

Abstract
Background
Telemedicine, a method of healthcare service delivery bridging geographic distances between patients and providers, has gained prominence. This modality is particularly advantageous for outpatient consultations, addressing inherent barriers of travel time and cost.
Objective
We aim to describe economical outcomes towards the implementation of a multidisciplinary telemedicine service in a high-complexity hospital in Latin America, from the perspective of patients.
Design
A cross-sectional study was conducted, analysing the institutional data obtained over a period of 9 months, between April 2020 and December 2020.
Setting
A high-complexity teaching hospital located in Cali, Colombia.
Participants
Individuals who received care via telemedicine. The population was categorised into three groups based on their place of residence: Cali, Valle del Cauca excluding Cali and Outside of Valle del Cauca.
Outcome measures
Travel distance, time, fuel and public round-trip cost savings, and potential loss of productivity were estimated from the patient’s perspective.
Results
A total of 62 258 teleconsultations were analysed. Telemedicine led to a total distance savings of 4 514 903 km, and 132 886 hours. The estimated cost savings were US$680 822 for private transportation and US$1 087 821 for public transportation. Patients in the Outside of Valle del Cauca group experienced an estimated average time savings of 21.2 hours, translating to an average fuel savings of US$149.02 or an average savings of US$156.62 in public transportation costs. Areas with exclusive air access achieved a mean cost savings of US$362.9 per teleconsultation, specifically related to transportation costs.
Conclusion
Telemedicine emerges as a powerful tool for achieving substantial travel savings for patients, especially in regions confronting geographical and socioeconomic obstacles. These findings underscore the potential of telemedicine to bridge healthcare accessibility gaps in low-income and middle-income countries, calling for further investment and expansion of telemedicine services in such areas.
Keywords: Telemedicine, Latin America, HEALTH ECONOMICS
STRENGTHS AND LIMITATIONS OF THIS STUDY.
This study originates from a database rich in georeferenced information for each patient.
The study uses actual costs of public and intermunicipal transportation for each individual in the dataset.
Individual preferences for public or private transportation were not accounted for in this study.
Productivity loss estimation did not consider the employment status of participants.
The measured calculations are indirect since there is no validated instrument available to measure individuals’ expenditure costs.
Introduction
In the last decade, there have been significant technological advances in healthcare. Telemedicine is a modality of healthcare services delivery, where patients and providers are separated by distance. Telehealth uses information and communication technology for the exchange of information, related to the diagnosis and treatment of diseases and injuries, and to strengthen research and continuing education of health professionals.1 This care model can be especially helpful for outpatient consultations, where barriers related to travel time and cost are constantly inherent for patients.2 3
Positive results regarding patient satisfaction and outcomes of telemedicine care have been reported in the literature.4 This tool has reduced costs in the health system of several countries.5 6 From the patient’s perspective, despite its inherent limitations, telemedicine has been well-received and has generated excellent patient satisfaction.6 7 Telemedicine led savings for patients and their companions, mainly those related to care, including travel time, distance and costs.8–10 However, most of the studies about patient savings related to telemedicine use had been conducted in high-income countries, providing information on the teleconsultation offered for a single state, locality or city.
The development and enhancement of telemedicine in Colombia have been under discussion since 2010. However, it was not until 2020, during the COVID-19 pandemic’s public health emergency, that the government began to actively promote its utilisation; this was driven by the enforcement of mandatory lockdown measures and the imperative to ensure continuous medical care. In this circumstance, Fundación Valle del Lili (FVL), a highly complex Colombian teaching hospital, quickly introduced a telemedicine service. Implementing this service encountered significant challenges, the availability of resources and the cultural resistance exhibited by patients towards this modality of attention.11 Our aim was to estimate the hypothetical transportation-related savings in time, distance and costs assumed for the patients due to outpatient care by the FVL telemedicine programme during April–December 2020.
Methods
Design and population
A retrospective study focused on the time and transportation cost savings experienced by the patients as a result of telemedicine interventions. Our study included patient who resided in Colombia and received outpatient teleconsultation through the FVL Telemedicine programme between April and December 2020. We excluded patients residing in countries other than Colombia, as well as those lacking residence information or address details. The study population was categorised based on their place of residence into the following three groups (figure 1):
Figure 1.

