

Abstract
Background
Digital health technologies (DHTs) are increasingly used in physical stroke rehabilitation to support individuals in successfully engaging with the frequent, intensive, and lengthy activities required to optimize recovery. Despite this, little is known about behavior change within these interventions.
Objective
This scoping review aimed to identify if and how behavior change approaches (ie, theories, models, frameworks, and techniques to influence behavior) are incorporated within physical stroke rehabilitation interventions that include a DHT.
Methods
Databases (Embase, MEDLINE, PsycINFO, CINAHL, Cochrane Library, and AMED) were searched using keywords relating to behavior change, DHT, physical rehabilitation, and stroke. The results were independently screened by 2 reviewers. Sources were included if they reported a completed primary research study in which a behavior change approach could be identified within a physical stroke rehabilitation intervention that included a DHT. Data, including the study design, DHT used, and behavior change approaches, were charted. Specific behavior change techniques were coded to the behavior change technique taxonomy version 1 (BCTTv1).
Results
From a total of 1973 identified sources, 103 (5%) studies were included for data charting. The most common reason for exclusion at full-text screening was the absence of an explicit approach to behavior change (165/245, 67%). Almost half (45/103, 44%) of the included studies were described as pilot or feasibility studies. Virtual reality was the most frequently identified DHT type (58/103, 56%), and almost two-thirds (65/103, 63%) of studies focused on upper limb rehabilitation. Only a limited number of studies (18/103, 17%) included a theory, model, or framework for behavior change. The most frequently used BCTTv1 clusters were feedback and monitoring (88/103, 85%), reward and threat (56/103, 54%), goals and planning (33/103, 32%), and shaping knowledge (33/103, 32%). Relationships between feedback and monitoring and reward and threat were identified using a relationship map, with prominent use of both of these clusters in interventions that included virtual reality.
Conclusions
Despite an assumption that DHTs can promote engagement in rehabilitation, this scoping review demonstrates that very few studies of physical stroke rehabilitation that include a DHT overtly used any form of behavior change approach. From those studies that did consider behavior change, most did not report a robust underpinning theory. Future development and research need to explicitly articulate how including DHTs within an intervention may support the behavior change required for optimal engagement in physical rehabilitation following stroke, as well as establish their effectiveness. This understanding is likely to support the realization of the transformative potential of DHTs in stroke rehabilitation.
Keywords: behavior change, behavior therapy, digital health technology, digital health, digital technology, health behavior, physical and rehabilitation medicine, scoping review, stroke rehabilitation
Introduction
Background
Digital health technologies (DHTs) comprise apps, programs, or software used in the health and social care systems [1]. They are considered to have almost unlimited potential to transform health care interventions and delivery and empower people to take a greater role in their own care and well-being [2,3].
Stroke is one of the leading causes of acquired disability worldwide, with around 12 million people experiencing a stroke each year [4]. Rehabilitation is a complex, multifaceted process [5] that facilitates those with health conditions and disabilities to participate in and gain independence in meaningful life roles [6]. It is considered an essential aspect of health care provision following a stroke [7] as a means to address poststroke impairments, which can involve motor, sensory, and cognitive functions. Changes in the ability to move due to impairment of both movement and sensory function are commonly experienced by people following a stroke [8] and are addressed by physical rehabilitation comprising regular, intensive practice and repetition of movements and tasks [9,10]. Conventional physical rehabilitation often struggles to deliver the intensity required to optimize recovery [11], and over recent years, there has been significant interest in the use of DHTs, such as virtual reality (VR), telerehabilitation, robotics, and activity monitors [12-16], to enhance and increase the intensity of rehabilitation. DHTs can provide a whole intervention or be used as a component of a wider intervention; the term DHT-based intervention has been used within this review to refer to both situations.
For many people who survive a stroke, rehabilitation requires individuals to engage in regular and frequent rehabilitative activities to achieve improvements in function and realize their optimal recovery. This necessitates adjustments to an individual’s behavior [17] over a sustained period of time. Changing behavior is a complex process and is underpinned by a variety of different theories, models, and frameworks [18], such as social cognitive theory [19] or the behavior change wheel framework [20]. Individual activities within a complex intervention that are designed to change behavior can be separated into replicable active components widely referred to as behavior change techniques (BCTs) [21]. Historically, labels applied to BCTs have lacked consensus, resulting in uncertainty and difficulty in comparing interventions. This has been addressed in the behavior change technique taxonomy version 1 (BCTTv1) [22], a classification system of 93 distinct BCTs clustered into 16 groups, which is a well-recognized tool to provide consistency with BCT reporting in interventions. DHTs provide an emerging opportunity to support the behavior change required within physical stroke rehabilitation interventions through facilitators that are embedded within the technology itself that aim to form, alter, or reinforce behaviors [23]. Understanding of this area is limited, with most literature exploring the use of DHTs to support behavior change focused on specific health-related behaviors such as physical activity or healthy eating [24] rather than as a core component of a type of rehabilitation intervention. Motivation is acknowledged to play an integral role in behavior change [25], and it is often assumed that DHTs provide motivation to engage with rehabilitation [26]. However, for this assumption to be realized, the DHTs must be able to support and deliver interventions that facilitate the vital changes in behavior needed to promote prolonged and sustained engagement in stroke rehabilitative activities. Imperative to this is understanding the theories, models, and frameworks that underpin interventions and the BCTs (active components) within the interventions [27-29]. The theories, models, and frameworks alongside the BCTs will be referred to hereinafter as approaches. Within the context of DHT-based physical stroke rehabilitation interventions, approaches to behavior change warrant further investigation.
Aim and Objectives
This scoping review aimed to identify if and how behavior change approaches are incorporated within DHT-based physical stroke rehabilitation interventions. Specifically, it sought to:
Establish if behavior change theories, models, and frameworks, or BCTs, are described when reporting on DHT-based interventions that have been developed or evaluated for use in poststroke physical rehabilitation.
Identify if behavior change theories, models, or frameworks underpin the interventions and which of these are being used.
Identify if the BCTTv1 is being used to report BCTs within interventions.
Determine which BCTs (based on the BCTTv1) can be identified within the interventions.
Explore whether the type of technology influences the techniques used to change behaviors.
Methods
Review Methodology
A scoping review was completed and reported following established guidelines [30,31] and the Preferred Reporting of Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR; Multimedia Appendix 1) [32]. The protocol was registered with the Open Science Framework [33].
Eligibility Criteria
Any published sources that reported a completed primary research study in which a behavior change approach could be identified within a DHT-based physical stroke rehabilitation intervention were included (Multimedia Appendix 2). Physical rehabilitation comprised interventions that addressed an impairment, or sequela of impairment, of sensory function and pain, neuromusculoskeletal and movement-related functions, or voice and speech, as defined by the International Classification of Functioning, Disability, and Health [34]. Completed primary research included all types of studies, both quantitative and qualitative, and no minimum sample size or intervention length was set. The BCTTv1 [22] was used to support the identification of BCTs within the interventions.
Information Sources and Search Strategy
A systematic database search was conducted in Embase, MEDLINE, PsycINFO, CINAHL, Cochrane Database of Systematic Reviews, CENTRAL Register of Controlled Trials, and AMED on March 21, 2023. The search was completed in collaboration with an information specialist who provided support with the development of the free text and thesaurus search terms, created the final search, adjusted the searches for the different databases, and ran the search. It consisted of 4 distinct search streams: behavior change, DHT, physical rehabilitation, and stroke, which were then combined (Multimedia Appendix 3). Searches were restricted to the English language (due to review resources) and by date to search from 2001; the date restriction acknowledges the main time period of DHT growth [35], captures sources reported in systematic reviews of DHTs in stroke rehabilitation [12-16], and is reflected in other scoping literature exploring DHTs [24]. Additional sources were identified by hand searching, including scrutiny of the included source reference lists.
Selection of Sources of Evidence
The titles and abstracts of deduplicated sources from database searches and hand searches were independently screened by 2 reviewers, 1 of whom had completed the BCTTv1 web-based training package [36] to inform decisions made around the use of BCTs. Any conflicts were discussed, and if a consensus was not reached, the source was included for full-text screening. Attempts were made to locate a completed study publication from eligible conference abstracts, protocols, and trial registry entries. Full-text sources were screened independently by 2 reviewers, and disagreements were resolved by a third reviewer. Reasons for full-text exclusion were recorded. EndNote X9 software (Clarivate) and the Rayyan web tool software (Qatar Computing Research Institute) [37] were used to facilitate the source selection process.
Data Charting Process
A review-specific data charting tool was developed and initially piloted using 3 sources by 3 reviewers, and then further developed iteratively throughout the process [30]. Data charting was completed collectively by 2 reviewers. When several sources referred to a single study, these sources were grouped together for data charting, and if a source identified additional sources for further detail of the intervention (eg, a protocol or supplementary material), then this information was also used to support data charting.
Data Items
The data charting tool was developed with reference to the Template for Intervention Description and Replication (TIDieR) checklist [27] and with a focus on the DHT-based intervention and behavior change approaches (Multimedia Appendix 4 [14,38-40]). In the absence of a recognized predefined taxonomy for DHTs, the DHTs used in the sources were charted iteratively by the type of technology [41] from the information provided about the intervention. Over time, DHT categories emerged and were defined (Multimedia Appendix 4). Discrete BCTs were identified from the intervention detail provided using the BCTTv1 [22] (Multimedia Appendix 5 [42]). A pragmatic decision was made that the single reviewer who had completed the BCTTv1 web-based training package [36] would code the interventions to the BCTTv1. Any areas of uncertainty were discussed in detail among the review team.
Synthesis of Results
In accordance with the aims of a scoping review, formal assessments of methodological quality were not completed [30,31]. Findings were synthesized using descriptive statistics facilitated by SPSS Statistics 28.0.0.0 (IBM Corp) and Microsoft Excel (version 2208; Microsoft Corporation) and presented in text, table, and chart formats. The characteristics of the included sources, specifically participant numbers, age, and time since stroke, and intervention details, were summarized to provide contextual information for the review. Time since stroke was based on a published timeline framework [43], which describes the following phases: acute (1-7 days), early subacute (7 days to 3 months), late subacute (3-6 months), and chronic (greater than 6 months).
The behavior change theories, models, or frameworks underpinning the DHT-based interventions and sources where interventions had already been coded to the BCTTv1 were summarized. The use of individual BCTs, as coded by reviewers from intervention descriptions, was briefly summarized; however, the main focus of the BCT synthesis was completed by grouping the BCTs into the 16 BCTTv1 clusters, in order to provide an overview of their use across the sources and allow comparison with other reviews [44,45]. A cluster was only identified once per source, irrespective of the number of individual BCTs within that cluster. Relationships between BCTTv1 clusters and between DHT type and BCTTv1 clusters were descriptively explored. A relationship map was used to visually represent the strength of the connections between the BCTTv1 clusters, with a thicker line indicating that variables were more frequently reported together. No inferential statistical analysis was used.
Results
Selection of Sources of Evidence
From a total of 1973 sources screened, 357 full-text sources were assessed for eligibility, then after grouping sources that referred to a single study, 103 (5%) distinct sources were included in the review [46-148] (Figure 1). Of the 245 sources excluded at full-text screening, 165 (67%) were excluded due to a lack of a behavior change approach.
