

Abstract
Background
In complex teeth like maxillary premolars, endodontic treatment success depends on a complete comprehension of root canal anatomy. The research on mandibular premolars’ root canal anatomy has been extensive and well-documented in existing literature. However, there appears to be a notable gap in available data concerning the root canal anatomy of maxillary premolars. This study aimed to explore the root canal morphology of maxillary premolars using cone-beam computed tomography (CBCT) imaging, considering age and gender variations.
Methods
From 500 patient CBCT scans, 787 maxillary premolar teeth were evaluated. The sample was divided by gender and age (10–20, 21–30, 31–40, 41–50, 51–60, and 61 years and older). Ahmed et al. classification system was used to record root canal morphology.
Results
The most frequent classifications for right maxillary 1st premolars were 2MPM1 B1 L1 (39.03%) and 1MPM1 (2.81%), while the most frequent classifications for right maxillary 2nd premolars were 2MPM1 B1 L1 (39.08%) and 1MPM1 (17.85%). Most of the premolars typically had two roots (left maxillary first premolars: 81.5%, left maxillary second premolars: 82.7%, right maxillary first premolars: 74.4%, right maxillary second premolars: 75.7%). Left and right maxillary 1st premolars for classes 1MPM1 and 1MPM1–2−1 showed significant gender differences. For classifications 1MPM1 and 1MPM1–2−1, age-related changes were seen in the left and right maxillary first premolars.
Conclusion
This study provides novel insights into the root canal anatomy of maxillary premolars within the Saudi population, addressing a notable gap in the literature specific to this demographic. Through CBCT imaging and analysis of large sample sizes, the complex and diverse nature of root canal morphology in these teeth among Saudi individuals is elucidated. The findings underscore the importance of CBCT imaging in precise treatment planning and decision-making tailored to the Saudi population. Consideration of age and gender-related variations further enhances understanding and aids in personalized endodontic interventions within this demographic.
Keywords: Cone beam computed tomography, Dental anatomy, Dental diagnostic imaging, Dental pulp, Endodontics, Morphology, Root, Root canal, Premolars
Introduction
The morphology and variability of root canal systems play a crucial role in the success of endodontic treatment [1, 2]. Understanding the intricacies of root canal anatomy is essential for effective diagnosis, treatment planning, and applying appropriate techniques. The research on mandibular premolars’ root canal anatomy has been extensive and well-documented in existing literature [3, 4]. However, there appears to be a notable gap in available data concerning the root canal anatomy of maxillary premolars [5–9].
Maxillary premolars present unique challenges due to their anatomical complexity, including multiple canals, isthmuses, and accessory canals [10, 11]. Accurately identifying and classifying root canal systems in maxillary premolars is crucial for diagnosis and achieving optimal treatment outcomes [12].
Despite the importance of understanding root canal morphology, there remains a gap in knowledge concerning maxillary premolars. This lack of comprehensive information on the root canal morphology of maxillary premolars hinders endodontic practitioners’ ability to deliver precise and successful treatments [13]. This study aims to fill this gap by conducting an investigation using cone-beam computed tomography (CBCT) imaging. CBCT, as a non-invasive and highly accurate imaging technique, offers the advantage of providing detailed three-dimensional representations of root canal systems, which were previously not easily achievable through conventional radiographs [14]. The high-resolution images obtained through CBCT will provide valuable data to enhance the knowledge and clinical management of root canal anatomy in these teeth, leading to better-informed treatment decisions and reduced complications [4, 15].
By analyzing a large sample size of CBCT images, we aim to comprehensively understand the root canal configuration in maxillary premolars, considering factors such as age and gender [16]. The findings of this study will contribute to enhancing the knowledge and clinical management of root canal anatomy in maxillary premolars, improving treatment success rates, and reducing complications.
By elucidating the variations and complexities of root canal morphology in maxillary premolars, this study will aid dental professionals in making informed decisions regarding treatment approaches, instrument selection, and the application of advanced endodontic techniques [17, 18]. Furthermore, the results will provide valuable insights for dental educators, researchers, and students, facilitating the development of standardized protocols and guidelines for managing root canal systems in maxillary premolars.
Methodology
Study design
This study employed a retrospective cross-sectional design to comprehensively investigate the root canal morphology of maxillary premolars using cone-beam computed tomography (CBCT) imaging. This design allows for the examination of a large sample size and facilitates the analysis of root canal anatomy variations among different age groups and genders. By retrospectively analyzing CBCT images, the study aimed to elucidate the complex root canal anatomy of maxillary premolars and identify potential factors influencing their variability.