Study area map with locations of patient residences. Grey-shaded area refers to the region of Valle del Cauca. Black point indicates Fundación Valle del Lili (FVL). Grey points represent areas of teleconsultation in Cali, Valle del Cauca excluding Cali and areas outside of Valle del Cauca.
Cali: people who live in the city of Cali, Valle del Cauca.
Valle del Cauca excluding Cali: people who live in other cities in Valle del Cauca, different to Cali.
Outside of Valle del Cauca: people who live in other departments, different to Valle del Cauca.
Overview of FVL Telemedicine Program
In Colombia, hospitals are categorised into four levels based on their degree of specialisation, subject to evaluation and approval by the national government. Level I hospitals primarily have low-complexity technology and provide care by general practitioners, offering outpatient consultations, hospitalisation, emergency services and essential diagnostic and treatment support. Level II hospitals expand their services to include gynaecology and obstetrics, surgery, internal medicine and paediatrics, incorporating technology of moderate complexity. Level III hospitals feature subspecialised personnel, adult and neonatal intensive care units, and advanced technology. At the highest level of care, level IV hospitals cater to patients in critical condition, offering highly complex subspecialties and the potential for organ transplantation.12 Moreover, it is noteworthy that the three largest cities in Colombia, Bogotá, Medellín and Cali, concentrate the majority of levels III and IV hospitals in the country, providing comprehensive medical services to the surrounding population. Additionally, Colombia boasts only 16 government-accredited teaching hospitals, representing hubs of specialist concentration. Access to specialist care in Colombia’s healthcare system requires authorisation from the patient’s healthcare plan, as patients cannot freely choose their own specialist. The patient healthcare plan assigns the care location based on contractual agreements, with telemedicine services typically included within the health plan. Conversely, smaller cities and towns may house levels 1 and 2 hospitals, offering care of basic to moderate complexity.12
FVL is a private, non-profit, high-complexity hospital located in Santiago de Cali, serving as a referral centre in the southwest region of Colombia. In 2019, the institution provided 511 124 outpatient visits, 75 890 emergency room visits and 26 878 inpatient stays. FVL’s telemedicine service, promoted and strengthened in March 2020 in response to the declaration of a health emergency by COVID-19 by the Ministry of Health, ensures the continuity of ambulatory health services throughout the Colombian territory. This initiative aims to address accessibility challenges, particularly in rural regions, by extending high-level medical services to remote areas. Through a robust referral and counter-referral mechanism, eligible patients requiring outpatient or home-based management can access specialised consultations, facilitating consultation scheduling and ensuring necessary care irrespective of geographic location.
FVL’s telemedicine service facilitates outpatient care across 64 medical specialties, employing an interactive modality that establishes remote communication between patients and healthcare professionals through real-time video calls. FVL’s telemedicine service is meticulously organised to ensure seamless access to outpatient care for patients. The process begins with appointment scheduling via telephone, available from Monday to Friday between 07:00 and 17:00, and on Saturdays from 08:00 to 13:00. Patients are carefully guided through administrative procedures, supplemented by instructional emails detailing telemedicine processes. Appointment confirmations are diligently conducted 24 hours in advance by verifying the submission of requisite documents to the designated email address. Teleconsultations and real-time video calls are facilitated through the Microsoft Teams platform. Patient data are recorded in the Enterprise Resource Planning systems of the hospital (SAP-IS-H Software), which host the electronic medical record. Following the consultation, a PDF containing consultation details, medical directives and prescriptions is dispatched to the patient’s email address. Patients who have difficulty due to low technology literacy or cognitive issues are assisted by the appointment agent during the booking process. Additionally, the receptionist provides support during the teleconsultation setup, including guidance on using the application for initiating the call.
Outcome measures
The following outcome measures were taken into consideration:
Travel distance savings: the distance in kilometre of round trip that the patient would have travelled for an in-person consultation at the FVL.
-
Travel time savings: the time in hours of round trip that the patient would have wasted for an in-person consultation at the FVL; it represents the patient work time loss due to the travel for an in-person consultation.