Figure 1.
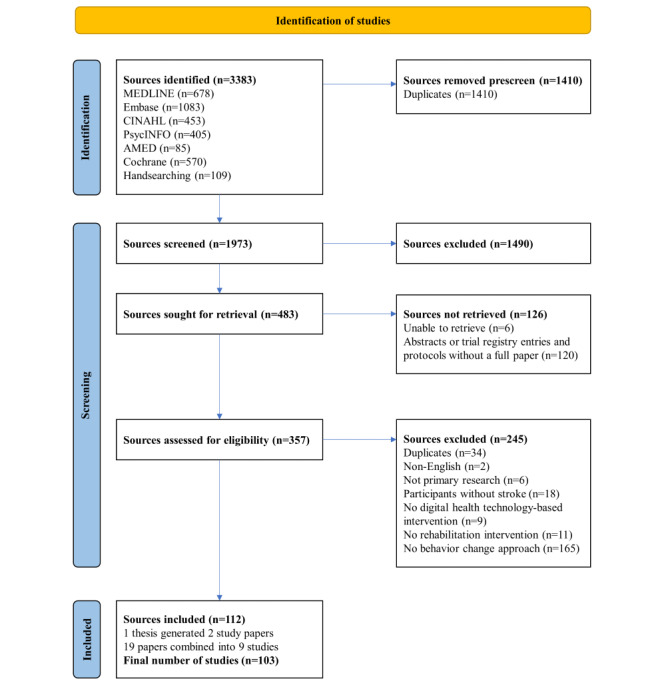
PRISMA (Preferred Reporting of Systematic Reviews and Meta-Analyses) flow diagram of the source selection process.
Characteristics of Sources of Evidence
General
All sources of evidence were studies and will be referred to as such hereinafter. The number of studies in this field has rapidly increased over time (Figure 2), from a single study in 2004 to 8 in 2022, with a peak of 15 in 2021. The majority (86/103, 83%) [47-51,53-56,58,59,61,63-68,71-86,89-95,97-105,107, 109,111,112,114,115,117-126,128-136,138-148] were published in the past 10 years. Most studies took place in North America (41/103, 40%) [46-49,52,55,56,60,64-67,69,70,72,74,76-78,80, 85-88,92,93,97,99,101,108-110,126-129,137,138,141,142,145] and Europe (35/103, 34%) [51,53,54,57,58,62,63,68,71,79, 81-84,89,111,113-125,132,136,140,143,146,147], with the remainder in Asia (16/103, 16%) [50,59,61,91,94,95,98,100, 102-104,107,135,139,144,148], Australasia (9/103, 9%) [75,96,105,106,112,130,131,133,134], Africa (1/103, 1%) [90], and a single multicontinental study (1/103, 1%) [73]. Almost half (45/103, 44%) the studies are reported as feasibility or pilot studies [49,56,58,64,66,68,69,72-74,76,77,79,82-84,89,90,92,93, 95,97,100-104,106,108,114,116,117,119,122,124-126,131,134,136,138, 139,141,143,147]. Other study designs included randomized controlled trials (20/103, 19%) [50,51,60,61,65,75,80,85,86, 91,107,109,112,128-130,137,144,146,148], single session investigations (19/103, 18%) [47,52,57,59,71,78,87,88, 98,110,115,118,120,123,127,132,133,135,142], nonrandomized experimental designs (13/103, 13%) [53-55,62,63,67,81,94, 96,99,105, 113,145], case studies (4/103, 4%) [46,48,70,140], and realist evaluations (2/103, 2%) [111,121].
Figure 2.
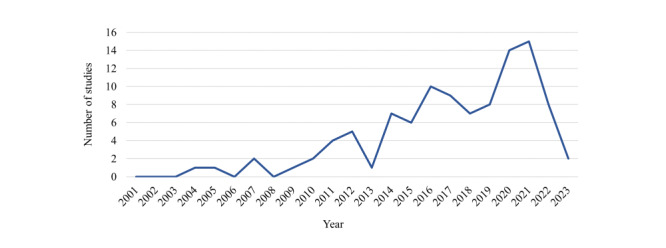
Number of studies by publication year (January 1, 2001, to March 21, 2023).
Participants
There were a total of 2825 participants in the 103 included studies. Studies tended to be small, with a median of 16 participants and a range of 1-188. Only half (55/103, 53%) the studies [46-48,50,56,57,59,61,64,67,69-72,78,79,82,87,88,92, 93,95-99,101,102,105,106,108,111-121,123-127,134, 138-140,142,143,145, 147] reported the minimum and maximum age of participants, which ranged from 17 to 99 years. Over three-quarters (83/103, 81%; 2508 participants) of studies reported the time since the onset of stroke. Of these 83 studies, 1 (1%; 48 participants) study [91] was conducted in the acute phase, 14 (17%; 504 participants) studies [60,61,68,74,79,92, 100,102,109,114,133,144,146,148] were conducted in the early subacute phase, 11 (13%; 316 participants) studies [59,65,66,72, 75,76, 81,104,107,121,134] were conducted in the late subacute phase, and 57 (69%; 1640 participants) studies [46,48,49,51, 53,54,57,63,64,67,69,70,73,78,80,82,84,85,88,89,93-99, 101,103,105,106,108,111-113,117-120,122-125,127-131,136-142, 145,147] were conducted in the chronic phase [43].
Study Intervention
An overview of study intervention characteristics is provided (Table 1). Interventions were focused on upper limb rehabilitation in almost two-thirds (65/103, 63%) of the studies [46-49,51,54-59,62-65,68,71,72,74,75,77-81,85-88,92,95, 96,99,101-103,105-108,110,112,113,116-118,121, 123-125,127,128,132,133,135-137,139-142,144-147]. Nearly all interventions (96/103, 93%) [46-80,84-94,96-117,119-121, 124-148] were delivered to individual participants, with over half (62/103, 60%) [46-50,53-58,60,61,64-70,72,74-77, 79,80,82-86,89,90,93,94,96,97,99,101,105,111, 112,116,117,119-122,126,129-131,134,136,138, 139,141,143-145,147] delivered fully or partly in the participant’s homes. Two-thirds (70/103, 68%) of studies [46-50,52-54,57,60,62,63,65-74,76-84,86-93,98,100,102, 104,108,109,112-115,117,118,120,122-125,129-131, 135-138, 140-142,144-146,148] included partial or full supervision of the intervention, with this predominately being provided face-to-face (48/70, 69%) [46,47,52,57,60,62,63,67,68,71,73, 78,81-84,86-89,91,92,98,100,102,104,108,109,112-115,117, 118,120,122-125,135-137,140,142,144-146,148]. Interventions lasted between a single session and 26 weeks.
Table 1.
Intervention characteristics.
| Intervention characteristics and details of characteristics | Studies (n=103), n (%) | ||
| Intervention focus | |||
|
|
Upper limb | 65 (63) | |
|
|
Multifocus | 13 (13) | |
|
|
Physical activity | 10 (10) | |
|
|
Mobility | 5 (5) | |
|
|
Activities of daily living | 4 (4) | |
|
|
Lower limb | 4 (4) | |
|
|
Balance | 1 (1) | |
|
|
Speech | 1 (1) | |
| Individual or group intervention | |||
|
|
Individual | 96 (93) | |
|
|
Group | 2 (2) | |
|
|
Combination | 4 (4) | |
|
|
Not reported | 1 (1) | |
| Intervention location | |||
|
|
Home | 48 (47) | |
|
|
Home and another setting | 14 (14) | |
|
|
Health care setting | 19 (18) | |
|
|
Research setting | 12 (12) | |
|
|
Not reported | 10 (10) | |
| Supervision | |||
|
|
Both supervised and unsupervised | 38 (37) | |
|
|
Supervised | 32 (31) | |
|
|
Unsupervised | 23 (22) | |
|
|
Not reported | 10 (10) | |
| Supervision contact | |||
|
|
Face-to-face | 48 (47) | |
|
|
Remote | 12 (12) | |
|
|
Combination (F2Fa and remote) | 10 (10) | |
|
|
Not supervised or unreported | 33 (32) | |
| Number of DHTb types | |||
|
|
1 | 57 (55) | |
|
|
2 | 30 (29) | |
|
|
3 | 16 (16) | |
| DHT type | |||
|
|
VRc | 58 (56) | |
|
|
App | 31 (30) | |
|
|
Sensor | 17 (17) | |
|
|
Activity monitor | 16 (16) | |
|
|
Audio-video platform | 15 (15) | |
|
|
Robotics | 13 (13) | |
|
|
Messaging platform | 11 (11) | |
|
|
Other | 4 (4) | |
aF2F: face-to-face.
bDHT: digital health technology.
cVR: virtual reality.
Of the 103 studies, over half (n=57, 55%) of the studies [46,47,51-54,57,61,63,67,68,70,71,73,75-78,81,84-86,88-91,93, 95,96,98,100,102-104,106,109,112,114,115,123-126,129,130,132,133,135-138, 140,143-147] included 1 type of DHT, 30 (29%) studies [48,49,55,56,58-60,62,64,69,83,92,94,97,99,101,105,107,108,110, 111,113,116,118,121,122,127,128, 139,142] included 2 types, and 16 (16%) studies [50,65,66,72,74,79, 80,82,87,117,119,120, 131,134,141,148] included 3 types. VR was the most frequently used DHT (58/103, 56%) [46-49,51-53,57,59,62,63, 65,66,69,71,72,74,77,78, 80,81,84-89,92,95,96,98,102-104,106, 112,113,115,117-120,123-128,132,135-137,140, 142,143,146-148] followed by apps (31/103, 30%) [50,55,56,58,61,64-66,72,74,75,79,82,83,94,97,99,101,105,108,111, 114,116,119-122,131,134,139,141]. Further information on intervention characteristics with detail on associated citations is available (Multimedia Appendix 6 [46-148]).
Synthesis of Results
Behavior Change Theories, Models, and Frameworks
Most studies (93/103, 90%) [46-49,51-62,64-73,75-89,91-93, 96-106,108-115,117-137,139, 140,142-148] endeavored to link the intervention to behavior change; however, in the majority of these studies (75/93, 81%) [46,51-56,58-62,64-69,71-73,75, 77-89,91-93,96,97,99-101,103-106,108,110,112,114,115,117-120, 123,124,127,128,131-137,139,140,142-144,146-148], this explanation was centered on the reporting of the techniques perceived to change behaviors without direct reference to use of the BCTTv1 or on the reporting of a component of the intervention or the whole of the intervention as motivating. These explanations lack detail on how or why this influences behavior change. Examples of this included “the app also provided performance feedback, allowing the user to compare their current performance against their score from the previous session” (Bhattacharjya et al [56]) and “games motivate patients to engage in enjoyable play behavior” (Cramer et al [66]). A limited number of studies (18/103, 17%) [47-49,57,70,76,98, 102,109,111,113,121,122,125,126,129,130,145] articulated 1 or more theories, models, or frameworks of behavior change. While it is acknowledged that the BCTTv1 is a taxonomy framework rather than a theoretical framework, for the purpose of this review, it has been included as a framework for behavior change. A total of 13 different theories, models, or frameworks were identified within these 18 studies, with social cognitive theory being the most frequently reported (6/18, 33%) [76,109,111,121,129,130], followed by the behavior change technique taxonomy (4/18, 22%) [48,49, 122,129], game design theory (3/18, 17%) [47,57,125], operant conditioning (3/18, 17%) [47,98,121], and self-determination theory (3/18, 17%) [48,49,126]. Further information on behavior change theories, models, and frameworks, with details on associated citations, is available (Multimedia Appendix 7 [47-49,57,70,76,98,102, 109,111,113,121,122,125,126,129,130,145]).