Ethical consideration
Ethical approval was obtained from the Local Committee of Bioethics for Research at the Dentistry College, King Abdul-Aziz University (Ethical Approval No. 025-02-22). Informed consent was obtained from the Committee of Bioethics for Research, College of Dentistry, King Abdul-Aziz University, Jeddah, Saudi Arabia, considering the retrospective nature of the study. This ensured that the study adhered to ethical standards and protected the rights and confidentiality of the participants. Additionally, the study complied with all relevant regulations and guidelines regarding the use of patient data for research purposes.
Sample size determination
The sample size for this study was determined using G Power 3.1.9.4 software, considering a chi-square test for goodness-of-fit, statistical power analysis, and an a priori approach. A comprehensive sample of 500 patient records was obtained, resulting in the evaluation of 787 maxillary premolar teeth. This large sample size enhances the statistical power of the study and allows for robust analysis of root canal morphology variations. It also increases the generalizability of the findings to the target population.
Inclusion and exclusion criteria
Inclusion criteria were carefully defined to ensure the selection of appropriate teeth for analysis. Healthy maxillary premolars with small carious or restorative crowns, fully formed root apex, and defect-free radiographic images were included in the study. Exclusion criteria were applied to eliminate potential confounding factors, including root canal-treated teeth, fractured upper and lower posterior teeth, post and core restorations, calcification, resorption defects, and anomalies of crown and root. These criteria helped ensure the homogeneity of the study sample and the validity of the results.
Imaging technique
CBCT images were acquired using the iCAT scanner system (Imaging Sciences International, Hatfield, PA, USA), a widely recognized and reliable imaging device in dentistry. Standardized imaging parameters (120 KVp, 5–7 mA) were employed to ensure consistent image quality across all scans. The use of CBCT allowed for the acquisition of detailed three-dimensional representations of root canal anatomy, enabling precise analysis and classification. High-resolution images obtained through CBCT provided valuable data for evaluating root canal morphology.
Calibration and reliability
Prior to data collection, calibration was conducted involving an expert endodontist and an observer. The observer underwent rigorous training to accurately identify and classify root canal morphology. Calibration involved the examination of 50 CBCT images, with discrepancies resolved through discussion to achieve consensus. The kappa test was utilized to determine the level of agreement between observers, and intra- and interobserver reliability was assessed. Furthermore, specimens were assessed independently by observers following calibration to minimize bias and ensure consistency in the evaluations. A high kappa value (0.8) was obtained, indicating substantial to almost perfect reliability, thereby ensuring the validity of the data collected. This rigorous calibration process helped minimize observer bias and enhance the reliability of the study findings.
Root and canal analysis
Root canal morphology was recorded and classified according to the classification system proposed by Ahmed et al. in 2017. This classification system provides a standardized framework for describing root canal configurations, facilitating comparisons across studies. The obtained CBCT images were meticulously analyzed, with root canal morphology recorded for each maxillary premolar (Fig. 1). The images were divided into age groups (10 to 20, 21 to 30, 31 to 40, 41 to 50, 51 to 60, and 61 years above) and categorized by gender (males and females) to explore variations in root canal anatomy. Detailed analysis of each image was conducted to identify the number of roots, canals, and any anatomical variations present.
Fig. 1.
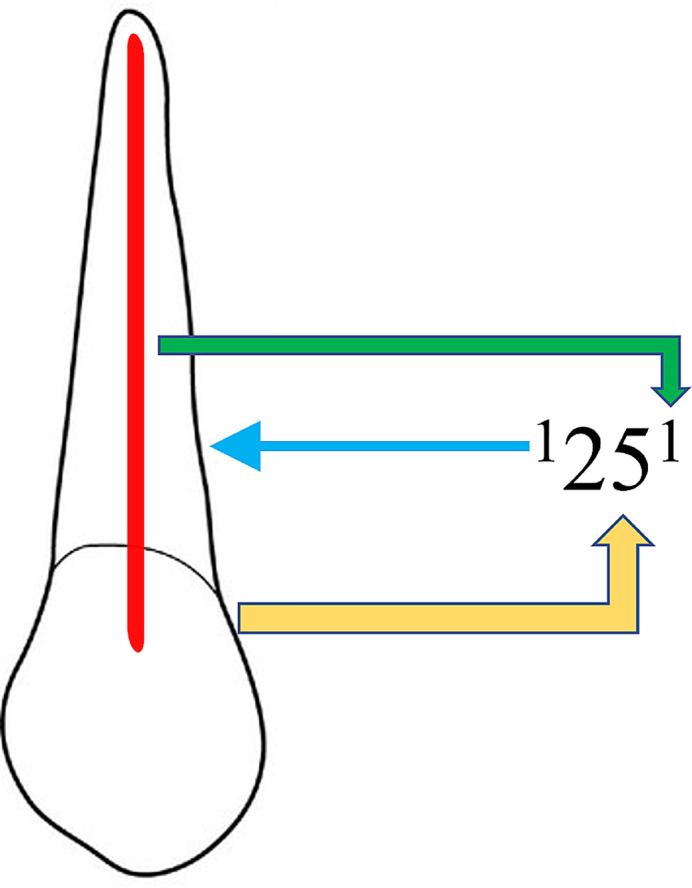
New classification system for root canal morphology of maxillary left second premolar classified using the new classification system, described as code 1251. The code consists of three components, the tooth number – Yellow color arrow, number of roots – blue color arrow and the root canal configuration – green color arrow. The number of roots is added as a superscript before the tooth number, so it is single root and tooth number (25). Description of root canal configuration is written as superscript after the tooth number on the course of the root canal starting from the orifices [O], passing through the canal [C], ending by the foramen [F], so it is single canal
Statistical analysis
Statistical analysis was performed using SPSS version 26 software. Descriptive statistics, including mean frequency and standard deviation, were calculated to summarize the data. The association between root canal morphology and age/gender was analyzed using the chi-square test or Fisher exact test, depending on the distribution of the data. Significance levels were set at p ≤ 0.05 to determine the statistical significance of the findings. Additionally, subgroup analyses were conducted to explore potential interactions between age, gender, and root canal morphology.
