

Abstract
Background:
Frailty is an important geriatric syndrome predicting adverse health outcomes in older adults. However, the longitudinal characteristics of frailty components in post-hip fracture patients are less understood. Adopting the Fried frailty definition, we examined the longitudinal trends and sex trajectory differences in frailty and its components over 1 year post-fracture.
Methods:
Three hundred and twenty-seven hip fracture patients (162 men and 165 women with mean age 80.1 and 81.5) from Baltimore Hip Studies 7th cohort with measurements at 22 days after admission, and months 2, 6, and 12 post-fracture were analyzed. Frailty components included: grip strength, gait speed, weight, total energy expenditure, and exhaustion. Longitudinal analysis used mixed effect models.
Results:
At baseline, men were sicker with worse cognitive status, and had higher weight and grip strength, but lower total energy expenditure than women (p < 0.001). The prevalence of frailty was 31.5%, 30.2%, and 28.2% at months 2, 6, and 12 respectively, showing no longitudinal trends or sex differences. However, its components showed substantial recovery trends over the post-fracture year after confounding adjustments, including increasing gait speed, reducing risk of exhaustion, and stabilized weight loss and energy expenditure over time. Particularly, while men's grip strength tended to remain stable over first year post surgery within patients, women's grip strength reduced significantly over time within patients. On average over time within patients, women were more active with higher energy expenditures but lower grip strength and weight than men.
Conclusion:
Significant recovery trends and sex differences were observed in frailty components during first year post-fracture. Overall frailty status did not show those trends over months 2–12 since a summary measure might obscure changes in components. Therefore, frailty components provided important multi-dimensional information on the complex recovery process of patients, indicating targets for intervention beyond the global binary measure of frailty.
Keywords: frailty, gait speed, grip strength, post hip fracture, total energy expenditure
INTRODUCTION
Frailty has been increasingly recognized as an important geriatric syndrome that predicts adverse health outcomes and poor health-related quality of life in older adults.1,2 The rapid growth of the aging population globally has raised public health concerns and the awareness of the potential impact of frailty. There are many frailty syndrome definitions available and a recent review identified 15 frailty scales used in orthopedic surgery alone.1,3 The physical frailty phenotype definition by Fried and colleagues has been widely used1,2,4 and is described as a syndrome of decreased resiliency and reserves, which is characterized by exhaustion, weight loss, weak grip strength, slow walking speed, and low energy expenditure. If three or more criteria are present, then the individual is defined as frail. Given there is no gold standard measurement of underlying true frailty and multiple components are often dichotomized based on study-specific cut points, it is important to evaluate this operational physical frailty definition as well as its components in various populations.
There has been much work on adverse medical consequences in hip fracture patients who are frail at the time of fracture versus those without frailty. A recent meta-analysis showed consistent findings in multiple studies linking frailty with in-hospital mortality, 30-day mortality, and surgical complications.5 Other work has shown increased length of hospital stay, higher hospital costs, and poorer functional recovery in patients who were frail at the time of their hip fracture.6,7 However, little work has been done to evaluate longitudinal trends in frailty and its five components in the recovery of patients after hip fracture and potential sex differences in this recovery over time. Although it has been shown that prior to hip fracture men, who represent approximately a quarter of hip fracture patients today, have poorer health and functioning than women,8,9 and that women are frailer than men (have higher Frailty Index scores10), there has been little work that explores sex differences in trajectory of frailty and its components post hip fracture. This is important information to know when treating hip fracture patients, planning for discharge, and developing rehabilitation interventions. This article addresses how the singular entity of physical frailty and its component parts capture longitudinal changes over the complex recovery process post fracture.
In addition to investigating frailty's five binary criteria, shown in many publications, this article focuses on individual assessment of the longitudinal characteristics of each of the five frailty components in their original continuous scale over the first year post-hip fracture. Even though “frailty” as a geriatric syndrome is often operationalized as a categorical “abnormality” measure (categorizing the underlying true continuous process by threshold values), discrete medical categories rarely capture the complexity of underlying functional declines. So, to capture the complex functional recovery process of hip fracture patients, it is important to evaluate the longitudinal trends of the five components in their original scales in men and women. Nonetheless, we recognize the value of the frailty concept and need for a discrete classification of this abnormality in medical practice and are not proposing a change to Fried and colleagues' frailty definition.
METHODS
Study population
The Baltimore Hip Studies (BHS) 7th cohort was a prospective observational study designed to examine sex differences in the recovery process after hip fracture.8 Hip fracture patients were recruited from eight participating BHS network hospitals in the Baltimore metropolitan area between 2006 and 2011. To ensure recruiting enough men and women patients to reach the study power, approximately equal proportion of men and women patients within calendar time were recruited from each hospital. Eligible participants were 65 years or older at the time of hospital admission for hip fracture (ICD-9 codes 820.00–820.9) and consented to enroll or had a proxy provide informed consent within 15 days of admission. Exclusion criteria included pathologic fracture, not community-dwelling at the time of fracture, non-English speaker, being bedbound for 6 months before fracture, residence >70 miles from the hospital, weight >300 pounds, no surgery, and hardware in the contralateral hip. This study protocol was approved by the University of Maryland Institutional Review Board (IRB) and the review boards of participating hospitals.