Behavior Change Techniques
Despite 4 studies acknowledging the BCTTv1, explicit BCTTv1 codes were only reported in 2 studies (2/103, 2%) [48,122]. However, a third study (1/103, 1%) mapped the techniques used to change behavior directly to the transtheoretical model [145]. There was a median of 3 (range 1-14) individual BCTs coded per study, with a total of 383 BCTs across the 103 studies. The most frequently identified individual BCTs were feedback on behavior and nonspecific reward (Multimedia Appendix 8).
There was also a median of 3 (range 1-8) BCTTv1 clusters per study, with a total of 288 clusters coded across the 103 studies. The most frequently used of the 16 possible clusters were feedback and monitoring (88/103, 85%) [46-60,62-69, 71-74,76,78-80,82-92,94-106,108-113,116,117,119-129,134-146,148], reward and threat (56/103, 54%) [46-49,51-53,55-57,62,65,69, 71,72,74,77,80,81,85,86,88,89,91,92,95,96,98,102,103,106-108,112,113,115, 117-119,121-125,128,132,134-137,140,142,143,146-148], goals and planning (33/103, 32%) [49,58,60,65-68,70,72,74,76,79,80, 82,83,90,91,93,94,97,100,109,111,112,121,122,126,129,130,134,138, 141,145], and shaping knowledge (33/103, 32%) [46,48,50, 53-56,58,60,61,64-72,74,75,86,94,97,101-103, 108,111,113,114,120,129-131,139-141]. Other BCTTv1 clusters used were social support (24/103, 23%) [48,49,58,60,64,67,70,72,73,79,80,82,84,90,93, 101,108,117,119,129-131,134,141], comparison of behavior (23/103, 22%) [46,50,53,54,60,61,64-66,74,75,81,86,101, 104,111,114,118,122,123,125,131,139], associations (16/103, 15%) [58,60,65,66,68,75,80,83,87,90,110,120,131,133,139,144], repetition and substitution (6/103, 6%) [60,82,109, 122,129,130], scheduled consequences (3/103, 3%) [47, 80,88], natural consequences (2/103, 2%) [129,138], comparison of outcomes (2/103, 2%) [47,133], antecedents (1/103, 1%) [60], and self-belief (1/103, 1%) [70]. The clusters of regulation, identity, and covert learning were not identified. Within the context of the review, it was noted that the reward and threat cluster only included reward-based BCTs. A tabulated summary and graphical representation of the BCTTv1 clusters is available (Multimedia Appendix 9 [46-148]).
The exploration of clusters that were reported together in an intervention (Figure 3) identified the strongest relationship between the clusters of feedback and monitoring and reward and threat. Clear links were also identified between feedback and monitoring and 4 other clusters: goals and planning, shaping knowledge, social support, and comparison of behavior, and between the shaping knowledge and comparison of behavior clusters.
Figure 3.
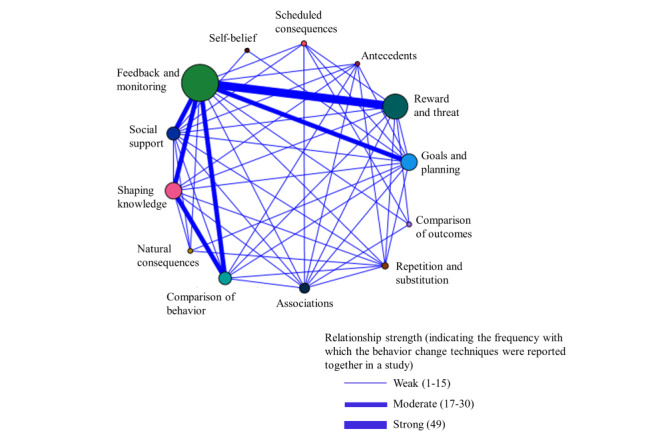
Relationships between behavior change technique taxonomy clusters.
Behavior Change Techniques and Digital Health Technology
The feedback and monitoring cluster was reported most frequently for all types of DHT (Figure 4), with the greatest proportion of this cluster in robotics (11/25, 44%) [59,62,87,92,110,113,117,127, 128,142,148], VR (52/148, 35%) [46-49,51-53,57,59,62,63,65,66,69,71,72,74,78,80,84-89,92, 95,96,98,102-104,106,112,113,117,119,120,123- 135-137,140, 142,143,146,148], and sensors (17/48, 35%) [50,55,56,87,94,99, 101,105,108,110, 111,116,119-121,134,141]. Robotics and VR also often used the reward and threat cluster (9/25, 36% [62,92, 107,113,117,118,128,142,148] and 48/148, 32% [46-49,51-53, 57,62,65,69,71,72,74,77,80,81,85,86,88,89,92,95,96,98,102,103,106, 112,113,115,117-119,123-125,128,132,135-137,140,142,143,146-148], respectively), while the goals and planning cluster was a dominant second cluster in activity monitors (13/53, 25%) [67,68,76,79, 80,82,91,100, 109,122,129,138,145].
Figure 4.
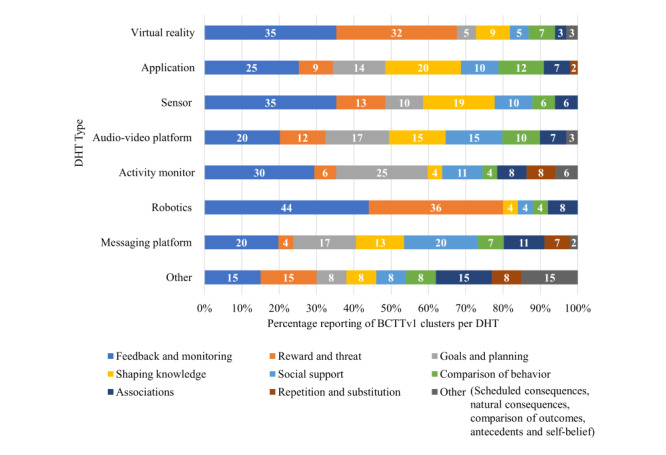
Percentage of behavior change technique taxonomy clusters use across the different types of digital health technology. BCTTv1: behavior change technique taxonomy version 1; DHT: digital health technology.
Discussion
Summary of Evidence
This scoping review provides a comprehensive overview of approaches used to support changes in behavior in DHT-based physical stroke rehabilitation interventions. Research in this field is in its infancy, with the predominance of studies in this review being described as pilot or feasibility studies with limited participants.
Despite using comprehensive behavior change search terms, only a limited number (103/1973, 6%) of screened sources were included. Over two-thirds of full-text sources were excluded as they did not describe or refer to any behavior change theories, models, or frameworks or BCTs, suggesting that in general, explicit behavior change approaches are not reported as being integral to DHT-based physical stroke rehabilitation.
Only 18 (17%) of the 103 included studies articulated a theory, model, or framework to underpin the intervention, which aimed to change behavior, despite widely published recommendations about the importance of overt use of theory when developing, evaluating, and reporting interventions [27,29], including those related to behavior change [28]. The proportion of studies articulating a behavior change theory, model, or framework in this work is significantly lower than review findings in non-rehabilitation DHT-based interventions that have sought to influence specific behaviors such as physical activity or weight control [24,44]. These reviews have identified up to two-thirds of sources reporting a theory, model, or framework. However, our findings mirror the relative absence of behavior change theories, models, and frameworks in rehabilitation interventions more generally, irrespective of whether they use digital technology [149] or not [45], and it is widely recognized that the complex nature of rehabilitation often results in the essential characteristics of interventions being poorly defined [150]. Consistent with our findings in these other reviews, a variety of theories, models, and frameworks were found to underpin interventions, with social cognitive theory being the most frequently reported [24,44,45,149]. The explicit description of BCTs using the BCTTv1 within DHT-based physical stroke rehabilitation interventions is also poorly reported (2%), despite a significant proportion of the sources being dated after the publication of the BCTTv1 in 2013 [22]. This lack of acknowledgment of behavior change approaches impedes the accumulation of knowledge within this field.
It is important that both the underpinning theory and BCTs are reported so the mechanisms by which the BCTs elicit change can be better understood [21]. The general assumption that the motivational and captivating aspects of DHTs will promote prolonged and repeated engagement with rehabilitative activities, in particular in those DHTs that incorporate game design [151], risks suboptimal outcomes for patients and wasted investment of time and money if the mechanisms by which the DHT elicits change are not considered.
When exploring which BCT clusters featured within the reviewed DHT-based interventions, the findings relating to the commonly used clusters of feedback and monitoring, goals and planning, and shaping knowledge are consistent with findings from DHT-based interventions to change a specific behavior [44] and non-DHT–based rehabilitation [45]. However, a novel finding in our review was the frequent identification of the reward and threat cluster, although it was noted that all techniques related to reward and none to threat. A large number of studies in this review used VR technology, which frequently incorporates gamified tasks or gameplay. Reward is an integral part of game design theory alongside feedback [152], and so it is perhaps unsurprising that the feedback and monitoring, and reward and threat clusters dominated and an association between these 2 clusters was seen.
Limitations
Rehabilitation is a process that comprises multiple behaviors and so exploring approaches to change behavior within this context was complicated. There were challenges in searching and screening sources for inclusion as few studies explicitly reported approaches to change behavior, and there is a similarity in the vocabulary used within behavior change and other theoretical approaches (eg, “feedback,” which is used within motor learning). Similarly, only a very small proportion of studies explicitly reported BCTs within interventions. The lack of clear reporting of behavior change introduces the risk that sources may be omitted during both the searching and screening process highlighting the difficulty of comprehensively reviewing this field of work. An inclusive approach to screening reduced the risk of erroneously excluding sources, but it is perhaps inevitable that the sources included reflect those studies that have reported a behavior change approach rather than all studies that have used one.
This lack of clear BCT reporting also posed challenges for intervention coding. The use of the BCTTv1 aimed to ensure the review used a generalizable nomenclature to describe BCTs, and the 1 reviewer who had completed BCTTv1 training coded all the interventions. It is acknowledged that decisions made in the application of the BCTTv1 within the context of the review will have introduced some subjectivity in intervention coding, which will ultimately influence the review findings. Although the coding process could have been made more robust by having a second reviewer trained in the BCTTv1 also code the interventions, regular and extensive discussions between all members of the review team took place with the aim of ensuring consistency with the coding process. Clear documentation as to how the BCTTv1 was used within this review (Multimedia Appendix 5) supports transparency as to the decisions made and the reproducibility of the review.
The absence of a recognized predefined taxonomy for DHTs posed a challenge when categorizing the DHT interventions, acknowledging that the distinction between the categories used to present the results is open to interpretation. A description of how the reviewers interpreted these categories is provided (Multimedia Appendix 4).