Measurements of car transportation were performed using Google Maps, taking the main FVL centre as the destination and the patient’s place of residence as the origin. The patient’s home address was defined by the address (for Cali residents) or the registered municipality of residence in the electronic medical record system. The car transport option and the quickest route were selected. The estimated distance and travel time were doubled to encompass the round-trip travel to and from the FVL.
-
Travel cost savings: the expenses related to round trip that the patient would have spent for an in-person consultation at the FVL. For all cases, two modes of transportation were considered: (1) private transportation, for which round-trip fuel expenses were calculated for; and (2) public transportation, for which taxi costs (Cali group) or intermunicipal bus costs (Valle del Cauca and Colombia groups) were calculated based on 2020 fare rates.
Fuel cost calculation: we took as a reference the cost per gallon of fuel reported by the Ministry of Mines and Energy for the year 2020 that was $8268 COP (US$2.24); and an average consumption of 40 km travelled per gallon
Calculation of public transportation cost savings: to calculate the cost public transportation for the population living in Cali, we considered the cab fare reported by the Cali Municipal Hall for the year 2020, which was $84 COP for each 80 m travelled. For residents in other areas of Valle del Cauca and Colombia, we searched on the virtual platforms of the country’s public transportation terminals to determine the fare cost of intermunicipal bus travel from the different localities to the city of Cali.
It should be highlighted that for the municipalities where river transportation is necessary, the travel cost and time required for each municipality were consulted, in addition to the cost and time of land transportation. For the municipalities that do not have land access, estimates were made of the airfare costs; these were excluded in the calculations of distance and time savings.
-
Potential loss of productivity: it pertains to the value of work time that the patient would have lost due to the round-trip travel required for in-person consultations.
Calculation of the potential loss of productivity: in Colombia, the legal minimum wage in force for the year 2020 was $877 803 COP (US$640.31), the workday corresponds to 48 hours/week, which is adjusted to 8 hours/day. The value of 1 hour worked was $3657 COP (US$2.67). With the above, the value that the patient would have lost due to lost work time secondary to the round trip to attend an in-person consultation was calculated
All costs were calculated with the purchasing power parity exchange rate of 1370.9 COP per USD as per CCEMG–EPPI Centre Cost Converter’ (v.1.7 last update: January 2024) (https://eppi.ioe.ac.uk/costconversion/) designed to facilitate international comparison of costs.13
To estimate distance per patient per trip for patients outside the city of Cali but with land access to the city we used the distance between the centre of the town and the exact address at FVL using available free software. For patients without land access, distance was not computed. For patients in the city of Cali, an exact street address to street address estimation was done with the help of specialised software that takes into account traffic and real routes. This however was costly to do for the 19 630 patients, so we estimated a sample of 753 using the formula for a minimum sample size for estimating a population mean with 95% level of confidence (parameter=1.96), a SD of 7 km and a marging of error (E) of 0.5 km. This calculation did not correct for the finite population correction factor as the population size was large relative to the sample size An extra 8% of patients were added to complete a sample of 814, allowed by the budget allocated to this task, increasing precision and accuracy. This resulted in a total of 1708 teleconsultations in the selected sample, indicating that a single individual may have undergone multiple consultations and follow-up appointments throughout the study period. These consultations represented 3.9% of the 44 182 teleconsultations conducted in this group. As a result, calculations for the total savings in this group were later extrapolated by multiplying the value obtained in the sample by 25.87.
Patient and public involvement
None.
Results
A total of 296 170 outpatient care consultations were made from April to December 2020. Among these, 152 consultations were excluded due to patients residing outside of Colombia. Consequently, 296 018 consultations were included, out of which 62 258 (21.03%) were conducted via telemedicine, involving to 27 948 individuals (online supplemental table 1). The median age of the population was 41 years (IQR 21–61), the majority were female (62.95%) and the median of teleconsultations per person was 1 (IQR 1–2) (table 1). Further details regarding the distribution of the number of teleconsultations per patient can be observed in (figure 2). Telemedicine services were primarily provided by psychiatry (8891, 14.28%), endocrinology (6088, 9.78%) and psychology (4603, 7.39%).
Table 1.