Study visits were conducted at baseline (within 22 days of admission) and at 2, 6, and 12 months after admission including questionnaires, measures of body composition, and functional performance. Hip fracture surgery was usually done within 3 days of admission and all baseline testing was done post-surgery. Out of 362 hip fracture patients in the BHS-7th cohort, 23 participants were removed: five participants failed to provide data at the baseline and 2-month follow-up visit, and another 18 were removed as a result of an IRB-requested post procedure audit, leaving 339 in the primary study analytic sample.8 For these analyses, our analytic sample contained 327 participants (165 women and 162 men) with available frailty measurements at month 2, since walking speed was first assessed during that visit.
Frailty and its components in BHS-7
Fried et al.'s operational definition of frailty from the CHS study was applied to BHS-7 study participants.1 Details of the measurement methods and cut points for the five frailty criteria used in the BHS-7 study are summarized in Table 1. Out of these five binary criteria, four of them were defined based on dichotomizing the associated continuous functional measurements, including best grip strength among six trials (three left and three right, in kg), speed of walking 3 m (m/s, gait speed), weight change (kg), and total energy expenditure based on self-report of physical activities in a typical week in the past month from the Yale questionnaire (kcal/week).8,11,12 Since the Yale questionnaire is different from the Minnesota Leisure Time Activities Questionnaire used in Fried et al.'s CHS study, our low energy expenditure criterion used a study-specific cut point.8,11,12 The measurement methods and cut points for weight loss, slowness (sex-specific criteria), weakness (sex-specific criteria), and exhaustion in the BHS study were the same as Fried et al.'s definition in the CHS study.1 Since the focus of this article is the longitudinal characteristics and sex trajectory differences of frailty components in original continuous scales, not binary measures, the key findings of this article are not sensitive to those cut points.
TABLE 1.
Definition of frailty and its binary criteria used in the BHS-7 study.
| Binary criteria | Method and cut points | Binary criteria | Method and cut points |
|---|---|---|---|
| Weight loss | Weight lost >10 pounds in the prior year (if missing, calibrate it by the generated weight loss speed per month from original weight variable) | Low energy expenditure | Total caloric expenditure based on self-report of physical activities in a typical week in past month from Yale questionnaire (kcal/week). Month 0 refers pre-fracture. kcals expenditure/week <465 |
| Slowness in gait speed | Speed of walking 3 m Speed ≤0.65 m/s for female height ≤ 159 cm, or male height ≤ 173 cm Speed ≤0.76 m/s for female height > 159 cm, or male height > 173 cm |
Weakness in grip strength | Best grip strength among six trials (three left and three right, in kg) Female: ≤17 kg for BMI ≤ 23 ≤17.3 for 23 < BMI ≤ 26 ≤18 for 26 < BMI ≤ 29 ≤21 for BMI > 29 Male: ≤29 kg for BMI ≤ 24 ≤30 for 24 < BMI ≤ 26 ≤30 for 26 < BMI ≤ 28 ≤32 for BMI > 28 |
| Exhaustion | Evaluation of 2 statements from the Center for Epidemiological Studies—Depression scale (CESD) Self-report of either of: (1) I feel everything I did was an effort? (2) I could not get going? |
Frailty status | ≥3 criteria presented Including weight loss, weak grip strength, slow walking speed, and low energy expenditure, and exhaustion |
This operational definition indicated that “frailty” as an important summary geriatric syndrome can be clinically diagnosed utilizing its continuous components capturing patients' resiliency declines over threshold values. To better understand the complex functional recovery process of hip fracture patients within first year post surgery, the primary outcomes of interest are binary frailty status and its five components in original scales using all available longitudinal data, including continuous weight, best grip strength among six trials, walking speed over 3 m, total energy expenditure in the week prior to measurement, as well as binary exhaustion. While most variables of interest are available at baseline and follow-up (months 0, 2, 6, and 12), walking speed and overall frailty status are only available at the three follow-up visits (month 2, 6, and 12).
Covariates and potential confounders
The confounders considered in this study were the following baseline covariates: age, education (in years), race (White vs non-White), comorbidity (Charlson Comorbidity Index), BMI (kg/m2), ADL (reported pre-fracture Lower Physical Activities of Daily Living), and 3MS (Modified Mini-Mental State Examination) score as a measure of baseline cognitive status.8,9
Statistical analysis
To assess sex differences in the baseline characteristics of our study sample, we used Student t test for continuous variables and chi-square tests for categorical variables in descriptive analyses. To visualize the longitudinal trends of frailty and its components across men and women, we compared their mean trajectories in plots.