Implications for Research
Future studies aimed at developing and evaluating DHT-based rehabilitation interventions, including those relating to physical stroke rehabilitation, need to ensure there is explicit recognition and reporting of the specific approaches used to change behavior, articulating both the theory on which the intervention is based and how the intervention plans to deliver the change in behavior using universally recognized terminology. This should be reported as part of a program theory and potential mechanisms of action, which are key parts of developing and evaluating complex interventions [29]. This detailed reporting would further support an understanding of how changes in behavior could be best enabled by DHT-based rehabilitation interventions and how this contributes to changes in patient outcomes. It would also enable further evaluation of the optimal behavioral components of interventions, enabling patients to use and clinicians to deliver the most effective DHT-based rehabilitative interventions. More generally, as the use of DHTs expands, there is an urgent need for some form of taxonomy to categorize and clearly define the different types of DHTs to facilitate consistent reporting, replication, and comparison of DHT-based interventions.
Conclusion
This novel and original review is the first to explore if and how approaches to change behavior are incorporated within DHT-based physical stroke rehabilitation. It demonstrates that a minority of studies report using approaches to change behavior within this context, despite these changes in behavior being vital to meet the demands of rehabilitative activities. Those who do report behavior change often lack the underpinning detail as to how the DHT-based intervention will facilitate these changes. In order for DHT-based interventions to realize their potential within rehabilitation and their impact on patient outcomes, approaches to change behavior must be embedded in the intervention and appropriately reported.
Acknowledgments
The authors would like to thank Catherine Harris (Information Specialist, University of Central Lancashire) for her assistance in developing the search strategy and running the searches, and Rebekah Murray (Undergraduate Research Intern, University of Central Lancashire) for her support with aspects of the screening and data charting process.
This work was funded by a UK Research and Innovation Future Leaders Fellowship (grant MR/T022434/1).
Abbreviations
- BCT
behavior change technique
- BCTTv1
behavior change technique taxonomy version 1
- DHT
digital health technology
- PRISMA-ScR
Preferred Reporting of Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
- TIDieR
Template for Intervention Description and Replication
- VR
virtual reality
Preferred Reporting of Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist.
Inclusion and exclusion criteria.
Full search strategy as used in Medline.
Data charting tool.
Review-specific behavior change technique taxonomy coding decisions.
Intervention characteristics (with associated references).
Behavior change theories, models, and frameworks reported (with associated references).
Individual behavior change techniques coded.
Behavior change technique taxonomy clusters identified (with associated references).
Data Availability
All data supporting this study are openly available from the University of Central Lancashire repository [153].
Footnotes
Authors' Contributions: RCS conceived the review focus and oversaw the work. HJG developed the review design and search strategy. HJG, KAJ, and RCS completed the screening of the identified sources. HJG and KAJ piloted the data charting tool. HJG completed the data charting, data analysis, and the initial manuscript draft. KAJ and RCS reviewed and made substantial contributions to the manuscript. All authors approved the final manuscript.
Conflicts of Interest: None declared.
References
- 1.Evidence standards framework for digital health technologies. National Institute of Clinical Excellence (NICE) 2018. [2022-01-25]. https://tinyurl.com/mpmrwrwx .
- 2.Castle-Clark S. The NHS at 70: What will new technology mean for the NHS and its patients? Kings Fund. 2018. [2024-04-05]. https://tinyurl.com/44k9fmat .
- 3.Topel E. The Topol review: preparing the healthcare workforce to deliver the digital future. Health Education England, NHS. 2019. [2022-01-19]. https://topol.hee.nhs.uk/
- 4.GBD 2019 Stroke Collaborators Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi: 10.1016/S1474-4422(21)00252-0. https://air.unimi.it/handle/2434/866438 .S1474-4422(21)00252-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wade DT. What is rehabilitation? An empirical investigation leading to an evidence-based description. Clin Rehabil. 2020;34(5):571–583. doi: 10.1177/0269215520905112. https://journals.sagepub.com/doi/abs/10.1177/0269215520905112?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rehabilitation. World Health Organisation. 2023. [2023-05-04]. https://www.who.int/news-room/fact-sheets/detail/rehabilitation .
- 7.Grefkes C, Fink GR. Recovery from stroke: current concepts and future perspectives. Neurol Res Pract. 2020;2:17. doi: 10.1186/s42466-020-00060-6. https://europepmc.org/abstract/MED/33324923 .60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lawrence ES, Coshall C, Dundas R, Stewart J, Rudd AG, Howard R, Wolfe CD. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke. 2001;32(6):1279–1284. doi: 10.1161/01.str.32.6.1279. https://www.ahajournals.org/doi/10.1161/01.STR.32.6.1279 . [DOI] [PubMed] [Google Scholar]
- 9.National clinical guideline for stroke for the United Kingdom and Ireland. Intercollegiate Stroke Working Party. 2023. [2023-05-02]. https://tinyurl.com/yxy6b9tp .
- 10.Veerbeek JM, van Wegen E, van Peppen R, van der Wees PJ, Hendriks E, Rietberg M, Kwakkel G. What is the evidence for physical therapy poststroke? a systematic review and meta-analysis. PLoS One. 2014;9(2):e87987. doi: 10.1371/journal.pone.0087987. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0087987 .PONE-D-13-44188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lang CE, Macdonald JR, Reisman DS, Boyd L, Kimberley TJ, Schindler-Ivens SM, Hornby TG, Ross SA, Scheets PL. Observation of amounts of movement practice provided during stroke rehabilitation. Arch Phys Med Rehabil. 2009;90(10):1692–1698. doi: 10.1016/j.apmr.2009.04.005. https://europepmc.org/abstract/MED/19801058 .S0003-9993(09)00353-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Laver KE, Lange B, George S, Deutsch JE, Saposnik G, Crotty M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev. 2017;11(11):CD008349. doi: 10.1002/14651858.CD008349.pub4. https://europepmc.org/abstract/MED/29156493 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Laver KE, Adey-Wakeling Z, Crotty M, Lannin NA, George S, Sherrington C. Telerehabilitation services for stroke. Cochrane Database Syst Rev. 2020;1(1):CD010255. doi: 10.1002/14651858.CD010255.pub3. https://europepmc.org/abstract/MED/32002991 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lynch EA, Jones TM, Simpson DB, Fini NA, Kuys SS, Borschmann K, Kramer S, Johnson L, Callisaya ML, Mahendran N, Janssen H, English C. Activity monitors for increasing physical activity in adult stroke survivors. Cochrane Database Syst Rev. 2018;7(7):CD012543. doi: 10.1002/14651858.CD012543.pub2. https://europepmc.org/abstract/MED/30051462 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mehrholz J, Pohl M, Platz T, Kugler J, Elsner B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev. 2018;9(9):CD006876. doi: 10.1002/14651858.CD006876.pub5. https://europepmc.org/abstract/MED/30175845 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mehrholz J, Thomas S, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2020;10(10):CD006185. doi: 10.1002/14651858.CD006185.pub5. https://europepmc.org/abstract/MED/33091160 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jones F, Riazi A. Self-efficacy and self-management after stroke: a systematic review. Disabil Rehabil. 2011;33(10):797–810. doi: 10.3109/09638288.2010.511415. [DOI] [PubMed] [Google Scholar]
- 18.National Institute of Clinical Excellence. UK: National Institute of Clinical Excellence (NICE); 2007. [2024-04-05]. Behaviour change: general approaches. https://tinyurl.com/yfthycch . [Google Scholar]
- 19.Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- 20.Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi: 10.1186/1748-5908-6-42. https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-6-42 .1748-5908-6-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carey RN, Connell LE, Johnston M, Rothman AJ, de Bruin M, Kelly MP, Michie S. Behavior change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med. 2019;53(8):693–707. doi: 10.1093/abm/kay078. https://europepmc.org/abstract/MED/30304386 .5126198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, Eccles MP, Cane J, Wood CE. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95. doi: 10.1007/s12160-013-9486-6. https://core.ac.uk/reader/191129821?utm_source=linkout . [DOI] [PubMed] [Google Scholar]
- 23.Oinas-Kukkonen H. A foundation for the study of behavior change support systems. Pers Ubiquit Comput. 2012;17(6):1223–1235. doi: 10.1007/s00779-012-0591-5. [DOI] [Google Scholar]
- 24.Taj F, Klein MCA, van Halteren A. Digital health behavior change technology: bibliometric and scoping review of two decades of research. JMIR Mhealth Uhealth. 2019;7(12):e13311. doi: 10.2196/13311. https://mhealth.jmir.org/2019/12/e13311/ v7i12e13311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.West R, Michie S. A Guide to Development and Evaluation of Digital Behaviour Change Interventions in Healthcare. London: Silverback Publishing; 2016. [Google Scholar]
- 26.Lewis GN, Rosie JA. Virtual reality games for movement rehabilitation in neurological conditions: how do we meet the needs and expectations of the users? Disabil Rehabil. 2012;34(22):1880–1886. doi: 10.3109/09638288.2012.670036. [DOI] [PubMed] [Google Scholar]
- 27.Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon-Woods M, McCulloch P, Wyatt JC, Chan AW, Michie S. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687. doi: 10.1136/bmj.g1687. https://core.ac.uk/reader/19913708?utm_source=linkout .bmj.g1687 [DOI] [PubMed] [Google Scholar]
- 28.Michie S, Prestwich A. Are interventions theory-based? development of a theory coding scheme. Health Psychol. 2010;29(1):1–8. doi: 10.1037/a0016939. https://eprints.whiterose.ac.uk/76353/ 2010-00152-001 [DOI] [PubMed] [Google Scholar]
- 29.Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, Boyd KA, Craig N, French DP, McIntosh E, Petticrew M, Rycroft-Malone J, White M, Moore L. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061. doi: 10.1136/bmj.n2061. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=34593508 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi: 10.1097/XEB.0000000000000050. https://journals.lww.com/ijebh/fulltext/2015/09000/guidance_for_conducting_systematic_scoping_reviews.5.aspx . [DOI] [PubMed] [Google Scholar]
- 31.Peters MDJ, Godfrey CM, McInerney P, Munn Z, Tricco AC, Khalil H. Scoping Reviews (2020 version) In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Adelaide, Australia: JBI; 2020. [2022-11-15]. [DOI] [Google Scholar]
- 32.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi: 10.7326/M18-0850. https://www.acpjournals.org/doi/abs/10.7326/M18-0850?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .2700389 [DOI] [PubMed] [Google Scholar]
- 33.Gooch H, Stockley R, Jarvis K. Behaviour change approaches within digital health technology-based interventions in physical rehabilitation following stroke: a scoping review protocol Version 2 081122. OSF Registries. 2022. [2022-11-15]. https://osf.io/yjn5g .
- 34.ICF checklist. World Health Organisation. 2003. [2022-01-19]. https://tinyurl.com/5fz6krew .
- 35.Hillyer M. How has technology changed—and changed us—in the past 20 years? World Economic Forum. 2020. [2023-10-18]. https://tinyurl.com/5n74wsym .
- 36.Online training. BCT Taxonomy v1. 2022. [2022-03-08]. http://www.bct-taxonomy.com/
- 37.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi: 10.1186/s13643-016-0384-4. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0384-4 .10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wadley M, Bradbury M, Stockley R. Virtual reality. The Chartered Society of Physiotherapy. [2024-03-29]. https://www.csp.org.uk/professional-clinical/digital-physiotherapy/virtual-reality .