Sociodemographic characteristics of the patients attended via telemedicine, between April and December 2020
| Variable | Total | Cali | Valle del Cauca excluding Cali | Outside of Valle del Cauca |
| Age, median (IQR) | 41 (21–61) | 41 (22–61) | 42 (19–61) | 41 (17–60.5) |
| Sex | ||||
| Female | 17 594 (62.95) | 12 462 (63.48) | 3573 (62.65) | 1552 (59.58) |
| Male | 10 354 (37.05) | 7168 (36.52) | 2130 (37.35) | 1053 (40.42) |
| Number of teleconsultations per patient | ||||
| 1–2 | 22 136 (79.23) | 15 574 (79.34) | 4499 (78.89) | 2063 (79.19) |
| 3–5 | 4100 (14.68) | 2817 (14.35) | 870 (15.26) | 413 (15.85) |
| 6–10 | 1078 (3.86) | 783 (3.99) | 198 (3.47) | 97 (3.72) |
| >10 | 624 (2.23) | 456 (2.32) | 136 (2.38) | 32 (1.23) |
Figure 2.
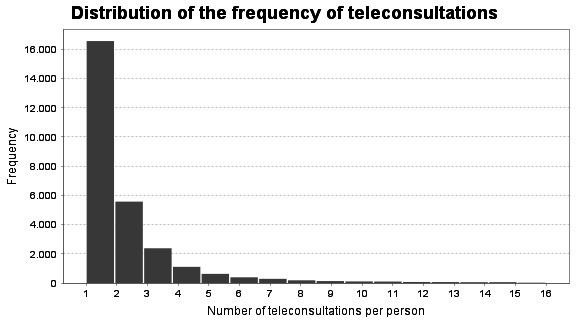
Distribution of the frequency of teleconsultations per person.
bmjopen-2024-084447supp001.pdf (34.1KB, pdf)
Total travel savings in terms of distance amounted to 4 514 903 km, and in terms of time, it reached 132 886 hours. The estimated travel cost savings were US$1 035 336 for private transportation (combining fuel cost savings and potential productivity gains) and US$1 442 335 for public transportation (cost of public transportation saved and potential productivity gains). The largest savings were in the rest of Colombia group, which are those people living in departments of Colombia other than Valle del Cauca. Table 2 shows the total and average savings per teleconsultation for each group. Furthermore, it was estimated that individuals residing in areas where access required air travel, could achieve savings of up to US$134 USD (SD 131.17) per teleconsultation.
Table 2.
Distance, time, fuel and public transportation savings observed by telemedicine consultation, between April and December 2020
| Variable | Total n=62 258 |
Cali n=44 182 |
Valle del Cauca excluding Cali n=12 707 |
Outside of Valle del Cauca n=5369 |
| Number of patients attended by telemedicine | 27 948 | 19 630 | 5703 | 2615 |
| Round-trip distance saved (km) | ||||
| Total | 4 514 903 | 644 758 | 1 295 538 | 2 574 607 |
| Mean (SD) | 72.55 (190) | 14.60 (9.44) | 101.95 (82.88) | 481.15 (454.02) |
| Median (IQR) | 20.80 (8.6–33.4) | 11.60 (6–23.6) | 76.40 (30.40–149) | 328 (258–750) |
| Round-trip time saved (hours) | ||||
| Total | 132 886 | 43 461 | 34 127 | 55 298 |
| Mean (SD) | 1.80 (7.02) | 0.98 (0.35) | 2.69 (1.43) | 10.33 (22.11) |
| Median (IQR) | 0.93 (0.43–1.27) | 0.90 (0.67–1.27) | 2.40 (1.33–3.17) | 6.73 (5.63–17.0) |
| Potential loss of productivity (USD) | ||||
| Total | 354 514 | 115 963 | 91 049 | 147 533 |
| Mean (SD) | 5.70 (18.73) | 2.62 (0.92) | 7.17 (3.82) | 27.6 (59.0) |
| Median (IQR) | 3.39 (2.04–4.26) | 2.40 (1.78–3.38) | 6.40 (3.56–8.45) | 18.0 (15.0–45.4) |
| Total fuel cost saved (USD) | ||||
| Total | 680 822 | 97 294 | 195 337 | 388 191 |
| Mean (SD) | 10.94 (28.64) | 2.20 (1.42) | 15.37 (12.50) | 72.5 (68.5) |
| Median (IQR) | 3.15 (1.30–5.05) | 1.75 (0.90–3.56) | 11.52 (4.58–22.47) | 49.5 (38.9–113.1) |
| Total cost of public transportation saved* (USD) | ||||
| Total | 1 087 821 | 494 237 | 185 582 | 408 002 |
| Mean (SD) | 17.48 (29.69) | 11.19 (7.23) | 14.60 (13.81) | 76.2 (74.6) |
| Median (IQR) | 8.88 (5.84–19.76) | 8.88 (4.60–18.08) | 7.29 (5.84–21.25) | 43.8 (40.8–109.4) |
| Saved transportation costs for municipalities with exclusively air income (USD)* | ||||
| Total | NA | NA | NA | 6170 |
| Mean (SD) | NA | NA | NA | 362.92 (356.05) |
| Median (IQR) | NA | NA | NA | 265.51 (265.51–496.03) |
*Refers to teleconsultations from people living in areas with no land access: Guapi (Cauca), Timbiquí (Cauca), Leticia (Amazonas) and San Andres (San Andres y Providencia).