To capture the complex continuous patient-specific post-surgery recovery process and quantify the longitudinal characteristics of frailty and its measurements in men and women, mixed effect models (REM)13,14 were used for this longitudinal study. Comparing to longitudinal analyses using marginal models (estimated by GEE), mixed effect models (REM) were chosen due to their superior properties.13,14 REM models used random effects (i.e., random intercepts in this study) to account for the heterogeneity in the study sample beyond what the observed variables could explain. The interpretations of REM results focused on patient-specific trajectory changes and sex trajectory differences within patients, which were more scientifically appealing in tracking patients' progress than the “population average differences” that marginal models typically provide. Furthermore, REM models provided better protections on their inference and results against the potential data missing at random issues. Sequential model fitting techniques were used in sharpening the mixed effect models, accounting for various levels of confounding adjustment and interaction terms. The final model was chosen based on AIC, BIC, and likelihood ration tests. In the final chosen REM models, “time” (month 0, 2, 6, and 12) was treated as a categorical variable and month indicators were used to capture longitudinal trends for overall frailty and its components. The interaction terms between time and sex were used to capture the longitudinal differences in frailty and its components' trajectories between women and men. These models provided not only more consistent interpretations on longitudinal trends across outcomes, but also same degree of flexibility in accommodating nonlinear longitudinal trends across all outcomes within first year follow up. Data were analyzed using SAS version 9.3 software (SAS Institute) and R software (RStudio 2021).
RESULTS
Table 2 shows the baseline characteristics by sex. On average over the 162 men and 165 women with a hip fracture, men were sicker with worse baseline cognitive status than women as shown by their significantly higher Charlson Comorbidity Index and lower 3MS scores. Men had higher body weight and grip strength, but reported lower total energy expenditure prior to the fracture than women. Furthermore, no significant sex differences were observed for age, education level, race, BMI, exhaustion, gait speed at month 2, and baseline ADL.
TABLE 2.
Sex differences in baselinea characteristics of hip fracture patients (N = 327).
| Men (n = 162) | Women (n = 165) | p-value | |
|---|---|---|---|
| Age, years (SD) | 80.1 (7.8) | 81.5 (7.9) | 0.100 |
| Education, years (SD) | 13.2 (3.8) | 13 (3.0) | 0.741 |
| Race, White (%) | 90.2% | 92.7% | 0.419 |
| Charlson Comorbidity Index (SD) | 2.5 (1.9) | 1.6 (1.6) | <0.001 |
| Body Mass Index, kg/m2 (SD) | 25.6 (4.5) | 25 (5.6) | 0.286 |
| Weight, kg (SD) | 79.0 (14.0) | 63.6 (14.2) | <0.001 |
| Grip strength, kg (SD) | 29.3 (9.7) | 18.6 (6.7) | <0.001 |
| Exhaustion (%) | 61.7% | 67.5% | 0.282 |
| Total energy expenditure, kcal/week (SD) | 2426.2 (2365.7) | 3625.4 (2600) | <0.001 |
| Gait speed at month 2, m/s (SD) | 0.32 (0.25) | 0.37 (0.23) | 0.134 |
| ADL score (SD) | 2.42 (2.58) | 2.75 (2.59) | 0.243 |
| 3MS score (SD) | 82.3 (16.4) | 86.0(16.6) | 0.045 |
Note: Values were mean (SD) of continuous variables or % of categorical variables.
Baseline was month 0, within 22 days of hospital admission. Gait speed was available starting from month 2.
Table 3 shows the longitudinal summary of frailty status and its five components in both binary and continuous scales during the year after hip fracture. The prevalence of frailty decreased very slightly within the first year of follow-up with 31.5% being frail at month 2, 30.2% at month 6, and 28.2% at month 12. Frailty status was not available at baseline due to unavailable gait speed. Figure 1 captures the associated longitudinal trajectory differences across men and women, where panel (A) shows the prevalence of the binary frailty components, and panel (B) shows the prevalence of overall frailty status and its components in their original continuous scales. The frailty plot in Figure 1B indicates that men on average had higher prevalence of frailty in months 2 (35.8%) and 6 (33.7%), but lower prevalence in month 12 (25.6%) than women (27.3%, 26.9%, and 30.4% at months 2, 6, and 12, respectively). However, both the longitudinal trends and the sex trajectory differences of frailty were not statistically significant. Table 3 also shows the recovery trends in the frailty components (in both scales), including substantial decreasing prevalence of weight loss, exhaustion, slowness, and low energy expenditure over month 2–12, as well as increasing trends in mean gait speed and total energy expenditure and stabilized weight over time after month 2. Comparing trajectories of frailty components in their original scale between men and women, Figure 1B shows that men were heavier, had greater grip strength, and lower total energy expenditure than women on average over time. Using the binary scale of the frailty components, Figure 1A shows men had a higher percentage of weight loss, and statistically significantly higher prevalence of weakness at month 2 as well as higher prevalence of low energy expenditure at month 6 than women. Even though frailty and its components both showed recovery trends over month 2 to month 12, the magnitudes of longitudinal trends and sex trajectory differences were considerably smaller and non-significant in overall frailty compared to its original components.
TABLE 3.
