitute twenty percent of the reimbursed price. 32 The methods for successfully implementing this new scheme are however not determined yet and require careful scientific analysis. Furthermore, the determination of the reimbursed price itself seemingly lacks a health economic rationale at this point. 33
The DigiG also accelerates the roll-out of the electronic recipe, which will significantly reduce the effort of prescription. Lastly, the law aims to make the activation of DiGAs more practical for patients by obligating health insurance companies to send out the codes within 14 days. 32
Even though there is evidence that DiGAs have been a relevant step in reducing barriers for the usage of DHAs, there is further need of research on the overall perception of all caregivers over all possible DiGAs in order to identify a systematic approach towards a broader acceptance of DiGAs. Especially Incentives for caregivers should be assessed separately as they were always mixed with the patients benefits, in order to allow a guided reduction of barriers and usage of incentives in order to allow for a higher acceptance. A comparison with the incentives in other countries that are introducing DiGAs will help to contextualise our findings once there are sufficient data points available.
Full list of searched Databases through the services are available here: https://connect.ebsco.com/s/article/What-content-is-included-in-my-EBSCO-Discovery-Service-EDS-profile?language=en_US; https://uws-uk.libguides.com/az.php?a=p
Footnotes
Contributorship: The research group of all authors integrated the idea for the analysis into the joint research project. CCJK designed the analysis and set up the methodology. CCJK and FK both independently conducted the review of the literature and quality assessment of the studies found. CCJK then wrote the article. FK, BS and SB reviewed the article for consistency, quality of results and discussion. All authors contributed to the revision of the manuscript and approved the final version of the manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval: This review contains no study on humans or animals and is therefore not subject to ethical approval.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor: CCJK.
ORCID iDs: Cordula C. J. Kreuzenbeck https://orcid.org/0000-0001-5034-7211
Sophie X. Brenner https://orcid.org/0000-0002-7179-9150
References
- 1.Initiative D21 e.V. D21-Digital-Index 2021/2022: Jährliches Lagebild zur Digitalen Gesellschaft, https://initiatived21.de/publikationen/d21-digital-index/2021-2022 (2022, accessed 5 October 2023).
- 2.Bundesanzeiger. Gesetz für eine bessere Versorgung durch Digitalisierung und Innovation (Digitale-Versorgung-Gesetz – DVG), https://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl119s2562.pdf#__bgbl__%2F%2F*%5B%40attr_id%3D%27bgbl119s2562.pdf%27%5D__1632300570503 (2019, accessed 5 October 2023).
- 3.Jorzig A, Sarangi F. Digitalisierung im Gesundheitswesen: Ein kompakter Streifzug durch Recht, Technik und Ethik. Berlin, Heidelberg: Springer, 2020. [Google Scholar]
- 4.G_NIUS. Early access to reimbursement for digital devices (PECAN), https://gnius.esante.gouv.fr/en/financing/reimbursement-profiles/early-access-reimbursement-digital-devices-pecan (2023, accessed 5 October 2023).
- 5.MINISTÈRE DE LA SANTÉ ET DE LA PRÉVENTION. Décrets, arrêtés, circulaires, https://www.legifrance.gouv.fr/download/pdf?id=wbSfyB0QarBmS_OXWPwKuQHzzERt1iX0PtobthCE6A0%3D (2023, accessed 5 October 2023).
- 6.Parlament Österreich. Digitale Gesundheitsanwendungen: Chancen und Risiken von Telemedizin, e- und mHealth sowie Digital Therapeutics, https://www.parlament.gv.at/fachinfos/rlw/Digitale-Gesundheitsanwendungen (2022, accessed 5 October 2023).
- 7.Spitzenverband Digitale Gesundheitsversorgung. Digitale Gesundheitsanwendungen in der Praxis: Was sind Digitale Gesundheitsanwendungen und wie werden sie verordnet?, https://digitalversorgt.de/wp-content/uploads/2023/01/ (2023, accessed 5 October 2023).