- 39.Cambridge dictionary. Cambridge University Press and Assessment. [2024-03-29]. https://tinyurl.com/2f2mx6kz .
- 40.Weber LM, Stein J. The use of robots in stroke rehabilitation: A narrative review. NeuroRehabilitation. 2018;43(1):99–110. doi: 10.3233/NRE-172408.NRE172408 [DOI] [PubMed] [Google Scholar]
- 41.English C, Ceravolo MG, Dorsch S, Drummond A, Gandhi DB, Green JH, Schelfaut B, Verschure P, Urimubenshi G, Savitz S. Telehealth for rehabilitation and recovery after stroke: state of the evidence and future directions. Int J Stroke. 2022;17(5):487–493. doi: 10.1177/17474930211062480. [DOI] [PubMed] [Google Scholar]
- 42.Taub E, Crago JE, Burgio LD, Groomes TE, Cook EW, DeLuca SC, Miller NE. An operant approach to rehabilitation medicine: overcoming learned nonuse by shaping. J Exp Anal Behav. 1994;61(2):281–293. doi: 10.1901/jeab.1994.61-281. https://europepmc.org/abstract/MED/8169577 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bernhardt J, Hayward KS, Kwakkel G, Ward NS, Wolf SL, Borschmann K, Krakauer JW, Boyd LA, Carmichael ST, Corbett D, Cramer SC. Agreed definitions and a shared vision for new standards in stroke recovery research: the Stroke Recovery and Rehabilitation Roundtable taskforce. Int J Stroke. 2017;12(5):444–450. doi: 10.1177/1747493017711816. https://journals.sagepub.com/doi/abs/10.1177/1747493017711816?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PubMed] [Google Scholar]
- 44.Asbjørnsen RA, Smedsrød ML, Solberg Nes L, Wentzel J, Varsi C, Hjelmesæth J, van Gemert-Pijnen JE. Persuasive system design principles and behavior change techniques to stimulate motivation and adherence in electronic health interventions to support weight loss maintenance: scoping review. J Med Internet Res. 2019;21(6):e14265. doi: 10.2196/14265. https://www.jmir.org/2019/6/e14265/ v21i6e14265 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bayly J, Wakefield D, Hepgul N, Wilcock A, Higginson IJ, Maddocks M. Changing health behaviour with rehabilitation in thoracic cancer: a systematic review and synthesis. Psychooncology. 2018;27(7):1675–1694. doi: 10.1002/pon.4684. [DOI] [PubMed] [Google Scholar]
- 46.Alankus G, Proffitt R, Kelleher C, Engsberg J. Stroke therapy through motion-based games: a case study. ACM Trans Access Comput. 2011;4(1):1–35. doi: 10.1145/2039339.2039342. [DOI] [Google Scholar]
- 47.Alankus G, Kelleher C. Reducing compensatory motions in motion-based video games for stroke rehabilitation. Hum Comput Interact. 2015;30(3-4):232–262. doi: 10.1080/07370024.2014.985826. [DOI] [Google Scholar]
- 48.Allegue DR, Kairy D, Higgins J, Archambault PS, Michaud F, Miller W, Sweet SN, Tousignant M. A personalized home-based rehabilitation program using exergames combined with a telerehabilitation app in a chronic stroke survivor: mixed methods case study. JMIR Serious Games. 2021;9(3):e26153. doi: 10.2196/26153. https://games.jmir.org/2021/3/e26153/ v9i3e26153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Allegue DR, Higgins J, Sweet SN, Archambault PS, Michaud F, Miller W, Tousignant M, Kairy D. Rehabilitation of upper extremity by telerehabilitation combined with exergames in survivors of chronic stroke: preliminary findings from a feasibility clinical trial. JMIR Rehabil Assist Technol. 2022;9(2):e33745. doi: 10.2196/33745. https://rehab.jmir.org/2022/2/e33745/ v9i2e33745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Asano M, Tai BC, Yeo FY, Yen SC, Tay A, Ng YS, de Silva DA, Caves K, Chew E, Hoenig H, Koh GC. Home-based tele-rehabilitation presents comparable positive impact on self-reported functional outcomes as usual care: the Singapore Tele-technology Aided Rehabilitation in Stroke (STARS) randomised controlled trial. J Telemed Telecare. 2021;27(4):231–238. doi: 10.1177/1357633X19868905. [DOI] [PubMed] [Google Scholar]
- 51.Ballester BR, Maier M, Mozo RMSS, Castañeda V, Duff A, Verschure PFMJ. Counteracting learned non-use in chronic stroke patients with reinforcement-induced movement therapy. J Neuroeng Rehabil. 2016;13(1):74. doi: 10.1186/s12984-016-0178-x. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-016-0178-x .10.1186/s12984-016-0178-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Bardack A, Bhandari P, Doggett J, Epstein M, Gagliolo N, Graff S, Li E, Petro E, Sailey M, Salaets N, Tousley B, Turner J. EMG biofeedback videogame system for the gait rehabilitation of hemiparetic individuals. Digital Repository at the University of Maryland. 2010. [2023-02-27]. https://drum.lib.umd.edu/bitstream/handle/1903/10082/CHIP.pdf?sequence=1&isAllowed=y .
- 53.Bellomo RG, Paolucci T, Saggino A, Pezzi L, Bramanti A, Cimino V, Tommasi M, Saggini R. The WeReha Project for an innovative home-based exercise training in chronic stroke patients: a clinical study. J Cent Nerv Syst Dis. 2020;12:1179573520979866. doi: 10.1177/1179573520979866. https://journals.sagepub.com/doi/10.1177/1179573520979866?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_1179573520979866 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Benvenuti F, Stuart M, Cappena V, Gabella S, Corsi S, Taviani A, Albino A, Marchese SS, Weinrich M. Community-based exercise for upper limb paresis: a controlled trial with telerehabilitation. Neurorehabil Neural Repair. 2014;28(7):611–620. doi: 10.1177/1545968314521003. https://journals.sagepub.com/doi/10.1177/1545968314521003 .1545968314521003 [DOI] [PubMed] [Google Scholar]
- 55.Bhattacharjya S, Stafford MC, Cavuoto LA, Yang Z, Song C, Subryan H, Xu W, Langan J. Harnessing smartphone technology and three dimensional printing to create a mobile rehabilitation system, mRehab: assessment of usability and consistency in measurement. J Neuroeng Rehabil. 2019;16(1):127. doi: 10.1186/s12984-019-0592-y. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-019-0592-y .10.1186/s12984-019-0592-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bhattacharjya S, Cavuoto LA, Reilly B, Xu W, Subryan H, Langan J. Usability, usefulness, and acceptance of a novel, portable rehabilitation system (mRehab) using smartphone and 3D printing technology: mixed methods study. JMIR Hum Factors. 2021;8(1):e21312. doi: 10.2196/21312. https://humanfactors.jmir.org/2021/1/e21312/ v8i1e21312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Burke JW, McNeill MDJ, Charles DK, Morrow PJ, Crosbie JH, McDonough SM. Optimising engagement for stroke rehabilitation using serious games. Vis Comput. 2009;25(12):1085–1099. doi: 10.1007/s00371-009-0387-4. [DOI] [Google Scholar]
- 58.Burridge JH, Lee ACW, Turk R, Stokes M, Whitall J, Vaidyanathan R, Clatworthy P, Hughes AM, Meagher C, Franco E, Yardley L. Telehealth, wearable sensors, and the internet: will they improve stroke outcomes through increased intensity of therapy, motivation, and adherence to rehabilitation programs? J Neurol Phys Ther. 2017;41(Suppl 3):S32–S38. doi: 10.1097/NPT.0000000000000183.01253086-201707001-00006 [DOI] [PubMed] [Google Scholar]
- 59.Cai S, Wei X, Su E, Wu W, Zheng H, Xie L. Online compensation detecting for real-time reduction of compensatory motions during reaching: a pilot study with stroke survivors. J Neuroeng Rehabil. 2020;17(1):58. doi: 10.1186/s12984-020-00687-1. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-020-00687-1 .10.1186/s12984-020-00687-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Chumbler NR, Quigley P, Li X, Morey M, Rose D, Sanford J, Griffiths P, Hoenig H. Effects of telerehabilitation on physical function and disability for stroke patients: a randomized, controlled trial. Stroke. 2012;43(8):2168–2174. doi: 10.1161/STROKEAHA.111.646943. https://www.ahajournals.org/doi/10.1161/STROKEAHA.111.646943 .STROKEAHA.111.646943 [DOI] [PubMed] [Google Scholar]
- 61.Chung BPH, Chiang WKH, Lau H, Lau TFO, Lai CWK, Sit CSY, Chan KY, Yeung CY, Lo TM, Hui E, Lee JSW. Pilot study on comparisons between the effectiveness of mobile video-guided and paper-based home exercise programs on improving exercise adherence, self-efficacy for exercise and functional outcomes of patients with stroke with 3-month follow-up: a single-blind randomized controlled trial. Hong Kong Physiother J. 2020;40(1):63–73. doi: 10.1142/S1013702520500079. https://europepmc.org/abstract/MED/32489241 .10.1142_S1013702520500079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Colombo R, Pisano F, Mazzone A, Delconte C, Micera S, Carrozza MC, Dario P, Minuco G. Design strategies to improve patient motivation during robot-aided rehabilitation. J Neuroeng Rehabil. 2007;4:3. doi: 10.1186/1743-0003-4-3. https://jneuroengrehab.biomedcentral.com/articles/10.1186/1743-0003-4-3 .1743-0003-4-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Colomer C, Llorens R, Noé E, Alcañiz M. Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke. J Neuroeng Rehabil. 2016;13(1):45. doi: 10.1186/s12984-016-0153-6. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-016-0153-6 .10.1186/s12984-016-0153-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Conroy SS, Harcum S, Keldsen L, Bever CT. Novel use of existing technology: a preliminary study of patient portal use for telerehabilitation. J Telemed Telecare. 2022;28(5):380–388. doi: 10.1177/1357633X20950172. [DOI] [PubMed] [Google Scholar]
- 65.Cramer SC, Dodakian L, Le V, See J, Augsburger R, McKenzie A, Zhou RJ, Chiu NL, Heckhausen J, Cassidy JM, Scacchi W, Smith MT, Barrett AM, Knutson J, Edwards D, Putrino D, Agrawal K, Ngo K, Roth EJ, Tirschwell DL, Woodbury ML, Zafonte R, Zhao W, Spilker J, Wolf SL, Broderick JP, Janis S. Efficacy of home-based telerehabilitation vs in-clinic therapy for adults after stroke: a randomized clinical trial. JAMA Neurol. 2019;76(9):1079–1087. doi: 10.1001/jamaneurol.2019.1604. https://europepmc.org/abstract/MED/31233135 .2736341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Cramer SC, Dodakian L, Le V, McKenzie A, See J, Augsburger R, Zhou RJ, Raefsky SM, Nguyen T, Vanderschelden B, Wong G, Bandak D, Nazarzai L, Dhand A, Scacchi W, Heckhausen J. A feasibility study of expanded home-based telerehabilitation after stroke. Front Neurol. 2020;11:611453. doi: 10.3389/fneur.2020.611453. https://digitalcommons.chapman.edu/pt_articles/149/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Danks KA, Roos MA, McCoy D, Reisman DS. A step activity monitoring program improves real world walking activity post stroke. Disabil Rehabil. 2014;36(26):2233–2236. doi: 10.3109/09638288.2014.903303. https://europepmc.org/abstract/MED/24670193 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Da-Silva RH, Moore SA, Rodgers H, Shaw L, Sutcliffe L, van Wijck F, Price CI. Wristband accelerometers to motivate arm exercises after Stroke (WAVES): a pilot randomized controlled trial. Clin Rehabil. 2019;33(8):1391–1403. doi: 10.1177/0269215519834720. [DOI] [PubMed] [Google Scholar]