NA, not apply.
The mean number of teleconsultations per patient was 2.10 (SD2.54) in Cali, 2.23 (SD 3.14) in Valle del Cauca excluding Cali and 2.05 (SD 2.28) for the Outside of Valle del Cauca group. The estimated mean cost savings for private transportation round trip per patient was US$10.13 in Cali, US$66.79 in Valle del Cauca excluding Cali and US$205.65 in outside of Valle del Cauca; and mean cost savings for public transportation expenses per patient was US$28.98 in Cali, US$50.22 in Valle del Cauca excluding Cali and US$213.25 in outside of Valle del Cauca. In addition, the transportation cost savings for individuals residing in areas with exclusive air access amounted to US$658.52, with a SD of US$392.49 (table 3).
Table 3.
Distance, time, fuel and public transportation per patient (all visits), between April and December 2020
| Variable | Cali n=19 630 n=814 |
Valle del Cauca excluding Cali n=5703 |
Outside of Valle del Cauca n=2615 |
| Teleconsultations per patient, mean (SD) | 2.10 (2.54) | 2.23 (3.14) | 2.05 (2.28) |
| Distance saved per patient (km), mean (SD) | 30.64 (52.80) | 227.17 (398.38) | 988.33 (1556.41) |
| Time saved per patients (hours), mean (SD) | 2.06 (2.90) | 5.98 (9.26) | 21.23 (51.47) |
| Potential loss of productivity (USD), mean (SD) | 5.51 (7.75) | 34.25 (60.7 | 56.63 (137.33) |
| Fuel cost saved per patient (USD), mean (SD) | 4.62 (7.96) | 32.54 (65.51) | 149.02 (234.67) |
| Cost of public transportation saved* (USD), mean (SD) | 23.47 (40.44) | 15.97 (24.70) | 156.62 (251.04) |
| Saved transportation costs for municipalities with exclusively air income (USD),* mean (SD) | NA | NA | 658.52 (392.49) |
*Refers to teleconsultations from people living in areas with no land access: Guapi (Cauca), Timbiquí (Cauca), Leticia (Amazonas) and San Andres (San Andres y Providencia).
NA, not apply.
Discussion
In low-income and middle-income countries, the population at the base of the socioeconomic pyramid bears a disproportionately high burden of disease, often facing limited access to health services due to lower purchasing power and residence in underserved areas. In such contexts, there is an urgent need to identify innovative short, medium and long terms to achieve effective universal health coverage, giving special strength to programmes that allow access in the most remote and vulnerable areas.14 15 Strengthening telehealth systems has the potential to improve health and socioeconomic status of different population groups. Extending healthcare services to these remote areas through telemedicine helps bridge this gap and facilitates substantial reductions in both time and distance.16–19 In Colombia, 7.2% of the population lives in rural areas,20 with significant challenges and obstacles when accessing healthcare services, particularly specialised medical care.15
In 2020, as the COVID-19 pandemic spread worldwide, world poverty increased, and poverty induced by COVID-19.21 Colombia was significantly affected by this issue, with a noticeable deterioration in its economic growth indicators. In 2020, the pandemic led to a 6.8% decline in Colombia’s economy (gross domestic product), contributing to an increase in the national unemployment rate by at least 8 percentage points, resulting in an average rate of 15.9, a 5.4 percentage points rise from the previous year.22 23 Furthermore, the proportion of informal employment increased from 45% to 49%.24 Thus, savings achieved by the programme were very timely in the midst of the worst economic year in Colombian history. The introduction of telemedicine led to average potential loss of productivity savings of US$5.51 and US$34.25 per patient for the population of Cali and Valle del Cauca, equivalent to 26% and 75% of a full day’s salary, respectively. For the population of Colombia, US$56.63 was saved per patient, representing 9% of the minimum monthly salary.