- 8.Gan DZQ, McGillivray L, Larsen ME, et al. Technology-supported strategies for promoting user engagement with digital mental health interventions: a systematic review. Digital Health 2022; 8: 1–27, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=157224448&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Randolph J. A Guide to Writing the Dissertation Literature Review, 2009.
- 10.Bettany-Saltikov J, McSherry R. How to do a systematic literature review in nursing: A step-by-step guide. 2nd ed. London: McGraw-Hill Education Open University Press, 2016. [Google Scholar]
- 11.Hawker S, Payne S, Kerr C, et al. Appraising the evidence: reviewing disparate data systematically. Qual Health Res 2002; 12: 1284–1299. [DOI] [PubMed] [Google Scholar]
- 12.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Br Med J 2009; 339: b2535. [PMC free article] [PubMed] [Google Scholar]
- 13.Breil B, Salewski C, Apolinário-Hagen J. Comparing the acceptance of mobile hypertension apps for disease management among patients versus clinical use among physicians: cross-sectional survey. JMIR Cardio 2022; 6: 1–17, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=157924927&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Blut M, Chong AYL, Tsigna Z, et al. Meta-analysis of the unified theory of acceptance and use of technology (UTAUT): challenging its validity and charting a research agenda in the red ocean. J Assoc Inform Syst 2022; 23: 13–95. [Google Scholar]
- 15.Götzl C, Hiller S, Rauschenberg C, et al. Artificial intelligence-informed mobile mental health apps for young people: a mixed-methods approach on users’ and stakeholders’ perspectives. Child Adolesc Psychiatry Mental Health 2022; 16: 1–19, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edm&AN=160294025&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hafner J, Schönfeld S, Tokgöz P, et al. Digital health interventions in depression care – A survey on acceptance from the perspective of patients, their relatives and health professionals. Healthcare (2227–9032) 2022; 10: N.PAG–N.PAG, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=159871534&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hafner J, Schönfeld S, Tokgöz P, et al. Akzeptanz von digitalen Gesundheitstechnologien bei leichter bis mittelgradiger Depression – Eine qualitative Analyse aus der Perspektive von Betroffenen, Angehörigen und Leistungserbringern. (German). Acceptance of Digital Health Interventions in Light to Moderate Depressive Disorders – A Qualitative Analysis from the Perspective of Affected Persons, Relatives and Health Professionals. (English) 2022; 49: 313–321, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edm&AN=158909217&site=eds-live&scope=site (2022). [DOI] [PubMed] [Google Scholar]
- 18.Löbner M, Stein J, Luppa M, et al. What comes after the trial? An observational study of the real-world uptake of an E-mental health intervention by general practitioners to reduce depressive symptoms in their patients. Int J Environ Res Public Health 2022; 19: 6203, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=157249214&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Murray E, Treweek S, Pope C, et al. Normalisation process theory: a framework for developing, evaluating and implementing complex interventions. BMC Med 2010; 8: 63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schinle M, Erler C, Kaliciak M, et al. Digital health apps in the context of dementia: questionnaire study to assess the likelihood of use among physicians. JMIR Format Res 2022; 6: 1–15, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edm&AN=158071389&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wangler J, Jansky M. Gesundheits-Apps als Instrumente der Prävention? – Eine Interviewstudie zu Potenzialen für das hausärztliche Setting. Digital health applications in primary care – Experiences and observations of general practitioners with regard to the use of DiGA 2020; 15: 340–346, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edssjs&AN=edssjs.1BE619D5&site=eds-live&scope=site (2020). [Google Scholar]