- 69.Deng H, Durfee WK, Nuckley DJ, Rheude BS, Severson AE, Skluzacek KM, Spindler KK, Davey CS, Carey JR. Complex versus simple ankle movement training in stroke using telerehabilitation: a randomized controlled trial. Phys Ther. 2012;92(2):197–209. doi: 10.2522/ptj.20110018. https://europepmc.org/abstract/MED/22095209 .ptj.20110018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Deutsch JE, Maidan I, Dickstein R. Patient-centered integrated motor imagery delivered in the home with telerehabilitation to improve walking after stroke. Phys Ther. 2012;92(8):1065–1077. doi: 10.2522/ptj.20110277. https://europepmc.org/abstract/MED/22499891 .ptj.20110277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Dias P, Silva R, Amorim P, Lains J, Roque E, Pereira ISF, Pereira F, Santos BS, Potel M. Using virtual reality to increase motivation in poststroke rehabilitation. IEEE Comput Graph Appl. 2019;39(1):64–70. doi: 10.1109/MCG.2018.2875630. [DOI] [PubMed] [Google Scholar]
- 72.Dodakian L, McKenzie AL, Le V, See J, Pearson-Fuhrhop K, Quinlan EB, Zhou RJ, Augsberger R, Tran XA, Friedman N, Reinkensmeyer DJ, Cramer SC. A home-based telerehabilitation program for patients with stroke. Neurorehabil Neural Repair. 2017;31(10-11):923–933. doi: 10.1177/1545968317733818. https://europepmc.org/abstract/MED/29072556 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Dorsch AK, Thomas S, Xu X, Kaiser W, Dobkin BH, SIRRACT investigators SIRRACT: an international randomized clinical trial of activity feedback during inpatient stroke rehabilitation enabled by wireless sensing. Neurorehabil Neural Repair. 2015;29(5):407–415. doi: 10.1177/1545968314550369. https://europepmc.org/abstract/MED/25261154 .1545968314550369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Edwards D, Kumar S, Brinkman L, Ferreira IC, Esquenazi A, Nguyen T, Su M, Stein S, May J, Hendrix A, Finley C, Howard E, Cramer SC. Telerehabilitation initiated early in post-stroke recovery: a feasibility study. Neurorehabil Neural Repair. 2023;37(2-3):131–141. doi: 10.1177/15459683231159660. https://journals.sagepub.com/doi/abs/10.1177/15459683231159660?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Emmerson KB, Harding KE, Taylor NF. Home exercise programmes supported by video and automated reminders compared with standard paper-based home exercise programmes in patients with stroke: a randomized controlled trial. Clin Rehabil. 2017;31(8):1068–1077. doi: 10.1177/0269215516680856.0269215516680856 [DOI] [PubMed] [Google Scholar]
- 76.Ezeugwu VE, Manns PJ. The feasibility and longitudinal effects of a home-based sedentary behavior change intervention after stroke. Arch Phys Med Rehabil. 2018;99(12):2540–2547. doi: 10.1016/j.apmr.2018.06.014.S0003-9993(18)30440-4 [DOI] [PubMed] [Google Scholar]
- 77.Fluet GG, Qiu Q, Patel J, Cronce A, Merians AS, Adamovich SV. Autonomous use of the home virtual rehabilitation system: a feasibility and pilot study. Games Health J. 2019;8(6):432–438. doi: 10.1089/g4h.2019.0012. https://europepmc.org/abstract/MED/31769724 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Foreman MH, Engsberg JR. A virtual reality tool for measuring and shaping trunk compensation for persons with stroke: design and initial feasibility testing. J Rehabil Assist Technol Eng. 2019;6:2055668318823673. doi: 10.1177/2055668318823673. https://journals.sagepub.com/doi/10.1177/2055668318823673?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2055668318823673 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Fusari G, Gibbs E, Hoskin L, Lawrence-Jones A, Dickens D, Crespo RF, Leis M, Crow J, Taylor E, Jones F, Darzi A. What is the feasibility and patient acceptability of a digital system for arm and hand rehabilitation after stroke? a mixed-methods, single-arm feasibility study of the 'OnTrack' intervention for hospital and home use. BMJ Open. 2022;12(9):e062042. doi: 10.1136/bmjopen-2022-062042. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=36171046 .bmjopen-2022-062042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Gauthier LV, Nichols-Larsen DS, Uswatte G, Strahl N, Simeo M, Proffitt R, Kelly K, Crawfis R, Taub E, Morris D, Lowes LP, Mark V, Borstad A. Video game rehabilitation for outpatient stroke (VIGoROUS): a multi-site randomized controlled trial of in-home, self-managed, upper-extremity therapy. EClinicalMedicine. 2022;43:101239. doi: 10.1016/j.eclinm.2021.101239. https://linkinghub.elsevier.com/retrieve/pii/S2589-5370(21)00520-4 .S2589-5370(21)00520-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Goršič M, Cikajlo I, Goljar N, Novak D. A multisession evaluation of an adaptive competitive arm rehabilitation game. J Neuroeng Rehabil. 2017;14(1):128. doi: 10.1186/s12984-017-0336-9. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-017-0336-9 .10.1186/s12984-017-0336-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Grau-Pellicer M, Lalanza JF, Jovell-Fernández E, Capdevila L. Impact of mHealth technology on adherence to healthy PA after stroke: a randomized study. Top Stroke Rehabil. 2020;27(5):354–368. doi: 10.1080/10749357.2019.1691816. [DOI] [PubMed] [Google Scholar]
- 83.Guidetti S, Gustavsson M, Tham K, Andersson M, Fors U, Ytterberg C. F@ce: a team-based, person-centred intervention for rehabilitation after stroke supported by information and communication technology—a feasibility study. BMC Neurol. 2020;20(1):387. doi: 10.1186/s12883-020-01968-x. https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-020-01968-x .10.1186/s12883-020-01968-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Held JP, Ferrer B, Mainetti R, Steblin A, Hertler B, Moreno-Conde A, Dueñas A, Pajaro M, Parra-Calderón CL, Vargiu E, Zarco MJ, Barrera M, Echevarria C, Jódar-Sánchez F, Luft AR, Borghese NA. Autonomous rehabilitation at stroke patients home for balance and gait: safety, usability and compliance of a virtual reality system. Eur J Phys Rehabil Med. 2018;54(4):545–553. doi: 10.23736/S1973-9087.17.04802-X. https://air.unimi.it/handle/2434/553392 .S1973-9087.17.04802-X [DOI] [PubMed] [Google Scholar]
- 85.Hernandez A, Bubyr L, Archambault PS, Higgins J, Levin MF, Kairy D. Virtual reality-based rehabilitation as a feasible and engaging tool for the management of chronic poststroke upper-extremity function recovery: randomized controlled trial. JMIR Serious Games. 2022;10(3):e37506. doi: 10.2196/37506. https://games.jmir.org/2022/3/e37506/ v10i3e37506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Hung NT, Paul V, Prakash P, Kovach T, Tacy G, Tomic G, Park S, Jacobson T, Jampol A, Patel P, Chappel A, King E, Slutzky MW. Wearable myoelectric interface enables high-dose, home-based training in severely impaired chronic stroke survivors. Ann Clin Transl Neurol. 2021;8(9):1895–1905. doi: 10.1002/acn3.51442. https://europepmc.org/abstract/MED/34415114 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Johnson MJ, Shakya Y, Strachota E, Ahamed SI. Low-cost monitoring of patients during unsupervised robot/computer assisted motivating stroke rehabilitation. Biomed Tech (Berl) 2011;56(1):5–9. doi: 10.1515/BMT.2010.050. [DOI] [PubMed] [Google Scholar]
- 88.Johnson MJ, Van der Loos HFM, Burgar CG, Shor P, Leifer LJ. Experimental results using force-feedback cueing in robot-assisted stroke therapy. IEEE Trans Neural Syst Rehabil Eng. 2005;13(3):335–348. doi: 10.1109/TNSRE.2005.850428. [DOI] [PubMed] [Google Scholar]
- 89.Jonsdottir J, Baglio F, Gindri P, Isernia S, Castiglioni C, Gramigna C, Palumbo G, Pagliari C, Di Tella S, Perini G, Bowman T, Salza M, Molteni F. Virtual reality for motor and cognitive rehabilitation from clinic to home: a pilot feasibility and efficacy study for persons with chronic stroke. Front Neurol. 2021;12:601131. doi: 10.3389/fneur.2021.601131. https://europepmc.org/abstract/MED/33897579 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Kamwesiga JT, Eriksson GM, Tham K, Fors U, Ndiwalana A, von Koch L, Guidetti S. A feasibility study of a mobile phone supported family-centred ADL intervention, F@ce, after stroke in Uganda. Global Health. 2018;14(1):82. doi: 10.1186/s12992-018-0400-7. https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-018-0400-7 .10.1186/s12992-018-0400-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Kanai M, Izawa KP, Kobayashi M, Onishi A, Kubo H, Nozoe M, Mase K, Shimada S. Effect of accelerometer-based feedback on physical activity in hospitalized patients with ischemic stroke: a randomized controlled trial. Clin Rehabil. 2018;32(8):1047–1056. doi: 10.1177/0269215518755841. [DOI] [PubMed] [Google Scholar]
- 92.Keeling AB, Piitz M, Semrau JA, Hill MD, Scott SH, Dukelow SP. Robot Enhanced Stroke Therapy Optimizes Rehabilitation (RESTORE): a pilot study. J Neuroeng Rehabil. 2021;18(1):10. doi: 10.1186/s12984-021-00804-8. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-021-00804-8 .10.1186/s12984-021-00804-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Kessler D, Anderson ND, Dawson DR. Occupational performance coaching for stroke survivors delivered via telerehabilitation using a single-case experimental design. Br J Occup Ther. 2021;84(8):488–496. doi: 10.1177/0308022620988471. https://journals.sagepub.com/doi/abs/10.1177/0308022620988471?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_0308022620988471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Kim DY, Kwon H, Nam KW, Lee Y, Kwon HM, Chung YS. Remote management of poststroke patients with a smartphone-based management system integrated in clinical care: prospective, nonrandomized, interventional study. J Med Internet Res. 2020;22(2):e15377. doi: 10.2196/15377. https://www.jmir.org/2020/2/e15377/ v22i2e15377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Kim J, Lee M, Kim Y, Eun SD, Yoon B. Feasibility of an individually tailored virtual reality program for improving upper motor functions and activities of daily living in chronic stroke survivors: a case series. Eur J Integr Med. 2016;8(5):731–737. doi: 10.1016/j.eujim.2016.05.001. [DOI] [Google Scholar]
- 96.King M, Hijmans JM, Sampson M, Satherley J, Hale L. Home-based stroke rehabilitation using computer gaming. N Z J Physiother. 2012;40(3):128–134. https://nzjp.otago.ac.nz/nzjp/article/view/39 . [Google Scholar]
