

Abstract
Objective:
The excessive growth of the food supplements’ industry highlights the need to focus attention on all aspects involved in their proper consumption; one that takes centre stage is advertising. The aim of this research is to analyse the presence of false and misleading claims in food supplements advertising. To this end, a relationship is established between the different types of health-related claims and the substances on which they are based, whether authorised or not by European Food Safety Authority (EFSA).
Design:
This empirical work conducts a content analysis of all radio mentions broadcast throughout 2017 on news/talk radio stations.
Setting:
Spain.
Participants:
All radio mentions broadcast on news/talk commercial radio stations in Spain with the highest audience levels. The corpus is composed of 437 advertisements.
Results:
Results indicate that 80·3 % of function claims included in the analysed advertisements are not authorised by EFSA, while 20·4 % of disease claims are not allowed by EU regulation. Likewise, almost half of the substances referred to (43·7 %) are illicit: 54·1 % in function claims, 57·3 % in disease claims and 73·7 % in the case of reduction of disease risk claims.
Conclusions:
This work reveals consistent failures to comply with European regulation on food supplements advertising. The widespread use of unauthorised health claims and substances is aggravated by the indirect recourse of illness as a persuasive argument, descriptions of alleged benefits as product attributes and the omission of essential information. This leads to dangerous misinformation and can pose serious health risks. Stronger legal mechanisms are needed for effective consumer protection.
Keywords: Food supplements, Health claims, Misleading advertising, EU regulation, European Food Safety Authority
Between 2013 and 2020, sales of vitamins and food supplements increased by 22·33 % in Western Europe, reaching a volume of 11 billion euros in the selected countries. In addition, daily consumption among Europeans has increased by 88·5 % over the last 5 years, standing at 32·8 % in 2021 compared with 2016’s 17·4 %. Spain exceeds the European average, with 35 % of Spaniards consuming food supplements on a daily basis(1). This ever-expanding health-related industry thriving in developed countries uses commercial strategies that aim to create a direct association between health and food. In these coordinates, the regulation, advertising and consumption of food supplements (dietary supplements in the USA) are matters of continuous debate, occupying a central place in academic and scientific research(2–4).
Previous studies have confirmed that consumers take food supplements to correct nutritional deficiencies and improve their general health(5,6). However, there are currently other reasons involved. Academics have shown that people’s perception of illness is the most significant predictor of food supplements consumption(7). They have also shown a correlation between chronic illness and the consumption of supplements(6,8) as an alternative to conventional medicine(9), to save money or to postpone seeking medical attention(5,6). In this respect, Bailey et al. (5) analysed the data of 11 956 American adults to conclude that supplements were in most cases taken out of personal choice (77 %) rather than following the advice of a medical professional (23 %). Nevertheless, consumers are often unaware that their misuse can cause severe health issues such as organ harm from inherent toxicity, interactions or product contamination. This is linked to an increase in the attendance rates at emergency wards and number of hospital admissions(2,10,11). In fact, scientific evidence supporting the real benefits and safety of food supplements is scarce(3) and consumers remain inadequately informed(9,10) or lack the capacity to correctly interpret the information transmitted by health claims(12,13). The public is misled by claims that present these types of products as an alternative to the chemicals of medication, although natural is not always synonymous with harmless(14). Consumption of food supplements also has a negative impact on consumers’ economies, as products in many cases do not fulfil their promises. But perhaps, the most damaging aspect of food supplements has to do with the health-related expectations of users who take them to treat life-threatening illnesses instead of seeking professional medical care. All this justifies the prohibition of health claims not verified by public administrations(15) and motivates this research.
Advertising takes centre stage in the demand for food supplements, with advertisements that, directly or indirectly, encourage their consumption as a substitute for traditional medicine, while promoting self-care as opposed to professional care(16). Growth industries and profit-driven markets continue to challenge advertisers’ ethical standards. All too often, veracity and the protection of consumer rights are secondary to the efficacy of persuasion. Marketing has striven in recent years to promote greater corporate social responsibility in its clients rather than fostering its own, acting with a ‘moral short-sightedness’(17) which favours strategic thinking. However, the sector’s lack of concern for the social effects of their commercial actions entails unreasonable damage to consumers. In fact, given the abundance of misleading advertising, the rise of academic attention on advertisers’ corporate social responsibility is not surprising(18–20). As a result, most countries have implemented regulatory measures to control the marketing and promotion of food supplements and health-related claims (H-RC).
European regulation(21) establishes that food supplements are foodstuffs whose purpose is to supplement our normal diet. They are concentrated sources of nutrients or other substances with nutritional or physiological effects, marketed in dose form – capsules, pastilles, tablets, pills, sachets of powder, ampoules of liquids, drop dispensing bottles and other similar forms of liquids and powders designed to be taken in measured small unit quantities. Only vitamins and minerals are considered nutrient substances and listed in Annexes I and II of the Directive. Although food supplements are regulated differently from food(22), they are a kind of foodstuff and the regulation of health claims made on food applies. European regulation considers three types of H-RC(21,23,24) in food supplements advertising:
So-called disease claims, which are not permitted in Europe under Article 2 (b) of Directive 2000/13/EC of the European Parliament and of the Council of 20 March 2000 on the approximation of the laws of the Member States relating to the labelling, presentation and advertising of foodstuffs(23). The article states that the labelling and methods used must not attribute to any foodstuff the property of preventing, treating or curing a human disease, or even refer to such properties. These prohibitions or restrictions also apply to advertising. Indeed, the same principle is applicable to the advertising of food supplements, under Article 6 of Directive 2002/46/EC of the European Parliament and Council of the 10 June 2002 on the approximation of the laws of the Member States relating to food supplements(21).