- 22.Wangler J, Jansky M. The use of health apps in primary care – results from a survey amongst general practitioners in Germany. Die Nutzung von Gesundheits-Apps in der Primärversorgung – Ergebnisse einer Umfrage unter Hausärzten in Deutschland 2021; 171: 148–156, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edm&AN=149905919&site=eds-live&scope=site (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wangler J, Jansky M. Digitale Gesundheitsanwendungen (DiGA) in der Primärversorgung – Erfahrungen und Beobachtungen von Hausärzt*innen hinsichtlich der Anwendung von DiGA. Digital health applications in primary care – Experiences and observations of general practitioners with regard to the use of DiGA 2022; 18: 1–9, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edssjs&AN=edssjs.14579F8D&site=eds-live&scope=site (2022). [Google Scholar]
- 24.Wangler J, Jansky M. Welche Potenziale und Mehrwerte bieten DiGA für die hausärztliche Versorgung? – Ergebnisse einer Befragung von Hausärzt*innen in Deutschland. What potential and added value do DiGA offer for primary care? – Results of a survey of general practitioners in Germany 2022; 65: 1–10, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edssjs&AN=edssjs.1DE313EB&site=eds-live&scope=site (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wangler J, Jansky M. Bedeutung und Einsatzpotenziale von Gesundheits-Apps in der diabetologischen Versorgung – Ergebnisse einer Befragungsstudie. (German). Significance and application potential of health apps in diabetological care – results of a survey study. (English) 2023; 18: 69–77, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edm&AN=161723084&site=eds-live&scope=site (2023). [Google Scholar]
- 26.Obermann K. Digitale Gesundheitsanwendungen(DiGA) in der Praxis: Erkenntnisse und Erfahrungen: Ärztinnen und Ärzte im Zukunftsmarkt Gesundheit 2022, Hamburg, 2022.
- 27.D.U.T Digitalisierungs- und Technologiereport Diabetes, Mainz, 2021, https://www.dut-report.de/2020/01/16/aerzteumfrage-2020/
- 28.Wangler J, Jansky M. Welchen Nutzen bringen Gesundheits-Apps für die Primärversorgung? Ergebnisse einer Befragung von Allgemeinmedizinern. Digital health applications in primary care – Experiences and observations of general practitioners with regard to the use of DiGA 2021; 16: 150–156, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edssjs&AN=edssjs.AF787888&site=eds-live&scope=site (2021). [Google Scholar]
- 29.Gerlinger G, Mangiapane N, Sander J. Digitale Gesundheitsanwendungen (DiGA) in der ärztlichen und psychotherapeutischen Versorgung. Chancen und Herausforderungen aus Sicht der Leistungserbringer. (German). Digital health applications (DiGA) in medical and psychotherapeutic care. Opportunities and challenges from the perspective of the healthcare providers. (English) 2021; 64: 1213–1219, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=152814301&site=eds-live&scope=site (2021). [DOI] [PubMed] [Google Scholar]
- 30.Radić M. Digitale Gesundheitsanwendungen: die Akzeptanz steigern. Deutsches Ärzteblatt 2021; 6: 286–292. [Google Scholar]
- 31.Nohl-Deryk P, Brinkmann JK, Gerlach FM, et al. Hürden bei der Digitalisierung der Medizin in Deutschland – eine Expertenbefragung. (German). Apps on Prescription in the Medical Office, but how? A Case-based Problem Outline of Medical-ethical Implications of DHA Usage. (English) 2018; 80: 939–945, http://search.ebscohost.com.pxz.iubh.de:8080/login.aspx?direct=true&db=edb&AN=133112997&site=eds-live&scope=site (2018). [DOI] [PubMed] [Google Scholar]
- 32.Bundesgesundheitsministerium. Kabinettvorlage Digital-Gesetz, 2023, https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Gesetze_und_Verordnungen/GuV/D/Kabinettvorlage_Digital-Gesetz-DigiG.pdf.
- 33.Koerber F, Schneider B, Kreuzenbeck C, et al. HPR72 regulation and reality of the market access process for digital health applications (DiGA) in Germany. Value Health 2023; 26: S266. [Google Scholar]