- 97.Kringle EA, Setiawan IMA, Golias K, Parmanto B, Skidmore ER. Feasibility of an iterative rehabilitation intervention for stroke delivered remotely using mobile health technology. Disabil Rehabil Assist Technol. 2020;15(8):908–916. doi: 10.1080/17483107.2019.1629113. https://europepmc.org/abstract/MED/31216917 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Kumar D, Sinha N, Dutta A, Lahiri U. Virtual reality-based balance training system augmented with operant conditioning paradigm. Biomed Eng Online. 2019;18(1):90. doi: 10.1186/s12938-019-0709-3. https://biomedical-engineering-online.biomedcentral.com/articles/10.1186/s12938-019-0709-3 .10.1186/s12938-019-0709-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Langan J, Bhattacharjya S, Subryan H, Xu W, Chen B, Li Z, Cavuoto L. In-home rehabilitation using a smartphone app coupled with 3D printed functional objects: single-subject design study. JMIR Mhealth Uhealth. 2020;8(7):e19582. doi: 10.2196/19582. https://mhealth.jmir.org/2020/7/e19582/ v8i7e19582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Lawrie S, Dong Y, Steins D, Xia Z, Esser P, Sun S, Li F, Amor JD, James C, Izadi H, Cao Y, Wade D, Mayo N, Dawes H. Evaluation of a smartwatch-based intervention providing feedback of daily activity within a research-naive stroke ward: a pilot randomised controlled trial. Pilot Feasibility Stud. 2018;4:157. doi: 10.1186/s40814-018-0345-x. https://pilotfeasibilitystudies.biomedcentral.com/articles/10.1186/s40814-018-0345-x .345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Lawson S, Tang Z, Feng J. Supporting stroke motor recovery through a mobile application: a pilot study. Am J Occup Ther. 2017;71(3):7103350010p1–7103350010p5. doi: 10.5014/ajot.2017.025023. [DOI] [PubMed] [Google Scholar]
- 102.Lee M, Pyun SB, Chung J, Kim J, Eun SD, Yoon BC. A further step to develop patient-friendly implementation strategies for virtual reality-based rehabilitation in patients with acute stroke. Phys Ther. 2016;96(10):1554–1564. doi: 10.2522/ptj.20150271. https://academic.oup.com/ptj/article/96/10/1554/2870245?login=false .ptj.20150271 [DOI] [PubMed] [Google Scholar]
- 103.Lee M, Son J, Kim J, Pyun SB, Eun SD, Yoon BC. Comparison of individualized virtual reality- and group-based rehabilitation in older adults with chronic stroke in community settings: a pilot randomized controlled trial. Eur J Integr Med. 2016;8(5):738–746. doi: 10.1016/j.eujim.2016.08.166. [DOI] [Google Scholar]
- 104.Lee MM, Shin DC, Song CH. Canoe game-based virtual reality training to improve trunk postural stability, balance, and upper limb motor function in subacute stroke patients: a randomized controlled pilot study. J Phys Ther Sci. 2016;28(7):2019–2024. doi: 10.1589/jpts.28.2019. https://europepmc.org/abstract/MED/27512255 .jpts-2016-095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Levy T, Crotty M, Laver K, Lannin N, Killington M. Does the addition of concurrent visual feedback increase adherence to a home exercise program in people with stroke: a single-case series? BMC Res Notes. 2020;13(1):361. doi: 10.1186/s13104-020-05202-2. https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-020-05202-2 .10.1186/s13104-020-05202-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Lewis GN, Woods C, Rosie JA, McPherson KM. Virtual reality games for rehabilitation of people with stroke: perspectives from the users. Disabil Rehabil Assist Technol. 2011;6(5):453–463. doi: 10.3109/17483107.2011.574310. [DOI] [PubMed] [Google Scholar]
- 107.Li X, Wang L, Miao S, Yue Z, Tang Z, Su L, Zheng Y, Wu X, Wang S, Wang J, Dou Z. Sensorimotor rhythm-brain computer interface with audio-cue, motor observation and multisensory feedback for upper-limb stroke rehabilitation: a controlled study. Front Neurosci. 2022;16:808830. doi: 10.3389/fnins.2022.808830. https://europepmc.org/abstract/MED/35360158 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Lum PS, Taub E, Schwandt D, Postman M, Hardin P, Uswatte G. Automated Constraint-Induced Therapy Extension (AutoCITE) for movement deficits after stroke. J Rehabil Res Dev. 2004;41(3A):249–258. doi: 10.1682/jrrd.2003.06.0092. https://www.rehab.research.va.gov/jour/04/41/3A/pdf/Lum.pdf . [DOI] [PubMed] [Google Scholar]
- 109.Mansfield A, Wong JS, Bryce J, Brunton K, Inness EL, Knorr S, Jones S, Taati B, McIlroy WE. Use of accelerometer-based feedback of walking activity for appraising progress with walking-related goals in inpatient stroke rehabilitation: a randomized controlled trial. Neurorehabil Neural Repair. 2015;29(9):847–857. doi: 10.1177/1545968314567968. https://journals.sagepub.com/doi/10.1177/1545968314567968 .1545968314567968 [DOI] [PubMed] [Google Scholar]
- 110.Matarić MJ, Eriksson J, Feil-Seifer DJ, Winstein CJ. Socially assistive robotics for post-stroke rehabilitation. J Neuroeng Rehabil. 2007;4:5. doi: 10.1186/1743-0003-4-5. https://jneuroengrehab.biomedcentral.com/articles/10.1186/1743-0003-4-5 .1743-0003-4-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Mawson S, Nasr N, Parker J, Davies R, Zheng H, Mountain G. A personalized self-management rehabilitation system with an intelligent shoe for stroke survivors: a realist evaluation. JMIR Rehabil Assist Technol. 2016;3(1):e1. doi: 10.2196/rehab.5079. https://rehab.jmir.org/2016/1/e1/ v3i1e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.McNulty PA, Thompson-Butel AG, Faux SG, Lin G, Katrak PH, Harris LR, Shiner CT. The efficacy of Wii-based Movement Therapy for upper limb rehabilitation in the chronic poststroke period: a randomized controlled trial. Int J Stroke. 2015;10(8):1253–1260. doi: 10.1111/ijs.12594. [DOI] [PubMed] [Google Scholar]
- 113.Mihelj M, Novak D, Milavec M, Ziherl J, Olenšek A, Munih M. Virtual rehabilitation environment using principles of intrinsic motivation and game design. Presence: Teleop Virt Environ. 2012;21(1):1–15. doi: 10.1162/pres_a_00078. [DOI] [Google Scholar]
- 114.Mitchell C, Bowen A, Tyson S, Conroy P. A feasibility randomized controlled trial of ReaDySpeech for people with dysarthria after stroke. Clin Rehabil. 2018;32(8):1037–1046. doi: 10.1177/0269215517748453. https://journals.sagepub.com/doi/10.1177/0269215517748453 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Moan ME, Vonstad EK, Su X, Vereijken B, Solbjør M, Skjæret-Maroni N. Experiences of stroke survivors and clinicians with a fully immersive virtual reality treadmill exergame for stroke rehabilitation: a qualitative pilot study. Front Aging Neurosci. 2021;13:735251. doi: 10.3389/fnagi.2021.735251. https://europepmc.org/abstract/MED/34795576 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Mountain G, Wilson S, Eccleston C, Mawson S, Hammerton J, Ware T, Zheng H, Davies R, Black N, Harris N, Stone T, Hu H. Developing and testing a telerehabilitation system for people following stroke: issues of usability. J Eng Des. 2010;21(2-3):223–236. doi: 10.1080/09544820903333792. [DOI] [Google Scholar]
- 117.Nijenhuis SM, Prange GB, Amirabdollahian F, Sale P, Infarinato F, Nasr N, Mountain G, Hermens HJ, Stienen AHA, Buurke JH, Rietman JS. Feasibility study into self-administered training at home using an arm and hand device with motivational gaming environment in chronic stroke. J Neuroeng Rehabil. 2015;12:89. doi: 10.1186/s12984-015-0080-y. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-015-0080-y .10.1186/s12984-015-0080-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Novak D, Nagle A, Keller U, Riener R. Increasing motivation in robot-aided arm rehabilitation with competitive and cooperative gameplay. J Neuroeng Rehabil. 2014;11:64. doi: 10.1186/1743-0003-11-64. https://jneuroengrehab.biomedcentral.com/articles/10.1186/1743-0003-11-64 .1743-0003-11-64 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Olafsdottir SA, Jonsdottir H, Bjartmarz I, Magnusson C, Caltenco H, Kytö M, Maye L, McGookin D, Arnadottir SA, Hjaltadottir I, Hafsteinsdottir TB. Feasibility of ActivABLES to promote home-based exercise and physical activity of community-dwelling stroke survivors with support from caregivers: a mixed methods study. BMC Health Serv Res. 2020;20(1):562. doi: 10.1186/s12913-020-05432-x. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-05432-x .10.1186/s12913-020-05432-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Olafsdottir SA, Jonsdottir H, Magnusson C, Caltenco H, Kytö M, Maye L, McGookin D, Bjartmarz I, Arnadottir SA, Hjaltadottir I, Hafsteinsdottir TB. Developing ActivABLES for community-dwelling stroke survivors using the Medical Research Council framework for complex interventions. BMC Health Serv Res. 2020;20(1):463. doi: 10.1186/s12913-020-05198-2. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-05198-2 .10.1186/s12913-020-05198-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Parker J, Mawson S, Mountain G, Nasr N, Zheng H. Stroke patients' utilisation of extrinsic feedback from computer-based technology in the home: a multiple case study realistic evaluation. BMC Med Inform Decis Mak. 2014;14:46. doi: 10.1186/1472-6947-14-46. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/1472-6947-14-46 .1472-6947-14-46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Paul L, Wyke S, Brewster S, Sattar N, Gill JMR, Alexander G, Rafferty D, McFadyen AK, Ramsay A, Dybus A. Increasing physical activity in stroke survivors using STARFISH, an interactive mobile phone application: a pilot study. Top Stroke Rehabil. 2016;23(3):170–177. doi: 10.1080/10749357.2015.1122266. [DOI] [PubMed] [Google Scholar]
- 123.Pereira F, Badia SBI, Jorge C, Cameirão MS. The use of game modes to promote engagement and social involvement in multi-user serious games: a within-person randomized trial with stroke survivors. J Neuroeng Rehabil. 2021;18(1):62. doi: 10.1186/s12984-021-00853-z. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-021-00853-z .10.1186/s12984-021-00853-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Perez-Marcos D, Chevalley O, Schmidlin T, Garipelli G, Serino A, Vuadens P, Tadi T, Blanke O, Millán JDR. Increasing upper limb training intensity in chronic stroke using embodied virtual reality: a pilot study. J Neuroeng Rehabil. 2017;14(1):119. doi: 10.1186/s12984-017-0328-9. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-017-0328-9 .10.1186/s12984-017-0328-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Popović MD, Kostić MD, Rodić SZ, Konstantinović LM. Feedback-mediated upper extremities exercise: increasing patient motivation in poststroke rehabilitation. Biomed Res Int. 2014;2014:520374. doi: 10.1155/2014/520374. doi: 10.1155/2014/520374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Proffitt R, Lange B. Feasibility of a customized, in-home, game-based stroke exercise program using the Microsoft Kinect® sensor. Int J Telerehabil. 2015;7(2):23–34. doi: 10.5195/ijt.2015.6177. https://europepmc.org/abstract/MED/27563384 .ijt-pg23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Rosati G, Oscari F, Reinkensmeyer DJ, Secoli R, Avanzini F, Spagnol S, Masiero S. Improving robotics for neurorehabilitation: enhancing engagement, performance, and learning with auditory feedback. IEEE Int Conf Rehabil Robot. 2011;2011:5975373. doi: 10.1109/ICORR.2011.5975373. [DOI] [PubMed] [Google Scholar]