Function claims (structure–function claims in the USA), which state, suggest or imply that a relationship exists between a food category – or one of its constituents – and health. Article 13.1 of Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on food(24) refers or describes the role of nutrients or other substances in the growth, development and functions of the body; in psychological and behavioural functions; and in slimming, weight-control, reduction in the sense of hunger or increase in the sense of satiety. These function claims are only permitted when based on and substantiated by generally accepted scientific evidence, authorised after scientific review by the European Food Safety Authority (EFSA) and listed in a register by the European Commission(12). Food supplements are concentrated sources of nutrients or other substances with a nutritional or physiological effect.
Reduction of disease risk claims, and those referring to children’s development and health, is any H-RC that states, suggests or implies that the consumption of a food category, a food or one of its constituents significantly reduces a risk factor involved in the development of a human disease. According to Article 14 of the mentioned Directive(24), these claims may be made when they have been authorised after application for inclusion in a Community list of such permitted claims. The Process for the Assessment of Scientific Support for Claims on Foods (PASSCLAIM) has ‘the potential to increase public confidence in the role of diet in maintaining and improving health and wellbeing’ (p. 1214S)(25).
Most studies analysing H-RC and product information in dietary supplements advertising refer to the Dietary Supplement Health and Education Act of 1994 of the Food and Drug Administration of the USA. Previous research by Soller, Rice and Ambrose(26) and Ethan et al. (27) has shown that function claims prevail in magazine dietary supplements advertisements, reaching 58 % and 79 %, respectively. However, Avery, Eisenberg and Cantor(28) found that 87 % of magazine dietary supplements advertisements contained function claims which referred to serious diseases and/or ailments such as cancer/risk of cancer, heart disease or deteriorating brain function. The work of Lee et al. (29) shows that prevalent claims in newspaper and television dietary advertisements referred to general health (40 %) were disease-specific (38·8 %), therapeutic (17·6 %) or were made for sexual, cosmetic or weight-loss purposes (14·7 %), while Chung et al. (30) demonstrated that 84·5 % of newspaper advertisements included up to twelve different disease claims per product. On the other hand, although some studies have shown that most dietary supplements advertisements failed to provide accurate and comprehensive information(31,32) and did not indicate the primary ingredient (79 %)(27), others concluded that this type of advertising included an identifiable ingredient (91·1 %) of the product containing two or more components(29). Finally, Philen et al. (33) found that amino acids were the most frequently mentioned ingredient (21·7 %) in health and bodybuilding magazines, whereas in the work of Lee et al. (29), herbal ingredients were mentioned in 70·1 % of cases.
Outside the scope of the US regulatory framework, Hassali et al. (34) evaluated the compliance of ingredients and functional claims made in women’s magazines with the guidelines established by the Malaysian Advertisements Board. They found that 13·3 % of advertisements in women’s magazines contained claims about restoring, improving or enhancing sexual health and that the most frequently mentioned ingredients were vitamins (17·8 %), proteins (10·2 %) and minerals (9·6 %).
In the European context, little research has been conducted to examine health-related information in food supplements advertising. Baudischova et al. (35) have paid attention to the adequacy of online information on the most consumed food supplements in the Czech Republic, analysing their active substances, general composition and the legitimacy of their health claims. They found that prohibited health claims were included in 8·5 % of Czech websites, with a prevalent presence of vitamins, minerals and non-herbal ingredients. Likewise, two studies by Perelló and Muela(36,37) are closely related to this research. In the first, they identified misleading claims in advertising of health-related products to quantify the presence of messages offering health benefits in Spain. In doing so, they analysed radio spots for products with intended healthcare purposes, from the perspective of Spanish regulation. The main result showed that health-related advertisements represent 69·09 % of unlawful claims(36). In the second study, they analysed the presence of different types of endorsers, some of them prohibited by European Directives and related to H-RC and product content information(37). This work revealed that celebrities prevail in function and reduction of disease risk claims (25 % and 11·4 %, respectively), while doctors frequently endorse food supplements in radio spots using disease claims (48·1 %). Additionally, 73 % of H-RC lack the compulsory substantiation of authorised ingredients. However, nothing so far has analysed H-RC and related product information in food supplements from the European regulatory perspective.
It is important to remember at this point that Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on foods establishes in Article 3 that health claims shall not be false, ambiguous or misleading. Since all H-RC must be truthful and the European Directive on food supplements only allows vitamins and minerals for substantiation(21), the main objective of this work is to analyse the presence of misleading and false claims and non-authorised ingredients to establish whether food supplements advertising breaches these regulatory principles.
Methods
According to the American Marketing Association, an advertising claim is a statement about the benefits, properties and/or performance of a product or service, designed to persuade consumers to make a purchase. Likewise, a health claim states, suggests or implies that a relationship exists between a food category, a food or one of its constituents and health(24). Taking this into consideration, we have chosen to analyse mentions in radio advertising due to the descriptive nature of their verbal messages, usually broadcast live by radio personalities.
On the other hand, 44 % of Spanish citizens(38) and 59 % of Europeans identify the radio medium as the news source they trust the most(39). In line with our decision, we selected Spanish news/talk radio stations providing informative content and up-to-date news. Two criteria were considered in the selection process: national coverage and transmission in Spanish.
According to data from the Estudio General de Medios(40), the stations with the highest audience levels are Cadena Ser, Cadena Cope and Onda Cero, which together total 9 000 000 daily listeners. The methodology used followed the quantitative approach of content analysis of all radio mentions broadcast throughout 2017. According to Krippendorff(41), this technique allows researchers to make ‘replicable and valid inferences from texts (or other meaningful matter) to the contexts of their use’ (p. 24).
Empirical application
The constituent data of the analysis were obtained from Arce Media (incorporated to the Nielsen database in 2007), dedicated to the collection of data for analysis of advertising activity in mainstream media. Using specific software, the company monitors and registers all radio advertising broadcast in different formats. The authors have bought access to the database and therefore to the mentions of the required product category broadcast in the referenced year in mp3 format.
In this work, food supplements are part of a non-medication group within the health category which includes food and vitamin complexes, tonics, energy boosters, cell regeneration supplements, weight-loss supplements, vitamins and other health and nutrition products. Following these selection criteria, the final corpus is composed of 437 radio mentions, comprising the entire universe. The analysis and coding process was conducted by two trained coders according to the variables and attributes presented in Table 1. The coders are two researchers, members of the research project funded by the Spanish Government under which this investigation has been carried out.