Longitudinal summary of frailty status and its five components (binary and continuous scale) over 1 year post hip fracture.
| Month 0 (n = 327) | Month 2 (n = 327) | Month 6 (n = 199) | Month 12 (n = 188) | ||
|---|---|---|---|---|---|
| Frailty | Frailty = 1, % | NAa | 31.5% | 30.2% | 28.2% |
| Weight loss | Weight loss, % | 28.4% | 40.9% | 19.8% | 17.3% |
| Weight, kg (SD) | 71.3 (15.9) | 69.5 (16.2) | 68.8 (16.0) | 69.7 (17.3) | |
| Exhaustion | Exhaustion, % | 64.7% | 40.0% | 38.0% | 37.7% |
| Weakness | Weakness, % | 53.7% | 49.6% | 55.5% | 58.1% |
| Grip strength, kg (SD) | 23.9 (9.9) | 23.9 (9.1) | 23.6 (10.0) | 22.8 (10.2) | |
| Slowness | Slowness, % | NAa | 93.4% | 89.6% | 88.8% |
| Gait speed, m/s (SD) | NAa | 0.35 (0.24) | 0.44 (0.25) | 0.46 (0.24) | |
| Low energy expenditure | Low energy expend, % | 11.2% | 25.7% | 22.0% | 17.4% |
| Total energy expenditure, kcal/week (SD) | 3044.1 (2556.5) | 1667.6 (1934.1) | 2220.5 (2053.8) | 2465.9 (2559.9) |
Note: Values were mean (SD) of continuous variables or % of categorical variables.
Gait Speed was available starting from month 2; therefore, both slowness and frailty status were missing at month 0.
FIGURE 1.
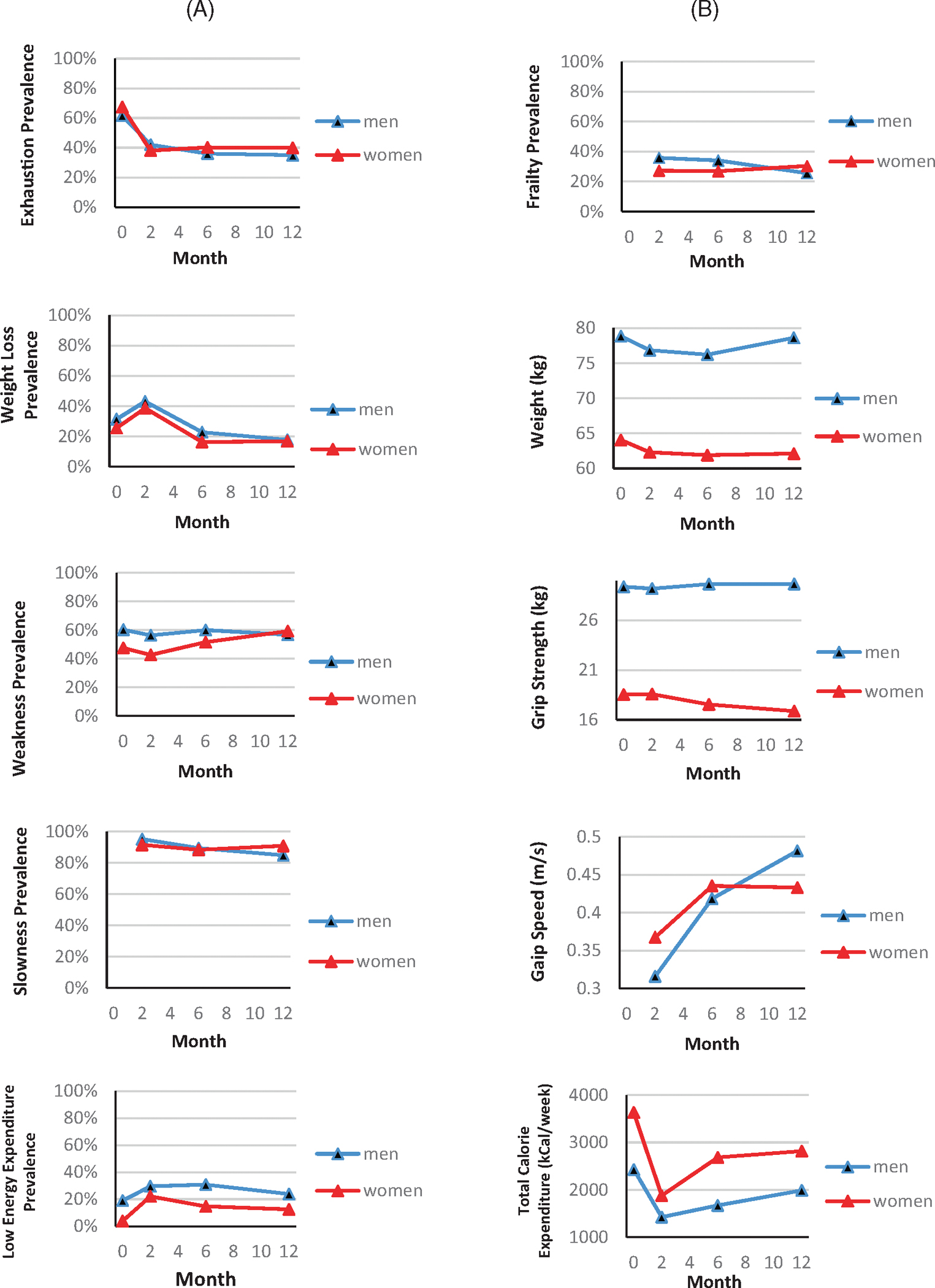
Longitudinal trajectory differences of frailty and its components across men and women over 1 year post hip fracture. Panel (A): frailty binary components, including (from top to bottom) exhaustion, weight loss, weakness, slowness, and low energy expenditure. Panel (B): overall frailty and its continuous components in their original scales, including (from top to bottom) overall frailty (binary), weight (kg), grip strength (kg), gait speed (m/s), and total caloric expenditure (kcal/week). Except the first row, the plots in each row are paired to show the longitudinal trajectories of the same frailty components in the binary scale (panel A) and continuous scale (panel B).