- 128.Rowe JB, Chan V, Ingemanson ML, Cramer SC, Wolbrecht ET, Reinkensmeyer DJ. Robotic assistance for training finger movement using a Hebbian model: a randomized controlled trial. Neurorehabil Neural Repair. 2017;31(8):769–780. doi: 10.1177/1545968317721975. https://europepmc.org/abstract/MED/28803535 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Sakakibara BM, Lear SA, Barr SI, Goldsmith CH, Schneeberg A, Silverberg ND, Yao J, Eng JJ. Telehealth coaching to improve self-management for secondary prevention after stroke: a randomized controlled trial of Stroke Coach. Int J Stroke. 2022;17(4):455–464. doi: 10.1177/17474930211017699. https://journals.sagepub.com/doi/abs/10.1177/17474930211017699?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PubMed] [Google Scholar]
- 130.Saywell NL, Vandal AC, Mudge S, Hale L, Brown P, Feigin V, Hanger C, Taylor D. Telerehabilitation after stroke using readily available technology: a randomized controlled trial. Neurorehabil Neural Repair. 2021;35(1):88–97. doi: 10.1177/1545968320971765. https://journals.sagepub.com/doi/abs/10.1177/1545968320971765?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Scrivener K, Sewastenko J, Bouvier-Farrell A, MacDonald K, Van Rijn T, Tezak J, Mandis N, Love S. Feasibility of a self-managed, video-guided exercise program for community-dwelling people with stroke. Stroke Res Treat. 2021;2021:5598100. doi: 10.1155/2021/5598100. doi: 10.1155/2021/5598100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Shah N, Amirabdollahian F, Basteris A. Designing motivational games for stroke rehabilitation. 7th International Conference on Human System Interactions (HSI); June 16-18, 2014; Costa da Caparica, Portugal. New Jersey: IEEE; 2014. pp. 166–171. [DOI] [Google Scholar]
- 133.Signal NEJ, McLaren R, Rashid U, Vandal A, King M, Almesfer F, Henderson J, Taylor D. Haptic nudges increase affected upper limb movement during inpatient stroke rehabilitation: multiple-period randomized crossover study. JMIR Mhealth Uhealth. 2020;8(7):e17036. doi: 10.2196/17036. https://mhealth.jmir.org/2020/7/e17036/ v8i7e17036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Simpson DB, Bird ML, English C, Gall SL, Breslin M, Smith S, Schmidt M, Callisaya ML. "Connecting patients and therapists remotely using technology is feasible and facilitates exercise adherence after stroke". Top Stroke Rehabil. 2020;27(2):93–102. doi: 10.1080/10749357.2019.1690779. [DOI] [PubMed] [Google Scholar]
- 135.Song X, van de Ven SS, Chen S, Kang P, Gao Q, Jia J, Shull PB. Proposal of a wearable multimodal sensing-based serious games approach for hand movement training after stroke. Front Physiol. 2022;13:811950. doi: 10.3389/fphys.2022.811950. https://europepmc.org/abstract/MED/35721546 .811950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Standen PJ, Threapleton K, Richardson A, Connell L, Brown DJ, Battersby S, Platts F, Burton A. A low cost virtual reality system for home based rehabilitation of the arm following stroke: a randomised controlled feasibility trial. Clin Rehabil. 2017;31(3):340–350. doi: 10.1177/0269215516640320. https://journals.sagepub.com/doi/abs/10.1177/0269215516640320?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .0269215516640320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Subramanian SK, Lourenço CB, Chilingaryan G, Sveistrup H, Levin MF. Arm motor recovery using a virtual reality intervention in chronic stroke: randomized control trial. Neurorehabil Neural Repair. 2013;27(1):13–23. doi: 10.1177/1545968312449695. https://journals.sagepub.com/doi/10.1177/1545968312449695 .1545968312449695 [DOI] [PubMed] [Google Scholar]
- 138.Sullivan JE, Espe LE, Kelly AM, Veilbig LE, Kwasny MJ. Feasibility and outcomes of a community-based, pedometer-monitored walking program in chronic stroke: a pilot study. Top Stroke Rehabil. 2014;21(2):101–110. doi: 10.1310/tsr2102-101.034G943Q06T42QMR [DOI] [PubMed] [Google Scholar]
- 139.Toh SFM, Gonzalez PC, Fong KNK. Usability of a wearable device for home-based upper limb telerehabilitation in persons with stroke: a mixed-methods study. Digit Health. 2023;9:20552076231153737. doi: 10.1177/20552076231153737. https://journals.sagepub.com/doi/10.1177/20552076231153737?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_20552076231153737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Tsekleves E, Paraskevopoulos IT, Warland A, Kilbride C. Development and preliminary evaluation of a novel low cost VR-based upper limb stroke rehabilitation platform using Wii technology. Disabil Rehabil Assist Technol. 2016;11(5):413–422. doi: 10.3109/17483107.2014.981874. [DOI] [PubMed] [Google Scholar]
- 141.Uswatte G, Taub E, Lum P, Brennan D, Barman J, Bowman MH, Taylor A, McKay S, Sloman SB, Morris DM, Mark VW. Tele-rehabilitation of upper-extremity hemiparesis after stroke: proof-of-concept randomized controlled trial of in-home Constraint-Induced Movement therapy. Restor Neurol Neurosci. 2021;39(4):303–318. doi: 10.3233/RNN-201100.RNN201100 [DOI] [PubMed] [Google Scholar]
- 142.Valdés BA, Van der Loos HFM. Biofeedback vs. game scores for reducing trunk compensation after stroke: a randomized crossover trial. Top Stroke Rehabil. 2018;25(2):96–113. doi: 10.1080/10749357.2017.1394633. [DOI] [PubMed] [Google Scholar]
- 143.Wairagkar M, McCrindle R, Robson H, Meteyard L, Sperrin M, Smith A, Pugh M. MaLT—combined motor and language therapy tool for brain injury patients using kinect. Methods Inf Med. 2017;56(2):127–137. doi: 10.3414/ME16-02-0015. https://core.ac.uk/reader/78918511?utm_source=linkout .16-02-0015 [DOI] [PubMed] [Google Scholar]
- 144.Wei WXJ, Fong KNK, Chung RCK, Cheung HKY, Chow ESL. "Remind-to-Move" for promoting upper extremity recovery using wearable devices in subacute stroke: a multi-center randomized controlled study. IEEE Trans Neural Syst Rehabil Eng. 2019;27(1):51–59. doi: 10.1109/TNSRE.2018.2882235. [DOI] [PubMed] [Google Scholar]
- 145.Whitford M, Schearer E, Rowlett M. Effects of in home high dose accelerometer-based feedback on perceived and actual use in participants chronic post-stroke. Physiother Theory Pract. 2020;36(7):799–809. doi: 10.1080/09593985.2018.1493759. [DOI] [PubMed] [Google Scholar]
- 146.Widmer M, Held JPO, Wittmann F, Valladares B, Lambercy O, Sturzenegger C, Palla A, Lutz K, Luft AR. Reward during arm training improves impairment and activity after stroke: a randomized controlled trial. Neurorehabil Neural Repair. 2022;36(2):140–150. doi: 10.1177/15459683211062898. https://journals.sagepub.com/doi/abs/10.1177/15459683211062898?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Wittmann F, Held JP, Lambercy O, Starkey ML, Curt A, Höver R, Gassert R, Luft AR, Gonzenbach RR. Self-directed arm therapy at home after stroke with a sensor-based virtual reality training system. J Neuroeng Rehabil. 2016;13(1):75. doi: 10.1186/s12984-016-0182-1. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-016-0182-1 .10.1186/s12984-016-0182-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Yuan Z, Peng Y, Wang L, Song S, Chen S, Yang L, Liu H, Wang H, Shi G, Han C, Cammon JA, Zhang Y, Qiao J, Wang G. Effect of BCI-controlled pedaling training system with multiple modalities of feedback on motor and cognitive function rehabilitation of early subacute stroke patients. IEEE Trans Neural Syst Rehabil Eng. 2021;29:2569–2577. doi: 10.1109/TNSRE.2021.3132944. https://ieeexplore.ieee.org/document/9638500 . [DOI] [PubMed] [Google Scholar]
- 149.Chong MS, Sit JWH, Karthikesu K, Chair SY. Effectiveness of technology-assisted cardiac rehabilitation: a systematic review and meta-analysis. Int J Nurs Stud. 2021;124:104087. doi: 10.1016/j.ijnurstu.2021.104087.S0020-7489(21)00234-0 [DOI] [PubMed] [Google Scholar]
- 150.Hart T, Dijkers MP, Whyte J, Turkstra LS, Zanca JM, Packel A, van Stan JH, Ferraro M, Chen C. A theory-driven system for the specification of rehabilitation treatments. Arch Phys Med Rehabil. 2019;100(1):172–180. doi: 10.1016/j.apmr.2018.09.109.S0003-9993(18)31310-8 [DOI] [PubMed] [Google Scholar]
- 151.Deterding S, Dixon D, Khaled R, Nacke L. From game design elements to gamefulness: defining "gamification". Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments; September 28-30, 2011; Tampere, Finland. New York, NY, US: Association for Computing Machinery; 2011. pp. 9–15. [DOI] [Google Scholar]
- 152.Barrett N, Swain I, Gatzidis C, Mecheraoui C. The use and effect of video game design theory in the creation of game-based systems for upper limb stroke rehabilitation. J Rehabil Assist Technol Eng. 2016;3:2055668316643644. doi: 10.1177/2055668316643644. https://journals.sagepub.com/doi/10.1177/2055668316643644?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2055668316643644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Welcome to UCLanData. University of Central Lancashire. [2024-03-29]. https://uclandata.uclan.ac.uk/383/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Preferred Reporting of Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist.
Inclusion and exclusion criteria.
Full search strategy as used in Medline.
Data charting tool.
Review-specific behavior change technique taxonomy coding decisions.
Intervention characteristics (with associated references).
Behavior change theories, models, and frameworks reported (with associated references).
Individual behavior change techniques coded.
Behavior change technique taxonomy clusters identified (with associated references).
Data Availability Statement
All data supporting this study are openly available from the University of Central Lancashire repository [153].