Table 1.
Categories, variables, attributes, concepts and definitions for the coding process
| Category | Variables | Attributes | Concept | Operationalised definition |
|---|---|---|---|---|
| Types of health-related claims * | Disease Claims (DC) | (1) Absence | Refer to the treatment, prevention or cure of a human illness. | The statement refers to the product’s effects on a disease, making an explicit claim (e.g. brand “X” improves arthrosis) or an implicit claim (e.g. brand “X” relieves joint pain). These claims are not allowed by European Regulation. |
| (2) Presence | ||||
| Function Claims (FC) † | (1) Absence | Refer or describe the role of nutrients or other substances in the growth, development and functions of the body; in psychological and behavioural functions; and in slimming, weight-control, reduction in the sense of hunger or increase in the sense of satiety. | Two examples of claims authorised by EFSA are: Ca is necessary for the preservation of bones in good condition, and it helps normal muscle function and neurotransmission. These claims are solely permitted when based on generally accepted scientific evidence and authorised after review by the European Food Safety Authority (EFSA). |
|
| (2) Authorised | ||||
| (3) Non-Authorised | ||||
| Reduction of Disease Risk Claims (RDRC) † | (1) Absence | State, suggest or imply that the consumption of a food category or one of its constituents significantly reduces a risk factor in the development of a human disease. | An example of a claim authorised by EFSA based on the previously mentioned mineral is: Ca contributes to reduce the loss of bone mineral in post-menopausal women. Low bone mineral density is a risk factor for osteoporotic bone fractures. These claims might be made when authorised by EFSA through the Process for the Assessment of Scientific Support for Claims on Foods (PASSCLAIM) and included in a Community list. |
|
| (2) Authorised | ||||
| (3) Non-Authorised | ||||
| Product content information * | (1) Vitamins † | (1) Absence | The mentioned ingredients and substances contained in the product. | |
| (2) Authorised | ||||
| (3) Non-Authorised | ||||
| (2) Mineral † | (1) Absence | |||
| (2) Authorised | ||||
| (3) Non-Authorised | ||||
| (3) Other substances † | (1) Absence | |||
| (2) Authorised | ||||
| (3) Non-Authorised |
Non-exclusive category, since one or more claims can be included in an advertisement. Conceptualisation was based on EU regulation.
To encode whether a claim or ingredient has been authorised by EFSA, it was verified in the official website of the EU register on nutrition and health claims. (http://ec.europa.eu/food/safety/labeling_nutrition/claims/register/public/?event=search).
Data reliability
The inter-codifier reliability was measured using Cohen’s Kappa(42), which raises a variation between 0·785 and 1, calculated with SPSS (version 17). With regard to the variables included in the category Types of Health-Related Claims, for Disease Claims k = 0·785, for Function Claims k = 1 and for Reduction of Disease Risk Claims k = 0·955. Finally, k = 1 in the case of all variables integrating the Product content information category, i.e. Vitamins, Minerals and Others. To respond to the few differences detected, a third working session took place. The discrepancies are mainly concentrated in the non-structural variables that required a subjective interpretation of advertising content related to therapeutic functions or disease symptoms and risks factors. Once these contradictions were detected, the authors and the coders themselves evaluated each case to properly adjust it to the initial formulation of each variable. After evaluating the different situations, the final coding of the cases in question was decided. The results listed below are based on a value k = 1 for all variables. In addition, all crossed data for the analysis of variables have undergone relevant statistical significance tests using nonparametric χ 2 analysis.
Results
The content analysis of the 437 food supplements radio mentions shows a high presence of claims and product ingredients non-authorised by EFSA. It is worth noting that the analysed variables are non-exclusive, since one or more claims and/or ingredients can be mentioned in an advertisement, as shown in Fig. 1. In this regard, the presence of function claims has been detected in all advertisements, non-authorised in 80·3 % of cases (351). On the other hand, and although prohibited by European regulation, disease claims are present in 1 of 5 advertisements (20·4 %). Finally, the presence of reduction of disease risk claims is marginal (8·7 %), but none of the thirty-eight cases detected has been authorised.
Fig. 1.