To quantify the longitudinal trends and associated sex trajectory differences of frailty and its five components over the 1 year, longitudinal data analyses (LDA) were conducted. Table 4 shows the results of the two final models: while results from LDA model 1 (random effect model with simple adjustment) confirmed the findings in Table 3 and Figure 1, the focus would be on the interpretations of LDA model 2 results after full confounding adjustment. Results for overall frailty showed no significant sex trajectory differences or longitudinal trends within participants over month 2–12 after confounding adjustment. Within the same fracture patient, even though the odds of being frail in month 12 was on average less than the same odds in month 2, this longitudinal trend was not statistically significant. Even though women seemed to have lower risk of being frail than men within same patient on average over time, this sex difference was not significant after adjusting for confounders.
TABLE 4.
Longitudinal data analysis (LDA) results quantifying frailty and five components’ longitudinal trends and associated sex trajectory differences over first year.
| LDA Model 1 |
LDA Model 2 |
|||
|---|---|---|---|---|
| Regression coeficient (95% CI) | p value | Regression coefficient (95% CI) | p value | |
| Frailty | ||||
| Month 6 | −0.12 (−0.75, 0.5) | 0.696 | −0.01 (−0.64, 0.63) | 0.985 |
| Month 12 | −0.67 (−1.35, 0) | 0.051 | −0.58 (−1.27, 0.11) | 0.098 |
| Women vs men | −0.56 (−1.16, 0.03) | 0.063 | −0.28 (−0.9, 0.33) | 0.362 |
| Month 6 × women | −0.01 (−0.9, 0.87) | 0.974 | −0.2 (−1.1, 0.7) | 0.661 |
| Month 12 × women | 0.75 (−0.17, 1.67) | 0.110 | 0.68 (−0.24, 1.61) | 0.149 |
| Grip strength | ||||
| Month 2 | −0.41 (−1.47, 0.65) | 0.452 | −0.36 (−1.45, 0.72) | 0.509 |
| Month 6 | −0.23 (−1.37, 0.91) | 0.697 | −0.31 (−1.46, 0.85) | 0.603 |
| Month 12 | −0.45 (−1.67, 0.77) | 0.468 | −0.69 (−1.93, 0.56) | 0.279 |
| Women vs men | −10.27 (−11.91, −8.64) | <0.0001 | −11.15 (−12.78, −9.53) | <0.0001 |
| Month 2 × women | −0.07 (−1.56, 1.42) | 0.930 | −0.16 (−1.67, 1.35) | 0.838 |
| Month 6 × women | −0.87 (−2.47, 0.74) | 0.289 | −0.87 (−2.49, 0.75) | 0.294 |
| Month 12 × women | −1.67 (−3.35, 0.01) | 0.051 | −1.50 (−3.20, 0.19) | 0.082 |
| Total energy expenditure | ||||
| Month 2 | −1010.7 (−1418.6, −602.7) | <0.0001 | −1070.7 (−1484.3, −657.2) | <0.0001 |
| Month 6 | −948.2 (−1400.2, −496.3) | <0.0001 | −993.9 (−1448.2, −539.6) | <0.0001 |
| Month 12 | −719.9 (−1193.5, −246.3) | 0.003 | −807.0 (−1284.2, −329.9) | 0.001 |
| Women vs men | 1271.0 (759.7, 1782.3) | <0.0001 | 994.4 (485.9, 1502.9) | 0.0001 |
| Month 2 × women | −769.4 (−1330.3, −208.4) | 0.007 | −701.9 (−1267.6, −136.3) | 0.015 |
| Month 6 × women | −50.8 (−668.7, 567.0) | 0.872 | −45.2 (−667.1, 567.7) | 0.887 |
| Month 12 × women | − 118.2 (−750.5, 514.1) | 0.714 | −35.7 (−672.3, 600.8) | 0.912 |
| Exhaustion | ||||
| Month 2 | −1.14 (−1.75, −0.53) | 0.0002 | −1.19 (−1.8, −0.57) | 0.0001 |
| Month 6 | −1.47 (−2.16, −0.78) | <0.0001 | −1.42 (−2.11, −0.73) | <0.0001 |
| Month 12 | −1.5 (−2.21, −0.8) | <0.0001 | −1.41 (−2.12, −0.7) | <0.0001 |
| Women vs men | 0.36 (−0.29, 1) | 0.279 | 0.44 (−0.21, 1.08) | 0.182 |
| Month 2 × women | −0.62 (−1.46, 0.23) | 0.155 | −0.51 (−1.36, 0.34) | 0.241 |
| Month 6 × women | −0.11 (−1.05, 0.83) | 0.820 | −0.12 (−1.06, 0.82) | 0.804 |
| Month 12 × women | −0.15 (−1.1, 0.81) | 0.763 | −0.12 (−1.07, 0.83) | 0.810 |
| Weight | ||||
| Month 2 | −2.85 (−3.85, −1.85) | <0.0001 | −2.67 (−3.69, −1.65) | <0.0001 |
| Month 6 | −2.83 (−3.94, −1.73) | <0.0001 | −2.60 (−3.72, −1.49) | <0.0001 |
| Month 12 | −1.34 (−2.49, −0.18) | 0.024 | −1.21 (−2.37, −0.04) | 0.042 |
| Women vs men | −14.17 (−17.20, −11.15) | <0.0001 | −13.67 (−15.9, −11.43) | <0.0001 |
| Month 2 × women | 0.20 (−1.21, 1.60) | 0.785 | 0.02 (−1.40, 1.43) | 0.982 |