Results
The distribution of maxillary premolars according to Ahmed’s classification was examined. Table 1 presents the distribution of premolars based on the classification categories. For right maxillary 1st premolars, the majority belonged to 2MPM1 B1 L1 (39.03%) and 1MPM1 (2.81%) categories. Similarly, for right maxillary 2nd premolars, 2MPM1 B1 L1 (39.08%) and 1MPM1 (17.85%) were the most prevalent categories.
Table 1.
Distribution of maxillary premolars according to Ahmed’s classification
| Classification | Right Max 1st PM | Right Max 2nd PM | Left Max 1st PM |
Left Max 2nd PM | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| 1 MPM 1 | 11 | 2.81 | 70 | 17.85 | 8 | 2.03 | 74 | 18.8 |
| 2 MPM 1 B 1 L 1 | 154 | 39.03 | 45 | 11.48 | 154 | 39.08 | 45 | 11.42 |
| 3 MPM MB 1 DB 1 L 1 | 1 | 0.25 | 3 | 0.77 | 2 | 0.5 | 2 | 0.5 |
| 1 MPM 1–2−1–2−1–2 | 1 | 0.25 | 1 | 0.25 | 0 | 0 | 0 | 0 |
| 1 MPM 2−1−2−1 | 0 | 0 | 1 | 0.25 | 1 | 0.25 | 0 | 0 |
| 1 MPM 2−1 | 4 | 1.02 | 2 | 0.51 | 6 | 1.52 | 2 | 0.5 |
| 1 MPM 1–2−1 | 22 | 5.61 | 52 | 13.26 | 26 | 6.6 | 52 | 13.2 |
| 1 MPM 2−2 | 11 | 2.81 | 9 | 2.3 | 9 | 2.28 | 5 | 1.26 |
| 1 MPM 1–2 | 3 | 0.77 | 1 | 0.25 | 4 | 1.01 | 3 | 0.76 |
| 1 MPM 1–2−1–2 | 1 | 0.25 | 1 | 0.25 | 0 | 0 | 0 | 0 |
| 1 MPM 2−1−2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.25 |
| Total | 208 | 52.8 | 185 | 47.2 | 210 | 53.3 | 184 | 46.7 |
MPM- Maxillary Premolar
Table 2 displays the distribution of maxillary premolars based on the number of roots. The majority of premolars had two roots (73.33% for left maxillary 1st premolars, 24.45% for left maxillary 2nd premolars, 74.03% for right maxillary 1st premolars, and 24.32% for right maxillary 2nd premolars) (Figs. 2, 3 and 4).
Table 2.
Distribution of maxillary premolars according to number of roots
| Number of roots | Left Max 1st PM | Left Max 2nd PM | Right Max 1st PM | Right Max 2nd PM |
|---|---|---|---|---|
| One root | 54 | 137 | 53 | 137 |
| Two roots | 154 | 45 | 154 | 45 |
| Three roots | 2 | 2 | 1 | 3 |
| Total | 210 | 184 | 208 | 185 |
Max PM- Maxillary premolar
Fig. 2.

CBCT View (Sagittal and axial) of left maxillary second premolar showing the code 1MPM1
Fig. 3.

CBCT View (Sagittal and axial) maxillary first and second premolars showing the canal variations
Fig. 4.