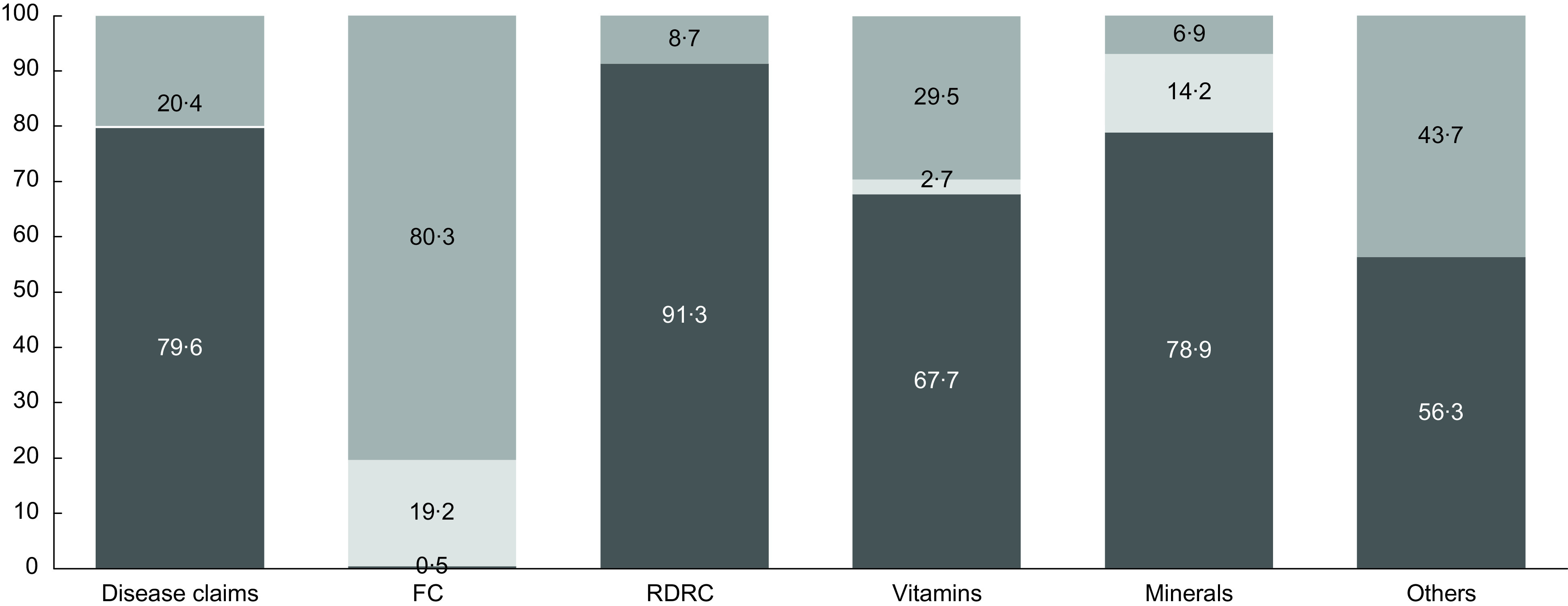
Presence of Health-Related Claims and Product Content Information (%). Absence;
Absence; Authorised;
Authorised;  Non-Authorised
Non-Authorised
As previously mentioned, only vitamins and minerals are considered nutrient substances in food supplements, while other product ingredients need to be authorised through PASSCLAIM by EFSA. The results in Fig. 1 show that nearly half of all other substances are illicit (43·7 %). Vitamins and minerals show an inverse proportionality; that is, a high presence of non-authorised claims mentioning vitamins goes together with a low presence of authorised claims, while in the case of minerals, the opposite is true – mentions of authorised substances (14·2 %) are more frequent than those of non-authorised substances.
The unallowed use of disease claims in advertising is particularly significant. The property of preventing or curing a human disease cannot be attributed to a food supplement. Nevertheless, the presence of this type of claim has been detected in eighty-nine advertisements, which in all instances mention a substance responsible for the improvement of consumers’ health. Specifically, vitamins, minerals and other substances appear in 24·7 %, 22·5 % and 57·3 % of these claims, respectively, when it is not legally possible to use advertising arguments based on the presence of these substances in such claims (Table 2). The following are two examples of disease claims identified in the analysis: ‘[to prevent the early symptoms of memory loss due to aging]’ and ‘[for you who suffer from discomfort and knee and joint pain]’.
Table 2.
Disease claim and product content information
| Absence | Presence | Total | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Vitamins* | Absence | 229 | 65·80 | 67 | 75·30 | 296 | 67·70 |
| Non-authorised presence | 119 | 34·2 | 22 | 24·7 | 141 | 32·30 | |
| Total | 348 | 100·00 | 89 | 100·00 | 437 | 100·00 | |
| Minerals† | Absence | 276 | 79·30 | 69 | 77·50 | 345 | 78·90 |
| Non-authorised presence | 72 | 20·70 | 20 | 22·50 | 92 | 21·1 | |
| Total | 348 | 100·00 | 89 | 100·00 | 437 | 100·00 | |
| Others‡ | Absence | 208 | 59·80 | 38 | 42·70 | 246 | 56·30 |
| Non-authorised presence | 140 | 40·20 | 51 | 57·30 | 191 | 43·70 | |
| Total | 348 | 100·00 | 89 | 100·00 | 437 | 100·00 | |
Disease Claim and Vitamins χ 2: 3626; Significance: P < 0·0163.
Disease Claim and Minerals χ 2: 55 539; Significance: P < 0·000.
Disease Claim and Others χ 2: 8397; Significance: P < 0·004.
If we apply the same analytical approach to function claims, Table 3 also shows a predominant presence of non-authorised claims that mention vitamins, minerals and other substances as advertising arguments to reinforce the health benefits of the advertised product. Of the 351 advertisements that include a function claim, 54·10 % mention other substances which have not been authorised. The following extracts provide examples of the same product in different advertisements using function claims: ‘[in cases of fatigue, physical or mental exhaustion]’, ‘[Brand X increases physical and mental energy]’ and ‘[it is revitalising thanks to its exclusive formula which will help you overcome tiredness and fatigue]’. These examples do not refer to any substance, yet the following one, from the same brand, does: ‘[with royal jelly, ginseng and vitamins, which help us recover our energy and vitality]’. Indeed, in the case of royal jelly, the status of claims such as ‘helps in cases of fatigue; helps to support our body’s vitality; helps to make you feel more energetic; enhancement of vitality/energy’ is non-authorised. The same applies to vitamins, present in 36·80 % of non-authorised claims. However, in the case of minerals, their non-authorised presence is residual when compared with the rest of substances, with only 8·5 %. In fact, these inorganic components are adequately mentioned and authorised in 73·8 % of function claims. The next example presents two authorised function claims substantiated with different minerals: ‘[it contains zinc which contributes to normal DNA synthesis, and selenium which protects cells against oxidative stress]’.
Table 3.