| Month 6 × women | 0.38 (−1.16, 1.91) | 0.630 | 0.13 (−1.41, 1.67) | 0.868 |
| Month 12 × women | −0.63 (−2.22, 0.95) | 0.432 | −0.83 (−2.42, 0.75) | 0.303 |
| Gait speed | ||||
| Month 6 | 0.07 (0.03, 0.11) | 0.0002 | 0.06 (0.03, 0.10) | 0.0007 |
| Month 12 | 0.11 (0.07, 0.15) | <0.0001 | 0.11 (0.07, 0.15) | <0.0001 |
| Women vs men | 0.03 (−0.03, 0.09) | 0.362 | 0.00 (−0.06, 0.05) | 0.992 |
| Month 6 × women | 0.03 (−0.02, 0.08) | 0.279 | 0.04 (−0.01, 0.09) | 0.130 |
| Month 12 × women | −0.03 (−0.09, 0.02) | 0.235 | −0.03 (−0.08, 0.02) | 0.295 |
Note: LDA Model 1 (Random effect model with simple adjustment): Y ~ ui + time + women + age + time × women. LDA Model 2 (Fully adjusted random effect model): Y ~ ui + time + women + age + time × women + education + race + comorbidity + BMI + ADL + 3MS. (Sex: women = 1, and men = 0, time × women are interaction terms). p-values came from t-test of LDA regression coefficients. Bold p-values indicate significance if rounded to two decimal places (≤0.05).
We found significant sex differences and marginally significant sex trajectory differences in grip strength. Women's grip strength on average was 11.15 kg lower (95% CI: [−12.78, −9.53], p-value <0.0001) than men's over time within patients, after adjusting all confounders. Longitudinally, women's grip strength showed a decreasing trend over first year post fracture, while men's grip strength tended to remain stable over time. The grip strength reduction within the same patient across month 12 versus month 0 was on average 1.50 kg more (95% CI: [−0.19, 3.20]) in women than men with a p-value 0.056 using likelihood ratio test or 0.082 using t-test, after adjusting all confounders.
We also found significant sex differences and sex trajectory differences in total energy expenditure over 1 week. Women were more active on average than men throughout the 1-year follow-up. Women's total energy expenditure in a week was on average 994.4 kcal/week more (95% CI: [485.9, 1502.9]) than men's over time within patients after adjusting for confounders. Longitudinally, both men's and women's total energy expenditure decreased over the year compared to pre-fracture reported at baseline, and men's declining trends were all significant across all months. Within the same patient, total energy expenditures dropped the most in the first 2 months after admission, and this total energy expenditure drop within first 2 month in women was on average 701.9 kcal/week (95% CI: [−1267.6, −136.3]) more than men after adjusting confounders. No such sex trajectory differences were detected in later months.
For exhaustion and weight, significant longitudinal trends were found in men with or without confounding adjustments, and no significant trajectory differences within patients were seen across men and women. Within same patient, the odds of being exhausted at month 2, month 6, or month 12 decreased significantly comparing to month 0 (baseline) after confounding adjustment. Furthermore, results showed that hip fracture patients lost significant weight on average over the 1-year period versus baseline within men shown by significant “time” (in month) effects, and this significant decreasing trend was faster within the first 2 months, and slowed down at month 6 and month 12. This model confirmed that women's weights were 13.67 kg (95% CI: [−15.9, −11.4]) on average less than men's over time.
For walking speed, significant longitudinal increasing trends were found in men, and no significant trajectory differences within patients were seen across men and women. Men's walking speed increased significantly during month 2 to month 12 post-surgery. Within the same patient, his walking speed at month 6 and month 12 were 0.06 m/s (95% CI: [0.03, 0.10]) faster and 0.11 m/s (95% CI: [0.07, 0.15]) faster than his speed at month 2 on average, after adjusting for confounders.