CBCT View (Sagittal and axial) maxillary first and second premolars showing the canal variations in more than one root
Tables 3 and 4 present the distribution of left and right maxillary 1st and 2nd premolars, respectively, based on gender. In Table 3, significant gender differences were observed for the classification 1MPM1 (p = 0.515) and 1MPM1–2−1 (p = 0.010*) for both left maxillary 1st and 2nd premolars. The number of males and females for MPM1 in left maxillary 1st premolars was 121 and 88, respectively, while for 1MPM1 in left maxillary 2nd premolars, it was 111 and 72, respectively. Similarly, for 1MPM1–2−1 in left maxillary 1st premolars, the number of males and females was 3 and 3, respectively, whereas for left maxillary 2nd premolars, it was 30 and 21, respectively.
Table 3.
Distribution of left maxillary 1st and 2nd premolar concerning gender
| Classification | Left Max 1st PM | Left Max 2nd PM | ||||
|---|---|---|---|---|---|---|
| Male | Female | P-value | Male | Female | P-value | |
| 1MPM1 | 6 | 2 | 36 | 38 | ||
| 2MPM1 B1 L1 | 93 | 61 | 37 | 8 | ||
| 3MPMMB1DB1 L1 | 1 | 1 | 1 | 1 | ||
| 1MPM2-1 | 0 | 1 | 2 | 0 | ||
| 1MPM1-2-1 | 3 | 3 | 0.515 | 30 | 21 | 0.010* |
| 1MPM2-2 | 12 | 13 | 4 | 1 | ||
| 1MPM1-2 | 3 | 6 | 1 | 2 | ||
| 1MPM2-1-2 | 3 | 1 | 0 | 1 | ||
| Total | 122 | 88 | 112 | 72 | ||
*Significant value <0.05; Chi-square test, MPM and Max PM- Maxillary Premolar
Table 4.
Distribution of right maxillary 1st and 2nd premolar concerning gender
| Classification | Right Max 1st PM | Right Max 2nd PM | ||||
|---|---|---|---|---|---|---|
| Male | Female | P-value | Male | Female | P-value | |
| 1MPM1 | 5 | 6 | 34 | 36 | ||
| 2MPM1 B1 L1 | 100 | 54 | 38 | 8 | ||
| 3MPMMB1DB1 L1 | 0 | 1 | 2 | 1 | ||
| 1MPM1-2-1-2-1-2 | 1 | 0 | 0 | 1 | ||
| 1MPM 2-1-2-1 | 0 | 0 | 0 | 1 | ||
| 1MPM2-1 | 1 | 3 | 0.032* | 2 | 0 | 0.003* |
| 1MPM 1-2-1 | 10 | 12 | 33 | 18 | ||
| 1MPM2-2 | 2 | 9 | 5 | 4 | ||
| 1MPM1-2 | 2 | 1 | 1 | 0 | ||
| 1MPM 1-2-1-2 | 1 | 0 | 0 | 1 | ||
| Total | 122 | 86 | 115 | 70 | ||
*Significant value <0.05; Chi-square test, MPM and Max PM- Maxillary Premolar
Table 4 indicates significant gender differences for the classification MPM1 (p = 0.032*) and 1MPM1–2−1 (p = 0.003*) in the right maxillary 1st premolars. The number of males and females for 1MPM1 in the right maxillary 1st premolars was 122 and 84, respectively, while for 1MPM1 in the right maxillary 2nd premolars, it was 115 and 70, respectively. Additionally, the number of males and females for 1MPM1–2−1 in right maxillary 1st premolars was 10 and 11, respectively, whereas, for right maxillary 2nd premolars, it was 33 and 18, respectively.
Tables 5 and 6 demonstrate the distribution of left and right maxillary 1st and 2nd premolars, respectively, based on age groups. In Table 5, significant differences were observed for the classification 1MPM1 (p = 0.053) and 1MPM1–2−1 (p = 0.002*) in left maxillary 1st premolars. The number of premolars in each age group for 1MPM1 in left maxillary 1st premolars ranged from 1 to 7, whereas for 1MPM1–2−1, it ranged from 0 to 3. For left maxillary 2nd premolars, significant differences were observed for the classification 1MPM1 (p = 0.002*) and 1MPM1–2−1 (p = 0.002*). The number of premolars in each age group for 1MPM1 in left maxillary 2nd premolars ranged from 6 to 38, whereas for 1MPM1–2−1, it ranged from 4 to 23.
Table 5.