Function claim and product content information
| Absence | Authorised presence | Non-authorised presence | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Vitamins* | Absence | 2 | 100·00 | 84 | 100·00 | 210 | 59·80 | 296 | 67·70 |
| Authorised presence | 0 | 0·00 | 0 | 0·00 | 12 | 3·40 | 12 | 2·70 | |
| Non-authorised presence | 0 | 0·00 | 0 | 0·00 | 129 | 36·80 | 129 | 29·50 | |
| Total | 2 | 100·00 | 84 | 100·00 | 351 | 100·00 | 437 | 100·00 | |
| Minerals† | Absence | 2 | 100·00 | 22 | 26·20 | 321 | 91·50 | 345 | 78·90 |
| Authorised presence | 0 | 0·00 | 62 | 73·80 | 0 | 0·00 | 62 | 14·20 | |
| Non-authorised presence | 0 | 0·00 | 0 | 0·00 | 30 | 8·50 | 30 | 6·90 | |
| Total | 2 | 100·00 | 84 | 100·00 | 351 | 100·00 | 437 | 100·00 | |
| Others‡ | Absence | 1 | 50·00 | 84 | 100·00 | 161 | 45·90 | 246 | 56·30 |
| Authorised presence | 0 | 0·00 | 0 | 0·00 | 0·00 | 0 | 0·00 | 0·00 | |
| Non-authorised presence | 1 | 50·00 | 0 | 0·00 | 190 | 54·10 | 191 | 43·70 | |
| Total | 2 | 100·00 | 84 | 100·00 | 351 | 100·00 | 437 | 100·00 | |
Function Claim and Vitamins χ 2: 51 004; Significance: P < 0·000.
Function Claim and Minerals χ 2: 304 578; Significance: P < 0·000.
Function Claim and Others χ 2: 80 753; Significance: P < 0·000.
Table 4 shows that reduction of disease risk claims also has a significant non-authorised presence. So much so, that there is not one single instance of vitamins, minerals or other substances authorised by EFSA to support this type of claim. Brands use reduction of disease risk claims to advertise how the consumption of a certain product can reduce the risk of developing a disease, as in the following extract of one the analysed advertisements: ‘[Brand X decreases bad cholesterol levels and prevents the formation of cholesterol oxidation]’. Although this type of claim is not particularly relevant in the analysed sample – it is only included in thirty-eight advertisements – non-authorised other substances are present in 73·7 % of cases and non-authorised minerals and vitamins in 18·4 % and 15·8 %, respectively. As a final consideration, it is worth noting that not one single instance of authorised substance has been detected in the reduction of disease risk claims included in the sample.
Table 4.
Reduction of disease risk claim and product content information
| Absence | Authorised presence | Non-authorised presence | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Vitamins* | Absence | 264 | 66·20 | 0 | 0·00 | 32 | 84·20 | 296 | 67·70 |
| Authorised presence | 12 | 3·00 | 0 | 0·00 | 0 | 0·00 | 12 | 2·70 | |
| Non-authorised presence | 123 | 30·80 | 0 | 0·00 | 6 | 15·80 | 129 | 29·50 | |
| Total | 399 | 100·00 | 0 | 0·00 | 38 | 100·00 | 437 | 100·00 | |
| Minerals† | Absence | 314 | 78·70 | 0 | 0·00 | 31 | 81·60 | 345 | 78·90 |
| Authorised presence | 62 | 15·50 | 0 | 0·00 | 0 | 0·00 | 62 | 14·20 | |
| Non-authorised presence | 23 | 5·80 | 0 | 0·00 | 7 | 18·40 | 30 | 6·90 | |
| Total | 399 | 100·00 | 0 | 0·00 | 38 | 100·00 | 437 | 100·00 | |
| Others‡ | Absence | 236 | 59·10 | 0 | 0·00 | 10 | 26·30 | 246 | 56·30 |
| Authorised presence | 0 | 0·00 | 0 | 0·00 | 0 | 0·00 | 0 | 0·00 | |
| Non-authorised presence | 163 | 40·90 | 0 | 0·00 | 28 | 73·70 | 191 | 43·70 | |
| Total | 399 | 100·00 | 0 | 0·00 | 38 | 100·00 | 437 | 100·00 | |
Reduction of disease risk claim and vitamins χ 2: 5469; Significance: P < 0·065.
Reduction of disease risk claim and minerals χ 2: 14 037; Significance: P < 0·001.
Reduction of disease risk claim and others χ 2: 15 201; Significance: P < 0·001.
Discussion
This work contributes to the scarce research on food supplements advertising in the European context(35,37), providing new insights. The analysis model proposed establishes a relationship between the different types of H-RC and the substances on which they are based, whether authorised or not by the different directives regulating food supplements in the EU. Thus, the main contribution of this work is that it analyses the compliance level of food supplements advertising in Spain with these regulatory principles, which must be respected by all European states.
Another distinctive contribution of this work is related to the selection of the analysed medium. This study has focused on news/talk radio stations due to their programming nature and audience, which is accustomed to news content. Indeed, radio is still considered the most trustworthy media source by Spaniards and Europeans(38,39). Although the main component of radio communication is verbal – as in the case of H-RC – product descriptions in advertising are always composed of verbal statements, so that this analysis model can be applied to any other type of media.
In line with previous research(28–30,35,37), this work has shown a high presence of disease claims – in one out of five analysed advertisements. Overall, the findings reveal that these illegal claims do not mention illnesses directly, although they do refer to them indirectly. For instance, ageing is manifestly referred to as joint pain instead of osteoarthritis, and memory loss is mentioned instead of senile dementia. Likewise, this type of claim, beyond the promise of healing and eliminating pain, prescribes the consumption of the product as a preventive measure, as shown in the following example: ‘[Mental agility and memory deteriorate with aging, especially after the age of 45. Brand X is a supplement that prevents this deterioration of memory and mental agility]’.
This analysis strongly confirms the findings of previous studies in which function claims were the most prevalent typology in food supplements advertising(26–29,34,37). The present work also concludes the absence of authorisation by EFSA in a striking majority of the claims (80·3 %). Describing health benefits as product attributes is another common practice in food supplements advertising: ‘[Brand X is the only product that normalises cholesterol]; [Brand Z looks after your memory]’. However, claims must only refer to the function of nutrients or other substances in terms of growth, development and functions of the body to preserve a healthy condition. Furthermore, our results have revealed claims that assure consumers of the alleged benefits of the product – ‘[Brand X is the solution]; [Brand X is a revitaliser of guaranteed effectiveness]’ – or appeal to a ‘[new, more powerful formula]’, ‘[exclusive formula]’, ‘[natural formula]’, ‘[effective formula tested by professional laboratories]’, or indicate that the product is available in pharmacies. These advertising practices influence consumer purchase decisions by omitting essential information about the product.