SUMMARY AND DISCUSSION
This article uniquely evaluates the longitudinal characteristics of five frailty components in their original continuous scale during the first year of post-surgery recovery. Both sex differences and sex trajectory differences also were evaluated to provide insight on how men and women differ in their recovery from hip fracture, which is relevant for both discharge planning and developing rehabilitation programs to improve outcomes in this condition. Since gait speed and frailty were not available at baseline, the longitudinal trends comparisons across frailty and its components below focused on month 2 to month 12, their commonly available time period. Even though all five individual frailty components in their original scales showed various levels of significant sex differences, longitudinal trends, and sex trajectory differences in month 2–12, the magnitudes of those trends and sex differences were considerably smaller and non-significant in overall frailty. With respect to the longitudinal recovery trends, four individual components (exhaustion, total energy expenditure, gait speed, weight) showed substantial improvements over the post-fracture year, while overall frailty prevalence did not. No sex differences and/or sex trajectory differences were observed for the binary frailty status, but they were found for grip strength and weight over month 2–12.
The overall frailty status summarizing the five dichotomous components was useful in capturing the overall physical syndrome of decreased resiliency and reserves in older adults.1,2,4 However, for post fracture patients, the frailty components measured in their original scales without dichotomization might capture the complex post-surgery recovery trends better than the binary frailty status over months 2–12. This summary frailty indicator might also be obscuring the different changes that are happening in its components longitudinally when comparing men and women. The individual components of frailty provide important multi-dimensional information on the complex recovery process of post-fracture patients, which could be useful biomarkers or prognostic factors facilitating the patient subgroup identification for intervention allocation and target therapy to reduce frailty and improve patients' post fracture functioning recovery.
One interesting feature of this study is that the prevalence of frailty in BHS-7 study sample was significantly higher in men than in women, which was different from the study population of the Cardiovascular Health Study (CHS).1 This finding that men with hip fracture had more frailty than women was compatible with previous research showing that male hip fracture patients did worse than females patients.9,15,16 The CHS study played a critical role in establishing Fried and colleagues' operational definition of frailty as an important geriatric syndrome for predicting adverse health outcomes in older adults. This study adds a valuable description of longitudinal characteristics of frailty and its five components in post hip fracture patients.
The findings of this study might be limited to the patient population in the metropolitan areas of Baltimore or areas with similar patient populations and care practices as in the Baltimore region.8,9,15 Also, this study is limited to the patient population who live in the community at the time of fracture; we did not include the individuals admitted from the nursing home, or being bedbound for 6 months before fracture. At the time study participants were enrolled, to the best of our knowledge, none of the eight study hospitals had orthogeriatric care programs, or established hip fracture specific nutrition or rehabilitation programs. Our study population was predominately White, with an average education consistent with some college education, and might not be generalizable to a more diverse hip fracture population. The longitudinal data analysis methods we used provided robust inference and results accounting for two types of missing data problems: missing completely at random and missing at random. Even though these two types of missing mechanisms could explain most of the missing data in observational studies, the higher death rate in men in BHS-7 post hip fracture patients8,16 could potentially raise concern of informative missing issue, which could be investigated in future studies. Despite some limitations, this study was the first quantifying the longitudinal characteristics of frailty and its five components measured in their original scales across men and women over the 1 year post hip fracture recovery period, as well as comparing various trends across those outcomes over months 2–12. The BHS-7 empowered this study with a comprehensive data set of equally sampled men and women hip fracture patients, providing enough power for our direct comparison by sex.
In caring for patients with hip fracture, early identification of the vulnerable patients at higher risk for poor recovery and providing more intensive rehabilitation is an important goal. The challenges in using binary frailty status to identify patients at risk post fracture are the multiple ways within the five domains that people can meet the criteria for frailty. There is also a range of recovery patterns in patients that frailty status alone does not capture as demonstrated here. Even though binary frailty measure can miss important longitudinal recovery trends and changes in hip fracture patients, its individual components measured in their original scales can provide more concrete multi-dimensional information on the complex functional recovery process. Some studies have shown that individual frailty components can reveal important information about function prior to meeting the criteria for frailty.17 This article provides valuable information supporting the use of individual frailty components as biomarkers or prognostic factors for early identification of patients at higher risk of poor recovery for intervention allocation to improve patients' long-term outcomes.
Key points.
Even though five individual frailty components in their original scales showed various levels of significant longitudinal recovery trends, sex differences, and sex trajectory differences in the first year post fracture recovery, the overall binary physical frailty status did not show any of those trends over months 2–12.
Why does this paper matter?
In contrast to using physical frailty status, the individual frailty components provided more precise multi-dimensional information of the complex recovery process of post fracture patients. The individual components could be useful biomarkers or prognostic factors for early identification of the vulnerable hip fracture patients at higher risk who are more likely to benefit from therapy or intervention for improving patients' post fracture functional recovery.
SPONSOR’S ROLE
The funding organization had no role in the design and conduct of the study; in the collection, management, analysis, and interpretation of data; in the preparation, review, or approval of the manuscript; and in the decision to submit the manuscript for publication.