Transportation cost is a determining factor in access to healthcare, especially for those living in rural areas not having a tertiary or complex centre nearby that can provide services by medical specialties.25 However, the need for more training in the use of technologies and the difficulties in acquiring technology that allows remote connection limit the implementation of telemedicine in these areas.6 26 In our study, the telemedicine programme succeeded in extending its reach to remote locations facing geographical challenges. These areas are accessible solely by air or sea. Examples include municipalities such as Guapi, Timbiquí, Leticia and San Andres Island. Enhancing telecommunication networks in these regions could yield substantial savings in time, distance and travel expenses for their residents.27 For people living in those municipalities, savings in transportation costs estimated per patient exceeded the 2020 monthly minimum wage.
Significant savings related to transportation and fuel expenses have been reported. These costs vary widely; studies have reported savings ranging from US$4.66 to US$150 per teleconsultation.4 28 Other studies have reported saved costs that encompass fuel expenses, insurance and maintenance, resulting in higher per-person savings. Few studies have addressed costs related to public transportation; given the importance of public transportation in Colombia, especially between and within cities, this variable was key for a more realistic measurement.29 When comparing the average public transportation expenses saved for the Cali, Valle del Cauca and rest of Colombia locations to the legal monthly minimum salary in Colombia for year 2020, it represents 3.67%, 5.08% and 24.19%, respectively, for the average patient.
Limitations of the current study include the retrospective approach to data collection, which limited the depth of analysis possible. Prospective data collection would have allowed for a more comprehensive examination, including factors such as work absenteeism, wait times, appointment duration and associated costs. In addition, the absence of provider expenditures in the cost-effectiveness (CE) assessment of telemedicine represents a significant gap. On the other hand, the Colombian healthcare system fully covers diagnostic and treatment services, which may mitigate the cost impact on patients or hospitals. However, the study did not measure these consequences and costs, which is a limitation. Additionally, the potential loss of productivity particularly affects the adult population aged between 21 and 61 years. The retirement age in Colombia for women is 57 years and for men is 62 years. Within the scope of the study, this constitutes a limitation as it was not measured.
The study also overlooked critical factors like internet usage and telecommunications connectivity, impacting the assessment of cost savings achieved through telemedicine adoption. Failure to consider participants’ transportation mode and employment status hindered insights into socioeconomic dynamics influencing telemedicine utilisation. Methodologically, the indirect calculation of expenditures introduced ambiguity, compounded by the absence of a validated instrument for precise measurement. Our objective in this paper was measuring savings using TM in comparison to a regular visit by the patient to our location; we did not seek a full economic evaluation which will include a CE study. The CE literature has shown that from a health systems perspective telemedicine programmes remain cost effective, but from a societal perspective there is a gap, and we leave a full economic evaluation for further research.
Future implications
The results encourage developing public policies and strengthening strategies incorporating digital health and telemedicine in Latin America’s countries. Our experience shows results aimed at reducing indirect patient costs related to providing health services and facilitating care by multiple specialties through teleconsultation.
Conclusion
Telemedicine brings to patients a significant travel savings, both in terms of time, distance, cost and potential loss of productivity; particularly in regions facing geographical and socioeconomic challenges. These findings emphasise the potential of telemedicine to bridge healthcare accessibility gaps in middle-income countries and the need to further develop and expand telemedicine services in such areas.