The high presence and ongoing repetition of false and unlawful claims(36) can lead to misinformation about what food supplements are and how they must be used(6–8,12–14). Consequently, and based on wrong beliefs, misled consumers buy and take food supplements which in most cases do not satisfy the health benefits advertised, often unaware of the health risks involved in their inadequate consumption.
Regarding the content information of food supplements advertising, and in line with previous studies(27,29,31–35), the results reveal the prevalence of advertisements which do not mention any regulated substances. Other substances prevail in the sample (43·7 %), even though the claims in which they appear have not been authorised. Unlike previous works which indicate that vitamins are the most mentioned substance(34,35), in our analysis, they hold second place (32·2 %) and their use is again illicit in most cases. Finally, minerals are the substance which registers the highest number of authorised claims, despite having the lowest presence (21 %), appearing in only 14·2 % of the radio mentions. The use of vague and general arguments such as ‘[Brand X provides vitamins, minerals and nutrients]’ is common in food supplements advertising. Although these arguments have been included in the coding process, they cannot be considered authorised insofar as they do not specify the substance or the health benefit provided.
Advertising, now ubiquitous, informs consumers of the existence of products on the market that respond to many needs, with enormous speed and efficiency. However, consumers can make mistaken purchase decisions(9,10,12,13) as a result of malpractices in the commercialisation of food supplements – illicit, deceptive and false claims, or the omission of essential information about the product’s characteristics and/or benefits(36). In this regard, it is important to consider that the current regulation(24) states as a general principle that health-related properties should not be uncertain, confusing or misleading.
Finally, the analysis shows a recurrent use of fear appeals and the inclusion of clinical or medical terms such as ‘symptoms’, or risk factors that contribute to the worsening of the quality of life; some statements even indicate the dosage to be taken, as if prescribed by a physician: ‘[Two capsules a day of Brand X relieves pain]; [two capsules a day is enough]; [one capsule a day reduces and normalises bad cholesterol levels]’.
Policy implications
While in a fast-growing market scenario, the demand for food supplements is expanding worldwide(1), legislation – relatively recent in the EU – and its compliance continue to be deficient. Food supplements advertising is controversial since it promotes and provides information about products which may pose a risk to consumers’ health or involve economic fraud(35,43).
The presence of illicit H-RC is a matter of serious concern that can lead to false beliefs and inappropriate behaviour in consumers(12–15). Many researchers and experts, e.g.,(4,9,10) have expressed their concern over these illicit practices and demanded more restrictive legislation and greater rigour in the supervision of manufacturers, given the administrative laxity, health problems caused and other issues detected since the application of the current legal text(2,4).
Recent studies have raised awareness of the significant presence of deceptive H-RC(29,35,36,44), which often lack scientific support(45) and plausibility(26,46). Although eliminating all misleading claims is the main objective of EU regulation, this research has identified the use of frequent vague claims that can definitely be considered deceptive by omission. Given the vast consumption of food supplements(1) and the irregularities detected in their advertising, it seems relevant to implement the following mechanisms to improve consumer protection: increased sanctions and control from self-regulation systems; stricter government supervision of the advertising activity and, in media, the implementation of a preclearance system to ensure that all messages are truthful and comply with regulation before their dissemination. Such actions would censor misleading messages before they reach the public and thus eliminate or drastically reduce the purchase of products that do not meet consumer expectations and their advertised benefits.
In view of its complexity, the issue must be approached comprehensively to include all stakeholders involved(47). The inclusion of food supplements in the market requires stricter regulation and monitoring by governments. For their part, public administrations and the media must monitor the content of food supplements advertisements to verify their compliance with legislation(9). The objective is to prevent unlawful, false or misleading H-RC from reaching consumers and to confront regulatory challenges in this area which continue to be disregarded(4). The effectiveness of self-regulation systems must be increased to include adequate sanctions for offenders in order to encourage advertisers to act with greater responsibility. Specifically, the Spanish self-regulation authority is constantly questioned because certain brands of food supplements have been advertising these types of unlawful H-RC for many years(36) and continue to do so today with total impunity, despite having been the subject of complaints in the past(48,49). In addition, administrations should improve public awareness of all aspects involved in the consumption of food supplements and other controversial products through educational campaigns, so future consumers can make informed purchase decisions.
Limitations and future research
The present work has addressed the radio medium and full-service broadcasting stations. Further research could extend the analysis to other types of radio stations and media. For example, it would be relevant to cross-nationally compare the presence of false and misleading H-RC of food supplements in selected European countries with a common regulatory framework, in order to gain insight into the impact of sociological and cultural factors on this framework.
The model developed in this research could be applied to the analysis of other types of claims included in Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on foods. In this regard, it would be interesting to cross-check the variables of nutrition claims with those of nutrients in food advertising or in certain categories of food different from food supplements, and confirm whether they are permitted or not to verify compliance with regulation. This analysis could feasibly be conducted based on updated information published by EFSA.
Another limitation of this work is that it only analyses the presence of H-RC and substances authorised in the regulation for food supplements. Therefore, future research could approach the same subject but from the perspective of self-regulation, through the analysis of complaints and resolutions. Likewise, an analysis from consumers’ perspective would be of great relevance to find out their level of knowledge and ability to distinguish between the different types of H-RC(43).
The findings of our work may also be used as the starting point of future research that would provide continuity and resolve emerging hypotheses. For instance, one of the three analysed news/talk radio stations did not broadcast food supplements mentions, which triggers an interest to determine the causes of this behaviour. On the other hand, it would be interesting to interview radio owners, radio personalities and newscasters to gain information about the advertising management process, paying special attention to the acceptance, production, revision and dissemination of food supplements advertisements and the verification of the information they provided within the message. Finally, lines of future research could also include an analysis of self-regulation and accountability systems and of radio stations’ editorial line or style guide.