FINANCIAL DISCLOSURE
The study reported in this manuscript was supported by R37AG009901, R01AG029315, T32AG000262, and P30AG028747 from the National Institute on Aging.
Footnotes
CONFLICT OF INTEREST STATEMENT
During the past year, Jay Magaziner consulted or served on advisory boards for Own the Bone Multidisciplinary Advisory Board of the American Orthopedic Association and the Fragility Fracture Network. None of these entities provided funding for the current project. Yi Huang, Denise Orwig, Hilary Hayssen, Wenxin Lu, Ann Gruber-Baldini, Nancy Chiles Shaffer, and Jack Guralnik have no conflicts to report.
REFERENCES
- 1.Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–M156. doi: 10.1093/gerona/56.3.m146 [DOI] [PubMed] [Google Scholar]
- 2.Gary R. Evaluation of frailty in older adults with cardiovascular disease: incorporating physical performance measures. J Cardiovasc Nurs. 2012;27(2):120–131. doi: 10.1097/JCN.0b013e318239f4a4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Roopsawang I, Zaslavsky O, Thompson H, Aree-Ue S, Kwan RYC, Belza B. Frailty measurements in hospitalised orthopaedic populations age 65 and older: a scoping review. J Clin Nurs. 2022;31(9–10):1149–1163. doi: 10.1111/jocn.16035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bandeen-Roche K, Xue QL, Ferrucci L, et al. Phenotype of frailty: characterization in the women's health and aging studies. J Gerontol A Biol Sci Med Sci. 2006;61(3):262–266. doi: 10.1093/gerona/61.3.262 [DOI] [PubMed] [Google Scholar]
- 5.Ma Y, Wang A, Lou Y, Peng D, Jiang Z, Xia T. Effects of frailty on outcomes following surgery among patients with hip fractures: a systematic review and meta-analysis. Front Med (Lausanne). 2022;9:829762. doi: 10.3389/fmed.2022.829762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Amata O, Panella L, Incorvaia C, et al. Role of frailty in functional recovery after hip fracture, the variable impact in restoring autonomy. Acta Biomed. 2022;92(6):e2021387. doi: 10.23750/abm.v92i6.11612 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kwak MJ, Digbeu BD, des Bordes J, Rianon N. The association of frailty with clinical and economic outcomes among hospitalized older adults with hip fracture surgery. Osteoporos Int. 2022;33(7):1477–1484. doi: 10.1007/s00198-021-06215-8 [DOI] [PubMed] [Google Scholar]
- 8.Orwig D, Hochberg M, Gruber-Baldini A, et al. Examining differences in recovery outcomes between male and female hip fracture patients: design and methodology of a prospective cohort study from the Baltimore Hip Studies. J Frailty Aging. 2018;7(3):162–169. doi: 10.14283/jfa.2018.15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Orwig DL, Abraham DS, Hochberg MC, et al. Sex differences in recovery across multiple domains among older adults with hip fracture. J Gerontol A Biol Sci Med Sci. 2022;77(7):1463–1471. doi: 10.1093/gerona/glab271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gordon EH, Peel NM, Samanta M, Theou O, Howlett SE, Hubbard RE. Sex differences in frailty: a systematic review and meta-analysis. Exp Gerontol. 2017;89:30–40. [DOI] [PubMed] [Google Scholar]
- 11.Dipietro L, Caspersen CJ, Ostfeld AM, Nadel ER. A survey for assessing physical activity among older adults. Med Sci Sports Exerc. 1993;25(5):628–642. [PubMed] [Google Scholar]
- 12.Taylor HL, Jacobs DR, Schucker B, Knudsen J, Leon AS, Debacker G. A questionnaire for the assessment of leisure time physical activities. J Chronic Dis. 1978;31(12):741–755. doi: 10.1016/0021-9681(78)90058-9 [DOI] [PubMed] [Google Scholar]
- 13.Laird NM, Ware JH. Random-effects models for longitudinal data. Biometrics. 1982;38:963–974. [PubMed] [Google Scholar]
- 14.Diggle PJ, Heagarty P, Liang KY, Zeger SL. Analysis of Longitudinal Data. [Chapters 7 and 9]. 2nd ed. Oxford University Press; 2002. [Google Scholar]
- 15.Shaffer NC, Huang Y, Abraham D, et al. Comparing longitudinal sarcopenia trends by definitions across men and women post hip fracture. J Am Geriatr Soc. 2020;68(7):1537–1544. doi: 10.1111/jgs.16417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bajracharya R, Guralnik JM, Magaziner JS, et al. Long-term sex differences in all-cause and infection-specific mortality post hip fracture. J Am Geriatr Soc. 2022;70(7):2107–2114. doi: 10.1111/jgs.17800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stenholm S, Ferrucci L, Vahtera J, et al. Natural course of frailty components in people who develop frailty syndrome: evidence from two cohort studies. J Gerontol A Biol Sci Med Sci. 2019;74(5):667–674. doi: 10.1093/gerona/gly132 [DOI] [PMC free article] [PubMed] [Google Scholar]