Distribution of left maxillary 1st and 2nd premolars concerning age
| Classification | Left Max 1st PM | Left Max 2nd PM | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | P-value | AGE | P-value | |||||||||||
| 10-20 | 21-30 | 31-40 | 41-50 | 51-60 | 60+ | 10-20 | 21-30 | 31-40 | 41-50 | 51-60 | 60+ | |||
| 1 MPM 1 | 1 | 3 | 3 | 0 | 1 | 0 | 13 | 23 | 16 | 9 | 7 | 5 | ||
| 2 MPM 1 B 1 L 1 | 17 | 41 | 47 | 20 | 14 | 15 | 5 | 16 | 14 | 4 | 3 | 3 | ||
| 3 MPM MB 1 DB 1 L 1 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | ||
| 1 MPM 2-1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | ||
| 1 MPM 1-2-1 | 0 | 1 | 2 | 0 | 2 | 1 | 0.053 | 2 | 13 | 13 | 11 | 9 | 4 | 0.002* |
| 1 MPM 2-2 | 3 | 7 | 5 | 5 | 3 | 3 | 0 | 3 | 1 | 0 | 1 | 1 | ||
| 1 MPM 1-2 | 0 | 3 | 1 | 1 | 1 | 3 | 0 | 0 | 1 | 2 | 0 | 0 | ||
| 1 MPM 2-1-2 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | ||
| Total | 21 | 60 | 59 | 26 | 22 | 22 | 20 | 56 | 48 | 27 | 20 | 13 | ||
*Significant value <0.05; Chi-square test, MPM and Max PM- Maxillary Premolar
Table 6.
Distribution of right maxillary 1st and 2nd premolars concerning age
| Classification | Right Max 1st PM | Right Max 2nd PM | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | P-value | AGE | P-value | |||||||||||
| 10-20 | 21-30 | 31-40 | 41-50 | 51-60 | 60+ | 10-20 | 21-30 | 31-40 | 41-50 | 51-60 | 60+ | |||
| 1 MPM 1 | 1 | 3 | 3 | 1 | 3 | 0 | 12 | 25 | 17 | 4 | 6 | 6 | ||
| 2 MPM 1 B 1 L 1 | 17 | 39 | 45 | 22 | 13 | 18 | 7 | 13 | 14 | 5 | 3 | 3 | ||
| 3 MPMMB 1 DB 1 L 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 1 | 0 | 0 | 0 | ||
| 1 MPM 1-2-1-2-1-2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | ||
| 1 MPM 2-1-2-1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | ||
| 1 MPM 2-1 | 0 | 1 | 1 | 0 | 2 | 0 | 0.055 | 0 | 0 | 1 | 1 | 0 | 0 | 0.002* |
| 1 MPM 1-2-1 | 3 | 7 | 8 | 1 | 0 | 3 | 1 | 15 | 12 | 7 | 7 | 10 | ||
| 1 MPM 2-2 | 0 | 4 | 2 | 1 | 2 | 2 | 0 | 3 | 3 | 0 | 0 | 3 | ||
| 1 MPM 1-2 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | ||
| 1 MPM 1-2-1-2 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | ||
| Total | 21 | 57 | 60 | 25 | 21 | 24 | 20 | 59 | 49 | 19 | 16 | 22 | ||
*Significant value <0.05; Chi-square test, MPM and Max PM - Maxillary Premolar
In Table 6, significant differences were observed for the classification 1MPM1 (p = 0.055) and MPM1 (p = 0.002*) in the right maxillary 1st and 2nd premolars, respectively. The number of premolars in each age group for 1MPM1 in the right maxillary 1st premolars ranged from 1 to 6, whereas for 1MPM1–2−1, it ranged from 0 to 15. For right maxillary 2nd premolars, significant differences were observed for the classification 1MPM1 (p = 0.002*) and 1MPM1–2−1 (p = 0.002*). The number of premolars in each age group for 1MPM1 in the right maxillary 2nd premolars ranged from 6 to 36, whereas for 1MPM1–2−1, it ranged from 3 to 15.
Discussion
The present study aimed to investigate the root canal morphology of maxillary premolars using cone-beam computed tomography (CBCT) imaging. By analyzing a large sample size of CBCT images, we sought to provide a comprehensive understanding of the complex and variable root canal configuration in maxillary premolars, considering factors such as gender and age.
As mentioned in the literature [11, 19], our findings revealed a diverse range of root canal configurations in maxillary premolars. Multiple canals, isthmuses, and accessory canals in these teeth pose a challenge to endodontic treatment, as it necessitates thorough exploration, disinfection, and meticulous instrumentation [20]. Recognizing such complex anatomy underscores the importance of employing advanced imaging techniques, such as CBCT, to accurately visualize and assess root canal morphology [21, 22].