Conclusions
The constant use of health claims not allowed by law in food supplements advertising is a matter of serious concern. Advertisers are held accountable when the regulation is breached, but the responsibility must be extended to include media owners, who currently act with total impunity. The worrying presence of deceptive messages – vague or false claims, and the omission of essential information – in food supplements advertising demands stricter monitoring and control from public administrations and self-regulation systems, and the introduction of exemplary sanctions to deter offenders and protect consumers. The conclusions drawn from the analysis of the European framework strongly suggest the need for an effective action plan that would modify the current regulation on food supplements advertising, as well as a common framework of sanctions. This would allow policymakers across Europe to protect consumers from the potentially harmful effects of their consumption, in many cases encouraged by advertising malpractices. In this respect and to preserve consumer safety, it seems essential to change the current regulation so that everybody involved in this illicit health-related advertising can be held accountable for their actions.
Acknowledgements
Acknowledgements: The authors would like to acknowledge to Bárbara Castillo Abdul and Fátima Gómez Buil for assistance in coding process. Financial support: This work was supported by the Ministry of Economy and Competitiveness of de Government of Spain, State Program R&D Oriented Society Challenges, under Grant (CSO2017-82267-R). Conflict of interest: The authors confirm that they have no conflicts to report. Authorship: C.M.-M. suggested the research idea, designed the study and outlined the variables to be considered. She provided the theoretical background and prepared the first draft of the paper. S.P.-O. was responsible for the research design and the elaboration of the manual for coders. He led the coding of the data, the statistical analysis and interpreted the results. A.G.-A. was involved in data collection and was the second evaluator in cases of discrepancies. She edited the last drafts of the paper. All of the authors were involved in preparing and reviewing the manuscript. Ethics of human subject participation: The study did not involve human subjects.
References
- 1. Euromonitor International (2021) Sales on Consumer Health. Vitamins and Dietary Supplements. https://www.portal.euromonitor.com/portal/statisticsevolution/index (accessed January 2021).
- 2. Binns CW, Lee MK & Lee AH (2018) Problems and prospects: public health regulation of dietary supplements. Annu Rev Public Health 39, 403–420. [DOI] [PubMed] [Google Scholar]
- 3. Kreth ML (2000) Exploring ‘responsibility’ in advertising: health claims about dietary supplements. Bus Commun Q 63, 66–72. [Google Scholar]
- 4. Starr RR (2015) Too little, too late: ineffective regulation of dietary supplements in the United States. Am J Public Health 105, 478–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bailey RL, Gahche JJ, Miller PE et al. (2013) Why US adults use dietary supplements. JAMA Intern Med 173, 355–361. [DOI] [PubMed] [Google Scholar]
- 6. Okleshen Peters CL, Shelton J & Sharma P (2003) An investigation of factors that influence the consumption of dietary supplements. Health Mark Q 21, 113–135. [DOI] [PubMed] [Google Scholar]
- 7. Pajor EM, Eggers SM, Curfs KCJ et al. (2017) Why do Dutch people use dietary supplements? Exploring the role of socio-cognitive and psychosocial determinants. Appetite 114, 161–168. [DOI] [PubMed] [Google Scholar]
- 8. Dickinson A & MacKay D (2014) Health habits and other characteristics of dietary supplement users: a review. Nutr J 13, 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Denham BE (2011) Dietary supplements—regulatory issues and implications for public health. JAMA 306, 428–429. [DOI] [PubMed] [Google Scholar]
- 10. Ashar BH, Miller RG, Pichard CP et al. (2008). Patients’ understanding of the regulation of dietary supplements. J Community Health 33, 22–30. [DOI] [PubMed] [Google Scholar]
- 11. Geller AI, Shehab N, Weidle NJ et al. (2015) Emergency department visits for adverse events related to dietary supplements. N Engl J Med 373, 1531–1540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Mariotti F, Kalonji E, Huneau JF et al. (2010) Potential pitfalls of health claims from a public health nutrition perspective. Nutr Rev 68, 624–638. [DOI] [PubMed] [Google Scholar]
- 13. Nocella G & Kennedy O (2012) Food health claims – what consumers understand. Food Policy 37, 571–580. [Google Scholar]
- 14. Royne MB, Myers SD, Deitz G et al. (2016) Risks, benefits, and competitive interference: consumer perceptions of prescription drug versus dietary supplement advertising. J Curr Issues Res Advert 37, 59–79. [Google Scholar]
- 15. Vladeck DC (2000) Truth and consequences: the perils of half-truths and unsubstantiated health claims for dietary supplements. JPP&M 19, 132–138. [Google Scholar]
- 16. Chandra A & Holt GA (1999) Pharmaceutical advertisements: how they deceive patients. J Bus Ethics 18, 359–366. [Google Scholar]
- 17. Drumwright ME & Murphy PE (2004) How advertising practitioners view ethics: Moral muteness, moral myopia, and moral imagination. J Advert 33, 7–24. [Google Scholar]
- 18. Ferrell OC & Ferrell L (2021) New directions for marketing ethics and social responsibility research. J Mark Theory Pract 29, 13–22. [Google Scholar]
- 19. Kulkarni A, Huerto R, Roberto CA et al. (2017) Leveraging corporate social responsibility to improve consumer safety of dietary supplements sold for weight loss and muscle building. Transl Behav Med 7, 92–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Serota KB (2019) Deceptive marketing outcomes: a model for marketing communications. In The Palgrave Handbook of Deceptive Communication, pp. 813–837 [Doncan-Morgan T, editor]. Cham: Palgrave Macmillan. [Google Scholar]
- 21. European Parliament and Council (2002) Directive 2002/46/EC of the European Parliament and of the Council of 10 June 2002 on the approximation of the laws of the Member States relating to food supplements (Text with EEA relevance). http://data.europa.eu/eli/dir/2002/46/2017-07-26 (accessed April 2018).