Supplementary Material
Acknowledgments
We thank to the Fundación Valle del Lili, especially the department of cost and budget for providing and supporting this current research.
Footnotes
Contributors: SIP and MFE designed and supervised the study. JJT and JA contributed to data collection. SIP, JJT, EEP-Z and LL-P contributed data analysis. SIP, MFE, EEP-Z, LL-P and JA contributed to literature review. EEP-Z, LL-P, JA, SIP and MFE contributed to drafting the manuscript. All authors read drafts of the manuscript and approved the final version. MFE is responsible for the overall content as the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer: The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author [MFE], upon reasonable request.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
This study was conducted according to the Declaration of Helsinki guidelines; and was classified as a risk-free study according to resolution No. 008430 of 1993, article 11, numeral A of the Ministry of Health and Social Protection of Colombia. The institutional ethics committee reviewed and approved the protocol (Protocol No. 1742; IRB/EC No. 090–2021, Act No. 06-2021). This study did not require intervention or intentional modification of the biological, physiological, psychological or social variables of the participants. Therefore, no informed consent was necessary.
References
- 1. WHO-ITU global standard for accessibility of telehealth services . World health organization, international telecommunication union en Geneva. 2022. Available: https://www.who.int/publications-detail-redirect/9789240050464
- 2. Bynum AB, Irwin CA, Cranford CO, et al. The impact of telemedicine on patients’ cost savings: some preliminary findings. Telemed J E Health 2003;9:361–7. 10.1089/153056203772744680 [DOI] [PubMed] [Google Scholar]
- 3. Spaulding R, Belz N, DeLurgio S, et al. Cost savings of telemedicine utilization for child psychiatry in a rural kansas community. Telemed J E Health 2010;16:867–71. 10.1089/tmj.2010.0054 [DOI] [PubMed] [Google Scholar]
- 4. Dullet NW, Geraghty EM, Kaufman T, et al. Impact of a university-based outpatient telemedicine program on time savings travel costs, and environmental pollutants. Value Health 2017;20:542–6. 10.1016/j.jval.2017.01.014 [DOI] [PubMed] [Google Scholar]
- 5. Snoswell CL, Taylor ML, Comans TA, et al. Determining if telehealth can reduce health system costs: scoping review. J Med Internet Res 2020;22:e17298. 10.2196/17298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Almathami HKY, Win KT, Vlahu-Gjorgievska E. Barriers and facilitators that influence telemedicine-based, real-time, online consultation at patients. J Med Internet Res 2020;22:e16407. 10.2196/16407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Eze ND, Mateus C, Cravo Oliveira Hashiguchi T. Telemedicine in the OECD: an umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS One 2020;15:e0237585. 10.1371/journal.pone.0237585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hussaini SMQ, Gupta A, Dusetzina SB. Financial toxicity of cancer treatment. JAMA Oncol 2022;8:788. 10.1001/jamaoncol.2021.7987 [DOI] [PubMed] [Google Scholar]
- 9. Tuckson RV, Dzau VJ, Lurie N. Creating healthy communities after disasters. N Engl J Med 2017;377:1806–8. 10.1056/NEJMp1711834 [DOI] [PubMed] [Google Scholar]
- 10. Patel KB, Turner K, Alishahi Tabriz A, et al. Estimated indirect cost savings of using telehealth among nonelderly patients with cancer. JAMA Netw Open 2023;6:e2250211. 10.1001/jamanetworkopen.2022.50211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Figueroa LM. Telehealth in Colombia, challenges associated with COVID-19. Biomedica 2020;40:77–9. 10.7705/biomedica.5594 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Escobar MF, Echavarría MP, Carvajal JA, et al. Hospital padrino: a collaborative strategy model to tackle maternal mortality: a mixed methods study in a middle-income region. Lancet Reg Health Am 2024;31:100705. 10.1016/j.lana.2024.100705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Shemilt I, James T, Marcello M. A web-based tool for adjusting costs to a specific target currency and price year. Evid & Pol 2010;6:51–9. 10.1332/174426410X482999 [DOI] [Google Scholar]