In our study, age emerged as a significant factor influencing the root canal morphology of maxillary premolars. The categorization into different age groups allowed for a nuanced exploration of these variations, corroborating previous research [23–25]. The age-specific analysis revealed noteworthy trends in the prevalence of certain root canal configurations. For instance, in left maxillary 1st premolars, the marginal significance (p = 0.053) for 1MPM1 suggests a potential shift in root canal anatomy with increasing age. This finding prompts further investigation into the underlying reasons for such variations across age groups. Similarly, the significant difference (p = 0.002*) observed in 1MPM1-2-1 in both left and right maxillary 1st premolars indicates distinct patterns in root canal morphology among different age brackets. This finding raises questions about whether these differences are attributed to developmental changes, wear and tear, or other factors associated with aging. These age-related changes can be attributed to factors such as dentin deposition and secondary dentin formation, which may alter the shape and complexity of the root canal system over time. Therefore, endodontists should consider these age-related variations when planning and performing root canal procedures, particularly in older patients [26]. Younger age groups may exhibit features associated with incomplete root development and open apices, while older age groups may show signs of maturation, closure of apices, and increased calcification [27]. The correlations between age-related changes in root canal morphology and systemic conditions enhance the clinical context. Systemic factors, such as hormonal changes, metabolic disorders, or medication use, may influence dental development and impact root canal anatomy differently across age groups [28]. Practitioners should consider these age-related nuances during treatment planning and execution, adjusting their approaches to accommodate the potential variations in root canal anatomy. For example, younger patients may exhibit different anatomical features compared to older individuals, influencing decisions related to instrumentation and obturation techniques.
Furthermore, our study identified gender-based differences in root canal morphology. This finding aligns with Ahmed et al. [19], who reported similar gender differences in maxillary premolars. Their study revealed a higher prevalence of multiple canals in males than females, which supports our observations of significant gender variations in root canal morphology. However, it is worth noting that Ahmed et al. did not mention the specific classification code 1MPM1–2−1 in their study, making a direct comparison somewhat limited.
Likewise, Cleghorn et al. [11] found that the prevalence of multiple canals in maxillary first premolars ranged from 30 to 73%, a range consistent with our findings. Shi et al., while studying the Chinese population [23], also noted significant differences in the number of roots and gender in both maxillary first and second premolars.
In a study conducted by Mashyakhy et al. [29] in a Saudi population, highly statistically significant differences in canal configurations were observed between genders in maxillary teeth. Similarly, Martins et al. [30] reported a gender difference in the root canal morphology of the Portuguese population. However, it is essential to mention that some contrasting results were found in specific subpopulations. For instance, no significant difference in root canal morphology was noted in the Malaysian subpopulation [31] and the German subpopulation [32].
In summary, our study adds to the existing body of literature by providing further evidence of gender-related variations in root canal morphology, and it is in line with previous research in this field.
This study’s utilization of CBCT imaging provided valuable insights into the three-dimensional morphology of maxillary premolars. CBCT has emerged as a powerful diagnostic tool in endodontics, enabling the visualization of intricate root canal anatomy [33]. Accurately assessing root canal morphology facilitates precise treatment planning, guiding clinicians in determining the appropriate access, instrumentation, and obturation techniques [34]. The present study has several advantages, reinforcing its conclusions’ reliability and veracity. First and foremost, a large sample size was used in the study, with 500 cone-beam computed tomography (CBCT) images in total, 1230 maxillary premolars included. This large sample size improves the study’s statistical power and broadens the applicability of the results to the intended population.
The study employed qualified endodontists and observers calibrated to evaluate root canal morphology to achieve precise and reliable analysis. To determine the classification of root canal morphology, 50 CBCT images were examined as part of the calibration process. The research boosted the consistency and accuracy of the results by creating a smooth decision-making process that reduced the possibility of observer bias.
In the present study, a standardized classification scheme was used. This classification system offers a reliable and standardized method for classifying root canal morphology. The study’s findings may be easily compared and integrated with those of other research utilizing the same approach because it used a recognized classification system. Understanding root canal morphology in maxillary premolars is ultimately enhanced by this, making it easier for future research and enabling meta-analyses.
Additionally, the study compared its findings to pertinent literature, enabling a thorough interpretation of the data in light of earlier research. The study offers important insights into the heterogeneity of root canal morphology in maxillary premolars by comparing the consistency or divergence of results across different populations and studies. The scientific knowledge base is expanded, and this topic is better understood thanks to the comparative method.
Strengths of our study
One of the key strengths of our study is the large sample size, which enhances the statistical power and generalizability of our findings. Additionally, the utilization of cone-beam computed tomography (CBCT) imaging allowed for detailed three-dimensional analysis of root canal morphology, providing valuable insights into the complexity of maxillary premolars. Our rigorous calibration process, involving expert endodontists and observers, ensured the reliability and accuracy of our data collection and analysis. Furthermore, by considering age and gender variations, we were able to explore the influence of demographic factors on root canal anatomy, contributing to a more nuanced understanding of this topic.
Limitations
Despite these strengths, our study also has several limitations that warrant consideration. Firstly, the retrospective nature of the study may introduce selection bias and limit the generalizability of the findings. Additionally, the study focused on a specific population, which may limit its applicability to other ethnic groups or regions. Furthermore, the reliance on CBCT imaging, while providing detailed anatomical information, is subject to radiation exposure and cost constraints. Moreover, the inclusion and exclusion criteria applied in the study may have inadvertently excluded certain teeth or patient populations, potentially affecting the representativeness of the sample.