- 22. Katan MB & de Roos NM (2003) Toward evidence-based health claims for foods. Science 299, 206–207. [DOI] [PubMed] [Google Scholar]
- 23. European Parliament and Council (2000) Directive 2000/13/EC of the European Parliament and of the Council of 20 March 2000 on the approximation of the laws of the Member States relating to the labelling, presentation and advertising of foodstuffs. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32000L0013&from=EN (accessed April 2018).
- 24. European Parliament and Council (2006) Regulation (EC) No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on nutrition and health claims made on foods. http://data.europa.eu/eli/reg/2006/1924/2014-12-13 (accessed April 2018).
- 25. Asp NG & Bryngelsson S (2008) Health claims in Europe: new legislation and PASSCLAIM for substantiation. J Nutr 138, 1210S–1215S. [DOI] [PubMed] [Google Scholar]
- 26. Soller RW, Rice LG & Ambrose PJ (2007) Disclaimers in dietary supplement print advertising: the bodybuilding category as a model case for change. Food Drug LJ 62, 375–386. [PubMed] [Google Scholar]
- 27. Ethan D, Basch CH, Berdnik A et al. (2016) Dietary supplements advertised in muscle enthusiast magazines: a content analysis of marketing strategies. Int J Men’s Health 15, 194–202. [Google Scholar]
- 28. Avery RJ, Eisenberg MD & Cantor JH (2017) An examination of structure-function claims in dietary supplement advertising in the US: 2003–2009. Prev Med 97, 86–92. [DOI] [PubMed] [Google Scholar]
- 29. Lee A, Vásquez LJ, Wong WC et al. (2015) Evaluation of dietary supplement advertisements in popular Spanish, Chinese, and Korean media outlets: a cross sectional study. BMC Nutr 1, 43. [Google Scholar]
- 30. Chung EP, Hwang HJ & Kim MK (2007) Evaluation of non-English dietary supplement advertisements in an ethnic minority community in America. Public Health Nutr 10, 834–837. [DOI] [PubMed] [Google Scholar]
- 31. Kava R, Meister KA, Whelan EM et al. (2002) Dietary supplement safety information in magazines popular among older readers. J Health Commun 7, 13–23. [DOI] [PubMed] [Google Scholar]
- 32. Shaw P, Zhang V & Metallinos-Katsaras E (2009) A content analysis of the quantity and accuracy of dietary supplement information found in magazines with high adolescent readership. J Altern Complement Med 15, 159–164. [DOI] [PubMed] [Google Scholar]
- 33. Philen RM, Ortiz DI, Auerbach SB et al. (1992) Survey of advertising for nutritional supplements in health and bodybuilding magazines. JAMA 268, 1008–1011. [PubMed] [Google Scholar]
- 34. Hassali MA, Saleem F, Aljadhey H et al. (2012) Evaluating the content of advertisements for dietary supplements in Malaysian women’s magazines. Drug Inf J 46, 723–728. [Google Scholar]
- 35. Baudischova L, Straznicka J, Pokladnikova J et al. (2018) The quality of information on the internet relating to top-selling dietary supplements in the Czech Republic. Int J Clin Pharm 40, 183–189. [DOI] [PubMed] [Google Scholar]
- 36. Perelló S & Muela C (2011) An analysis of health-related advertising in Spanish radio. Cuadernos Info 29, 67–76. [Google Scholar]
- 37. Muela-Molina C, Perelló-Oliver S & García-Arranz A. (2021). Health-related claims in food supplements endorsements: a content analysis from the perspective of EU regulation. Public Health 190, 168–172. [DOI] [PubMed] [Google Scholar]
- 38. Toharia JJ (2017) Pulso de España 2016. Un informe sociológico [The pulse of Spain 2016. A sociological report]. http://metroscopia.org/confianza-en-las-instituciones-espana-en-perspectiva-comparada/ (accessed November 2018).
- 39. European Commission (2018) Flash Eurobarometer 464 Report. Fake news and disinformation online. https://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/ResultDoc/download/DocumentKy/82797 (accessed June 2019).
- 40. AIMC (Asociación para la Investigación de Medios de Comunicación) (2017) Resumen General del EGM (Estudio General de Medios) [EGM (Media General Study) General Report] February 2017 to November 2017. https://www.aimc.es/a1mc-c0nt3nt/uploads/2017/05/resumegm317.pdf (accessed December 2017).
- 41. Krippendorff K (2018) Content Analysis: An Introduction to its Methodology, 4th ed. Los Ángeles: Sage. [Google Scholar]
- 42. Cohen J (1960) A coefficient of agreement for nominal scales. Educ Psychol Meas 20, 37–46. [Google Scholar]
- 43. DeLorme DE, Huh J, Reid LN et al. (2012) Dietary supplement advertising in the US: a review and research agenda. Int J Advert 31, 547–577. [Google Scholar]
- 44. Parker BJ (2003) Food for health. The use of nutrient content, health, and structure/function claims in food advertisements. J Advert 32, 47–55. [Google Scholar]
- 45. McCann MA (2005) Dietary supplement labeling: cognitive biases, market manipulation & consumer choice. Am J Law Med 31, 215–268. [DOI] [PubMed] [Google Scholar]
- 46. Brennan R, Czarnecka B, Dahl S et al. (2008) Regulation of nutrition and health claims in advertising. J Advert Res 48, 57–70. [Google Scholar]
- 47. Aschemann-Witzel J (2011) The EU health claim regulation in international comparison: review of the possible impact on food marketing and consumer protection. CAB Rev 6, 1–7. [Google Scholar]
- 48. Muela-Molina C (2014) Misleading advertising in food products. In Communication and Body Image, pp.149–164 [Sánchez Hernández MF, Jiménez Morales M & Carrillo Durán MV, editors]. México: Pearson. [Google Scholar]
- 49. Perelló-Oliver S, Muela-Molina C & Hormigos-Ruiz J (2016) Unlawful advertising, health products and self-regulation. Cuadernos Info 38, 51–67. [Google Scholar]