- 14. Departamento Administrativo Nacional de Estadística (DANE) . Situación de las mujeres rurales desde las estadísticas oficiales, 2022. Available: https://www.dane.gov.co/files/investigaciones/notas-estadisticas/oct-2022-nota-estadistica-mujer-rural-presentacion.pdf
- 15. Brundisini F, Giacomini M, DeJean D, et al. Chronic disease patients’ experiences with accessing health care in rural and remote areas: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser 2013;13:1–33. [PMC free article] [PubMed] [Google Scholar]
- 16. Speyer R, Denman D, Wilkes-Gillan S, et al. Effects of telehealth by allied health professionals and nurses in rural and remote areas: a systematic review and meta-analysis. J Rehabil Med 2018;50:225–35. 10.2340/16501977-2297 [DOI] [PubMed] [Google Scholar]
- 17. Carroll M, Cullen T, Ferguson S, et al. Innovation in Indian healthcare: using health information technology to achieve health equity for American Indian and Alaska native populations. Perspect Health INF Manag 2011;8:1d. [PMC free article] [PubMed] [Google Scholar]
- 18. Lagomarsino G, Garabrant A, Adyas A, et al. Moving towards universal health coverage: health insurance reforms in nine developing countries in Africa and Asia. Lancet 2012;380:933–43. 10.1016/S0140-6736(12)61147-7 [DOI] [PubMed] [Google Scholar]
- 19. Balabanova D, Mills A, Conteh L, et al. Good health at low cost 25 years on: lessons for the future of health systems strengthening. Lancet 2013;381:2118–33. 10.1016/S0140-6736(12)62000-5 [DOI] [PubMed] [Google Scholar]
- 20. Dirección de Epidemiología y Demografía . Análisis de Situación de Salud (ASIS) Colombia, 2020. Ministerio de Salud y Protección Social, 2020. [Google Scholar]
- 21. Moyer JD, Verhagen W, Mapes B, et al. How many people is the COVID-19 pandemic pushing into poverty? A long-term forecast to 2050 with alternative scenarios. PLoS One 2022;17:e0270846. 10.1371/journal.pone.0270846 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Departamento Administrativo Nacional de Estadística (DANE) . Comunicado de Prensa Producto Interno Bruto (PIB) IV Trimestre y Año 2020. Bogotá D.C, 2021. [Google Scholar]
- 23. Departamento Administrativo Nacional de Estadística (DANE) . Boletín Técnico Gran Encuesta Integrada de Hogares (GEIH) Diciembre 2020. Bogotá D.C, 2021. Available: https://www.dane.gov.co/files/investigaciones/boletines/ech/ech/bol_empleo_dic_20.pdf [Google Scholar]
- 24. Departamento Administrativo Nacional de Estadísticas - DANE . Empleo Informal y Seguridad Social, 2023. Available: https://www.dane.gov.co/index.php/estadisticas-por-tema/salud/informalidad-y-seguridad-social/empleo-informal-y-seguridad-social-historicos
- 25. Wolfe MK, McDonald NC, Holmes GM. Transportation barriers to health care in the United States: findings from the national health interview survey, 1997-2017. Am J Public Health 2020;110:815–22. 10.2105/AJPH.2020.305579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Zachrison KS, Boggs KM, Hayden EM, et al. Understanding barriers to telemedicine implementation in rural emergency departments. Ann Emerg Med 2020;75:392–9. 10.1016/j.annemergmed.2019.06.026 [DOI] [PubMed] [Google Scholar]
- 27. Atmojo JT, Sudaryanto WT, Widiyanto A, et al. Telemedicine, cost effectiveness, and patients satisfaction: a systematic review. J Health Policy Manage 2020;5:103–7. 10.26911/thejhpm.2020.05.02.02 [DOI] [Google Scholar]
- 28. Paquette S, Lin JC. Outpatient telemedicine program in vascular surgery reduces patient travel time, cost, and environmental pollutant emissions. Ann Vasc Surg 2019;59:167–72. 10.1016/j.avsg.2019.01.021 [DOI] [PubMed] [Google Scholar]
- 29. Ministerio de Transporte . Transporte en Cifras 2021. Anuario Nacional de Transporte 2022;55–8. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2024-084447supp001.pdf (34.1KB, pdf)
Data Availability Statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author [MFE], upon reasonable request.