Future research endeavors should explore the relationship between root canal morphology and treatment outcomes in maxillary premolars to enhance our knowledge further. Long-term follow-up studies can provide valuable insights into the success rates and potential complications associated with different root canal configurations. Furthermore, advancements in imaging modalities and treatment techniques, such as guided endodontics and regenerative approaches, hold promise for overcoming the challenges posed by complex root canal anatomy.
Conclusion
This study provides novel insights into the root canal anatomy of maxillary premolars within the Saudi population, addressing a notable gap in the literature specific to this demographic. Through CBCT imaging and analysis of large sample sizes, the complex and diverse nature of root canal morphology in these teeth among Saudi individuals is elucidated. The findings underscore the importance of CBCT imaging in precise treatment planning and decision-making tailored to the Saudi population. Consideration of age and gender-related variations further enhances understanding and aids in personalized endodontic interventions within this demographic. Moving forward, these findings inform clinical practice within the Saudi community, emphasizing the need for customized approaches to optimize treatment outcomes.
Acknowledgements
Not applicable.
Author contributions
Conception and design of the study: MIK, and TYN. Acquisition of data: AZ and SJ. Analysis and interpretation of data: RB and AHA. Drafting the article: MIK, RB, AHA and SJ. Revising it critically for important intellectual content: MIK, AZ, HAA, MAA and TYN. All authors approved the final submitted version.
Funding
The current paper did not receive any external funding.
Data availability
All data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declarations
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Ethics approval
Ethical approval for this retrospective study was obtained from the Local Committee of Bioethics for Research at the Dentistry College, King Abdul-Aziz University, with Ethical Approval No. 025-02-22. Informed consent was obtained from the Committee of Bioethics for Research, College of Dentistry, King Abdul-Aziz University, Jeddah, Saudi Arabia, considering the study’s retrospective nature. Before any investigation or treatment, the patients signed a general consent form, allowing the use of findings in future studies and publications without revealing personal information. The informed consent was obtained from all subjects and/or their legal guardian(s).
Conflict of interest
All the authors declare that they have no known conflicts of interest in terms of competing financial interests or personal relationships that could have an influence or are relevant to the work reported in this paper.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Schilder H. Cleaning and shaping the root canal. Dental Clin N Am. 1974;18(2):269–96. doi: 10.1016/S0011-8532(22)00677-2. [DOI] [PubMed] [Google Scholar]
- 2.Karobari MI, et al. Application of two systems to classify the root and canal morphology in the human dentition: a national survey in India. Journal of Dental Education; 2023. [DOI] [PubMed]
- 3.Vertucci FJ. Root canal anatomy of the human permanent teeth Oral surgery, oral medicine, oral pathology, 1984. 58(5): pp. 589–599. [DOI] [PubMed]
- 4.Karobari MI, et al. Evaluation of root and canal morphology of mandibular premolar amongst Saudi subpopulation using the new system of classification: a CBCT study. BMC Oral Health. 2023;23(1):1–11. doi: 10.1186/s12903-023-03002-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Martins JN, et al. Worldwide Assessment of the Root and Root Canal characteristics of Maxillary Premolars–A Multi-center Cone-Beam Computed Tomography cross-sectional study with Meta-analysis. J Endod. 2024;50(1):31–54. doi: 10.1016/j.joen.2023.10.009. [DOI] [PubMed] [Google Scholar]
- 6.Ahmed HMA. A critical analysis of laboratory and clinical research methods to study root and canal anatomy. Int Endod J. 2022;55:229–80. doi: 10.1111/iej.13702. [DOI] [PubMed] [Google Scholar]
- 7.Mashyakhy M. Anatomical evaluation of maxillary premolars in a Saudi population: an in vivo cone-beam computed tomography study. J Contemp Dent Pract. 2021;22(3):284–9. doi: 10.5005/jp-journals-10024-3070. [DOI] [PubMed] [Google Scholar]
- 8.Merhej M-J et al. Root and Root Canal Morphology of Premolars in a Sample of the Lebanese Population: Clinical Considerations 2022.
- 9.Karobari MI et al. Assessment of Root Canal Morphology of Maxillary Premolars: A CBCT Study Exploring Age and Gender Variations 2023. [DOI] [PMC free article] [PubMed]
- 10.Pécora JD, et al. Internal anatomy, direction and number of roots and size of human mandibular canines. Braz Dent J. 1993;4(1):53–7. [PubMed] [Google Scholar]
- 11.Cleghorn BM, et al. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod. 2006;32(9):813–21. doi: 10.1016/j.joen.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 12.Karobari MI, et al. Root and root canal morphology classification systems. Int J Dent. 2021;2021:1–6. doi: 10.1155/2021/6682189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tian YY, et al. Root and canal morphology of maxillary first premolars in a Chinese subpopulation evaluated using cone-beam computed tomography. Int Endod J. 2012;45(11):996–1003. doi: 10.1111/j.1365-2591.2012.02059.x. [DOI] [PubMed] [Google Scholar]
- 14.Karobari MI, et al. Roots and root canals characterization of permanent mandibular premolars analyzed using the cone beam and micro computed tomography—a systematic review and metanalysis. J Clin Med. 2023;12(6):2183. doi: 10.3390/jcm12062183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Iqbal A, et al. Evaluation of root canal morphology in permanent maxillary and mandibular anterior teeth in Saudi subpopulation using two classification systems: a CBCT study. BMC Oral Health. 2022;22(1):171. doi: 10.1186/s12903-022-02187-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Karobari MI, et al. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: a CBCT clinical study. Australian Endodontic J. 2021;47(2):202–16. doi: 10.1111/aej.12454. [DOI] [PubMed] [Google Scholar]
- 17.Versiani MA, et al. Root and root canal morphology of four-rooted maxillary second molars: a micro–computed tomography study. J Endod. 2012;38(7):977–82. doi: 10.1016/j.joen.2012.03.026. [DOI] [PubMed] [Google Scholar]
- 18.Neelakantan P, et al. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010;36(10):1622–7. doi: 10.1016/j.joen.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 19.Ahmad IA, et al. Root and root canal morphology of maxillary first premolars: a literature review and clinical considerations. J Endod. 2016;42(6):861–72. doi: 10.1016/j.joen.2016.02.017. [DOI] [PubMed] [Google Scholar]
- 20.Dastgerdi AC, et al. Isthmuses, accessory canals, and the direction of root curvature in permanent mandibular first molars: an in vivo computed tomography study. Volume 45. Restorative Dentistry & Endodontics; 2020. 1. [DOI] [PMC free article] [PubMed]
- 21.Scarfe WC et al. Use of cone beam computed tomography in endodontics International journal of dentistry, 2009. 2009. [DOI] [PMC free article] [PubMed]
- 22.Karobari MI, et al. Root and root canal configuration characterization using microcomputed tomography: a systematic review. J Clin Med. 2022;11(9):2287. doi: 10.3390/jcm11092287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shi Z-Y, et al. Root canal morphology of maxillary premolars among the elderly. Chin Med J. 2017;130(24):2999–3000. doi: 10.4103/0366-6999.220295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hu R, et al. Aging changes of the root canal morphology in maxillary first premolars observed by cone-beam computerized tomography. Zhonghua Kou Qiang Yi Xue Za Zhi = Zhonghua Kouqiang Yixue Zazhi = Chin J Stomatology. 2016;51(4):224–9. doi: 10.3760/cma.j.issn.1002-0098.2016.04.008. [DOI] [PubMed] [Google Scholar]
- 25.Thomas R, et al. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J. 1993;26(5):257–67. doi: 10.1111/j.1365-2591.1993.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 26.Mashyakhy M, et al. Root and root canal morphology differences between genders: a comprehensive in-vivo CBCT study in a Saudi population. Acta Stomatol Croatica. 2019;53(3):213. doi: 10.15644/asc53/3/5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nuni E, et al. Endodontic Treatment for Young Permanent Teeth, in contemporary endodontics for children and adolescents. Springer; 2023. pp. 281–321.
- 28.Gilroy FG. Perceptions of general health and root canal treatment in New Zealand general dental practice. University of Otago; 2020.
- 29.Martins JN, et al. Gender influence on the number of roots and root canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int. 2018;49(2):103–11. doi: 10.3290/j.qi.a39508. [DOI] [PubMed] [Google Scholar]
- 30.Pan JYY, et al. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health. 2019;19(1):1–15. doi: 10.1186/s12903-019-0710-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bürklein S, et al. Evaluation of the root canal anatomy of maxillary and mandibular premolars in a selected German population using cone-beam computed tomographic data. J Endod. 2017;43(9):1448–52. doi: 10.1016/j.joen.2017.03.044. [DOI] [PubMed] [Google Scholar]
- 32.Yoza T, et al. Cone-beam computed tomography observation of maxillary first premolar canal shapes. Anat Cell Biology. 2021;54(4):424–30. doi: 10.5115/acb.21.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kulinkovych-Levchuk K, et al. Guided endodontics: a Literature Review. Int J Environ Res Public Health. 2022;19(21):13900. doi: 10.3390/ijerph192113900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Karobari MI, et al. Micro computed tomography (Micro-CT) characterization of root and root canal morphology of mandibular first premolars: a systematic review and meta-analysis. BMC Oral Health. 2024;24(1):1. doi: 10.1186/s12903-023-03624-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data supporting the findings of this study are available from the corresponding author upon reasonable request.